










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.2 Santo André maio/ago. 2021
https://doi.org/10.36311/jhgd.v31.12226
ORIGINAL ARTICLE
Surgery associated with radiotherapy in patients affected by metastatic medular compression: scientific production of the health area
Oswaldo Roberto NascimentoI; Gabrielle do Amaral Virginio PereiraII, III; Mauro José de Deus MoraisII, IV, V; Ankilma do Nascimento Andrade FeitosaVI; Marcelo Ferraz de CamposII, VII; Luciano Miller Reis RodriguesII, V
IGrupo de Cirurgia da Coluna Vertebral, Centro Universitário FMABC - Santo André, São Paulo, Brasil
IILaboratório de Delineamento de Estudos e Escrita Científica, Centro Universitário FMABC - Santo André, São Paulo, Brasil
IIIPrograma de Pós-Graduação em Ciências Médicas, Faculdade de Medicina da Universidade de São Paulo (FMUSP) - São Paulo, São Paulo, Brasil
IVUniversidade Federal do Acre (UFAC) - Rio Branco, Acre, Brasil
VPrograma de Pós-Graduação em Ciências da Saúde, Centro Universitário FMABC - Santo André, São Paulo, Brasil
VIFaculdade Santa Maria - Cajazeiras, Paraíba, Brasil
VIIServiço de Neurocirurgia, Hospital Heliópolis - São Paulo, São Paulo, Brasil
ABSTRACT
INTRODUCTION: The spine is the most frequent area of bone metastasis in patients with systemic neoplastic disease. The goal of its treatment is immediate decompression, in order to prevent deterioration or reverse the deficit in neurological function
OBJECTIVE: To analyze the characteristics of the scientific literature on the effectiveness of surgery associated with radiotherapy to improve the neurological deficit caused by metastatic spinal cord compression
METHODS: Descriptive study based on bibliometric and scientometric methods. Using both, it is possible to qualify, verify and give meaning to the data and have, as a result, a broad study about the productions of the theme in question. Articles published in the National Library of Medicine (Pubmed), Web of Science and Virtual Health Library (VHL) were used, searched using keywords obtained from the Descriptors in Health Sciences (DeCS), of the VHL
RESULTS: The searches resulted in 131 articles. After filtering by reading titles, 100 articles were selected for reading the abstract. At the end of the collection, 15 articles were selected. Of these, the year of publication was distributed every two years for analysis, with a significant growth in 2015 and 2016. As for the origin of the studies, 60% (n = 9) had data collection developed in China, Japan or the United States of America. Regarding the gender of the sample, 57.14% of them contained the predominantly or totally male sample and 42.85% female. Regarding the histological type of tumor, there was a wide variation between studies. In some of them, the sample contained different groups of tumor diagnosis
CONCLUSION: The combination of surgery with postoperative radiotherapy proved to be effective and more efficient than these alone for the treatment of patients affected by metastatic neurological compression
Keywords: spinal cord compression, radiotherapy, surgery, neoplasm metastasis.
Authors summary
Why was this study done?
The study was carried out to exhaust the scientific literature regarding surgery associated with radiotherapy in patients suffering from metastatic spinal cord compression and to assist in the decision of oncology physicians and professionals in choosing the best treatment for the patient.
What did the researchers do and find?
The researchers carried out a descriptive study using bibliometric and scientometric methods and found that the combination of surgery with postoperative radiotherapy is effective and more efficient than these alone for the treatment of patients affected by metastatic neurological compression.
What do these findings mean?
Decompression surgery and postoperative radiotherapy was mostly palliative. Some factors such as individual treatment strategy, according to the histology of the primary tumor, plan of treatment strategies carried out in a multidisciplinary manner, risk-benefit of radiotherapy, assessment of the degree of spinal instability, improvement in communication and referral between specialists in oncology showed an increase in the survival of these patients. Furthermore, the combination of these treatments is effective and more efficient than these alone. These findings are important for cancer treatment planning and help professionals to seek greater survival.
INTRODUCTION
The spine is the most frequent area of bone metastasis in patients with systemic neoplastic disease1. Vertebral involvement in such patients is associated with worse morbidity and mortality rates, impairing prognosis and quality of life. Approximately half of patients with advanced malignancy have metastatic development in the spine2,3.
The evolution of cancer therapies provides greater survival for patients affected by metastatic lesions. More aggressive treatments aimed at the tumor cell, associated with efficient and less invasive surgical techniques are essential in this process. This improvement in survival has increased the diagnosis and monitoring of metastatic lesions in the spine, making spinal cord compression a more common clinical entity2.
Malignancy-Associated Spinal Cord Compression (MASC) is considered a serious oncologic emergency, in which breast, prostate, and lung cancers are the most common etiologies. In about 60 to 80% of patients with MASC there is involvement of the thoracic spine4. This condition causes, in addition to pain, hypercalcemia and pathological fracture, which can result in neurological deterioration5.
Treatment of spinal metastases depends on histology, site of disease, extent of epidural disease, extent of metastases elsewhere, and neurological status. Without immediate and adequate interventions, MASC can result in irreversible neurological deficits, such as motor and sensory dysfunctions and incontinence of feces and urine5,6.
Vertebral involvement in cancer patients is associated with worse morbidity and mortality rates, impairing prognosis. The quantification of vertebral involvement, vertebral canal invasion, presence of neurological compression, nerve status, general health status and prognosis malignancy, determined by the primary histology of the tumor, are some of the key factors for surgical planning and definition of therapeutic targets3,7.
Surgery and radiotherapy, or combinations of both, are the main treatment options for MASC. The main objective is the immediate decompression of the spinal cord, in order to prevent further deterioration or reverse the deficit in neurological function. For most solid tumors, except radiosensitive ones, surgery followed by radiotherapy has been shown to produce superior functional results compared to radiation treatment alone. Despite the effectiveness of surgery followed by palliative radiotherapy, which enables immediate decompression and facilitates the mechanical stabilization of the spine directly, it is performed in only 10-15% of these patients5,6,8.
Therefore, the aim of this study is to analyze the characteristics of the scientific literature regarding the effectiveness of surgery associated with radiotherapy to improve the neurological deficit caused by metastatic spinal cord compression.
METHODS
Descriptive study based on bibliometric and scientometric methods. Bibliometrics allows you to plan and find a certain number of journals that answer a specific question and critically analyze the studies available in the databases. Scientometrics has as its object of analysis the production, consumption and circulation of scientific production. Using both, it is possible to qualify, verify and give meaning to data and have, as a result, a broad study about the productions of the theme in question9.
The review was guided by a question developed in the format of a structured clinical question following the PICOS principle, which is "does the combination of surgery and radiotherapy improve the neurological deficit installed by metastatic neurological compression?". The following methodology was used: population of interest or health problem (P), which corresponds to patients who suffer metastatic neoplasia with spinal cord compression; intervention (I), radiotherapy and surgery; comparator (C), which does not apply; outcome (O), improvement of the neurological deficit; and study (S), all types of studies that met the eligibility criteria.
Primary research articles published in the last 10 years in all languages found were included. The bibliographic search was carried out in the Publisher Medline (PubMed), Virtual Health Library (VHL) and Web of Science electronic databases, using keywords obtained from VHL Descriptors in Health Sciences (DeCS) in August 2020.
In Pubmed, a search was performed using descriptors: Spinal Cord Compression AND Radiotherapy AND surgery AND Neoplasm Metastasis, with the filters "Humans" and "Free full text", excluding those studies that were not performed with a human sample and those that are paid and/or difficult to access. In Web of Science, "Topic" and document types (open access) were searched with the same descriptors and in the VHL it was searched for title, abstract and subject, with the same descriptors.
For the selection of articles, three steps were used: (I) search for evidence in the databases; (II) exclusion of those in duplicates and revisions, (III) reading of titles and abstracts, with analysis of eligibility criteria; and (IV) full text analysis of eligible papers. All studies that met the inclusion criteria and did not have any of the exclusion criteria were included.
Published studies were eligible when meeting the criteria: (1) study population diagnosed with neoplastic cancer, (2) the entire sample with metastatic neurological compression, (3) at least part of the sample underwent a combination of surgery and radiotherapy. There were no restrictions on sample size. Articles were excluded if: (1) They used secondary databases (books, theoretical works or secondary reviews), (2) used populations not explicitly identified with metastatic cancer, (3) had radiosurgery as therapeutic intervention, (4) performed minimally invasive procedures, (5) non-original articles, such as editorials and comments, (6) those in which no part of the sample underwent surgery and (7) no part of the sample underwent radiotherapy.
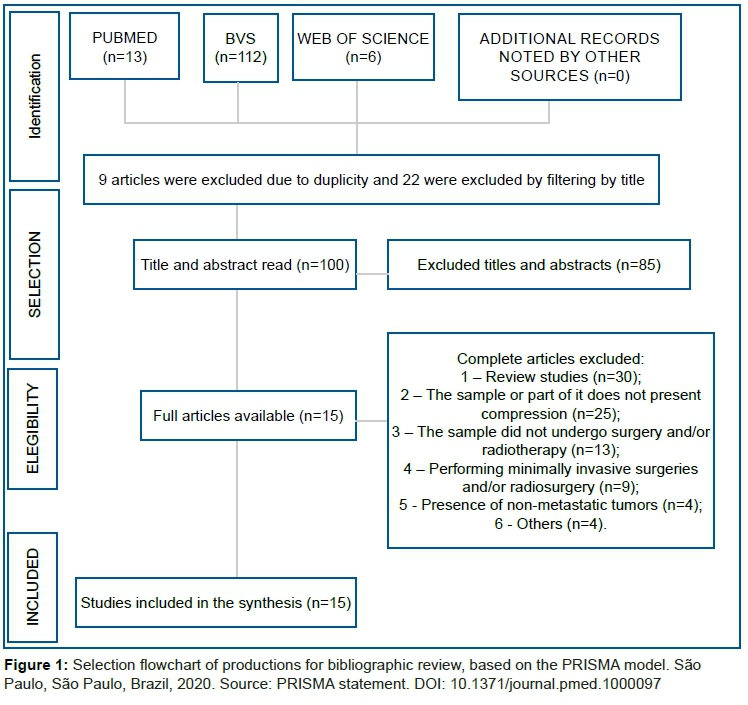
The flowchart shown in figure 1 shows the path taken to select publications. The steps of identification, selection, eligibility, inclusion and extraction of data were developed in a dual and independent way. Disagreements were decided by a third reviewer. The qualitative synthesis step was developed by the review team.
The productions that were repeated were considered only once. The retrieval of articles was performed in the database itself and, when unavailable, through the Journal Portal of the Coordination for the Improvement of Higher Education Personnel (Capes), on the journal's website, or by requesting the manuscript to the main author.
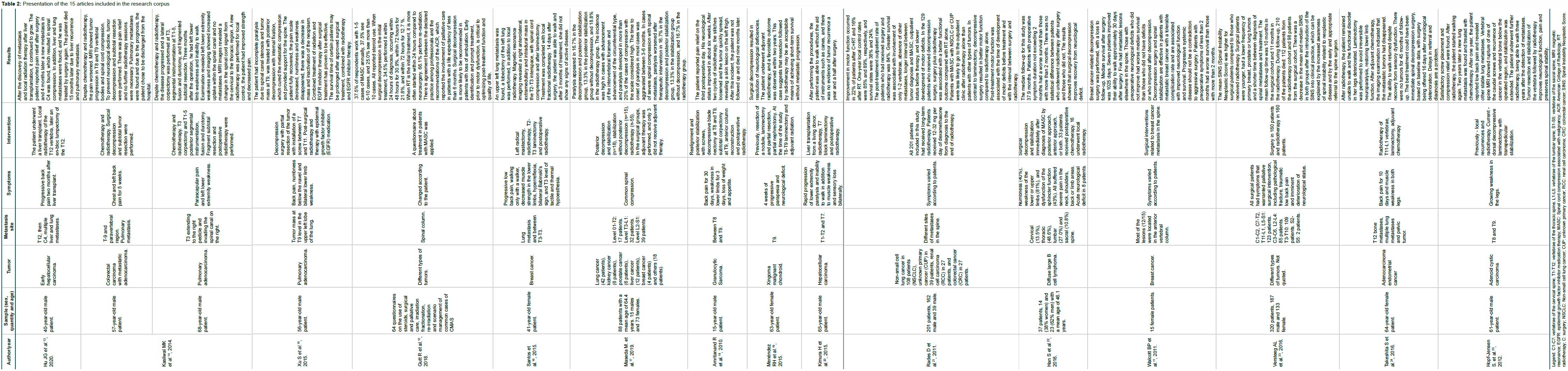
Fifteen articles were analyzed, from which the following information was extracted: reference, year of publication, journal, country in which it was carried out, type of study, area of knowledge, titles/professional training of authors, institutions to which the authors were linked, origin of the study, objectives, sample, type of tumor, location of metastasis, location of compression, symptoms, intervention, study design and main results.
All information extracted respected ethical aspects, reliably presented, cited and described, according to the ideas, definitions and concepts used by the authors of the articles.
RESULTS
Searches carried out in the databases resulted in 131 articles. After filtering by reading titles, 100 articles were selected for reading the abstract. At this stage, studies were excluded mainly because they were review studies, because the sample did not have patients with compression and because they did not undergo surgery and/or radiotherapy. At the end of the collection, 15 articles were selected.
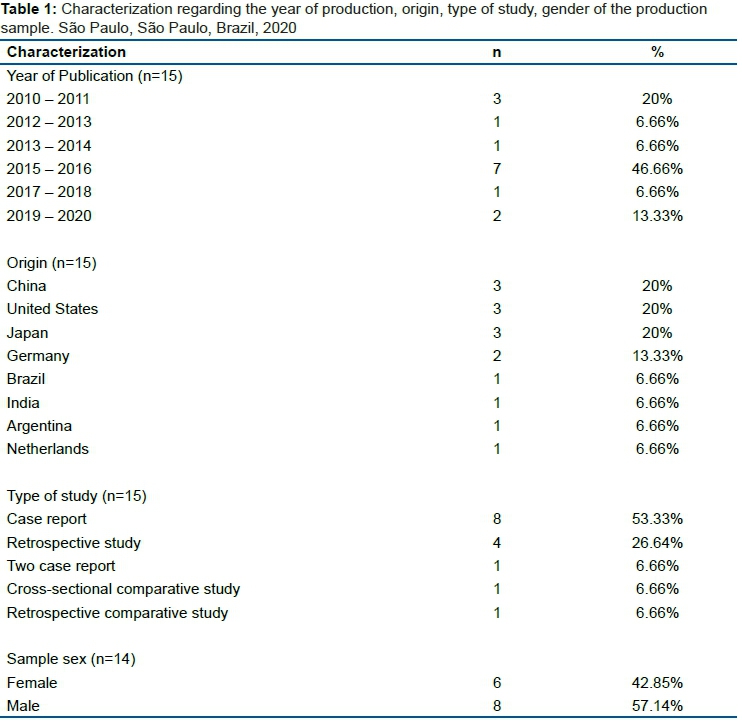
Of the articles analyzed, the year of publication was distributed every two years for analysis, with a significant growth in the year 2015 and 2016. As for the origin of the studies, 60% (n=9) had data collection developed in China, Japan or the United States of America. As for the types of studies found, most are case reports. Although reviews of randomized clinical trials are frequent, there is an increasing number of reviews prepared based on observational investigations, such as cohort, case-control, cross-sectional, series and case reports10.
Regarding the gender of the sample of 14 studies, 57.14% of them contained the predominantly or totally male sample and 42.85% female. This result may have limitations because the study by Walcott BP et al.11 had a limited sample only in patients undergoing spinal surgery due to metastasis caused by breast cancer, which is prevalent in women. The study by Gutt R et al.12 was not specifically included in this analysis because its sample consisted of questionnaires answered by health professionals. All this information was arranged in table 1.
Regarding the histological type of tumor, there was a wide variation between studies. In some of them, the sample contained different groups of tumor diagnosis. These and other characteristics can be observed and compared in table 2.
DISCUSSION
In this study we found that the purpose of decompression surgery and postoperative radiotherapy is palliative. Some factors, such as an individual treatment strategy, according to the histology of the primary tumor, a multidisciplinary plan, risk-benefit assessment and the degree of spinal instability, improve communication and referral between specialists. Furthermore, the combination of surgery with postoperative radiotherapy proved to be effective and more efficient than these isolated treatments for the treatment of patients affected by metastatic neurological compression.
Spinal metastases are common in patients with cancer. The interventions aim to significantly improve the quality of life, reducing pain, avoiding the harm that compression can cause and maintaining neurological function and mechanical stability. The average survival time of those with bone metastases has increased substantially in recent decades thanks to advances in cancer treatment options. Factors such as non-surgical intervention and misdosing are related to an unfavorable neurological outcome14,23,24.
Palliative radiotherapy for the treatment of bone metastases is a clinically effective option for patients with spinal metastases considered unsuitable for surgery, although radiotherapy alone is often not able to control tumor progression. Although possible, surgical intervention for patients with spinal tumor progression is hampered due to prior radiation, along with an increased risk of infection13.
Treatment of hepatocellular carcinoma by liver transplantation is considered effective. In the report by Hu JG et al.13, after the procedure, the patient was diagnosed with metastasis in the T12 vertebra. Immediate surgical intervention was not indicated due to decreased liver function. Local radiotherapy was performed, which resulted in a decrease in symptoms. The size of the lesion increased, indicating progressive disease and, therefore, the patient was treated with an en bloc lumpectomy. One month after surgery, a C4 metastasis with spinal cord compression was found, in addition to multiple liver and lung metastases. After resection, without the presentation of new secondary tumors, the patient died 15 months after transplantation due to liver recurrence and lung metastases. The authors further state that en bloc lumpectomy may be a viable therapeutic option for patients with progression of solitary vertebral metastases after transplantation.
In a report of two cases of spinal cord compression due to metastases from different tumors, carried out in the United States, it was found that surgical intervention produces improvement in pain and in the quality of life of patients with symptomatic spinal metastases. Increasing awareness of uncommon or rare complications is essential in preventing and managing the disease. The authors state that the objective of surgery in the treatment of vertebral metastases is to reduce pain and maintain neurological function and vertebral stability. The decision to proceed with the surgery must be determined in an interdisciplinary consultation14.
The cases presented suggest that patients with unintentional durotomy during surgery for extradural resection should be monitored for recurrence of intradural tumors by early imaging. Durotomy during surgery for metastatic tumors can have unique complications compared to those during surgery to treat degenerative disorders14.
The patient diagnosed and treated by Xu S. et al.15 underwent surgery for decompression and internal fixation, postoperative radiation and medication that inhibits the epidermal growth factor (EGFR). After 24 months, examinations showed a reduction in mass and inactivation of the neoplasm of the left upper lobe and T9 vertebra. It is important that orthopedic oncologists consider combining radiotherapy and EGFR inhibitor therapy with surgery for the treatment of compressive lung cancer metastasis in the spine. The survival time of certain patients may be prolonged after surgical treatment combined with radiotherapy and EGFR inhibitor therapy.
A survey that included questions about steroid use, surgical care, palliative care, irradiation fractionation, re-irradiation, and management of common case scenarios of MASC was conducted. Of the professionals interviewed, 37.5% see 1-5 cases annually, 37.5% see 6-10 cases, and 25.0% see more than 10 cases per year. All respondents reported using steroid therapy. When surgical decompression is the initial treatment, 34.5% are performed within 24 hours of diagnosis, within 48 hours for 30.9%, within 72 hours for 21.8% and within 72 hours for 12.7 % of respondents12.
When radiotherapy is the recommended initial treatment, it is started within 24 hours in 83.9%, within 48 hours for 12.9%, and within 72 hours for 3.2% of respondents. 66.1% perform re-radiation. When necessary, radiotherapy is often started within 24 hours compared to neurosurgery. The study still briefly reports some cases to professionals. In the first, a 60-year-old woman with good loss of performance and ambulation. In relation to it, 93.4% of respondents selected surgical decompression followed by radiotherapy12.
For the second scenario, a 60-year-old woman with good performance, symptoms of back pain and paresthesia. The majority (75.8%) selected surgical decompression followed by radiotherapy again. For the third scenario, a 60-year-old woman with good performance and mild lower extremity weakness secondary to multiple myeloma, only 18.3% selected the option of surgical decompression followed by radiotherapy. As recommended by the ACR (American College of Radiology) guidelines, all respondents recommended the use of steroids12.
In accordance with the ACR guidelines, all respondents reported involvement of palliative care in patients with a life expectancy of less than six months. The responses to the case scenarios demonstrate that surgical decompression is more likely to be recommended for those with loss of ambulation. Early identification of MASC and prompt treatment, before the onset of motor dysfunction, is essential to improve post-treatment function and quality of life12.
In Brazil, a 28-year-old female patient was diagnosed with breast ductal adenocarcinoma. She underwent left radical mastectomy with lymphadenectomy, followed by chemotherapy and local radiotherapy. With 10 years of follow-up, she had pulmonary metastasis on CT scan. A lobectomy of the left lung and local radiotherapy were performed. Magnetic resonance imaging revealed an extramedullary and intradural metastatic mass in the T2-T3 interspace, with spinal cord compression. Laminectomy treatment was completed with local radiotherapy, started 10 days after surgery. 14 days later the patient was able to walk and after 3 months she had no signs of active disease. Thus, Santos et al.16 states that the purpose of surgery should be strictly palliative with the intention of reducing pain and neurological deficits.
Difficulty in re-covering complete spinal cord paralysis has been reported, therefore tumor-induced metastatic cord paralysis should be treated as soon as possible before it becomes irreversible. Early therapeutic intervention has been performed to prevent skeletal-related events (SREs), such as paralysis and pathological fracture. One study included 88 patients with epidural spinal cord compression who were separated by therapeutic intervention, being a decompression and posterior stabilization group (n = 18), a posterior stabilization group without decompression (n = 15), and another radiotherapy group (n=55). In the surgical groups (n = 33), adjuvant therapy, such as postoperative radiotherapy, chemotherapy and treatment with bone modifying agents, was properly performed, and only three patients did not undergo it17.
Surgery was prioritized when pain from spinal instability was severe. However, there were no clear criteria for selecting treatment methods. In cases of severe spinal compression with spinal metastasis, paralysis worsened after therapeutic intervention in 16.7% in the decompression and posterior stabilization group, 13.3% in the stabilization group without decompression, and 16.7% in the radiotherapy group. It was found that in patients with more severe symptoms, such as paralysis and pathological fracture, the treatment of surgery and post-surgical radiotherapy started earlier17.
In the case report carried out by Amritanand R et al.18, a mass was found that caused spinal compression in a 15-year-old patient with back pain and weakness of the lower limbs. The diagnosis was granulocytic sarcoma, which, when originated from the vertebral column, can cause spinal cord compression and neurological deficits. Although this is radiosensitive, there is a risk of wound breakage, as seen in this patient. He had dorsal compression and a mechanically unstable spine due to a pathological dislocation.
Surgical goals were canal decompression, tumor removal, spinal alignment stabilization, and reconstruction to allow rapid ambulation. The patient underwent posterior realignment and stabilization with pedicle screws, decompressive blade nectomy of the T8 and T9 vertebrae, subtotal corpectomy of the T9 vertebra, and reconstruction of the anterior column with a titanium cage. The patient reported substantial pain relief, improvement in neurological deficit and was able to walk independently within 4 weeks after surgery. After two cycles of radiotherapy, the stitches loosened, and the tumor rapidly spread. A skin lesion was noted on the left thigh. The patient decided not to follow up and died 9 months later. Therefore, an early diagnosis is necessary, in addition to surgical intervention adapted to the patient's presentation, followed by appropriate chemotherapy and radiotherapy. The potential for wound rupture after radiotherapy must be taken into account18.
In 1990, a patient underwent resection of a subcutaneous nodule in the epigastrium, with a diagnosis of malignant chondroid xaringoma. Seven years later, the tumor rescinded in the same location and was removed again. In 2004, the tumor returned again and a liver metastasis was found. She underwent left hepatic lobectomy and partial resection of the thoracoabdominal wall with thoracoplasty. One year later a mass was found in the right kidney and a partial nephrectomy was performed, which was again consistent with malignant chondrodoma. An infiltrating tumor was found in the left pedicle of T-9 that could not be completely resected. After the discovery of neurological compression at T8-9, a laminectomy was performed, the mass was removed, and the medulla decompressed. Therefore, liver and kidney metastases were discovered 14 and 15 years after removal of the primary spinal tumor and 21 years after excision of the skin tumor19.
The main treatment options for spinal metastases are radiotherapy and surgery, the latter of which may be the best option in cases of neurological deterioration caused by spinal metastases. In Japan, a man diagnosed with hepatocellular carcinoma underwent a liver transplant from a living donor and experienced pain 3 years later. New metastases were found in the thoracic spine. Corpectomy, T7 block laminectomy and postoperative radiotherapy were performed. After performing the procedures, the patient was able to walk without the cane, and there was no evidence of recurrence in 1.5 years of follow-up20.
In the study by Rades D. et al.21, an investigation was carried out to find out whether decompression surgery associated with postoperative radiotherapy treatment was superior or inferior to radiotherapy alone in patients with metastatic spinal cord compression. Improvement in motor function, outpatient post-processing rates and recovery of neurological status occurred more frequently in those who underwent both procedures. One-year spot control rates were 85% and 89%. Non-small cell lung cancer (NSCLC) and unknown primary cancer (CUP) were associated with lower outpatient rates after radiotherapy alone. A higher survival rate was found in the group that received both treatments. Those with involvement of only one or two vertebrae had better performance, longer interval between tumor diagnosis and neurological compression.
In the subgroup analysis of 129 patients that decompressive surgery with stabilization of the involved vertebrae (DDSS) plus radiotherapy (RT) (n = 43) was associated with a significantly better functional outcome compared with RT alone (n = 86). The data from the present analysis revealed a trend towards better outcomes after radiotherapy alone compared with laminectomy plus radiotherapy. In contrast to laminectomy, DDSS resulted in significantly better motor function compared to radiotherapy alone. Post-treatment motor function was significantly associated with the time of development of motor deficits before treatment and with the interval between surgery and radiotherapy21.
A retrospective study was carried out in a sample of 37 individuals to investigate the impact of surgical decompression on the recovery of neurological deficit caused by diffuse large B cell lymphoma (DLBCL) over an 11-year period. The main clinical features included numbness, weakness of the lower or upper limbs, and dysfunction of the sphincter function. All patients suffered from severe pain within the neck, shoulders, back or limb areas and 8 had acute neurological deficit. Surgical decompression and stabilization were performed immediately after the diagnosis of metastatic neurological compression. Postoperatively, 33 received chemotherapy and 16 underwent local radiotherapy22.
The authors claim that the combination of chemotherapy and radiotherapy is effective in managing metastatic neurological compression. However, surgical treatment should be considered in case of acute vertebral collapse, if diagnosis is uncertain and biopsy is required, or deterioration of neurological symptoms. The results demonstrated that surgical decompression improves recovery from neurological deficit. Those with preoperative symptom duration not exceeding 2 months had a worse prognosis. Surgical decompression could improve recovery from neurological deficit in patients with metastatic neurological compression associated with DLBCL22.
Among breast cancer patients, the spine is the most common site for skeletal metastases. About half develop pain or neurological deficits or spinal cord compression, or both. In the study by Walcott BP et al.11, 14 patients underwent open surgery for the treatment of breast cancer metastases in the spine. Median survival was 1025 days; systemic disease control did not predict survival duration. Half of the sample had an improvement in their ability to walk in the first 30 days after surgery.
The authors reveal that aggressive therapy, including surgery, is warranted for patients with symptomatic metastatic spinal cord compression from breast cancer, even in the setting of advanced and progressive systemic disease. Decompression surgery and spinal stabilization are effective in patients with metastatic breast cancer to the spine with a tolerable rate of complications and are associated with proven neurological function and overall survival. Although stereotaxic radiosurgery is also used to treat metastatic spinal tumors with favorable results, it has not been shown to be superior to surgery in the immediate treatment of a compression syndrome11.
A retrospective study contained all patients with spinal metastases treated with palliative surgery or radiotherapy in the period 2009-2013 at two spinal centers. Treatment was multidisciplinary and assessment of spinal instability was just one of several factors that should be considered. The SINS (Spinal Instability Neoplastic Score) help physicians who treat patients with metastatic disease to identify spinal instability before the onset of neurological deficits. The study demonstrated that its introduction into routine clinical practice led to a decrease in spinal instability in radiotherapy and in the surgical cohort. The decrease in the score can be explained by the increased awareness of spinal instability related to the neoplasm and by the early and appropriate referral to the spine surgeon23.
In Japan, despite the completion of radiotherapy, one patient remained unable to walk and the functional impairment of her legs increased. Laminectomy was performed 19 days after admission, restoring lower limb function and the ability to walk in a wheelchair. After three courses of adjuvant chemotherapy, CT scan indicated that all metastatic tumors had disappeared. She regained the ability to walk and remained tumor free after 45 months of follow-up. Despite this, the sensory dysfunction was still recovering. The patient was offered spinal decompression surgery 16 days after neurological deterioration. The best treatment could have been immediate spinal decompression surgery, it is important to avoid delays in referral and diagnosis for a better prognosis24.
According to the report by Hopf-Jensen S. et al.25, in 2000 the patient had been treated for adenoidcystic paracarcinoma (ACC) of the maxillary sinuses, and for local recurrences in 2002 and 2005, followed by radiotherapy. Years later, a metastatic osteolytic disease was found in T8 and T9, associated with an epidural soft tissue mass, and spinal cord compression. The patient was immediately referred to the hospital and a dorsal decompressive laminectomy was performed with stabilization from T6 to T11. The patient recovered and was mobilized in the ward.
Postoperative radiotherapy was started, and the patient managed his daily activities, being able to maintain his balance when walking, climbing stairs and swimming. Two years later, lung metastases were found, which were treated with chemotherapy. One year later, the patient was readmitted to the emergency room with low back pain and stable lung metastases were found. Magnetic resonance imaging of the spine showed a rupture of one of the caudal screws and recurrence of cancer in the vertebral bone below the operated region. In an additional surgery, stabilization was extended, and more radiotherapy fractions were performed. The patient was able to walk three years after the detection of metastases. Therefore, tumor resection and stabilization of the vertebral elements, followed by external beam radiotherapy, improve neurological function and pain and preserve spinal stability25.
By surgically restoring the mechanical needs of vertebral elements destroyed by cancer, pain is often reduced, and mobility increased. Although stereotaxic radiosurgery is also used to treat metastatic spinal tumors with favorable results, in some studies it has not been shown to be superior to surgery in the immediate treatment of a compression syndrome, when compared to surgery. Stereotactic radiosurgery for the treatment of spinal metastases has been specifically studied and considered effective and remains an option for the control of tumors in patients who choose not to undergo surgery or are considered as non-suitable surgical candidates11, there may also be a role for radiosurgery after decompression surgery, but this type of treatment was not studied in this review.
CONCLUSION
The purpose of decompressive surgery and postoperative radiotherapy were mostly palliative. Some factors such as individual treatment strategy according to the histology of the primary tumor, plan of treatment strategies carried out in a multidisciplinary manner, risk-benefit of radiotherapy, assessment of the degree of spinal instability, improvement in communication and referral between specialists in oncology showed an increase in the survival of these patients. The combination of surgery with postoperative radiotherapy proved to be effective and more efficient than these isolated treatments for the treatment of patients affected by metastatic neurological compression.
Authors' Contributions:
All authors contributed to the conception and design of the study. Material preparation, data collection and analysis were carried out by MJD, ORN and GAVP. The first draft of the manuscript was written by ORN and GAVP. All authors commented on previous versions of the manuscript, read and approved the manuscript.
Financing
Not Applicable.
Acknowledgments:
We thank the Health Department of the State of Acre (SESACRE), Acre, Brazil; the Federal University of Acre (UFAC), Acre, Brazil and the Centro Universitário FMABC, Santo André, São Paulo, Brazil; for the opportunity and training of masters and doctors and researchers in the health area through the agreement 007/2015 - SESACRE/UFAC/FMABC) and all researchers, undergraduate, masters and doctoral students of the Study Design and Scientific Writing Laboratory of the FMABC University Center that enabled the development of research and science in the Western Amazon, Brazil.
Conflicts of Interest:
Not Applicable.
REFERENCES
1.Harrington KD. Current concepts review. Metastatic disease of the spine. Journal of Bone and Joint Surgery - Series A. 1986; 68(7): 1110-5. [ Links ]
2.Rodrigues LMR, Filho ESV, Ueno FH, Fujiki EN, Milani C. Qualidade de vida de pacientes submetidos Á descompressão por lesão vertebral metastática. Acta Ortopedica Brasileira [Internet]. 2011 [cited 2021 Jun 23]; 19(3): 149-53. Available from: http://www.scielo.br/aob [ Links ]
3.Oliveira MF de, Rotta JM, Botelho RV. Survival analysis in patients with metastatic spinal disease: the influence of surgery, histology, clinical and neurologic status. Arquivos de Neuro-Psiquiatria. 2015; 73: 330-5. [ Links ]
4.Prasad D, Schiff D. Malignant spinal-cord compression. The Lancet Oncology [Internet]. 2005 Jan [cited 2021 Jun 23]; 6(1): 15-24. Available from: http://linkinghub.elsevier.com/retrieve/pii/S1470204504017097 [ Links ]
5.Lo SSM, Lutz ST, Chang EL, Galanopoulos N, Howell DD, Kim EY, et al. ACR appropriateness criteria® spinal bone metastases [Internet]. Vol. 16, Journal of Palliative Medicine. J Palliat Med; 2013 [cited 2021 Jun 23]. p. 9-19. Available from: https://pubmed.ncbi.nlm.nih.gov/23167547/ [ Links ]
6.Akram H, Allibone J. Spinal surgery for palliation in malignant spinal cord compression. Clinical Oncology [Internet]. 2010 Nov [cited 2021 Jun 23];22(9):792-800. Available from: https://pubmed.ncbi.nlm.nih.gov/20702075/ [ Links ]
7.Fehlings MG, David KS, Vialle L, Vialle E, Setzer M, Vrionis FD. Decision making in the surgical treatment of cervical spine metastases. [Internet]. Vol. 34, Spine. Spine (Phila Pa 1976); 2009 [cited 2021 Jun 23]. Available from: https://pubmed.ncbi.nlm.nih.gov/19829270/ [ Links ]
8.Chang CM, Chen HC, Yang Y, Wang RC, Hwang WL, Teng CLJ. Surgical decompression improves recovery from neurological deficit and may provide a survival benefit in patients with diffuse large B-cell lymphoma-associated spinal cord compression: A case-series study. World Journal of Surgical Oncology [Internet]. 2013 Apr 19 [cited 2021 Jun 23]; 11. Available from: https://pubmed.ncbi.nlm.nih.gov/23601178/ [ Links ]
9.BIBLIOMETRIA, CIENTOMETRIA, INFOMETRIA: CONCEITOS E APLICAÇÕES [Internet]. [cited 2021 Jun 23]. Available from: https://brapci.inf.br/index.php/res/v/119278 [ Links ]
10.10. Galvão TF, Pereira MG. Revisões sistemáticas da literatura: passos para sua elaboração. Epidemiologia e Serviços de Saúde. 2014 Mar;23(1): 183-4. [ Links ]
11.Walcott BP, Cvetanovich GL, Barnard ZR, Nahed B V., Kahle KT, Curry WT. Surgical treatment and outcomes of metastatic breast cancer to the spine. Journal of Clinical Neuroscience [Internet]. 2011 [cited 2021 Jun 23]; 18(10): 1336-9. Available from: https://pubmed.ncbi.nlm.nih.gov/21782449/ [ Links ]
12.Gutt R, Malhotra S, Jolly S, Moghanaki D, Cheuk A V., Fosmire H, et al. Management of metastatic spinal cord compression among veterans health administration radiation oncologists. Annals of Palliative Medicine [Internet]. 2018 Apr 1 [cited 2021 Jun 23]; 7(2): 234-41. Available from: https://pubmed.ncbi.nlm.nih.gov/29764185/ [ Links ]
13.Hu JG, Lu Y, Lin XJ. En Bloc lumpectomy of T12 vertebra for progressive hepatocellular carcinoma metastases following liver transplantation: A case report. Medicine (United States) [Internet]. 2020 Jan 1 [cited 2021 Jun 23]; 99(2). Available from: https://pubmed.ncbi.nlm.nih.gov/31914098/ [ Links ]
14.Kasliwal MK, Tan LA, O'Toole JE. Intradural tumor recurrence after resection of extradural metastasis: A rare but potential complication of intraoperative durotomy: Report of 2 cases. Journal of Neurosurgery: Spine [Internet]. 2014 [cited 2021 Jun 23]; 20(6): 734-9. Available from: https://pubmed.ncbi.nlm.nih.gov/24725179/ [ Links ]
15.Xu S, Yu X, Xu M. Long-term survival of a patient with lung cancer metastasis to the spine following surgical treatment combined with radiation and epithelial growth factor receptor inhibitor therapy: A case report. Experimental and Therapeutic Medicine [Internet]. 2015 Jan 1 [cited 2021 Jun 23]; 9(1): 117-9. Available from: https://pubmed.ncbi.nlm.nih.gov/25452785/ [ Links ]
16.Gonçalves V, Santos D, Alves De Carvalho Cavalcante R, Alberto R, Marques S, Zaccariotti VA. Metástase espinhal intradural e extramedular: relato de caso Intradural and Extramedular Spinal Metastases: Case Report. 2014 [cited 2021 Jun 23]; Available from: http://dx.doi.org/ [ Links ]
17.Maseda M, Uei H, Nakahashi M, Sawada H, Tokuhashi Y. Neurological outcome of treatment for patients with impending paralysis due to epidural spinal cord compression by metastatic spinal tumor. Journal of Orthopaedic Surgery and Research [Internet]. 2019 Sep 3 [cited 2021 Jun 23]; 14(1). Available from: /pmc/articles/PMC6724255/ [ Links ]
18.Amritanand R, Venkatesh K, Premkumar AJ, Sundararaj GD. Pathological dislocation of the dorsal spine following granulocytic sarcoma in a non-leukaemic patient. European Spine Journal [Internet]. 2010 [cited 2021 Jun 23]; 19(SUPPL.2). Available from: https://pubmed.ncbi.nlm.nih.gov/19688354/ [ Links ]
19.Menéndez RH, Erice SG, Bas CA, Casas G, Dillon HS. Spinal cord compression secondary to metastasis of malignant chondroid syringoma: Case report. Journal of Neurosurgery: Spine [Internet]. 2015 Mar 1 [cited 2021 Jun 23]; 22(3): 310-3. Available from: https://pubmed.ncbi.nlm.nih.gov/25555054/ [ Links ]
20.Tomita K, Kawahara N, Baba H, Tsuchiya H, Fujita T, Toribatake Y. Total en bloc spondylectomy: A new surgical technique for primary malignant vertebral tumors. Spine [Internet]. 1997 Feb 1 [cited 2021 Jun 23]; 22(3): 324-33. Available from: https://pubmed.ncbi.nlm.nih.gov/9051895/ [ Links ]
21.Rades D, Huttenlocher S, Bajrovic A, Karstens JH, Adamietz IA, Kazic N, et al. Surgery followed by radiotherapy versus radiotherapy alone for metastatic spinal cord compression from unfavorable tumors. International Journal of Radiation Oncology Biology Physics [Internet]. 2011 Dec 1 [cited 2021 Jun 23]; 81(5). Available from: https://pubmed.ncbi.nlm.nih.gov/21277114/ [ Links ]
22.Han S, Yang X, Jiang D, Zhou W, Liu T, Yan W, et al. Surgical outcomes and prognostic factors in patients with diffuse large b-cell lymphoma-associated metastatic spinal cord compression. Spine [Internet]. 2016 Aug 1 [cited 2021 Jun 23]; 41(15): E943-8. Available from: https://pubmed.ncbi.nlm.nih.gov/26890958/ [ Links ]
23.Versteeg AL, Velden JM, Verkooijen HM, Vulpen M, Oner FC, Fisher CG, et al. The Effect of Introducing the Spinal Instability Neoplastic Score in Routine Clinical Practice for Patients With Spinal Metastases. The Oncologist [Internet]. 2016 Jan 14 [cited 2021 Jun 23]; 21(1): 95-101. Available from: http://dx.doi.org/10.1634/theoncologist.2015-0266 [ Links ]
24.Takeshita S, Todo Y, Okamoto K, Minobe S, Kato H. Thoracic laminectomy with spinal fixation in a nonambulatory patient with metastatic vertebral tumor from endometrial carcinoma. Journal of Obstetrics and Gynaecology Research [Internet]. 2016 Oct 1 [cited 2021 Jun 23]; 42(10): 1395-9. Available from: https://pubmed.ncbi.nlm.nih.gov/27277163/ [ Links ]
25.Hopf-Jensen S, Buchalla R, Rubarth O, Peters J, Dunker H, Hensler HM, et al. Unusual spinal metastases from an adenoid cystic carcinoma of the maxillary sinus. Journal of Clinical Neuroscience. 2012 May 1; 19(5): 772-4. [ Links ]
 Correspondence:
Correspondence:
Oswaldo Roberto Nascimento
oswaldoroberto@uol.com.br
Manuscript received: March 2021
Manuscript accepted: May 2021
Version of record online: July 2021


{kind=link}
{kind=link}
{kind=link}