










Servicios Personalizados
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.2 Santo André mayo/ago 2021
http://dx.doi.org/10.36311/jhgd.v31.12223
ORIGINAL ARTICLE
Relationship between motor-cognitive functions and hemodynamic response of individuals with chronic stroke during and after an acute bout of aerobic exercise
Samantha Helena do CarmoI; Laércio da Silva PaivaII; Fernando AdamiII; Francisco Naildo Cardoso LeitãoIII; Cleide Maria de Paula RebouçasIV; Vitor Engracia ValentiV; Rodrigo Daminello RaimundoVI
IDepartamento de Fisioterapia, Centro Universitário FMABC, Santo André, São Paulo, Brazil;
IILaboratório de Epidemiologia e Análise de Dados do Centro Universitário FMABC, Santo André, São Paulo, Brazil;
IIILaboratório Multidisciplinar de Estudos e Escrita Científica em Ciências da Saúde da Universidade Federal do Acre (UFAC), Rio Branco, Acre, Brazil;
IVLaboratório de Delineamento de Estudos e Escrita Científica- LABDEEC da UNINORTE, Rio Branco, Acre, Brasil. reboucas;
VCentro de Estudos do Sistema Nervoso Autônomo (CESNA), Departamento de Fonoaudiologia, Faculdade de Filosofia e Ciências, UNESP, Marília, São Paulo, Brazil;
VILaboratório de Delineamento e Escrita Científica do Centro Universitário FMABC, Santo André, São Paulo, Brazil
ABSTRACT
BACKGROUNG: Individuals post-stroke commonly presents functional and cardiorespiratory deficits besides a physical inactivity lifestyle in the chronic phase of disease. Considering this, there is a hypothesis that hemodynamic responses could be affected by motor, cognitive and cardiorespiratory deficits during the aerobic exercise. In order to identify functional conditions that can influence the aerobic performance of these individuals, correlations between functional variables and hemodynamic responses during and after the aerobic exercise were studied. As a secondary purpose, the ability of return to hemodynamic resting state were also analyzed
METHODS: In this experimental study, after being evaluated about their motor and cognitive function, balance and prognosis, forty participants underwent a 30-minute aerobic exercise session on a treadmill. Training heart rate, arterial blood pressure, oxygen pulse saturation, heart rate, and respiratory rate were measured before begin the exercise session, every five minutes during the exercise and five minutes after it
RESULTS: Cardiorespiratory parameters within normality limits in all phases of the exercise and the capacity of returning to the resting state were observed. Moderate inverse correlations were found between Berg Scale and oxygen pulse saturation (r =-0.401, p = 0.01), between MMSE and diastolic blood pressure (r = -0.406, p = 0.009), age and diastolic blood pressure (r = -0.435, p = 0.005) and between injury time and RR (r = -0.454, p = 0.003). Relationship between the lesion side and the 20 minutes phase of aerobic exercise was also observed (p = 0.042
CONCLUSION: Post- stroke individuals present moderate correlation between hemodynamic and respiratory responses during aerobic exercise and balance, muscle strength, injury time, age and side of lesion. They also have the capacity to return to their cardiorespiratory and cardiovascular resting state right after the activity besides their cardiorespiratory deficits
Keywords: stroke, aerobic exercise, heart rate, blood pressure, respiratory rate.
Authors summary
Why was this study done?
Considering the deficits that these individuals have in the motor and cardiorespiratory system and the lack of information about the influence that one capacity can exert on the other, the authors decided to assess whether there were correlations between the characteristics of the lesion, sociodemographic, anthropometric and functional characteristics of individuals with stroke and its hemodynamic response when submitted to aerobic training.
What did the researchers do and find?
After being evaluated for motor and cognitive functions, individual characteristics and brain damage, and anthropometric variables, forty participants underwent a 30-minute aerobic exercise session on a treadmill. and had their cardiorespiratory responses recorded. With these data, correlation measures were applied and showed that post-stroke individuals have a moderate correlation between cardiorespiratory responses during aerobic exercise and balance, muscle strength, injury time, age and side of the injury, in addition to the ability to return to the state. of rest soon after activity, despite their cardiorespiratory deficits.
What do these findings mean?
Through the results of this study, it is possible to observe that characteristics of brain injury, balance capacity, muscle strength and age are variables that influence the cardiorespiratory performance of these individuals during aerobic exercise. Thus, deficits in these abilities may indicate a worse performance during aerobic activity and should be considered by professionals in the rehabilitation process, as well as aiming to improve these abilities during therapy can promote better performance in this task.
INTRODUCTION
Stroke is the second largest cause of death worldwide, reaching about 6.2 million deaths/year and only standing behind of cardiovascular disease. Every year, in all world, 15 million people are affected by stroke, of these individuals, 5 million are permanently physically incapacitated, according to WHO1,2. In Brazil, is the major cause of motor incapacity in adults3.
The consequences of stroke in the brain tissue are severe, lead to neurological deficits and, as a result, to the sensory, motor and cognitive impairment, and may vary according to the affected brain area and degree of complexity4,5. Cardiovascular and respiratory deficits are very common and may be serious in individuals post-stroke6-8, moreover, people one year post-stroke seems to remain not being active enough to improve or maintain their physical health9 while this physical inactivity can increase the risk of recurrent stroke and cardiovascular events10.
Considering the deficits that this individual has in both motor and cardiorespiratory system and the lack of information about the influence that one capacity could be on each other, the research questions were: Is there a correlation between prognosis, balance, motor, cognitive functions and the cardiorespiratory performance during and after aerobic exercise? Can chronic individuals post-stroke be able to perform aerobic exercise and return to their resting cardiorespiratory parameters in a proper time despite the deficits and physical inactivity lifestyle that they commonly present?
METHODS
Design
Experimental study with one time intervention.
Participants, therapists, centers
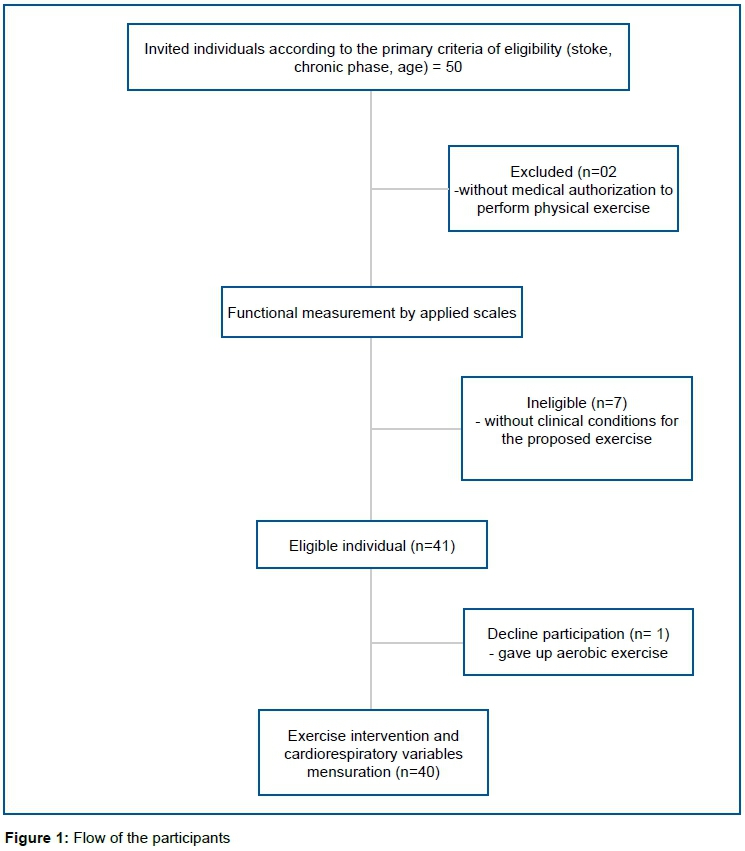
Forty individuals of both sexes, aged 40 to 65 years with stroke, both hemorrhagic and ischemic types, confirmed by image exam and medical report, injury time over one year and adequate score on the motor and cognitive applied scales were included in the study. Individuals without gait conditions, not included the ones due to stroke, or clinical conditions for the proposed exercises and tests, association of other neurological diseases, weight above 150kg, and without medical authorization to perform physical exercise were excluded of the survey.
The number of participants was determined by convenience sample, the participants were recruited and underwent evaluation into Faculdades Metropolitanas Unidas (São Paulo, Brazil) and the methods used were applied by the first and senior authors. The study was approved by the Ethics Committee in Research of the School of Medicine of ABC (Protocol No. 33353) and all volunteers signed an informed consent form.
Intervention
Outcomes measures
For the measurement of the anthropometric variables weight and height, the participants were weighed without shoes, and with the minimum of possible clothes, in electronic scale, with capacity of up to 150kg and subdivisions of up to 10g. For the measure of height, participants pressed the heels, calves, buttocks and shoulders to the wall, positioning the head according to the Frankfurt plan. A stadiometer fixed to the wall was used, with subdivisions in centimeters and millimeters. Based on these data, the Body Mass Index (BMI) was measured by weight (kg)/height (m), and data such as time, type and brain injury side lesion, the latter were collected with a medical report.
Primary outcomes
For functional conditions characterization of these individuals, four scales were applied: Mini-Mental State Examination (MMSE)11, Berg scale12, Fugl Meyer13 and Orpington Scale14.
Mini-Mental State Examination
The MMSE is a validated instrument to evaluate the individual's cognitive capacity. It is composed of 7 specific cognitive functions categories: time orientation, space orientation, word register, attention and calculation, memory of words, language and visual constructive capacity. The score range from 0 to 30 points.
Berg Scale
The participants were analyzed for their balance through the Berg Scale, an also validated scale composed by 14 commands that evaluate the static and dynamic balance, according to the proposed activities, and measure the performance of the individual tested on a scale of 0 to 4 points for each one of the 14 commands. The maximum score is 56 points, the results below 45 points are considered as predictive of fall, being this the necessary score to consider adequate the balance ability of the individual.
Fugl Meyer
Physical performance will be qualified through the Fugl-Meyer scale. This scale evaluates five dimensions of impairment for motor control aspects: bone articulation range of motion, pain, motor impairment of upper and lower limbs and balance. The data are scored from 0 to 3 points for each item, with a total 226 points score, and considering motor impairment at 100 points as result.
Orpington Scale
In order to evaluate the incapacities due to the cerebrovascular event, this scale evaluates activities of daily living through motor deficits in the upper limb, proprioception, balance and cognition. Its score ranges from 1.6 to 6.8; characterizing the vascular event in mild, moderate or severe.
Secondary outcomes
Systolic (SBP) and diastolic blood pressure (DBP), heart rate (HR), respiratory rate (RR) and oxygen pulse saturation (SAT) measurements were initially collected. The SAT data were collected by visualizing the Onim-Indumeda model 9500 portable finger oximeter Nonin, SBP and DBP data were obtained by a single measurement indirectly verified by means of a WelchAllyn brand sphygmomanometer positioned on the left arm of the subject and Littmann-3M Classic II stethoscope on the median region of the antecubital fossa. For RR a timer was used to count how many thoracic incursions the individual could make in one minute. The heart rate was recorded by the Polar brand S810i cardiofrequencymeter.
After obtaining the resting heart rate (RHR) and maximum heart rate (HRmax) by age, through the formula (HRmax = 220 - age), the training heart rate (HRt) was calculated given by the Karvonen formula = RHR (SD (HRmax - RHR) x% training). The percentage of training (% training) stipulated was 50 and 70%, as recommended in American Heart Association's guideline for physical activity in stroke survivors15.
All the measurements were collected by one single examiner with over 10 years of experience.
Exercise protocol
Having calculated training heart rate, the participants were instructed to walk on a treadmill RT250pro of the Movement brand (treadmill model containing anterior and lateral armrest) for aerobic exercise. During the session, support of the arms on the treadmill was allowed, as the individual felt safer.
The aerobic exercise session had a total duration of 30 minutes. In the first 5 minutes a warm-up was played, then, the individuals were instructed to perform 25 minutes of exercise reaching 70% of HRt, considered the peak of exercise. For this, the speeds of treadmill were constantly changed during the experiment to reach the FR training Five minutes after the end of the exercise was considered the recovery time. At the resting state, considered the initial phase (before begin the session), every 5 minutes of the exercise and 5 minutes after it, at the recovery phase, the measurements SBP, DBP, HR, RR and SAT were collected.
This aerobic session occurred around 01h30 and 3h30 p.m. and all the participants were instructed to abstain from caffeine for 8 hours prior, food (2 hours prior) and vigorous exercise prior to testing.
Data analysis
Qualitative variables were presented in absolute frequency and relative frequency. The quantitative variables were presented by mean and median measures, standard deviation and 25th and 75th percentiles measures and respective 95% confidence intervals (95% CI), according to the Shapiro-Wilk normality test.
To analyze the moments of the hemodynamic parameters of post-stroke individuals submitted to aerobic training was performed by linear regression and extracted: the angular coefficient (β), significance (p), predictive capacity of the model (r2 and r2-adjusted). The dependent variables was time (exercise time in minutes) and the independent variables were heart rate, oxygen saturation, systolic blood pressure, mean blood pressure and respiratory rate. The variables that did not present normal distribution were normalized by the criterion suggested by the statistical program: square, cubic, square root, 1/square, 1/cubic, log and inverse.
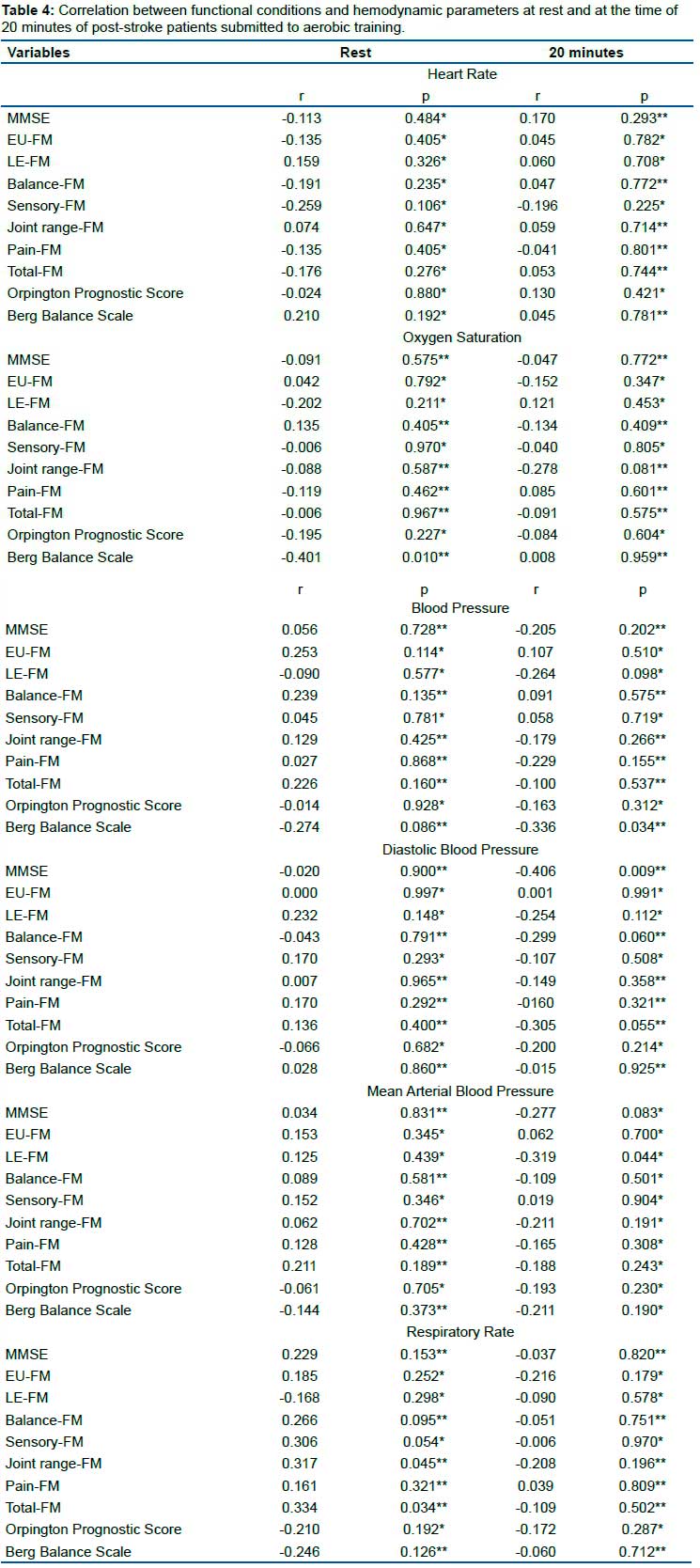
The Pearson and Spearman correlation test was used to correlate the variables related to functional conditions and hemodynamic parameters at rest and at the time of 20 minutes.
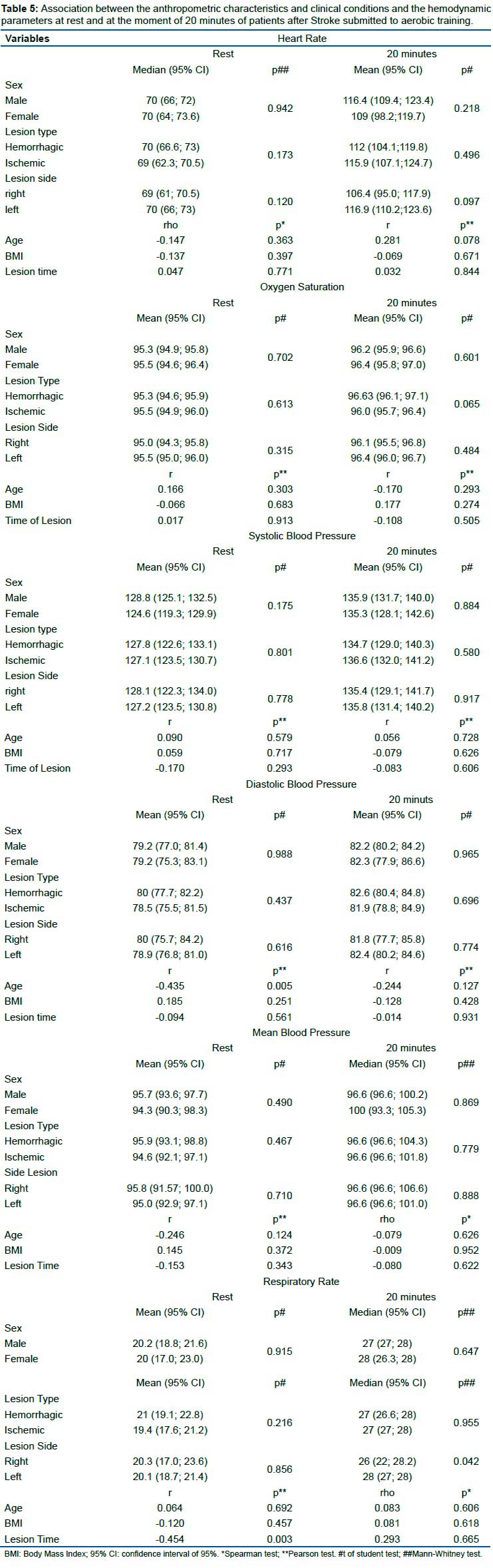
In order to correlate and to associate the anthropometric characteristics and clinical conditions with the hemodynamic parameters at rest and at the moment of 20, the Pearson and Spearman correlation test, the student t test and the Mann-Whitney test were used.
Correlations were classified as null (r = 0 to 0.03), weak (r = 0.03 to 0.35), moderate (r = 0.35 to 0.65), strong (r = 0.65 at 0.95), very strong (r = 0.95 to 0.99) and perfect (r = 1), and direct and indirect (positive and negative, respectively).
The confidence level considered was 95% and the statistical program used was the Data Analysis and Statistical Software for Professionals (Stata) version 11.0®.
Source of support
This study received financial support from the Foundation for Amparo and Research of the State of São Paulo - FAPESP (Process 2016 / 11867-3).
Role of the Funding Source
The funders played no role in the design, conduct, or reporting of this study.
RESULTS
Flow of participants, therapists, centers through the study
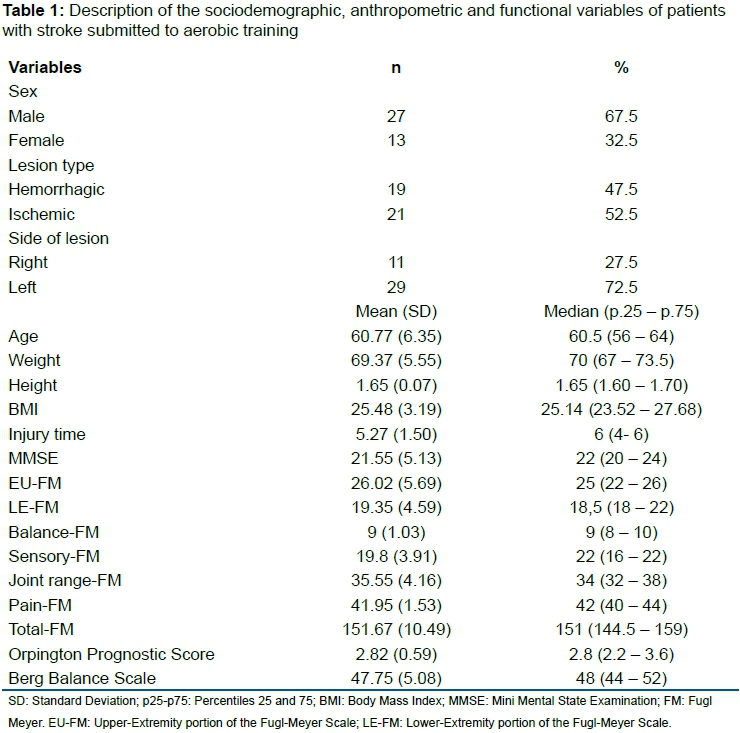
Figure 1 presents the flow of participants through the study. Anthropometrics and sociodemographic characteristics of the participants are summarized in table 1. The sample was composed by 27 (67,5%) male individuals, 21 (52,5%) of ischemic lesion type and 29 (72,5%) had lesion on the left side.
Hemodynamic response and breathing frequency behavior during aerobic exercise
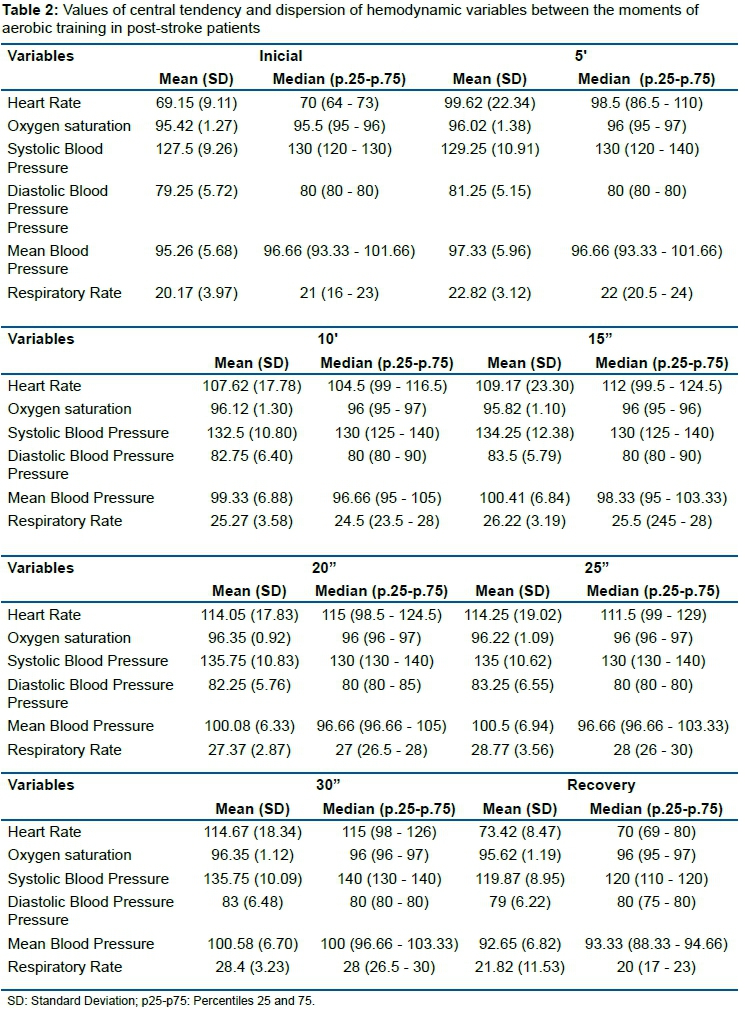
Hemodynamic variables presented during the aerobic exercise was HR 69.15 bpm (SD 9.11) at the initial phase, reaching 114.25bpm (SD 19.02) at the peak of exercise, and returning to 73.42bpm (SD 8.47) at the end of the it. In relation to SAT, its onset was 95.42% (SD 1.27), reached 96.22% (SD 1.09) and returned to 95.62% (SD 1.19). The SBP measure was 127.5mmHg (SD 9.26) in the initial phase, reached 135.0mmHg (SD 10.62) and decreased to 119.87mmHg (SD 8.95). The DBP, initiated at 79.25mmHg (SD 5.72), reached 83.25mmHg (SD 6.55) and decreased to 79.00mmHg (SD 6.22). The MBP (mean blood pressure) was 95.26mmHg (SD 5.68) initially for 100.50mmHg (SD 6.94) and 92.65mmHg (SD 6.82). Finally, the RR of these individuals started at 20.17rpm (SD 3.97) went to 28.77rpm (SD 3.56) at 25 minutes of exercise and reached 21.82rpm (SD 11.53) at recovery. These data are described and detailed in table 2.
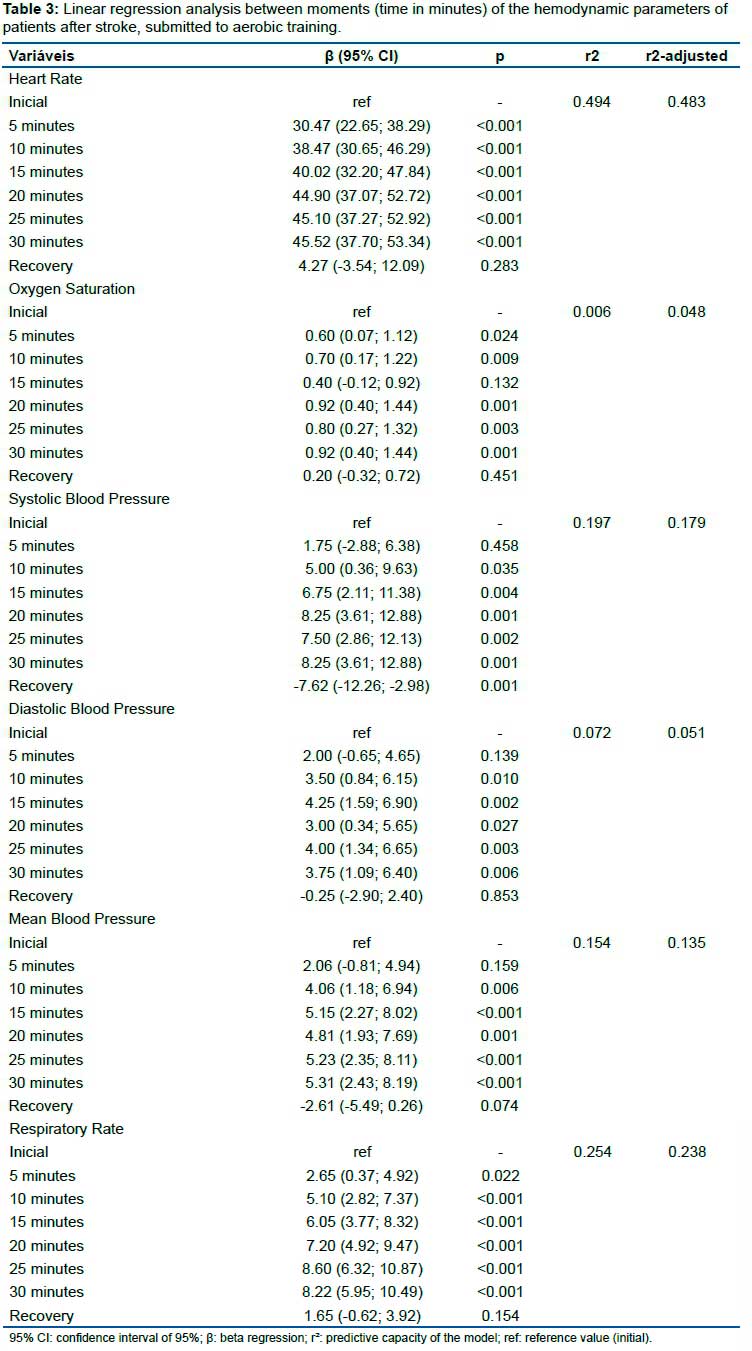
The results presented in table 3 demonstrate the relation of time in function of hemodynamic parameters and their influence on them through a linear regression analysis. It can be observed that for the hemodynamic parameters (heart rate, oxygen saturation, systolic blood pressure, mean blood pressure and respiratory rate) there was an increase in the parameters as the exercise time increased (time in minutes), except for the recovery time.
There are no statistically significant differences between the initial and recovery phases. Between the aerobic exercise time, which is subdivided in measurements collected each 5 minutes, to the final 30 minutes, statistically significant differences were found for each phases, except for the phases and parameters mentioned below: between the 15 minutes phase versus initial time there were no significant changes to the SAT; between the 5 minutes phase versus initial time also no significant changes were found for SBP, DBP and MBP. Among the variables, we found weak correlations for SAT, SBP, DBP, MBP, RR and time; and moderate for HR and time (table 3). Correlations between variables
Regarding the functional conditions and the hemodynamic parameters, whose data are described in table 4, we found a moderate inverse correlation (r = -0.401, p = 0.01) for the Berg Scale as a function of SAT; weak inverse correlation (r = -0.036, p = 0.03) for Berg Scale as a function of SBP; moderate inverse correlation (r = -0.406, p = 0.009) for MMSE as a function of DBP; weak inverse correlation (r = -0.319, p = 0.044) for LE-FM as a function of MBP; (r = 0,317, p = 0.045) for FM ROM as a function of RR and direct correlation (r = 0.334, p = 0.034) for Total FM as a function of RR.
Association between the clinical and anthropometric characteristics and the hemodynamic parameters are described in Table 5. We found statistical significance for moderate inverse correlation (r = -0.435, p = 0.005) between age and DBP for moderate inverse correlation (r = -0.454 , p = 0.003) between injury time and RR. Relationships between the lesion side and the 20 minute phase of aerobic exercise were also observed (p = 0.042).
DISCUSSION
It is well established that low levels of cardiorespiratory fitness are associated with a high risk of developing cardiovascular disease, mortality due to various causes, and even practicing exercise can prevent stroke itself.8,16.
There are several coherent and well-developed studies that prove that implement cardiorespiratory training is essential for this group17-21. However, it is also known that, after experiencing stroke, cardiovascular and cardiorespiratory deficits are commonly present in the health condition of these individuals5-8, added to this, Baert et al.9 carried out a study that indicates that individuals in chronic phase of stroke can be physically active, but not enough to increase or maintain their physical health. Considering this deficits that this individuals has in both motor and cardiorespiratory system, their inactivity and the lack of information about the influence that one capacity could be on each other, the researchers were instigated to investigate the correlation between prognosis, balance, motor, cognitive functions and the cardiorespiratory performance during and after aerobic exercise and the ability to perform aerobic exercise and return to their resting cardiorespiratory parameters in a proper time.
Primary aim of this study was to explore the correlations between the cited parameters and the functional conditions measures obtained through the applied scales and significant results were also found.
For balance ability, according to our data, a moderate inverse correlation was found, indicating that as lower is this capacity, the higher is the SAT percentage (r = -0.401, p = 0.01) and weak inverse correlation, also indicating that when the lower is the capacity of balance, the higher will be the SBP at 20 minutes of exercise (r = - 0.336, p = 0.03), which could instigate the question if improvements in balance could also provide a decrease in blood pressure levels during the exercise. Acar et al.22 and Abate et al.23 did not found relationship between hypertension and postural balance in elderly however they were not submitted to aerobic exercise and had no brain tissue damage.
In addition, moderate inverse correlation between cognition and DBP at 20 minutes of exercise was found, showing that as lower the cognitive ability of these individuals, as higher the DBP values at this stage of the training (r= -0.406, p=0.00). Forte et al.24, in their systematic review, identified that higher blood pressure is associated with a higher risk of cognitive decline, however the study was conducted in people without dementia or stroke. Likewise, a weak inverse correlation was also observed for LE-FM in relation to MBP, indicating higher values of this variable at 20 minutes of training for individuals who present lower muscle strength in these members, which could also indicate that muscle strengthening may be a protective factor for maintain blood pressure in adequate levels during aerobic exercise.
There were also direct weak correlations for range of motion and pain in relation to RR (r = 0.317, p = 0.04, r = 0.334, p = 0.03, respectively), demonstrating that the higher the ROM and motor impairment, the higher the RR values will be.
We observed a moderate inverse correlation for age, demonstrating that the higher this variable, the higher is the DBP (r= -0.435, p= 0.005), as already known. The longer is the time since the lesion, the lower is the RR (r= 0.454, p= 0.003).
Regarding the relation between variables, this is an unprecedented study and there are no studies that evaluated these outcomes associated with aerobic exercise prior to this article so we could compare results.
Second aim of this study was to analyze the acute effects of an aerobic exercise session on the hemodynamic response and breathing frequency of individuals with chronic stroke. Thus, the observed results within normal limits in the collected measures, besides the capacity to reach expected values for this exercise during the peak of the activity and to return to the initial parameters.
At the resting stage, the initial values of SBP presented by our sample are considered high, but not characterized as hypertension, according to the AHA blood pressure statements25. At 25 minutes of exercise, BP is increased as expected to any subject undergoing exercise.
Our results showed a decrease in SBP found at the recovery period (initial SBP = 127, SD 9.26mmHg; final SBP = 119.87mmHg, SD 8.95), this event can be described as the post-exercise hypotension effect (PEH)26-29. Considering the benefits of PEH obtained by a regular training for the hypertensive population of this group, the result can be also beneficial.
It is possible to observe that, in the resting condition, the HR presented is 69bpm (SD 9.11), a normal value range of HR30. During exercise, this value increases to 114.25bpm (SD 19.02), which represents the ability of these individuals to achieve the submaximal HR proposed during the training. In the recovery phase, HR returns to 73.42bpm (SD 8.47), which may indicate good performance of vagal activation and sympathetic withdrawal during the following minutes after the event. The heart rate recovery (HRR), is frequently altered in populations with cardiovascular diseases or associated with risk factors31 and delays in this recovery are strongly linked to mortality32. Despite the cardiac comorbidities that frequently accompany this group, our sample had a good performance of this system before, during and after exercise.
Respiratory deficits may also be very common in individuals post-stroke, especially when the brainstem is compromised. Muscle weakness, decreased respiratory mechanisms and lung volumes, reduced chest wall mobility, physical inactivity, associated diseases and cardiovascular changes may further impair this ability of the subject and lead to less resistance to exercise, shortness of breath, sedentary lifestyle and, more importantly, recurrence of stroke33. On this variable, the results presented by our sample are also positive: participants submitted to aerobic exercise at rest indicate RR within normal range presenting 20.17rpm (SD 3.97) during the peak of the exercise rate reached 28.77rpm (SD 3.56) and, at the recovery stage, 21.82rpm (SD 11.53).
A few authors studied cardiorespiratory responses of chronic individuals post-stroke for some different purposes and registered measurements that were also used in this study. Results of Billinger et al.5 showed a HR peak (127.4bpm, SD 28.8) and RR (33.0rpm, SD 8.5) larger than our group, as did Baert et al.9 whose results for this variable was also higher than ours (133.3bpm, SD 31.5), Olivier et al.34 measured HR peak and, once more, there were found larger results compared to ours. In contradiction, Salbach et al.35 founded a HR peak lower than our findings (98.3bpm, SD 17.1).
Comparing cardiorespiratory performance between individuals post-stroke and healthy individuals, the study by Tomczak et al.36 found no differences between this groups, except for the resting HR parameter, which was higher in the stroke group and a lower training HR than the control group was observed. The latest result differs from our findings, since the individuals were able to reach training HR, however the other analyzed parameters in the exercise and rest phases corroborate with those found in our study. Marsden et al.37 submitted post stroke and healthy individuals to aerobic training; concluded that the stroke group has lower cardiorespiratory fitness than the healthy individuals group matched by age and sex.
Although the samples of these studies were similar to the assessed individuals in our research, these divergences were observed as well as a lack of cardiorespiratory and cardiovascular measurements information. It is important to emphasize that despite all of these studies contribute for our results analyze, none of them aimed or registered the recovery parameters after the submitted exercise.
Study Limitations
The sample size is recognized as a study limitation and it is justified by the choice to use a convenience sample.
CONCLUSION
Post- stroke individuals present moderate correlation between hemodynamic and respiratory responses during aerobic exercise and balance, muscle strength, injury time, age and side of lesion. They also have the capacity to return to their cardiorespiratory and cardiovascular resting state right after the activity besides their cardiorespiratory deficits.
Acknowledgments
1- The authors would like to thank the financial support from the Fundação de Amparo à Pesquisa do Estado de São Paulo for believing and investing in this project and the members of the Laboratório de Delineamento de Estudos e Escrita Científica do Centro Universitário FMABC for all the rich collaboration in this study;
2- To the Secretaria de Estado de Saúde do Acre (SESACRE), the Federal University of Acre (UFAC) and the Centro Universitário Saúde FMABC, for the interinstitutional partnership through agreement nº. 007/2015, for the training of health professionals in Acre, Western Amazon, Brazil.
Conflict of interest
None declared.
REFERENCES
1.As 10 principais causas de morte [Internet]. [cited 2021 Jun 24]. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death [ Links ]
2.WHO EMRO Acidente vascular cerebral, acidente vascular cerebral | Tópicos de saúde [Internet]. [cited 2021 Jun 24]. Available from: http://www.emro.who.int/health-topics/stroke-cerebrovascular-accident/index.html [ Links ]
3.Mazzola D, Polese JC, Schuster RC, Oliveira SG de. Perfil dos pacientes acometidos por acidente vascular encefálico assistidos na Clínica de Fisioterapia Neurológica da Universidade de Passo Fundo. Revista Brasileira em Promoção da Saúde. 2007;22-7. [ Links ]
4.Teixeira-Salmela LF, Silva PC e, Lima RCM, Augusto ACC, Souza AC de, Goulart F. Exercise Machines and aerobic conditioning on functional performance of chronic stroke survivors. Acta Fisiátrica [Internet]. 2003 Aug 9 [cited 2021 Jun 24]; 10(2): 54-60. Available from: https://www.revistas.usp.br/actafisiatrica/article/view/102441 [ Links ]
5.Billinger SA, Taylor JM, Quaney BM. Cardiopulmonary response to exercise testing in people with chronic stroke: A retrospective study. Stroke Research and Treatment [Internet]. 2012 [cited 2021 Jun 24]; 2012. Available from: /pmc/articles/PMC3180817/ [ Links ]
6.Ovando AC, Michaelsen SM, Dias JA, Herber V. Licenciado sob uma Licença Creative Commons. Fisioter Mov. 2010; 23(2): 253-69. [ Links ]
7.Rimmer JH, Wang E. Aerobic exercise training in stroke survivors [Internet]. Vol. 12, Topics in Stroke Rehabilitation. Top Stroke Rehabil; 2005 [cited 2021 Jun 24]. p. 17-30. Available from: https://pubmed.ncbi.nlm.nih.gov/15735998/ [ Links ]
8.Winstein CJ, Stein J, Arena R, Bates B, Cherney LR, Cramer SC, et al. Guidelines for Adult Stroke Rehabilitation and Recovery. Stroke [Internet]. 2016 Jun 1 [cited 2021 Jun 24]; 47(6): e98-169. Available from: https://www.ahajournals.org/doi/10.1161/STR.0000000000000098 [ Links ]
9.Baert I, Feys H, Daly D, Troosters T, Vanlandewijck Y. Are patients 1 year post-stroke active enough to improve their physical health? Disability and Rehabilitation [Internet]. 2012 [cited 2021 Jun 24]; 34(7): 574-80. Available from: https://pubmed.ncbi.nlm.nih.gov/21981331/ [ Links ]
10.Meschia JF, Bushnell C, Boden-Albala B, Braun LT, Bravata DM, Chaturvedi S, et al. Guidelines for the primary prevention of stroke: A statement for healthcare professionals from the American heart association/American stroke association. Stroke [Internet]. 2014 Dec 11 [cited 2021 Jun 24]; 45(12): 3754-832. Available from: /pmc/articles/PMC5020564/ [ Links ]
11.Tombaugh TN, Mclntyre NJ. The Mini-Mental State Examination: A Comprehensive Review. J Am Geriatr Soc. 1992; 40(9): 922-35. DOI: 10.1111/j.1532-5415.1992.tb01992.x [ Links ]
12.Berg K, Dauphinee, SW, Williams JI . The Balance Scale: reliability assessment with elderly residents and patients with an acute stroke. Scand J Rehabil Med. 1995; 27(1):27-36 [ Links ]
13.Gladstone DJ, Danells CJ, Black SE. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties. Neurorehabil Neural Repair. 2002; 16(3): 232-240. DOI:10.1177/154596802401105171 [ Links ]
14.Kalra L, Crome P. The Role of Prognostic Scores in Targeting Stroke Rehabilitation in Elderly Patients. J Am Geriatr Soc. 1993; 41(4): 396-400. DOI:10.1111/j.1532-5415.1993.tb06947.x [ Links ]
15.Billinger SA, Arena R, Bernhardt J, et al. Physical activity and exercise recommendations for stroke survivors: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014; 45(8): 2532-2553. DOI:10.1161/STR.0000000000000022 [ Links ]
16.Prior PL, Suskin N. Exercise for stroke prevention. Stroke Vasc Neurol. 2018; 3(2): 59-68. DOI:10.1136/svn-2018-000155 [ Links ]
17.Brogårdh C, Lexell J. Effects of cardiorespiratory fitness and muscle-resistance training after stroke. PM R. 2012; 4(11): 901-907. DOI:10.1016/j.pmrj.2012.09.1157 [ Links ]
18.Carr M, Jones J, Author A, et al. Physiological effects of exercise on stroke survivors. Top Stroke Rehabil. 2003; 9(4): 57-64. Disponível em: http://www.ncbi.nlm.nih.gov/pubmed/14523700 [ Links ]
19.Pang MYC, Charlesworth SA, Lau RWK, Chung RCK. Using aerobic exercise to improve health outcomes and quality of life in stroke: Evidence-based exercise prescription recommendations. Cerebrovasc Dis. 2013; 35(1): 7-22. DOI:10.1159/000346075 [ Links ]
20.Prout EC, Mansfield A, McIlroy WE, Brooks D. Patients' perspectives on aerobic exercise early after stroke. Disabil Rehabil. 2016; 39(7): 984-690. DOI:10.3109/09638288.2016.1161833 [ Links ]
21.Tiozzo E, Youbi M, Dave K, et al. Aerobic, Resistance, and Cognitive Exercise Training Poststroke. Stroke. 2015; 46(7): 2012-2016. DOI:10.1161/STROKEAHA.114.006649 [ Links ]
22.Acar S, Demırbüken İ, Algun C, Malkoç M, Tekın N. Is hypertension a risk factor for poor balance control in elderly adults? J Phys Ther Sci. março de 2015; 27 (3): 901-4. [ Links ]
23.Abate M, Di Iorio A, Pini B, Battaglini C, Di Nicola I, Foschini N, et al. Effects of hypertension on balance assessed by computerized posturography in the elderly. Arch Gerontol Geriatr. agosto de 2009; 49 (1): 113-7. [ Links ]
24.Europe pmc [Internet]. [citado 24 de junho de 2021]. Disponível em: https://europepmc.org/article/MED/31354419 [ Links ]
25.High blood pressure [Internet]. www.heart.org. [citado 24 de junho de 2021]. Disponível em: https://www.heart.org/en/health-topics/high-blood-pressure [ Links ]
26.Halliwill JR, Buck TM, Lacewell AN, Romero SA. Postexercise hypotension and sustained postexercise vasodilatation: what happens after we exercise? Exp Physiol. janeiro de 2013; 98 (1): 7-18. [ Links ]
27.Cardiovascular observations on Tarahumara Indian runners-the modern Spartans. American Heart Journal. 1o de março de 1971; 81 (3): 304-14. [ Links ]
28.Cardoso CG, Gomides RS, Queiroz ACC, Pinto LG, da Silveira Lobo F, Tinucci T, et al. Acute and chronic effects of aerobic and resistance exercise on ambulatory blood pressure. Clinics (Sao Paulo). março de 2010; 65 (3): 317-25. [ Links ]
29.Carpio-Rivera E, Moncada-Jiménez J, Salazar-Rojas W, Solera-Herrera A. Acute effects of exercise on blood pressure: a meta-analytic investigation. Arq Bras Cardiol. maio de 2016; 106 (5): 422-33. [ Links ]
30.American Heart Association. Acessado em Junho de 2018 em https://www.heart.org/en/health-topics/high-blood-pressure/the-facts-about-highbloodpressure/all-about-heart-rate-pulse [ Links ]
31.Peçanha T, Silva-Júnior ND, Forjaz CL de M. Heart rate recovery: autonomic determinants, methods of assessment and association with mortality and cardiovascular diseases. Clinical Physiology and Functional Imaging. 2014; 34 (5): 327-39. [ Links ]
32.Cole CR, Blackstone EH, Pashkow FJ, Snader CE, Lauer MS. Heart-rate recovery immediately after exercise as a predictor of mortality. N Engl J Med. 28 de outubro de 1999; 341 (18): 1351-7. [ Links ]
33.Europe pmc [Internet]. [citado 24 de junho de 2021]. Disponível em: http://europepmc.org/article/PMC/2845242 [ Links ]
34.Olivier C, Doré J, Blanchet S, Brooks D, Richards CL, Martel G, Robitaille NM, Maltais DB. Maximal cardiorespiratory fitness testing in individuals with chronic stroke with cognitive impairment: practice test effects and test-retest reliability Arch Phys Med Rehabil. 2013; 94(11): 2277-82. doi: 10.1016/j.apmr.2013.03.016 [ Links ]
35.Salbach MN, MacKay-Lyons M, Solomon P, Howe J, McDonald A, Bayley MT, Veitch S, Sivarajah L, Cacoilo J, Mihailidis A. The role of theory to develop and evaluate a toolkit to increase clinical measurement and interpretation of walking speed and distance in adults post-stroke Disabil Rehabil. 2021 16; 1-17. doi: 10.1080/09638288.2020.1867653 [ Links ]
36.Tomczak CR, Jelani A, Haennel RG, Haykowsky MJ, Welsh R, Manns PJ. Cardiac reserve and pulmonary gas exchange kinetics in patients with stroke. Stroke. 1o de novembro de 2008; 39 (11): 3102-6. [ Links ]
37.Marsden DL, Dunn A, Callister R, Levi CR, Spratt NJ. Characteristics of exercise training interventions to improve cardiorespiratory fitness after stroke: a systematic review with metaanalysis. Neurorehabil Neural Repair. dezembro de 2013; 27 (9): 775-88. [ Links ]
 Correspondence:
Correspondence:
Rodrigo Daminello Raimundo
rodrigo.raimundo@fmabc.br
Manuscript received: January 2021
Manuscript accepted: May 2021
Version of record online: July 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}