










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.30 no.3 São Paulo set./dez. 2020
http://dx.doi.org/10.7322/jhgd.v30.11063
ORIGINAL ARTICLE
Trends in case-fatality rates of COVID-19 in the World, between 2019 - 2020
Tendência das taxas de letalidade de covid-19 no mundo, entre 2019-2020
Henrique de Moraes BernalI; Carlos Eduardo SiqueiraII, III; Fernando AdamiI; Edige Felipe de Sousa SantosI, IV
ILaboratório de Delineamento em Estudos e Escrita Científica, Centro Universitário Saúde ABC, Av. Príncipe de Gales, 667 - Santo André - SP - Brazil - CEP - 09060-590
IISchool for the Environment, University of Massachusetts Boston. 100 Morrissey Boulevard, Boston, MA, 02125
IIIGraduate Entry Medical School, University of Limerick, V94 T9PX, Limerick, Ireland
IVFaculdade de Saúde Pública, Universidade de São Paulo (USP), Av. Dr. Arnaldo, 715 - São Paulo - SP - Brasil - CEP - 01246-904
ABSTRACT
INTRODUCTION: CoV infections can potentially cause from a simple cold to a severe respiratory syndrome, such as the Severe Acute Respiratory Syndrome and the Middle East Respiratory Syndrome (MERS-CoV). The COVID-19 created a new reality for global healthcare models
OBJETIVE: To evaluate trends in case-fatality rates of COVID-19 in the World
METHODS: We conducted a population-based time-series study using public and official data of cases and deaths from COVID-19 in Argentina, Australia, Brazil, Chile, China, Colombia, France, Germany, India, Iran, Italy, Japan, Mexico, Morocco, New Zealand, Nigeria, Peru, Saudi Arabia, South Africa, South Korea, Spain, Switzerland, United Kingdom, United States and Russian, between December, 2019 and August, 2020. Data were based on reports from European Centre for Disease Prevention and Control. COVID-19 was defined by the International Classification of Diseases, 10th revision (U07.1). A Prais-Winsten regression model was performed and the Daily Percentage Change (DPC) calculated determine rates as increasing, decreasing or flat
RESULTS: During the study period, trends in case-fatality rates in the world were flat (DPC = 0.3; CI 95% [-0.2: 0.7]; p = 0.225). In Africa, Morocco had decreasing trends (DPC = -1.1; CI 95% [-1.5: -0.7]; p < 0.001), whereas it were increasing in South Africa (p < 0.05) and flat in Nigeria (p > 0.05). In the Americas, Argentina showed a decreasing trend in case-fatality rates (DPC = -0.6; CI 95% [-1.1: -0.2]; p = 0.005), the U.S. had flat trends (p > 0.05) and all other American countries had increasing trends (p < 0.05). In Asia, Iran had decreasing trends (DPC = -1.5; CI 95% [-2.6 : -0.2]; p = 0.019); China and Saudi Arabia showed increasing trends (p < 0.05), while in India, Japan and South Korea they were flat (p > 0.05). European countries had mostly increasing trends (p < 0.05): Germany, Italy, Spain, the UK and Russia; France and Switzerland had flat trends (p > 0.05). Finally, in Oceania, trends in case-fatality rates were flat in Australia (p > 0.05) and increasing in New Zealand (p < 0.05
CONCLUSION: Trends in case-fatality rates of COVID-19 in the World were flat between December, 31 and August, 31. Argentina, Iran and Morocco were the only countries with decreasing trends. On the other hand, South Africa, Brazil, Canada, Chile, Colombia, Mexico, Peru, China, Saudi Arabia, Germany, Spain, United Kingdom, Russian and New Zealand had increasing trends in case-fatality rate. All the other countries analyzed had flat trends. Based on case-fatality rate data, our study supports that COVID-19 pandemic is still in progress worldwide
Keywords: COVID-19, Trends, Case-Fatality, Epidemiology.
RESUMO
INTRODUÇÃO: As infecções por CoV podem causar desde um simples resfriado até uma síndrome respiratória grave, como a Síndrome Respiratória Aguda Grave e a Síndrome Respiratória do Oriente Médio (MERS-CoV). O COVID-19 impôs uma nova realidade em termos de modelos globais de saúde
OBJETIVO: Avaliar as tendências das taxas de letalidade do COVID-19 no mundo
MÉTODO: Estudo de séries temporais de base populacional usando dados públicos e oficiais de casos e mortes por COVID-19 na Argentina, Austrália, Brasil, Chile, China, Colômbia, França, Alemanha, Índia, Irã, Itália, Japão, México, Marrocos, Nova Zelândia, Nigéria, Peru, Arábia Saudita, África do Sul, Coreia do Sul, Espanha, Suíça, Reino Unido, Estados Unidos (EUA) e Rússia, entre 31 dezembro de 2019 e 31 agosto de 2020. Os dados foram baseados nos relatórios do Centro Europeu de Prevenção e Controle de Doenças. COVID-19 foi definido pela Classificação Internacional de Doenças, 10ª revisão (U07.1). Para análise estatística, foi realizado o modelo de regressão de Prais-Winsten, a partir do qual foi possível calcular a variação percentual de mudança diária (DPC) das taxas, classificadas como crescentes, decrescentes ou estacionárias
RESULTADOS: Durante o período do estudo, as taxas de letalidade no mundo permaneceram estacionárias (DPC = 0,3; IC 95% [-0,2: 0,7]; p = 0,225). Na África, Marrocos teve tendência decrescente (DPC = -1,1; IC 95% [-1,5: -0,7]; p <0,001), enquanto na África do Sul houve tendência crescente (p < 0,05) e estacionária na Nigéria (p > 0,05). Em relação às Américas, a Argentina revelou tendência decrescente nas taxas de letalidade (DPC = -0,6; IC 95% [-1,1: -0,2]; p = 0,005), os EUA demonstraram tendência estacionária (p > 0,05) e todos os outros países americanos demonstraram tendências crescentes (p < 0,05). Na Ásia, o Irã apresentou tendência decrescente (DPC = -1,5; IC 95% [-2,6: -0,2]; p = 0,019); China e Arábia Saudita apresentaram tendências crescentes (p <0,05), enquanto Índia, Japão e Coreia do Sul mantiveram tendência estacionária (p > 0,05). A maioria dos países europeus apresentaram tendências crescentes (p <0,05): Alemanha, Itália, Espanha, Reino Unido e Rússia; França e Suíça demonstraram tendências estacionárias (p > 0,05). Por fim, na Oceania, a tendência nas taxas de letalidade na Austrália foi estacionária (p > 0,05) e aumentou na Nova Zelândia (p < 0,05
CONCLUSÃO: A tendência nas taxas de letalidade por COVID-19 no mundo permaneceu estacionária entre 31 de dezembro de 2019 e 31 de agosto de 2020. Argentina, Irã e Marrocos foram os únicos países com tendências decrescentes. Por outro lado, África do Sul, Brasil, Canadá, Chile, Colômbia, México, Peru, China, Arábia Saudita, Alemanha, Espanha, Reino Unido, Rússia e Nova Zelândia apresentaram tendências crescentes de letalidade. Todos os outros países analisados demonstraram tendências estacionárias. De acordo com dados de letalidade, nosso estudo confirma que a pandemia de COVID-19 ainda está em fase de progressão em todo o mundo
Palavras-chave: COVID-19, Tendência, Letalidade, Epidemiologia.
Authors summary
Why was this study done?
• COVID-19 created a new reality in terms of global healthcare models.
• The scientific evidence so far available are not enough to meet the demands of the pandemic.
• Epidemiological studies are relevant to trigger public health strategies for spread control.
What did the researchers do and find?
• We conducted a population-based time-series study using public and official data of cases and deaths from COVID-19 in Argentina, Australia, Brazil, Chile, China, Colombia, France, Germany, India, Iran, Italy, Japan, Mexico, Morocco, New Zealand, Nigeria, Peru (33538625), Saudi Arabia, South Africa, South Korea, Spain, Switzerland, United Kingdom (UK), United States (U.S.) and Russia, between December, 2019 and August, 2020.
• Trends in case-fatality rates were decreasing only in three countries among twenty-six analyzed: Argentina, Iran and Morocco. It was more significant in Iran.
• Nigeria, the U.S., India, Japan, South Korea, France, Switzerland and Australia had flat trends in case-fatality rates due to COVID-19.
• All the other countries analyzed in our study had increasing trends in case-fatality rates, with more significant results among countries of America and Europe.
What do these findings mean?
• Increasing trends in case-fatality rates were higher between countries of Americas and Europe, suggesting a greater severity of the disease in those continents.
• Decreasing trends in case-fatality rates found in Argentina, Iran and Morocco should attract international attention in order to guide public health policies to reduce COVID-19 case-fatality.
• Based on case-fatality data, our study supports that COVID-19 pandemic is still in progress worldwide.
INTRODUCTION
The coronaviruses (CoV) are a large family of viruses, so named because of surface spikes that looks resemble a crown (corona, Latim)1. The CoV infections can potentially cause from a simple cold to a severe respiratory syndrome, such as the Severe Acute Respiratory Syndrome (SARS-CoV) and the Middle East Respiratory Syndrome (MERS-CoV)1,2. The COVID-19 is a new variant of the coronaviruses, first isolated in China. The novel coronavirus differs from the others because of its high impact in public health and the huge number of new cases reported in a short time-period2,3.
The COVID-19 created a new reality for global healthcare delivery models1,2. The scientific evidence so far available are not enough to meet the demands to face the pandemic, since data about specific treatment and vaccines are insufficient (WHO)4, which forces governments to recommend social distancing as the principal effective strategy to contain the spread of the disease.
Pandemic scenarios require information in order to promptly (re)organize health practices and to provide health care, such as prevention and treatment, control and rehabilitation, since it is essential to health care managers and providers5. To address this demand, epidemiological studies are relevant to trigger public health strategies to control.
Furthermore, this global scenario suggests that nobody can now be protected from an emerging and poorly known infectious disease. It would be unwise to make specific predictions about the natural history of the disease or the results to containing SARS-CoV-2 outbreaks, but it is possible to make some incipient conclusions and to protect the most vulnerable from the virus6.
In the health area7, research is designed to develop reliable data on problems and needs that are important to the individual/community, with a particular focus on guiding practitioners. In line with that, findings about social distancing are probably effective to reduce case-fatality, since they are suitable to prevent and control the extensive spread of COVID-198.
There is a lack of population-based studies assessing the trends in case-fatality rates in different countries in the world, which is crucial information to understand the pandemic dynamic, the severity of the disease and to elaborate public global health policies5. The traditional cumulative case-fatality rates may possibly underestimate the real case-fatality, since each region of the world is experiencing a different stage of the pandemic9. Case-fatality rates are not static. Rather, they tend to be dynamic and change over time. Thus, we aimed to evaluate trends in case-fatality rates of COVID-19 around the World.
METHODS
This a population-based time-series study with public and official data available on the website of the European Centre for Disease Prevention and Control (https://www.ecdc.europa.eu/en).
Data were collected on August 31, 2020, by household address for COVID-19 reported cases. Population data were extracted from the Country Meters website (https://countrymeters.info/en), and included the following countries: Argentina (45,757,489 inhabitants), Australia (2,5949,452 inhabitants), Brazil (217,040,683 inhabitants), Chile (18,944,479 inhabitants), China (1,410,334,120 inhabitants), Colombia (50,697,280 inhabitants), France (65,790,781 inhabitants), Germany (81,466,451 inhabitants), India (2,195,755,104 inhabitants), Iran (84,341,761 inhabitants), Italy (60,016,386 inhabitants), Japan (125,901,152 inhabitants), Mexico (136,136,481 inhabitants), Morocco (36,833,644 inhabitants), New Zealand (4,695,515 inhabitants), Nigeria (208,242,721), Peru (33,538,625 inhabitants), Saudi Arabia (35,457,606 inhabitants), South Africa (57,581,898), South Korea (51,472,090 inhabitants), Spain (45,690,902 inhabitants), Switzerland (8,770,577 inhabitants), United Kingdom (66,679,096 inhabitants), United States (333,487,241 inhabitants), and Russia (146,590,156 inhabitants).
The study analyzed cases and deaths reported between December 31, 2019 and August 31, 2020. New cases and deaths were collected according to day of reporting.
Study population, inclusion and exclusion criteria
The World Health Organization assigned the emergency ICD-10 code of "U07.1 COVID-19, virus identified" to a disease diagnosis of COVID-19 confirmed by laboratory testing.
Data collection started in different dates in each country according to the reporting of new cases. In Argentina, it started on March 03; in Australia, on January 25; in Brazil, on January 26; in Canada, on January 26; in China, on January 21; in Chile, on March 03; in Colombia, on March 07; in France, on January 25; in Germany, on January, 28; in India, on January 30; in Iran, on February 20; in Italy, on January 31; in Japan, on January 21; in Mexico, on February 29; in Morocco, on March 03; in New Zealand, on February 28; in Nigeria, on February 28; in Peru, on March 07; in Saudi Arabia, on March 03; in South Africa, on March 06; in South Korea, on January 21; in Spain, on February 02; in Switzerland, on February 26; in the United Kingdom, on January 31; in the United States, on January 21; and in Russia, on February 01.
All confirmed cases and deaths of COVID-19 were included. They were registered according to the 10th Revision of the International Classification of Diseases (ICD-10) as COVID-19, virus identified (U07.1).
Data Collection Procedures
Data were extracted from the public and official data system of European Centre for Disease Prevention and Control (ECDC), section "Latest situation update, epidemiological curve and global distribution." ECDC is closely monitoring the outbreak, providing risk assessments and public health guidance.
Confirmed cases and deaths were collected from national health information systems responsible for registering, analyzing and publishing official country health data. The data were transferred to the European Centre for Disease Prevention and Control, which updated it daily.
Data about the resident population of each country was obtained from the Country Meters website and we projected population from January to August, 2020 The population data account for the total country population as of January 01, 2020.
In order to minimize possible discrepancies, the data were extracted by two different researchers independently.
Statistical analysis
The COVID-19 incidence (new cases / population) and mortality (deaths / population) rates were calculated, per 1,000,000 inhabitants, and case-fatality (total deaths / total cases) rates, as daily percentage, between January and May 2020.
For trend analyses, we used methods proposed by Antunes and Cardoso (2015)10. Time-series rates were calculated using a Prais-Winsten regression model, which allowed first-order autocorrelation corrections on values by time. Thus, the following values were estimated: angular coefficient (β) and respective probability (p), considering a significance level of 95% confidence interval (CI 95%).
The data modeling process included transforming rates (dependent variable = Y value) into a base 10 logarithmic function. The independent variable (X value) was days of historical series. We also used the Durbin-Watson test to measure the existence of a first-order autocorrelation of the time series of the daily coefficients, and to verify if the correlation was compatible with the random regression residuals hypothesis11.
The logarithm rates results (β) of Prais-Winsten regression allowed to estimate the Daily Percent Chance (DPC) in each country, with the respective confidence intervals (95% CI)10:

This procedure made it possible to determine rates as increasing, decreasing or flat, and to quantify percent change in daily12 incidence, mortality and case-fatality rates. The trend was considered to be flat when the coefficient was not significantly different from zero (p > 0.05).
To facilitate the visualization of the trends in case-fatality rates, we reduced the random variation in the graph using the five-order moving average technique11.
RESULTS
We used the Stata 15.1 statistical software to conduct statistical analyses (College Station, TX, U.S. 2018).
Case-fatality Rates
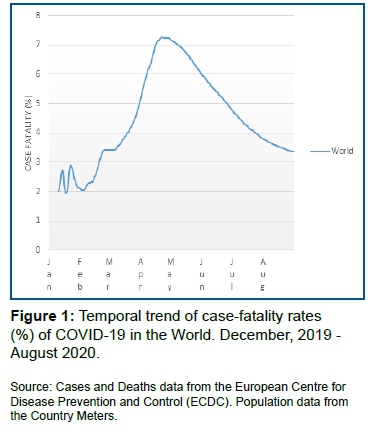
Between December 31, 2019, and August 3, 2020, the case-fatality due to COVID-19 in the world was 3.4%.
In Africa, among countries analyzed, the highest case-fatality was found in South Africa (2.2%), followed by Nigeria (1.9%) and Morocco (1.8%). Similar results were found in Oceania: Australia (2.4%) and New Zealand (1.6%) (Table 1).
In the Americas, Mexico had the greatest case-fatality rate: 10.8%, which represents the fourth country with the highest percentage. Canada also showed high case-fatality rate: 7.1%. In the other American countries we found similar percentages in case-fatality rates, except Chile, where it was 0.5%, the lowest rate between all countries (Table 1).
Asia had two different profile of groups: China and Iran had case-fatality rate above 5.0%, while the rest of Asian countries showed rates below 2.0% (Table 1).
Europe had the most heterogeneous results compared with other continents. Italy, France and United Kingdom had case-fatality rates above 10.0%. Spain and Switzerland show intermediary rates among European countries, while German and Russia were the countries with the lowest rates in case-fatality in the continent. (Table 1).
Trends in case-fatality rates
Trends in case-fatality rates in the world were flat (DPC = 0.3; CI 95% [-0.2 : 0.7]; p = 0.225) in the study period (Table 2, Fig. 1).
Morocco was one of the three countries in which the case-fatality rate was decreasing (DPC = -1.1; CI 95% [-1.5 : -0.7]; p < 0.001). In Nigeria, the case-fatality was flat, while in South Africa it was increasing (Table 2, Fig. 2).

In the Americas, Argentina had decreasing trends in case-fatality (DPC = -0.6; CI 95% [-1.1: -0.2]; p = 0.005), while all other countries had increasing trends. The United States, on the other hand, had flat rate trends. (Table 2, Fig. 3).

With regard to Asian countries, Iran showed decreasing trends in case-fatality rate (DPC = -1.5; CI 95% [-2.6: -0.2]; p = 0.019). China and Saudi Arabia had increasing trends, while India and South Korea showed flat tendency (Table 3, Fig. 4).

In Europe, France and Switzerland had flat trends in case-fatality, but all the other countries had increasing tendency (Table 3, Fig. 5).

Finally, in Oceania, Australia had flat tendency, while New Zealand had increasing trends in case-fatality due to COVID-19 (Table 3, Fig 6).

DISCUSSION
We estimated trends in case-fatality rates by calculating the Daily Percent Change in case-fatality rates, which allows the understanding of the dynamic of the pandemic better than simply analyzing rates9. Between December 31, 2019 and August 31, 2020, trends in case-fatality due to COVID-19 in the world remained flat. Argentina, Iran and Morocco were the only countries that had decreasing trends in case-fatality rates. Nigeria, United States, India, Japan, South Korea, France, Germany, Switzerland and Australia had flat tendency. All other countries showed increasing trends, which can indicate progressive severity of the disease around the five continents.
Our findings showed case-fatality rates in the world similar to Zhao et al. study, who found a rate of 3.1% after analyzing 30 studies with 53.000 patients12. Another study estimating case-fatality rates showed expected rates for this pandemic ranging from 2.9% to 3.0%9. As we already pointed out, case-fatality rates are not static, but rather dynamic. Our statistical analyses of world trends suggest a flat tendency (p > 0.05).
Increasing Case-Fatality Rate Trends
South Africa, Brazil, Canada, Chile, Colombia, Mexico, Peru, China, Saudi Arabia, Germany, Italy, Spain, United Kingdom, Russia and New Zealand had increasing trends in case-fatality rates due to COVID-19. Among all of them, Canada, Mexico, Peru, Germany, Italy, Spain and United Kingdom had case-fatality rates above the world's rate, which can possibly indicate an highest severity of the disease in those nations. Germany, Spain and United Kingdom showed the greatest Daily Percent Change, indicating that Europe still is the continent most affected by COVID.
With regard to Canada, our results contrasts with Abdollahi et al. findings, who found a case-fatality rate of 1.6% (CI 95% 0.7%-3.1%) on April 22, which is significantly lower than ours13. It demonstrates that COVID-19 has substantially increased over the past 4 months. Therefore, it is noteworthy that Canada had a high severity of the disease, which is still in progress.
Regarding Europe, we found the same behavior for case-fatality rates pointed by Pachetti et al., who described a significant lower rate for Germany (0.31% CI 95% [0.29; 0.33]) compared to the other nations, on April 3014. Although the estimation og case-fatality rates are not high in Germany, this country had the second increasing Daily Percent Change in case-fatality rates among all 26 countries analyzed. Aside from Germany, Russia had low case-fatality rates, but it had also increasing trends. The United Kingdom had the highest case-fatality rate and upward trend among the nations analyzed in our study.
Flat Case-Fatality Rate Trends
Nigeria, United States, India, Japan, South Korea, France, Switzerland, Australia had flat tendency in case-fatality rates due to COVID-19. France and Switzerland were the only nations with rates above the world's, which suggests the hypothesis that Europe is not in a regression phase of the pandemic.
With respect to Australia, Chin et al. already noted signs that pandemic was under control. They identified case-fatality rates raging 0.4% to 3.0%, tending to decrease after March 2915. This decrease may be attributed to timely implementation and strict enforcement of bans on travel and social gatherings, as well as concerted diagnostic and management strategies.
The United States also showed signs of controlling the spread of COVID-19. On April 22, Abodollahi et al. reported a case-fatality rate of 6.1% (CI 95% 5.4%-6.9%)13, which corresponds approximately 2 times our results. This finding suggests that case-fatality rates might have decreased in the previous 4 months and a new flat trend emerged.
Decreasing Case-Fatality Rate Trends
Morocco, Argentina and Iran showed decreasing trends ins case-fatality rates of COVID-19. Despite of that, Iran was the only country in which case-fatality was above the estimative of the world's rate.
As of May 13, 2020 Ouchetto et al. reported case-fatality rate 5.26% in Morocco16, almost 3 times greatest than our findings, supporting the hypothesis that pandemic is tending to be controlled in this nation.
Regarding Iran, we have to interpret these results with parsimony, since according to studies, cases reported in official statistics at the beginning of the epidemics were likely to grossly underestimate the total of actual cases. Thus estimating the actual case-fatality rates due to COVID-19 is currently impossible17.
It is important to highlight that our analysis was based on public and official secondary data from the European Centre for Disease Prevention and Control. Even considering unknown underreporting, these are the best available data to formulate public health policies. The analysis of incidence, mortality, case-fatality rates and their respective trends allowed for measurement of risk, severity, and magnitude, which are defining indicators to understand the dynamics of pandemics6.
The time-series regression model used in this study allowed to dimension the existence the Daily Percent Change (DPC) in case-fatality rates, which made it possible to measure the dynamic variation of the pandemic among 26 countries around the five continents worldwide.
CONCLUSIONS
Trends in case-fatality rates of COVID-19 in the World were flat between December, 31 and August, 31. Argentina, Iran and Morocco were the only countries with decreasing trends. On the other hand, South Africa, Brazil, Canada, Chile, Colombia, Mexico, Peru, China, Saudi Arabia, Germany, Spain, United Kingdom, Russian and New Zealand had increasing trends in case-fatality rate. All the other countries analyzed had flat trends. Based on case-fatality rate data, our study supports that COVID-19 pandemic is still in progress worldwide.
Funding
None.
Competing interests
None declared.
Ethical approval
Not required.
Acknowledgements
We thank Prof. Luiz for his contributions in the study design and scientific writing.
Contact the authors for more information
Henrique M. Bernal - henriquembernal@hotmail.com
Carlos Eduardo Siqueira - carlos.siqueira@umb.edu
Fernando Adami - Fernando.adami@fmabc.br
Edige Felipe de Sousa Santos - edige@usp.br
REFERENCES
1.Brasil. Ministério da Saúde. What coronavirus is? (COVID-19). [cited 2020 Mair 09] Available from: https://coronavirus.saude.gov.br/ [ Links ]
2.Pimentel RMM, Daboin BEG, Oliveira AG, Macedo Jr H. The dissemination of COVID-19: an expectant and preventive role in global health. J Hum Growth Dev. 2020; 30(1): 135-140. DOI: http://doi.org/10.7322/jhgd.v30.9976 [ Links ]
3.Phelan A, Katz R, Gostin LO. The Novel Coronavirus Originating in Wuhan, China: Challenges for Global Health Governance. JAMA. 2020; 323(8): 709-10. DOI: http://doi.org/10.1001/jama.2020.1097 [ Links ]
4.World Health Organization (WHO). Available on: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/malaria-and-the-covid-19-pandemic [ Links ]
5.Abreu LC. Integrated actions and strengthening of Public Health System in Brazil in a time of pandemic. J Hum Growth Dev. 2020; 30(1): 05-08. DOI: https://doi.org/10.7322/jhgd.v30.9980 [ Links ]
6.Pandemic responses: Planning to neutralize SARSCoV-2 and prepare for future outbreaks. PLoS Med 17(4): e1003123. DOI: https://doi.org/10.1371/journal.pmed.1003123 [ Links ]
7.Dircinha S. Scientific method and research in health: orientation for professional practice. J Hum Growth Dev. 2019; 29(1): 5-9. DOI: http://dx.doi.org/10.7322/jhgd.157742 [ Links ]
8.Valenti VE, Menezes PL, de Abreu ACG, Alves Vieira GN, Garner DM. Social distancing measures could have reduced estimated deaths related to COVID-19 in Brazil. J Hum Growth Dev. 2020; 30(2):164-169. DOI: https://doi.org/10.7322/jhgd.v30.10360 [ Links ]
9.Abou Ghayda R, Lee KH, Han YJ, et al. Estimation of global case fatality rate of coronavirus disease 2019 (COVID-19) using meta-analyses: Comparison between calendar date and days since the outbreak of the first confirmed case [published online ahead of print, 2020 Aug 31]. Int J Infect Dis. 2020; S1201-9712(20) 30694-9. DOI: https://doi.org/10.1016/j.ijid.2020.08.065 [ Links ]
10.Antunes JLF, Cardoso MRA. [Using time series analysis in epidemiological studies]. Epidemiol Serv Saúde 2015; 24 (03) 565-576. [ Links ]
11.Calderon MG, Santos EFS, Abreu LC, Raimundo RD. Increasing prevalence, time trend and seasonality of gastroschisis in São Paulo state, Brazil, 2005-2016. Sci Rep. 2019; 9(1):14491. Published 2019 Oct 10. DOI: https://doi.org/10.1038/s41598-019-50935-1 [ Links ]
12.Zeng W, Zhang Y, Wang L, et al. Ambient fine particulate pollution and daily morbidity of stroke in Chengdu, China. PLoS One. 2018; 13(11): e0206836. Published 2018 Nov 6. DOI: https://doi.org/10.1371/journal.pone.0206836 [ Links ]
13.Zhao X, Zhang B, Li Pet al. (2020). Incidence, clinical characteristics and prognostic factor of patients with COVID-19: A systematic review and meta-analysis. medRxiv 2020.03.17.20037572. DOI: https://doi.org/10.1101/2020.03.17.20037572 [ Links ]
14.Abdollahi E, Champredon D, Langley JM, Galvani AP, Moghadas SM. Temporal estimates of case-fatality rate for COVID-19 outbreaks in Canada and the United States. CMAJ. 2020; 192(25): E666-E670. DOI:10.1503/cmaj.200711. [ Links ]
15.Pachetti M, Marini B, Giudici F, et al. Impact of lockdown on Covid-19 case fatality rate and viral mutations spread in 7 countries in Europe and North America. J Transl Med. 2020; 18(1): 338. Published 2020 Sep 2. DOI: https://doi.org/10.1186/s12967-020-02344-6 [ Links ]
16.Chin KL, Ofori-Asenso R, Jordan KA, Jones D, Liew D. Early signs that COVID-19 is being contained in Australia. J Infect. 2020; 81(2): 318-356. DOI: https://doi.org/10.1016/j.jinf.2020.04.042 [ Links ]
17.Ouchetto O, Drissi Bourhanbour A, Boumhamdi M. Effectiveness of containment measures to control the spread of COVID-19 in North Africa [published online ahead of print, 2020 Sep 3]. Disaster Med Public Health Prep. 2020; 1-15. DOI: https://doi.org/10.1017/dmp.2020.314 [ Links ]
18.Battegay M, Kuehl R, Tschudin-Sutter S, Hirsch HH, Widmer AF, Neher RA. 2019-novel Coronavirus (2019-nCoV): estimating the case fatality rate-a word of caution. Swiss Med Wkly. 2020;150(0506). [ Links ]
 Correspondence:
Correspondence:
Edige Felipe de Sousa Santos
edige@usp.br
Received: May 2020
Revised: September 2020
Accepted: September 2020


{kind=link}
{kind=link}
{kind=link}