










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.2 Santo André maio/ago. 2021
http://dx.doi.org/10.36311/jhgd.v31.11410
ORIGINAL ARTICLE
Prevalence and factors associated with metabolic syndrome in a vulnerable population in northern Brazil: a cross-sectional study
Mayzza Campina RodriguesI, II; Erika da Silva MacielIII; Fernando Rodrigues Peixoto QuaresmaIII; Luis Fernando Castagnino SestiIV; Laércio da Silva PaivaI; Hugo Macedo JuniorV; Francisco Albino de AraújoV; Fernando Luiz Affonso FonsecaV; Fernando AdamiI
ILaboratório de Epidemiologia e Análise de Dados. Centro Universitário FMABC, Santo André, São Paulo, SP 09060-870, Brazil;
IISecretaria de Estado da Saúde do Tocantins SES/TO, Palmas, Tocantins, TO 77015-212, Brazil
IIIUniversidade Federal do Tocantins UFT/TO, Miracema, Tocantins, TO 77650-000, Brazil;
IVCentro Universitário Luterano de Palmas - CEULP/ULBRA, Palmas, TO 77019-900, Brazil;
VLaboratório de Delineamento de Estudos e Escrita Científica, Centro Universitário FMABC, Santo André, São Paulo, SP 09060-870, Brazil
ABSTRACT
INTRODUCTION: metabolic syndrome (SM) is a set of metabolic imbalances that are associated with the development of cardiovascular diseases, type 2 diabetes mellitus, in addition to other chronic non-communicable diseases. SM has been gaining prominence in the scientific community mainly due to link with the increase of the obesity epidemic in the world
OBJECTIVE: To analyze the factors associated with metabolic syndrome and its prevalence in a vulnerable population in the Northern Region of Brazil
METHODS: This is a cross-sectional study with artisanal fishers from the state of Tocantins, and data collected between 2016 and 2017 were used. The outcome variable for MS was defined according to the criteria of the International Diabetes Federation. The following variables were assessed: socioeconomic and demographic information, fish consumption, and smoking. For statistical and data analysis, the Shapiro-Wilk test, Poisson regression, Student's t-test, and interquartile regression were evaluated
RESULTS: The general prevalence rate (PR) of MS was 31.9% higher in women than in men. The factors associated with MS were economic class and smoking, and there was an association between socioeconomic class and smoking (p=0.015). The most prevalent component was abdominal obesity with a rate of 62.5% (95% confidence interval [CI]: 54.5, 70.5). The prevalence of MS in terms of sex (PR=2.27, 95% 1.04 CI, 4.92, p=0.037), smoking (PR=2.40, 95% CI, 30, p=0.003) and years of professional experience (>10 PR=2.07, 95% CI 1.06, 4.05, p=0.033) was also assessed
CONCLUSION: In the present study, the prevalence of SM was associated with smoking and socioeconomic status, which is considered high when compared to the worldwide prevalence. These findings highlight the importance of looking at public policies so that health services can develop actions that generate greater adherence to good health practices by the population
Keywords: obesity, cardiovascular disease, lifestyle, vulnerable population.
Authors summary
Why was this study done?
Chronic non-communicable diseases are among the main causes of death in the world; among the many causes stands out the, Metabolic Syndrome, characterized by a set of factors that increase the chances of the development of cardiovascular diseases and other health problems. However, there are still few population-based studies that assess metabolic syndrome in Brazil, especially with populations in conditions of social vulnerability.
What did the researchers do and find?
We conducted the research in four artisanal fisheries colonies in the State of Tocantins, Brazil, on the banks of the Luís Eduardo Magalhães Hydroelectric Plant Lake, between the years 2016 and 2017. The socioeconomic, sociodemographic, anthropometric, biochemical, and systemic blood pressure variables were evaluated. Metabolic Syndrome was defined based on the parameters of the International Diabetes Federation. The results indicated a prevalence of 31.9%, which was considered high when compared to the worldwide prevalence by the International Diabetes Federation group, which found a result between 20-25%. The main factors associated with this prevalence were smoking and socioeconomic status.
What do these findings mean?
Metabolic Syndrome is a factor that increases the risk of developing Chronic Noncommunicable Diseases and especially cardiovascular diseases, which are associated with smoking and socioeconomic status can influence the increase in prevalence over time.
INTRODUCTION
The effects of globalization, rapid urbanization, and increased life expectancy, in addition to harmful health behaviors, which include the use of alcohol and cigarettes, can be seen in the development of Chronic Noncommunicable Diseases (NCDs), as indicated by data from the World Health Organization Health (WHO)1.
Metabolic Syndrome (MS), a gateway to the development of NCDs, is characterized by a set of metabolic imbalances that include excess abdominal fat, high levels of triglycerides, low level of high-density lipoprotein-cholesterol (HDL-C), levels high blood pressure, and insulin resistance2 and can increase the risk of morbidity and mortality due to cardiovascular diseases by 2.5 times3.
Much has been discussed about MS and the increased impact of premature morbidity and mortality in the general population. Still, little has been studied about the relationship with vulnerable populations, asare artisanal fishers.
It is important to consider that the time of exposure of fishers to conditions of social, economic, environmental vulnerability and habits resulting from lifestyle can lead to progressive changes in morbidity and mortality and the epidemiological transition of the health-disease process of this population.
It is important to consider that social vulnerability brings to the research field a concept of a link between the global structural relations of society and the risk situations in which certain populations are exposed4 as in the case of artisanal fishers.
There is little scientific evidence about this important population and, in order to understand these processes and improve public policies and health promotion, studies need to be carried out5.
Artisanal fishing is a manual activity with high energy expenditure; however, in fishers, social and economic factors, such as low income and education, working conditions and difficulty accessing health services6-8, can lead to an unbalanced diet resulting in overweight and/or obesity. In addition, factors such as sex, ethnicity, education, and housing conditions influence NCDs9 characteristics also observed in this population.
In this context of vulnerability, in the state of Tocantins, Brazil, the riverside populations, which include artisanal fishers, were affected by the construction of the Luís Eduardo Magalhães Hydroelectric Plant in 2002. Since then, a change has been observed in the work activities and in the lifestyle of the fishers, which can affect the risk of developing MS and, consequently, NCDs.
Therefore, considering that the indicators of MS are associated with lifestyle patterns, this study aimed to analyze the factors associated with SM and its prevalence in a vulnerable population in the Northern Region of Brazil.
METHODS
Study design
This is a cross-sectional study10 conducted with artisanal fishers, characterized as a vulnerable population.
Period and location of research
The Tocantins state in Brazil is rich in freshwater rivers, fishing sources, leisure activities, and other jobs. In the state, artisanal fishing uses small boats and few and/or simple fishing instruments.
Fishing activity is regulated by the Rural Development Institute of the State of Tocantins, and there are currently 35 fishing colonies in the state. Of these, four colonies around the lake that were dammed by the construction of the Luís Eduardo Magalhães Hydroelectric Plant were chosen due to the greater ease of access.
Fishers from four colonies of the lake of the Luís Eduardo Magalhães Hydroelectric Power Plant were included in this study. The colonies were: Itaobi, in Brejinho de Narazé, Z-10 and Associação Parque Sucupira, in Palmas and COPEMITO - Fisher's Colony of Miracema, in Miracema.
Studied population and Eligibility Criteria
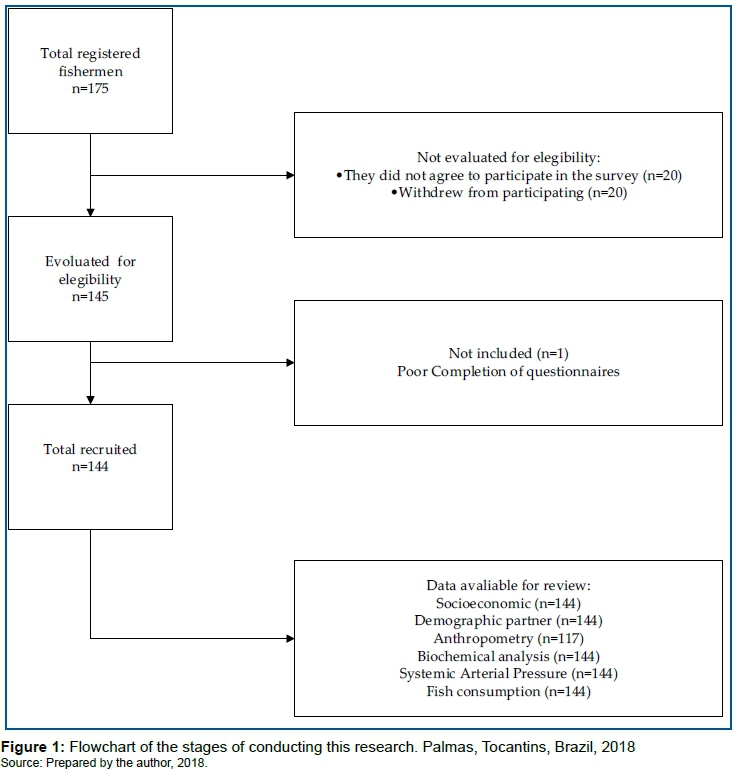
The sample was obtained by convenience sampling and was composed of participants who met the inclusion criteria, being: fishers over the age of 18 who agreed to participate voluntarily by accepting and signing the Free and Informed Consent Form. Meanwhile, those who did not agree to participate in the study and did not participate in any study stage were excluded. Thus, 144 fishers were included (figure 1).
Data collection
Data were collected between 2016 and 2017 through interviews previously scheduled by the presidents of the colonies and through semi-structured interviews previously conducted by trained researchers. The study started after the authorization of the fishers, and data collection was scheduled.
Data collection was carried out in different stages. First, the leaders were contacted and authorized to present the project to the fishers of the respective colonies; then, a return was scheduled for the next stages. After signing the informed consent form by the fishers who agreed to participate in the research, blood samples were collected and anthropometric assessments and interviews were carried out.
Data analysis
Variables
Socioeconomic and demographic characteristics, anthropometric data (abdominal perimeter), results of biochemical analyzes (glucose levels, HDL-cholesterol, and triglycerides), and systemic blood pressure were evaluated. Based on the measurement of these variables, we classify metabolic disorders and SM according to the parameters established by the International Diabetes Federation (IDF). SM was the outcome variable, and the other variables were used as exposure variables.
Socioeconomic Characteristics
The socioeconomic level was assessed using the Brazilian Economic Classification questionnaire11 and questions about the participants' sex and age.
Fish Consumption
The assessment of the perception of fish consumption was performed using the instrument proposed and validated by Maciel et al.12, which aimed to identify the pattern of consumption and barriers in adults.
Central Obesity
The evaluation of the abdominal perimeter was performed to measure central obesity with an anthropometric tape (Sanny brand), and the measurement was obtained from the midpoint between the last rib and the iliac crest. At the same time, the participant was in an orthostatic position, as recommended by the Association Brazilian for the study of obesity and metabolic syndrome13. For the classification of abdominal obesity, the values recommended by the IDF were as follows: ≥90 cm for men and ≥80 cm for women3.
Biological Tests
Triglyceride levels ≥150mg/dL, HDL-cholesterol <40mg/dL for men and <50mg/dL for women and fasting blood glucose <100 mg/dL were analyzed, according to the IDF21 criteria and non-HDL-cholesterol classified as <160mg/dL low risk, <130 mg/dL intermediate, <100 mg/dL high and <80 mg/dL very high to estimate cardiovascular risk with the variable SM14. Biochemical indicators were obtained by collecting peripheral venous blood, with participants fasting for 12 hours, compliance with biosafety rules. The samples were kept under refrigeration and laboratory analysis within one hour after collection by the enzymatic-colorimetric method by automation. (BS-200E Mindray ®).
Systemic Blood Pressure
Blood pressure (BP) was measured with a sphygmomanometer and stethoscope, based on the recommendations of the VII Brazilian Guideline for Hypertension15.
Metabolic Syndrome
The definitions widely used to establish SM are those of the World Health Organization (WHO), National Cholesterol Education Program's Adult Treatment Panel III (NCEP-ATP III) and International Diabetes Federation (IDF) which, although they have common characteristics, differ in their points of view which makes it difficult to have a universal classification of the prevalence of SM.
In this study, SM was defined according to the IDF3 criteria, which defines the presence of abdominal obesity with cutoff points specific to ethnic groups and at least two other metabolic risk factors, which may include the presence of hyperglycemia, dyslipidemia, and/or arterial hypertension.
Study Size
As there were no studies that estimated the prevalence of SM in artisanal fishers, the prevalence rate ranged from 14.9% to 65.3%, as presented by Vidigal et al.16 in a systematic review on the prevalence of SM in adults. In the colonies studied, the total number of registered artisanal fishers was 175. When considering an error of 5%, confidence level (CI) of 95%, and test power of 80%, the estimated sample size ranged from 93 to 121. When adding 10% of the sample to possible losses, the final sample size for this study was approximately 142.
Statistical methods
Standard descriptive statistics were used. Qualitative variables were presented as absolute and relative frequencies. Quantitative variables were presented as measures of central tendency and respective interval estimates (95% CI), according to the normality of the data, assessed by the Shapiro-Wilk test.
The associated measures were roughly estimated. To estimate the prevalence ratio (PR) of SM and its 95% CI, Poisson regression with robust variance was used. Meanwhile, quantitative variables were presented as mean or median, assessed by Student's t-test and interquartile regression.
The explanatory models were estimated using Poisson regression with robust variance by the stepwise backward method, with the entry (p=0.20) and removal (p=0.05) criteria. The level of significance was set at 5%. Stata® software version 11.0 was used (StataCorp, LC).
Social vulnerability
There are many definitions for the concept of vulnerability, and they are always related to the object of which one intends to study, this being neither a subject as young nor as old.
However, the definition of choice for the concept of social vulnerability in the present study was that of Andrew17 (2015), who points out that social vulnerability results from the accumulation of multiple and varied social problems and is bi-directionally important as a risk factor for poor health outcomes. As a pragmatic consideration for the provision and planning of health care, however, it is important to note that data were not analyzed to define a vulnerability index to which the population of artisanal fishers studied here ise exposed.
Ethical and legal aspects of research
The project was submitted to and approved by the Human Research and Ethics Committee (CAAE 50419215.5.0000.5516).
RESULTS
175 artisanal fishers registered in the studied colonies, residents of the municipalities of Brejinho de Nazaré, Palmas, and Miracema do Tocantins, were contacted. However, after the initial contact, only 144 fishers participated in the survey.
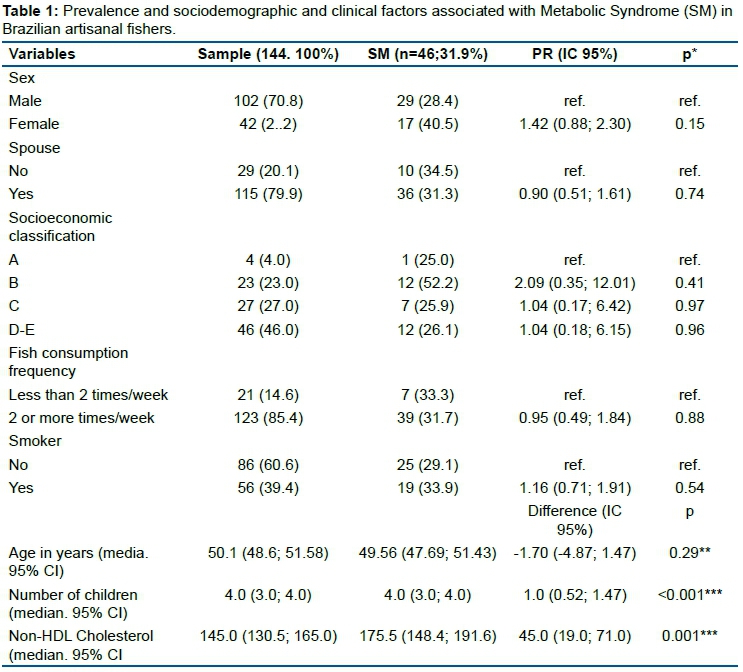
144 artisanal fishers were evaluated, most of them men (70.8%, n=102), spouse (79.9%, n=115) and socioeconomic classification D or E (46.0%; =46). Regarding lifestyle, most reported consuming fish 2 or more times a week (85.4%; n=123) and 39.4% (n=56) were smokers. Participants had a mean age of 50.1 (95% CI: 48.6; 51.58) years, median (95% CI) of 4.0 (3.0; 4.0) children and a mean HDL-C level of 145.0 (130.5, 165.0) (table 1).
Regarding the components of the metabolic disorder for the definition of MS according to the IDF criteria, the most prevalent was the high abdominal perimeter, observed in 62.5% of the participants, which is a mandatory criterion, followed by low HDL-C levels in 59.7% of patients and high triglyceride levels in 26.4% of participants (table 2).
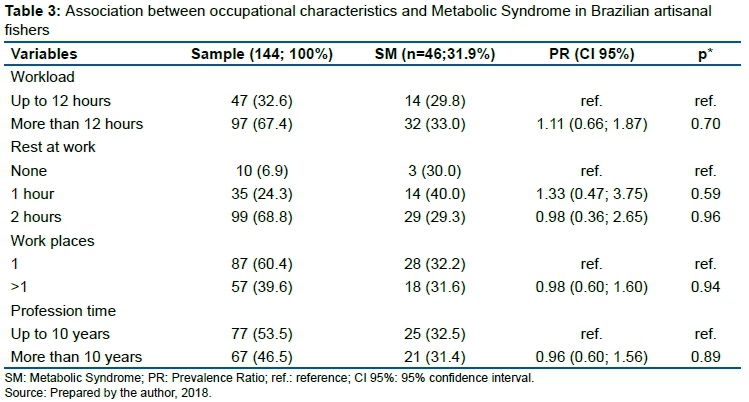
Most fishers worked 12 hours a day (67.4%, n=97), with two hours of rest (68.8%, n=99), and worked in only one place (60.4%, n=87). Most fishers reported working in the activity for at least 10 years (53.5%, n=77) (table 3).
Of the 144 fishers, 46 had SM, and the rate was 31.9. Of the sociodemographic characteristics studied, only the number of children showed a statistically significant difference, and the individuals who presented metabolic syndrome had a median of 1 (ranging from 0.52 to 1.47) more children when compared to individuals without metabolic syndrome (p <0.001) (table 1). The non-HDL-c variable showed a statistically greater difference in participants with MS when compared to participants without SM (p <0.001) (table 1).
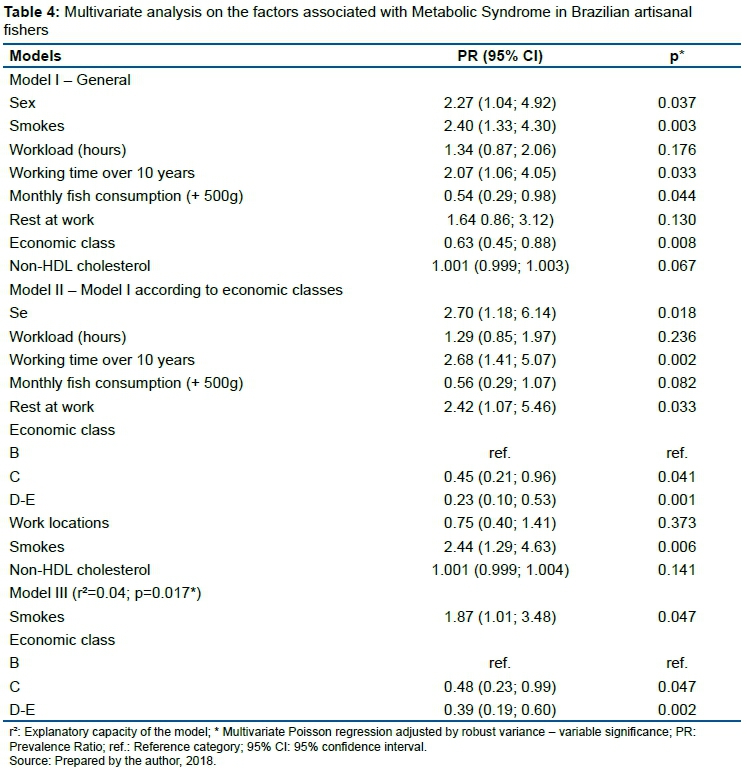
In the multivariate analysis adjusted for socioeconomic variables and occupational characteristics, some explanatory models were used to analyze the factors associated with SM.
In model 1, with an explanatory capacity of 6% (r2=0.06, p=0.002), sex (PR=2.27, 95% CI: 1.04, 4.92, p=0.037), smoking (PR=95, 95% CI 1.33, 4.30, p=0.003) and work experience over 10 years (PR=2.07, 95% CI 1.06, 4.05, p=0.033) were associated with higher prevalence of SM. On the other hand, economic class (PR=0.63, 95% CI: 0.45, 0.88, p=0.008) and weekly fish consumption (>500 g) were correlated with a lower prevalence of SM (PR=54, 95% CI: 0.29, 0.98, p=0.044) (table 4).
On the other hand, when individuals classified in economic class A were excluded due to the small sample size (model 2), a higher prevalence of SM was observed in fishers who rest at work (PR=2.42, 95% CI, 1.07, 5.46, p=0.033). Meanwhile, a lower prevalence of SM was observed in fishers classified in economic classes C, D and E (PR: 0.45, 95% CI 0.21, 0.96, p=0.041 and PR=0.23, CI 95%: 0.10, 0.53, p=0.001).
In addition, in model 3, after adjusting for sex, there was a higher prevalence of SM in smokers (PR: 1.87, 95% CI: 1.01, 3.48, p=0.047) and lower prevalence in fishers classified as economic classes C, D and E with reference to class B (PR=0.48, 95% CI: 0.23, 0.99, p = 0.047) for individuals in class C (PR = 0.39, ranging from 0, 19 to 0.60, p = 0.002 in class C) (table 4).
Considering the influence of socioeconomic status and smoking on the prevalence of MS in fishers, a sensitivity analysis was performed to identify the association between these characteristics and SM. In this analysis, an association was observed between socioeconomic class and smoking (p=0.015). In other words, the highest number of smokers was observed in social classes D and E (55.6%), followed by classes C (33.3%) and B (22.7%). No class A smokers were observed (table 5).
DISCUSSION
The main findings of this study indicated that the associated factors were smoking and socioeconomic status and that approximately 31.9% of artisanal fishers had MS, which is higher than the general prevalence rate (20% -25%)3. In addition, MS was more prevalent among class B participants; however, the lower the economic level of the fishers, the greater the prevalence of smokers.
The present study found an association between smoking and MS, and there was a greater number of smokers in classes D and E, which can lead to a change in the prevalence of MS and economic classes, indicating that the main risk factor for MS is the tobacco use and not necessarily an economic class.
There is a 26% increase in the risk of MS in active smokers than in non-smokers18. Koster et al.19 found a strong association between smoking and deposition of abdominal fat, in addition to a five-fold increase in the risk of death from diseases such as cancer, coronary heart disease, stroke, diabetes mellitus, pulmonary emphysema, and kidney disease. These results reinforce that smoking is a risk factor for NCDs.
As for the socioeconomic level, a lower prevalence of SM was observed among fishers from lower social classes, different from what was reported in the literature, as in the case of the USA, in which low educational level and income/poverty index are associated with the presence of SM20. In addition, Moreira et al.21 found a higher prevalence of SM in individuals of lower socioeconomic status, although the result was not statistically significant.
With regard to the value found for the prevalence of SM, studies also carried out with quilombola populations in the north of the country found similar prevalences, 32.1%22 and 33.3%23, respectively.
The data in this study also corroborate those found in other studies, although the prevalence may vary according to the definition criteria used, as in the USA (34.2%)20 and Nigeria (35.1%)19.
However, it is difficult to make comparisons between the prevalence of SM due to different definition criteria with variable cutoff points and few studies evaluating SM in vulnerable populations, as in the case of artisanal fishers.
Stratification by sex in the study showed a higher prevalence of MS among women, which was also found in other studies20,25. This difference can be attributed to the different cutoff points for abdominal circumference, dyslipidemia attributed to the greater deposit of body fat, and the reduction of estrogen levels found in women26.
In this study, the components with the highest prevalence were increased waist circumference, low levels of HDL-C, and high levels of triglycerides. This finding confirmed that MS is a disorder that may be associated with obesity.
According to the IDF, the presence of abdominal obesity is the essential criterion for cardiometabolic risks3. The increase in obesity can be understood as a product of greater urbanization, nutritional transition, and reduced physical activity27, considering its growing pandemic. Its complications affect the morbidity and mortality profile of all countries.
In a population-based study with a sample of 1,116 individuals in an urban population in the southwest of the country, using the NCEP ATP III and IDF criteria, Gronner et al.25 found that approximately 72.6% of the individuals had an increase in the circumference of the waist according to criteria similar to those found in this study. The lipid profile is one of the tools used to assess the risk of cardiovascular disease, its control, and prognosis. However, it is not part of the criteria used for the diagnosis of SM; data on the low level of non-HDL-C can significantly contribute to the interpretation of metabolic changes.
This indicator was used as a marker superior to LDL-C for the definition of cardiovascular risk and therapeutic efficacy for cases of myocardial infarction, in addition to the low cost for estimation28. The NCEP ATP-III has a low level of non-HDL-C as a secondary therapy target in individuals with decreased levels of HDL-C associated with high levels of triglycerides (≥200-499 mg/dL) as a strategy for the specific treatment of dyslipidemias29.
Thus, in our study, a statistically significant difference was observed between the non-HDL-C variable and participants with MS. Participants with MS had the largest variable, 175.5 (148.4; 191.6) when comparing participants without MS, 145.0 (130.5; 165.0). Our findings corroborate those of a study conducted in India that aimed to identify the association between non-HDL-C and SM in participants with and without coronary heart disease. The results showed a significant association between non-HDL-C and SM30.
The prevalence of SM is associated with several factors that directly impact the development of NCDs, especially cardiovascular diseases and diabetes mellitus, and knowing these determining factors mainly in a vulnerable population such as artisanal fishers become important to provide promotional actions to health that aims to adopt a lifestyle with healthy eating and physical activity.
CONCLUSION
There is a high prevalence of MS when compared to general data, which reinforces that this condition is an important public health problem. Tobacco use increases the risks of NCDs, and the association of MS with smoking found in the study, when also compared with the socio-economic situation, demonstrates that the prevalence values of MS can increase over the years in this population, since there may be an increase of the incidence of MS in the population economically classified as class D-E.
Notably, future studies should be conducted to determine the general prevalence of MS among the Brazilian population and how life habits can influence the development of this condition. In addition to promoting the attention of public managers to the formulation of public policies that can promote the population changing habits for a healthier lifestyle. Since only access to information does not guarantee adherence to the routine of good health practices.
Authors' contributions
MCR - responsible for all aspects of the main text of the manuscript and the communication and management of communication between the co-authors. ESM - contribution in the conception, design, elaboration, and revision of the intellectual content of the manuscript. FRPQ and LFCS - contributions in the conception of the manuscript, assistance in the interpretation of the data, and the formulation of the argumentation and revision of the entire writing. LPS - contributions to the revision version to be published. FAA - contributions to the revision version to be published. FLAF - contributions to the revision version to be published. FA - substantial contributions to the revision and final approval of the version to be published. All authors read and approved the final manuscript.
Financing
The research was funded by the EMBRAPA Management System (SEG), Macro 4 program, with the number MP4SEG 04.13.09.001.00. EMBRAPA intermediated access to the colonies through the leaders so that the research was presented and data collection was carried out. The company also collaborated with the transportation of researchers to the colonies and with the materials used in the data collection. The financing company did not participate in the construction of this manuscript, only in the mediation for data collection.
Acknowledgments
We thank the fishing colonies for their trust, support, and participation in this project.
Conflicts of interest
The authors declare that they have no conflicts of interest regarding the authorship and/or publication of this article.
REFERENCES
1.Relatório de status global sobre álcool e saúde 2018 [Internet]. [citado 1º de abril de 2021]. Disponível em: https://www.who.int/publications-detail-redirect/9789241565639 [ Links ]
2.Saad MAN, Cardoso GP, Martins W de A, Velarde LGC, Cruz Filho RA da. Prevalence of metabolic syndrome in elderly and agreement among four diagnostic criteria. Arquivos Brasileiros de Cardiologia [Internet]. 2014 [citado 1º de abril de 2021]; Disponível em: http://www.gnresearch.org/doi/10.5935/abc.20140013 [ Links ]
3.The IDF consensus worldwide definition of the metabolic syndrome. Obes metabol. 15 de setembro de 2005; 2(3): 47-9. [ Links ]
4.Barbosa IR, Gonçalves RCB, Santana RL. Mapa da vulnerabilidade social do município de Natal-RN em nível de setor censitário. J Hum Growth Dev. 6 de maio de 2019; 29(1): 48-56. [ Links ]
5.Freitas ICM de, Moraes SA de. O efeito da vulnerabilidade social sobre indicadores antropométricos de obesidade: resultados de estudo epidemiológico de base populacional. Rev bras epidemiol. junho de 2016; 19(2): 433-50. [ Links ]
6.Pena PGL, Gomez CM. Health of subsistence fishermen and challenges for Occupational Health Surveillance. Ciênc saúde coletiva. dezembro de 2014; 19(12): 4689-98. [ Links ]
7.Silva ELP da, Wanderley MB, Conserva M de S. Proteção social e território na pesca artesanal do litoral paraibano. Serv Soc Soc. março de 2014; (117): 169-88. [ Links ]
8.Faraco LFD, Filho JMA, Daw T, Lana P da C, Teixeira CF. Vulnerabilidade de pescadores no litoral sul do Brasil e sua relação com áreas marinhas protegidas em um cenário de declínio da pesca. Desenvolvimento e Meio Ambiente [Internet]. 31 de agosto de 2016 [citado 1º de abril de 2021]; 38(0). Disponível em: https://revistas.ufpr.br/made/article/view/45850 [ Links ]
9.Barros MB de A, César CLG, Carandina L, Torre GD. Desigualdades sociais na prevalência de doenças crônicas no Brasil, PNAD-2003. Ciênc saúde coletiva. dezembro de 2006; 11(4): 911-26. [ Links ]
10.Zangirolami-Raimundo J, Echeimberg JDO, Leone C. Research methodology topics: Cross-sectional studies. J Hum Growth Dev. 28 de novembro de 2018; 28(3): 356-60. [ Links ]
11.Critério brasil - abep [Internet]. [citado 1º de abril de 2021]. Disponível em: http://www.abep.org/criterio-brasil [ Links ]
12.Maciel E da S, Vasconcelos JS, Silva LKS da, Sonati JG, Galvão J, Silva D da, et al. Designing and validating the methodology for the Internet assessment of fish consumption at a university setting. Food Sci Technol (Campinas). junho de 2014; 34(2): 315-23. [ Links ]
13.Abeso: Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica [Internet]. Abeso. [citado 1º de abril de 2021]. Disponível em: https://abeso.org.br/ [ Links ]
14.Faludi A, Izar M, Saraiva J, Chacra A, Bianco H, Afiune Neto A, et al. Atualização da diretriz brasileira de dislipidemias e prevenção da aterosclerose - 2017. Arquivos Brasileiros de Cardiologia [Internet]. 2017 [citado 1º de abril de 2021]; 109(1). Disponível em: http://www.gnresearch.org/doi/10.5935/abc.20170121. [ Links ]
15.Malachias MVB, Bortolotto LA, Drager LF, Borelli F a. O, Lotaif L a. D, Martins LC, et al. 7th brazilian guideline of arterial hypertension: chapter 12 - secondary arterial hypertension. Arquivos Brasileiros de Cardiologia. setembro de 2016; 107(3): 67-74. [ Links ]
16.de Carvalho Vidigal F, Bressan J, Babio N, Salas-Salvadó J. Prevalence of metabolic syndrome in Brazilian adults: a systematic review. BMC Public Health. dezembro de 2013; 13(1): 1198. [ Links ]
17.Andrew MK. Frailty and social vulnerability. Frailty in Aging. 2015; 41: 186-95. [ Links ]
18.Sun K, Liu J, Ning G. Active smoking and risk of metabolic syndrome: a meta-analysis of prospective studies. Barengo NC, organizador. PLoS ONE. 17 de outubro de 2012; 7(10): e47791. [ Links ]
19.Humphries MC, Gutin B, Barbeau P, Vemulapalli S, Allison J, Owens S. Relations of adiposity and effects of training on the left ventricle in obese youths: Medicine & Science in Sports & Exercise. setembro de 2002; 34(9): 1428-35. [ Links ]
20.Moore JX. Metabolic syndrome prevalence by race/ethnicity and sex in the united states, national health and nutrition examination survey, 1988-2012. Prev Chronic Dis [Internet]. 2017 [citado 1º de abril de 2021]; 14. Disponível em: https://www.cdc.gov/pcd/issues/2017/16_0287.htm [ Links ]
21.Moreira GC, Cipullo JP, Ciorlia LAS, Cesarino CB, Vilela-Martin JF. Prevalence of metabolic syndrome: association with risk factors and cardiovascular complications in an urban population. Barengo NC, organizador. PLoS ONE. 2 de setembro de 2014; 9(9): e105056. [ Links ]
22.Luisi C, Figueiredo FW dos S, Sousa LV de A, Quaresma FRP, Maciel E da S, Adami F. Prevalence of and factors associated with metabolic syndrome in afro-descendant communities in a situation of vulnerability in northern brazil: a cross-sectional study. Metabolic Syndrome and Related Disorders. maio de 2019; 17(4): 204-9. [ Links ]
23.Sousa LVDA, Maciel EDS, Quaresma FRP, Abreu ACG de, Paiva LDS, Fonseca FLA, et al. Quality of life and metabolic syndrome in brazilian quilombola communities: a crosssectional study. J Hum Growth Dev. 28 de novembro de 2018; 28(3): 316-28. [ Links ]
24.Sabir AA, Jimoh A, Iwuala SO, Isezuo SA, Bilbis LS, Aminu KU, et al. Metabolic syndrome in urban city of North-Western Nigeria: prevalence and determinants. The Pan African Medical Journal [Internet]. 27 de janeiro de 2016 [citado 1º de abril de 2021]; 23 (19). Disponível em: https://www.panafrican-med-journal.com/content/article/23/19/full [ Links ]
25.Gronner MF, Bosi PL, Carvalho AM, Casale G, Contrera D, Pereira MA, et al. Prevalence of metabolic syndrome and its association with educational inequalities among Brazilian adults: a population-based study. Braz J Med Biol Res. julho de 2011; 44(7): 713-9. [ Links ]
26.Rocha FL, Melo RLP de, Menezes TN de, Universidade Federal de Campina Grande, Brazil, Universidade Federal da Paraíba, Brazil, Universidade Estadual da Paraíba, Brazil. Factors associated with metabolic syndrome among the elderly in the northeast of Brazil. Rev bras geriatr gerontol. dezembro de 2016; 19(6): 978-86. [ Links ]
27.Misra A, Khurana L. Obesity and the metabolic syndrome in developing countries. The Journal of Clinical Endocrinology & Metabolism. novembro de 2008; 93 (11_supplement_1): s9-30. [ Links ]
28.Sigdel M, Yadav BK, Gyawali P, Regmi P, Baral S, Regmi SR, et al. Non-high density lipoprotein cholesterol versus low density lipoprotein cholesterol as a discriminating factor for myocardial infarction. BMC Res Notes. dezembro de 2012; 5 (1): 640. [ Links ]
29.Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the national cholesterol education program (Ncep) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult treatment panel iii). JAMA: The Journal of the American Medical Association. 16 de maio de 2001; 285(19): 2486-97. [ Links ]
30.Garg PR, Kabita S, Sinha E, Kalla L, Kaur L, Saraswathy KN. The association of non-HDL cholesterol with the presence of metabolic syndrome in North Indian subjects with and without CAD. Annals of Human Biology. janeiro de 2013; 40 (1): 111-5. [ Links ]
 Correspondence:
Correspondence:
Mayzza Campina Rodrigues
mayzza.rodrigues@gmail.com
Manuscript received: January 2021
Manuscript accepted: May 2021
Version of record online: July 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}