










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.1 Marília ene./abr. 2021
http://dx.doi.org/10.36311/jhgd.v31.10925
ORIGINAL ARTICLE
Chagas Disease in the Western Brazilian Amazon: Epidemiological Overview from 2007 to 2018
Fernanda Portela MadeiraI, II; Adila Costa de JesusI, II; Madson Huilber da Silva MoraesI, II; Natália Froeder BarrosoIII; Gabriela Vieira de Souza CastroI, II; Mariane Albuquerque Lima RibeiroI, IX, X; Joseane Elza Tonussi MendesIX, X; Luís Marcelo Aranha CamargoI, IV, V, VI, VII; Dionatas Ulises de Oliveira MeneguettiI, VIII; Paulo Sérgio BernardeI, II
IStrict Sensu Post-Graduate Program in Health Sciences in Western Amazonia, Universidade Federal do Acre, Rio Branco, Acre, Brazil
IIMultidisciplinary Center, Universidade Federal do Acre, Campus Floresta, Cruzeiro do Sul, Acre, Brazil
IIICenter for Health and Sports Sciences, Federal University of Acre, Rio Branco, Acre, Brazil
IVInstitute of Biomedical Sciences -5, University of São Paulo, Monte Negro, Rondônia, Brazil
VDepartment of Medicine, Centro Universitário São Lucas, Porto Velho, Rondônia, Brazil
VICentro de Pesquisa em Medicina Tropical de Rondônia-CEPEM/SESAU, Rondônia, Brazil
VIIINCT/CNPq EpiAmo-Rondônia, Brazil
VIIIColégio de Aplicação, Universidade Federal do Acre, Rio Branco, Acre, Brazil
IXPrograma de Pós-Graduação em Ciências da Saúde, Centro Universitário Saúde ABC, Santo André, São Paulo, Brasil
XLaboratório de Delineamento de Estudo e Escrita Científica, Centro Universitário FMABC, Santo André, São Paulo, Brasil
ABSTRACT
INTRODUCTION: Chagas disease (CD) is a disease caused by the protozoan flagellates of the Kinetoplastid order Trypanosoma cruzi. Approximately 8,000,000 people are infected worldwide, mainly in Latin America, causing disabilities and more than 10,000 deaths per year
OBJECTIVE: This study aimed to describe the epidemiological panorama of CD in the Western Brazilian Amazon from 2007 to 2018.
METHODS: In this ecological study, secondary data regarding the confirmed cases of T. cruzi infection in the states of Acre, Amazonas, Rondônia, and Roraima were collected from the Single Health System Notification Information System of the Department of Informatics of the Single Health System and were analyzed. The data were used to characterize the epidemiological profile of T. cruzi infection and to determine the frequency of infection in Western Amazonia.
RESULTS: A total of 184 cases of CD were reported in Western Amazonia, and the highest number of cases was reported in the states of Amazonas and Acre.
CONCLUSION: The epidemiological panorama of the Western Brazilian Amazon from 2007 to 2018 includes a greater number of cases of T. cruzi infection in men aged 20-39 years and those living in rural areas. Oral transmission was prevalent in the region during the study, and the highest number of cases was reported in the months of April and December. Epidemiological data are an important resource for understanding the dynamics of CD and the main aspects related to the health-disease process.
Keywords: Epidemiological data, Epidemiology, American trypanosomiasis.
Authors summary
Why was this study done?
This study aimed to describe the epidemiological panorama of CD in the Western Brazilian Amazon from 2007 to 2018.
What did the researchers do and find?
In this ecological study, secondary data regarding the confirmed cases of T. cruzi infection in the states of Acre, Amazonas, Rondônia, and Roraima were collected from the Single Health System Notification Information System of the Department of Informatics of the Single Health System and were analyzed
What do these findings mean?
A total of 184 cases of CD were reported in Western Amazonia, and the highest number of cases was reported in the states of Amazonas and Acre. The epidemiological panorama of the Western Brazilian Amazon from 2007 to 2018 includes a greater number of cases of T. cruzi infection in men aged 20-39 years and those living in rural areas. Oral transmission was prevalent in the region during the study, and the highest number of cases was reported in the months of April and December. Epidemiological data are an important resource for understanding the dynamics of CD and the main aspects related to the health-disease process.
INTRODUCTION
Chagas disease (CD) is a disease caused by the protozoan flagellate of the Kinetoplastid order Trypanosoma cruzi, whose vector is an insect belonging to the Reduviidae family and subfamily Triatominae popularly known as barber1.
The most common method of T. cruzi transmission reported by several previous studies is through the vector; unlike other vector-borne diseases, the transmission of T. cruzi does not occur by inoculation of the parasite with the vector's saliva, but by exposure to feces or urine containing the infectious forms1,2. Other forms of disease transmission include transplacental, blood transfusion, organ transplantation, ingestion of contaminated food, and laboratory accidents3 the possibility of contamination by consumption of contaminated game meat4 and sexual intercourse5 be ignored as well.
Eight million people are infected with T. cruzi worldwide, mainly in Latin America, causing disabilities and more than 10, 000 deaths per year6. In addition, CD has been increasingly detected in non-endemic countries because of human migration6.
After more than a hundred years of discovery, trypanosomiasis remains a social and public health problem in Latin America and is considered as an "invisible giant," mainly because of the latency period that the disease can present and because it is difficult to treat during the chronic phase, causing serious injuries to vital organs7. It is also considered a neglected tropical disease as only a few investments were made to study this condition and produce the necessary drugs7,8, in addition to affecting the poorest population8.
In 2016, Brazil reported a DALY rate (indicator of days of life lost or poorly lived) of 64.7% due to CD, noting that the regions, which previously recorded the lowest number of DALYs, had an increase between 1990 and 2016, including the northern region of the country, where oral transmission CD is prevalent9.
In the Brazilian Amazon, increasing outbreaks of the disease have been reported in the last 10 years10, mainly due to the consumption of contaminated food, generating concern among public health managers. It is necessary to understand the epidemiology of this disease in the region; hence, this study aimed to describe the epidemiological panorama of CD in the Western Brazilian Amazon from 2007 to 2018.
METHODS
Study Design
This ecological study was conducted to examine the confirmed cases of acute CD in Western Amazonia.
Study Location and Period
The data extracted were from the four states of Western Amazonia: Acre (AC), Amazonas (AM), Roraima (RR) and Rondônia (RO), as shown in figure 1.
Study Population and Eligibility Criteria
Positive cases of acute CD, reported in the period from 2007 to 2018, were included in the study. The following variables were analyzed: gender, age group, form of contagion (oral, vector, accidental, and others), seasonality, and area (rural, urban, or peri-urban). By contrast, cases reported outside the survey period were excluded.
Data Collection
In this study, we collected the secondary data from the Single Health System Notification Information System (SINAN)11 of the Department of Informatics of the Single Health System and the Brazilian Institute of Geography and Statistics (IBGE)12. These data were used to determine the population number and frequency of infection, and to characterize the epidemiological profile of people infected with T. cruzi.
Data Analysis
Frequency rates were calculated (number of cases/population of the locality in the year surveyed per 100,000 inhabitants).
Ethical and Legal Aspects of the Research
Approval from the Ethics Committee was not required because secondary data were used.
RESULTS
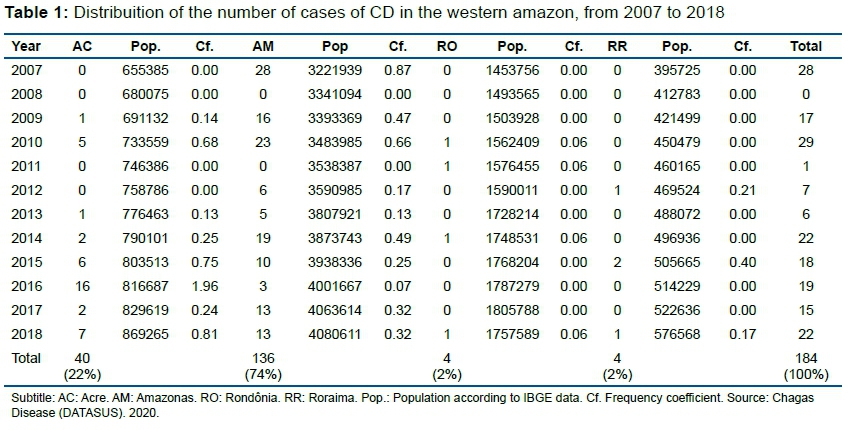
In 2007 to 2018, 184 confirmed cases of acute CD were reported in Western Amazonia. The cases registered in the states of Amazonas and Acre together represent more than 90% of the notifications in the period, in the entire region included in the study (table 1).
A higher incidence of the disease was observed in men and in those aged 20-39 years. Approximately 56% of the notifications reported in this study were due to oral infection; the months of December and April had the highest number of reported cases. A higher number of people with CD was also observed to be living in rural areas (table 2).
DISCUSSION
Studies based on the frequency in which trypanosomiasis occurs at the regional level, detecting possible endemic areas, together with some sociodemographic factors, can serve as a basis to establish important epidemiological parameters, especially in states where CD is not endemic.
In this study, CD was predominant in men, and this may be related to the participant's work activities, such as extraction of açaí and piassava; these activities increases the men's exposure to the vector and consequently to CD. In similar surveys conducted in the states of Pará13 and Acre14, the highest frequency was also reported in men; this finding is not consistent with the results of another survey conducted in Amazonas, which reported that women had higher exposure to CD15. This higher occurrence in men may be related to their work activities, such as extraction of natural products, which increases the possibility of contact with the disease vector.
The age group that is most frequently affected in this study corroborates with that in other studies. This finding indicates that the risk of CD infection increases during the most productive age of the individual and in those living in rural areas; during this period, the individual's most common activities were plant extraction and farming15,16.
Results of other studies conducted in the same geographical region corroborate with those of our study, which reported a higher rate of infection in rural areas. This finding is because of the populations' higher consumption of açaí and the processing of this fruit without following proper sanitary procedures, thus increasing the possibility of outbreaks by oral transmission10,14.
Although CD in the Western Amazon region is still more prevalent in the rural areas, data from the World Health Organization6 showed that changes in the epidemiological profile of the disease due to rural exodus, deforestation, and urbanization have made CD a more urban and peri-urban phenomenon6; this has been observed in this study, where an increase in notifications has been noted in the peri-urban areas. In a recent study, an increase in CD in the peri-urban area was observed in Venezuela17. Souza-Júnior et al. (2017) also observed a higher incidence of CD in an urban area in the municipality of Barcarena, Pará.
Increase in CD outbreaks due to oral transmission in the Amazon region, possibly caused by the consumption of agro-extractivist forest products without proper sanitary regulation, was pointed out as the primary reason for changing the traditional view of the Amazon as a region free of CD and acute CD18 Oral transmission is considered as a neglected transmission route19 consumption of açaí (Euterpe oleraceae) being indicated as the primary food involved in the transmission of this disease10.
Transmission through vectors found in the study population's residences has not yet been registered in the region of Western Brazilian Amazon, although transmission by vectors that opportunely invade the houses20. However, these vector-borne transmission records made available by SINAN suggest the need for an in-depth epidemiological investigation, since 31% of transmissions were registered vector-borne in a region in Roraima where there is only evidence of triatomine domiciliation21.
Although vector-borne transmissions by wild triatomine can possibly occur, either through direct contact with forest areas or by intrusion of these insects in an individual's home, it is possible that the data reported as vector-borne transmission have not been adequately investigated to prove this form of transmission22.
Another important factor reported in this study is that CD was more prevalent during December and April, and this finding is similar to that in another study conducted in the state of Amazonas in a different period15. Meanwhile, Oliveira et al. (2018) observed greater seasonality of CD in the month of June, possibly because the outbreaks that occurred in the region during that period were due to an oral transmission. Souza- Júnior et al. (2017) observed a higher occurrence of CD during the months with higher temperatures, suggesting that this condition favors deforestation and burning.
Hence, further studies should be conducted to evaluate the factors that interfere with the seasonality of the disease; however, the seasonal difference between the states may also be attributed to the wide harvest period of açaí in the Amazon region. This period of fruit productivity coincides with the period of greater rainfall, from December to May23. Outbreaks occurring outside this period and by oral transmission can be explained mainly by the storage of the crop products, which are available for consumption even beyond the harvest season.
Thus, in Western Amazon, T. cruzi infection may occur throughout the year, mainly because of the large consumption of açaí and fruits of other palm trees. The risk of oral transmission through ingestion of products from palm trees was confirmed in a previous study, in which the T. cruzi DNA was detected in 10% of the açaí pulp sold in Pará and Rio de Janeiro24. This fact brings a warning and reinforces the hypothesis on the year-round risk of T. cruzi infection, active in the fat of açaí pulps that are frozen for prolonged periods10; thus, the products stored during the harvest may transmit the parasite even if they are consumed beyond this period.
The state of Amazonas, with the highest number of CD notifications in Western Amazonia, has already been reported in other epidemiological studies that also point to the high prevalence of acute infection and attribute the first autochthonous cases of the disease to the extraction of piassava15,25. However, if the frequency coefficients are considered, Acre can also be considered as a state of great epidemiological importance; it has the highest number of people affected by the disease compared with Amazonas.
Acre had a considerable increase in disease notifications from 2016 onward. This fact was confirmed by Oliveira et al. (2018), who observed an increase of 316.7% in cases of CD compared with that in the previous year, which was the period in which the outbreaks that occurred in the state were due to oral transmission. Data provided by the State Epidemiological Surveillance in 2019 point to another outbreak of CD involving 15 people in the state, which further increases this coefficient.
The states of Acre and Amazonas presented frequency coefficients above the national coefficient; the data from the Ministry of Health showed that the average annual incidence of CD throughout the country is 0.061 cases per 100,000 inhabitants, with the northern region responsible for 91% of the notifications26. However, these coefficients were lower than those reported in Pará, with the highest prevalence of CD in the country and located in the northern region11.
Rondônia, with five cases of acute CD, corresponds to 2% of the total notifications presented in this study.
The low prevalence of CD in Rondônia may be related to the economic activities, according to the IBGE data, farming activities were more common in this state than extractive activities. Moreover, Rondônia is one of the smallest producers of açaí in Western Amazonia and has the largest cattle herd in the region12.
Carvalho et al.27 observed a low invasion of triatomine in homes and a pattern of rural properties in Monte Negro, Rondônia, which do not favor the domiciliation of triatomine. In this municipality, the houses are mostly made of concrete and roofs are made of tiles, including henhouses and other deposits; in the same study, a large amount of triatomine were found in Orbygnia speciosa (Babaçu) palm trees, which mostly grow in pasture areas.
Other investigations have already reported the presence of T. cruzi-infected vectors in areas near human habitats and the infestation of these vectors in babassu. The development of this palm specie in that state suggests the presence of triatomine28,29.
Research regarding the vectors in the state of Rondônia made possible the discovery of a new triatomine species (Rhodnius montenegrensis)30 with reports of natural infection by T. cruzi and vector capacity31, further increasing the risk of CD transmission. There were also data on the state of individuals infected with T. cruzi from endemic areas of the country, suggesting non-autochthonous infections28; moreover, the presence of vectors and reservoirs may enable the establishment of a long-term domestic protozoan cycle, despite the low number of households infested with triatomine.
The destruction of natural ecotopes with agricultural expansion and the presence of triatomine, especially in areas close to human habitats, combined with the high rates of natural infection of these insects make the state of Rondônia an endemic area of CD, observing the presence of all links in the chain of transmission of the disease in the region28.
Another state of Western Amazonia with a lower frequency of CD was Roraima. In one study, it states that Roraima is not considered as an endemic area for the disease32; however, some factors of epidemiological importance deserve to be observed, such as the report of colonization of a Triatoma maculata species in an urban home in the state capital21 and the identification of new vector species in the state33 besides the intense migratory relationship of the state with other endemic areas of the country and the neighboring country, Venezuela17.
An epidemiological study conducted in agricultural settlements in the state of Roraima detected the presence of triatomine near human habitats and animal shelters, demonstrating the potential for domiciliation of existing populations21 and consequently the establishment of domestic and peridomestic cycles of the disease. As a result, autochthonous transmission of CD in the state34.
Roraima also received immigrants from Venezuela as of 2014; with this, there was a resurgence of previously eradicated diseases35 and an increase in the number of cases of other infectious diseases such as malaria36. This situation is worrisome, since the study reported the abandonment of the Chagas control program in the neighboring country and stated that it remains unclear whether blood banks are being traced17. Venezuela reported an increase in the transmission of CD, and the severe shortage of medications, due to the crisis faced by the country, has forced patients to seek medical care and treatment in neighboring countries17 including Brazil, particularly in the state of Roraima.
The lack of vaccine for CD and low investment in drug production37 indicate that the focus of management is still vector control and interference in the disease cycle, justifying the need for constant surveillance of epidemiological factors favorable to the emergence of infections.
These data are important, since these states are located in the same geographic region and share several cultural aspects, besides migration. The transmission dynamics in the Amazon as a whole follows a similar pattern, demonstrating that the entire region is exposed to CD.
CONCLUSION
The epidemiological picture of CD in Western Amazonia from 2007 to 2018 corresponded to the notification of a total of 184 cases of the disease, with 2010 having the highest number of records. The epidemiological survey identified the highest occurrence in men, individuals aged 20 to 39 years, and those living in rural areas. The main route of transmission is oral, and CD commonly occurs in the months of April and December, coinciding with the rainy periods and therefore the harvest of fruits like açaí.
The description of the epidemiological panorama of CD is important to perceive the changes that have occurred over time and to identify the determining factors in the health-disease process. In addition, an efficient data recording system is required to ensure effective surveillance and to monitor the transmission dynamics in different environments in the Amazon region. The adoption of compulsory notification of CD in the chronic phase starting this year will allow a more real dimensioning of this endemic, since, in addition to removing many affected by the disease from invisibility, it will improve the data system for the implementation of more efficient means of disease prevention and access to treatment by the affected populations, leading to a more detailed epidemiological panorama of CD in the future.
Author Contributions
Conceptualization, F. P. M.; A. C. J.; M. H. S. M.; D. U. O. M. and P. S. B.; Methodology, F. P. M.; A. C. J.; M. H. S. M.; N. F. B.; G. V. S. C.; M. A. L. R.; L. M. A. C.; D. U. O. M. and P. S. B.; data collection, F.P.M.; A. C. J.; N. F. B.; G. V. S. C.; M. A. L. R.; L. M. A. C.; D. U. O. M. and P. S. B.; data analysis, , F.P.M.; A. C. J.; N. F. B.; G. V. S. C.; M. A. L. R.; L. M. A. C.; D. U. O. M. and P. S. B.; formal analysis, , F.P.M.; A. C. J.; M. A. L. R.; L. M. A. C.; D. U. O. M. and P. S. B.; investigation, F.P.M.; L. M. A. C.; D. U. O. M. and P. S. B.; writing - preparation of the original draft, F. P. M.; A. C. J.; M. H. S. M.; N. F. B.; G. V. S. C.; M. A. L. R.; J. E. M. T.; L. M. A. C.; D. U. O. M. and P. S. B. writing - proofreading and editing, F. P. M.; A. C. J.; M. H. S. M.; N. F. B.; G. V. S. C.; M. A. L. R.; J. E. M. T.; L. M. A. C.; D. U. O. M. and P. S. B. financing acquisition, J. E. M. T.; L. M. A. C.; D. U. O. M. and P. S. B. All authors read and agreed with the published version of the manuscript.
Acknowledgments
We thank Acre State Secretariat of Health (SESACRE), Acre - Brazil, the Federal University of Acre (UFAC), Acre - Brazil and the Santo ABC University Center (FMABC) Santo André, São Paulo - Brazil, for the opportunity to develop Masters, Doctors and Researchers training in health, through Agreement 007/2015 - SESACRE/UFAC/FMABC) and all researchers, undergraduate, masters and doctorates students of the Laboratory of Study Design and Scientific Writing of the ABC University Center (FMABC) and thus made it possible to develop research and science in the Western Amazon, Brazil.
Conflicts of Interest
There are no conflicts of interest.
REFERENCES
1.Chagas C. Nova tripanozomiaze humana: estudos sobre a morfolojia e o ciclo evolutivo do Schizotrypanum cruzi n. gen., n. sp., ajente etiolojico de nova entidade morbida do homem. Mem Inst Oswaldo Cruz. 1909; 1(2): 159-218. DOI: 10.1590/S0074-02761909000200008 [ Links ]
2.Galvão C. Vetores da doença de Chagas no Brasil. Curitiba: Sociedade Brasileira de Zoologia, 2014; p.26-31. DOI: https://doi.org/10.7476/9788598203096 [ Links ]
3.Coura JR. The main sceneries of Chagas disease transmission. The vectors, blood and oral transmissions - A comprehensive review. Mem Inst Oswaldo Cruz. 2014; 110(3): 277-82. DOI: 10.1590/0074-0276140362 [ Links ]
4.Sangenis LHC, Nielebock MAP, Santos C da S, Silva MCC da, Bento GMR. Transmissão da doença de Chagas por consumo de carne de caça: revisão sistemática. Rev bras epidemiol. 2016; 19(4): 803-11. DOI: 10.1590/1980-5497201600040010 [ Links ]
5.Araujo PF, Almeida AB, Pimentel CF, Silva AR, Sousa A, Valente SA, et al. Sexual transmission of American trypanosomiasis in humans: a new potential pandemic route for Chagas parasites. Mem Inst Oswaldo Cruz. 2017; 112(6): 437-46. DOI: 10.1590/0074-02760160538 [ Links ]
6.World Health Organization (WHO). Chagas disease (American trypanosomiasis) [cited 2019 nov 10]. Available from: https://www.who.int/chagas/epidemiology/en/ [ Links ]
7.Benatti RD, Oliveira GH, Bacal F. Heart Transplantation for Chagas Cardiomyopathy. J Heart Lung Transplant. 2017; 36(6): 597-603. DOI: 10.1016/j.healun.2017.02.006 [ Links ]
8.Gosling AF, Gelape CL. Chagas Disease and the Kissing Bug: An Invisible Giant. J Cardiothorac Vasc Anesth. 2019; 33(8): 2349-50. DOI: 10.1053/j.jvca.2019.01.014 [ Links ]
9.Martins-Melo FR, Carneiro M, Ribeiro ALP, Bezerra JMT, Werneck GL. Burden of Chagas disease in Brazil, 1990-2016: findings from the Global Burden of Disease Study 2016. Int J Parasitol. 2019; 49(3-4): 301-10. DOI: 10.1016/j.ijpara.2018.11.008 [ Links ]
10.Santana RAG, Guerra MGVB, Sousa DR, Couceiro K, Ortiz JV, Oliveira M, et al. Oral Transmission of Trypanosoma cruzi, Brazilian Amazon. Emerg Infect Dis. 2019; 25(1): 132-5. DOI: 10.3201/eid2501.180646 [ Links ]
11.DATASUS - Tecnologia da Informação do SUS (BR). Doenças de chagas Aguda, Brasil [cited 2020 apr 20]. Available from:http://www2.datasus.gov.br/DATASUS/index.php?area=0203&id=29890013&VObj=http:// tabnet.datasus.gov.br/cgi/deftohtm.exe?sinannet/cnv/chagas [ Links ]
12.Instituto Brasileiro de Geografia e Estatística (IBGE). IBGE Cidades- Pesquisa. [cited 2020 marc 12]. Available from: https://cidades.ibge.gov.br/pesquisas [ Links ]
13.Santos WS, Alves VR, Pontes AN, Diseases F. A doença de chagas no município de Abaetetuba, Pará, Brasil. Rev Bras Multidiscip. 2020; 23(1): 62-70. DOI: https://doi.org/10.25061/2527-2675/ReBraM/2020.v23i1.699 [ Links ]
14.Oliveira GF de, Ribeiro MAL, Castro GV de S, Menezes ALR, Lima RA, Silva RPM, et al. Retrospective study of the epidemiological overview of the transmission of Chagas disease in the State of Acre, South-Western Amazonia, from 2009 to 2016. J Hum Growth Dev. 2018; 28(3): 329-36. DOI: https://doi.org/10.7322/jhgd.152187 [ Links ]
15.Menezes ALR, Oliveira GF de, Ribeiro MAL, Castro GV de S, Lima RA, Meneguetti DU de O. Epidemiological overview of chagas disease in the state of Amazonas, from 2004 to 2014. Revista de Epidemiologia e Controle de Infecção. 2019; 9(2). DOI: 10.17058/reci.v9i2.12127 [ Links ]
16.Sousa Júnior A da S, Palácios VR da CM, Miranda C do S, Costa RJF da, Catete CP, Chagasteles EJ, et al. Análise espaço-temporal da doença de Chagas e seus fatores de risco ambientais e demográficos no município de Barcarena, Pará, Brasil. Rev bras epidemiol. 2017; 20(4): 742-55. DOI: 10.1590/1980-5497201700040015 [ Links ]
17.Grillet ME, Hernández-Villena JV, Llewellyn MS, Paniz-Mondolfi AE, Tami A, Vincenti-Gonzalez MF, et al. Venezuela's humanitarian crisis, resurgence of vector-borne diseases, and implications for spillover in the region. The Lancet Infectious Diseases. 2019; 19(5): e149-61. DOI: 10.1016/S1473-3099(18)30757-6 [ Links ]
18.Aguilar HM, Abad-Franch F, Dias JCP, Junqueira ACV, Coura JR. Chagas disease in the Amazon Region. Mem Inst Oswaldo Cruz. 2007; 102(suppl 1): 47-56. DOI: 10.1590/S0074-02762007005000098 [ Links ]
19.Robertson LJ, Devleesschauwer B, Noya BA de, González ON, Torgerson PR. Trypanosoma cruzi: Time for International Recognition as a Foodborne Parasite. PLOS Neglected Tropical Diseases. 2016; 10(6): e0004656. DOI: 10.1371/journal.pntd.0004656 [ Links ]
20.Abad-Franch F, Monteiro FA. Biogeography and evolution of Amazonian triatomines (Heteroptera: Reduviidae): implications for Chagas disease surveillance in humid forest ecoregions. Mem Inst Oswaldo Cruz. 2007; 102(suppl 1): 57-70. DOI: 10.1590/S0074-02762007005000108 [ Links ]
21.Ricardo-Silva A, Gonçalves TCM, Luitgards-Moura JF, Lopes CM, Silva SP da, Bastos AQ, et al. Triatoma maculata colonises urban domicilies in Boa Vista, Roraima, Brazil. Mem Inst Oswaldo Cruz. 2016; 111(11): 703-6. DOI: 10.1590/0074-02760160026 [ Links ]
22.Ribeiro Castro MAL, de Souza Castro GV, de Souza JL, de Souza CR, Ramos LJ, de Oliveira J, et al. First report of Panstrongylus megistus (Hemiptera, Reduviidae, Triatominae) in the State of Acre and Rondônia, Amazon, Brazil. Acta Tropica. 2018; 182: 158-60. DOI: 10.1016/j.actatropica.2018.02.032 [ Links ]
23.Soeiro da Silva Dias T, Barreiros de Souza E, Gonçalves Jardim MA, Oliveira Ponte de Souza PJ, Paulino da Rocha EJ, Nascimento Pinheiro A, et al. Estimativa climática sazonal da produtividade de açaí (Euterpe oleracea mart.) no Estado do Pará - cenários futuros. RBGF. 2019; 12(2): 517-33. DOI: 10.26848/rbgf.v12.2.p517-533 [ Links ]
24.Ferreira RTB, Cabral ML, Martins RS, Araujo PF, da Silva SA, Britto C, et al. Detection and genotyping of Trypanosoma cruzi from açai products commercialized in Rio de Janeiro and Pará, Brazil. Parasites Vectors. 2018; 11(1): 233. DOI: 10.1186/s13071-018-2699-6 [ Links ]
25.Barbosa M das GV, Ferreira JMBB, Arcanjo ARL, Santana RAG, Magalhães LKC, Magalhães LKC, et al. Chagas disease in the State of Amazonas: history, epidemiological evolution, risks of endemicity and future perspectives. Rev Soc Bras Med Trop. 2015; 48(suppl 1): 27-33. DOI:10.1590/0037-8682-0258-2013 [ Links ]
26.Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Boletim Epidemiológico. Chagas aguda no Brasil: série histórica de 2000 a 2013. Secr Vigilância em saúde [Internet]. 2015; 46(2358-9450): 1-9. Available from: http://portalsaude.saude.gov.br/images/pdf/2015/agosto/03/2014-020.pdf [ Links ]
27.Carvalho EOC de, Rosa JA da, Carvalho AA de, Chaves HCO, Souza EA de, Ostermayer AL, et al. Study on Chagas disease occurrence in the municipality of Monte Negro, State of Rondônia, Brazilian Amazon. Rev Soc Bras Med Trop. 2011; 44(6): 703-7. DOI: 10.1590/S0037-86822011000600010 [ Links ]
28.Massaro DC, Rezende DS, Camargo LMA. Estudo da fauna de triatomíneos e da ocorrência de doença de Chagas em Monte Negro, Rondônia, Brasil. Rev bras epidemiol. 2008; 11(2): 228-40. DOI: 10.1590/S1415-790X2008000200005 [ Links ]
29.Meneguetti DU de O, Trevisan O, Camargo LMA, Rosa RM. Natural infection of triatomines (Hemiptera: Reduviidae) by trypanosomatids in two different environments in the municipality of Ouro Preto do Oeste, State of Rondônia, Brazil. Rev Soc Bras Med Trop. 2012; 45(3): 395-8. DOI: 10.1590/S0037-86822012000300023 [ Links ]
30.Da Rosa JA, Rocha CS, Gardim S, Pinto MC, Mendonça VJ, Filho JCRF, et al. Description of Rhodnius montenegrensis n. sp. (Hemiptera: Reduviidae: Triatominae) from the state of Rondônia, Brazil. Zootaxa. 2012; 3478(1): 62-76. DOI: 10.11646/zootaxa.3478.1.8 [ Links ]
31.Bilheiro AB, da Rosa JA, de Oliveira J, Belintani T, Fontes G, Medeiros JF, et al. First Report of Natural Infection with Trypanosoma cruzi in Rhodnius montenegrensis (Hemiptera, Reduviidae, Triatominae) in Western Amazon, Brazil. Vector-Borne and Zoonotic Diseases. 2018; 18(11): 605-10. DOI: 10.1089/vbz.2018.2266 [ Links ]
32.Moura, J. F. L. Aspectos epidemiológicos da doença de chagas em áreas de colonização agrícola no estado de Roraima [thesis]. Rio de Janeiro: Instituto Oswaldo Cruz, Rio de Janeiro, 2001. [ Links ]
33.Gama Neto J de L, de Oliveira J, da Rosa JA, dos Santos FM, Macedo VA, Costa da Silva M. Two new records of Triatominae (Hemiptera: Reduviidae) from Roraima state, Brazil. RCHE. 2020; 46(2): 321-7. DOI: 10.35249/rche.46.2.20.23 [ Links ]
34.Luitgards-Moura JF, Borges-Pereira J, Costa J, Zauza PL, Rosa-Freitas MG. On the possibility of autochthonous Chagas disease in Roraima, Amazon region, Brazil, 2000-2001. Rev Inst Med trop S Paulo. 2005; 47(1): 45-54. DOI: 10.1590/S0036-46652005000100008 [ Links ]
35. Arruda-Barbosa L de, Sales AFG, Souza ILL de. Reflexos da imigração venezuelana na assistência em saúde no maior hospital de Roraima: análise qualitativa. Saude soc. 2020; 29(2): e190730. DOI: 10.1590/s0104-12902020190730 [ Links ]
36.Editoria, "Saúde e Migração: ensaio reflexivo da migração Venezuela em Roraima, por Tarcia Costa," in Revista Mundorama, 13/09/2017, https://mundorama.net/?p=23927 [ Links ]
37.Bezerra WS, Meneguetti DU de O, Camargo LMA. A BUSCA DE FÁRMACOS PARA TRATAMENTO DA TRIPANOSSOMÍASE AMERICANA: 103 ANOS DE NEGLIGÊNCIA. Saúde (Santa Maria). 2012; 38(1): 09-20. DOI: 10.5902/223658344813. [ Links ]
 Correspondence:
Correspondence:
dionatas@icbusp.org
Manuscript received: September 2020
Manuscript accepted: December 2020
Version of record online: March 2021


{kind=link}
{kind=link}
{kind=link}