










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282On-line version ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.3 Santo André Sep./Dec. 2021
http://dx.doi.org/10.36311/jhgd.v31.12605
ORIGINAL ARTICLE
DOI: 10.36311/jhgd.v31.12605
COVID-19 mortality and lethality in the state of Pará, legal Amazon, Brazil
Célia Guarnieri da SilvaI, II; Luiz Vinicius de Alcantara SousaIII; Laércio da Silva PaivaIII; Tassiane Cristine MoraisII, V; Mariane Albuquerque Lima RibeiroI, IV; Maura Regina RibeiroII; Carlos Bandeira de Mello MonteiroII, VI
IPrograma de Pós-Graduação em Ciências da Saúde, Centro Universitário FMABC - Santo André, São Paulo, Brazil
IILaboratório de Delineamento de Estudo e Escrita Científica, Centro Universitário FMABC - Santo André, São Paulo, Brazil
IIILaboratório de Epidemiologia e Análise de Dados, Centro Universitário FMABC - Santo André, São Paulo, Brazil
IVCentro de Ciências da Saúde e do Desporto, Universidade Federal do Acre - Rio Branco, Acre, Brazil
VDepartamento de Educação Integrada em Saúde, Universidade Federal do Espírito Santo - Vitória, Espírito Santo, Brazil
VIEscola de Artes, Ciências e Humanidades da Universidade de São Paulo (EACH-USP), Departamento de Pós-Graduação em Ciências da Reabilitação - São Paulo, São Paulo, Brazil
ABSTRACT
INTRODUCTION: the growth of coronavirus indices in the North region highlights the region's historical social inequalities and the problems in accessing citizenship.
OBJECTIVE: to analyze the mortality and lethality of COVID-19 in the state of Pará, Brazil.
METHODS: this is an ecological study with a time series design of secondary data. All registered cases and deaths reported by COVID-19 in the period from March 2020 to June 2021, in the state of Pará, Brazil, were considered. The incidence and mortality and lethality rates were used. The daily percentage variation and their respective 95% confidence intervals were estimated.
RESULTS: the total number of confirmed cases and deaths from COVID-19 in the state of Pará was 552,937 and 15,469, respectively, from March 2020 to June 2021. Incidence and mortality rates from March 2020 to June 2021 were, respectively, 6,407.9 and 179.3 per 100,000 inhabitants and the lethality was 43.3. Regarding the analysis of the daily trend of rates in the period from March 2020 to June 2021, both mortality and incidence increased.
CONCLUSION: it was found that the behavior of the trend of rates in the first wave was increasing in the incidence of confirmed cases and the lethality decreasing, and in the second wave, the mortality and lethality rates were increasing.
Keywords: COVID-19, SARs-CoV-2, mortality, lethality, lockdown, quarantine.
Authors summary
Why was this study done?
The purpose of the study is to analyze temporal variations in mortality and lethality from COVID-19 in the state of Pará, North region, Brazil.
What did the researchers do and find?
The trend of rates in the first period (March to November 2020) was increasing in the incidence of confirmed cases and lethality decreasing, and in the second period (December 2020 to June 2021), mortality and lethality rates were increasing.
What do these findings mean?
The contribution of this analysis supports preventive actions, control and treatment, reduction of mortality and definition of priorities within the area of public health.
INTRODUCTION
In the year 2020, an outbreak of the new Coronavirus in China became an international public health problem. In a short period, a pandemic was declared with different impacts signaled by the World Health Organization (WHO). COVID-19 had a remarkable impact on global economic development, harmed health systems, the political and social field1.
Approximately 180 million cases have been registered around the world. South America was recently declared by the World Health Organization as a new epicenter of the SARS-CoV-2 pandemic2.
The Unified Health System (SUS), despite the hospital and health crisis, guarantees access to millions of inhabitants, in person and digitally, developing an artificial intelligence system for non-presential care. Despite all measures, the pandemic had a profound impact on the Brazilian population, especially its population in a vulnerable situation, aggravated by the high rate of unemployment3. With death records exceeding 500 thousand victims of the disease, the lack of control of the pandemic in the country is worrying4. It began in 2021 without effective intervention measures, strategies for health promotion and combating the virus, overloading the hospital system, general beds, and intensive care units (ICU)5.
One of the concerns linked to the COVID-19 pandemic refers to the capacity of the health system structure to support the demand for care and treatment of people affected by this disease6.
In Brazil, one of the countries most affected by the COVID-19 pandemic, mortality data do not reflect the actual number of deaths from the disease. Between February 23 and August 8, 2020, 46,028 deaths from respiratory causes were recorded in the eight cities (Rio de Janeiro, São Paulo, Manaus, Belém, Fortaleza, Recife, Cuiabá, and Curitiba). The high and heterogeneous percentage of excess respiratory deaths suggests high underreporting of deaths from COVID-19, reinforces regional inequalities and the need to review deaths associated with respiratory symptoms6,7.
The growth of coronavirus indices in the North region, therefore, highlights the historical social inequalities of the region and the problems in accessing citizenship8.
With few epidemiological studies in the northern region of Brazil, the gaps in information on the epidemiology of COVID-19 show the highest incidence rates of COVID-19 in this region9,10. The Northern region took the third place early in the COVID-19 pandemic outbreak, with confirmed cases at approximately 16% as of May 5, 202011.
In the State of Pará, 4,756 cases were registered, with an incidence rate of 788 cases in 49 days after confirmation of the first COVID-19 infection. The first confirmed case of the disease was reported on March 18, 2020, in the city of Belém, capital of the state. The first notification of death occurred on April 1, 2020, and since then the curve of new cases and incidence of deaths has been frequent and recorded with high rates in the region11.
The investigation and characterization of epidemiological aspects, analyzing the temporal variations of COVID-19 mortality and lethality in the North region to understand the disease behavior in the population of the State of Pará, can lead to timely and adequate interventions for the prevention of worse outcomes.
Therefore, the objective is to analyze the mortality and lethality of COVID-19 in the state of Pará, Brazil.
METHODS
This is an ecological study conducted according to the protocol proposed by Abreu, Elmusharaf and Siqueira (2021)12, using time series of public and official data available on the website of the Department of Health of the State of Pará, Brazil (https://www.covid-19.pa.gov.br/#/).
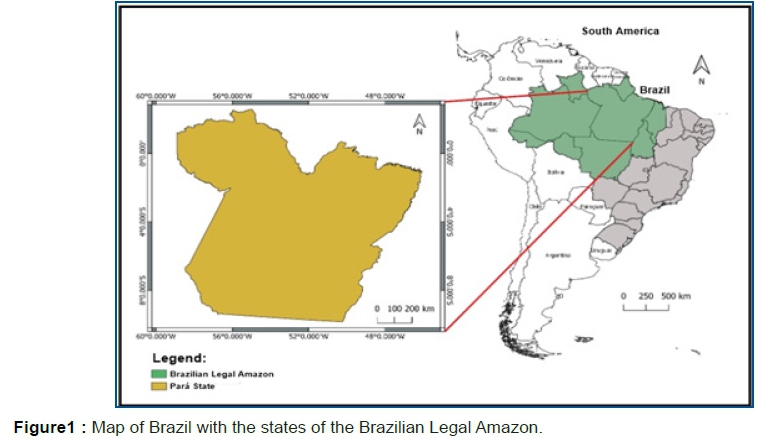
The Legal Amazon comprises nine states, Acre, Amapá, Amazonas, Mato Grosso, Pará, Rondônia, Roraima, Tocantins, and part of Maranhão, totaling 772 municipalities. Its territorial extension corresponds to about 59% of the Brazilian territory, its population is equivalent to 13% of the total inhabitants of Brazil and 60% of the country's indigenous population live in the region12,13. Pará has an estimated population of 8,777,124 inhabitants, an HDI of 0.64614 (figure 1).
Data were classified according to notification date and deaths according to closing date. All cases and deaths registered by COVID-19 in the period from March 2020 to June 2021, in the state of Pará, Brazil, were considered. Extracted by two researchers independently, to minimize the collection bias and ensure the quality and reliability of the data obtained.
All notifications of cases and deaths related to COVID-19 were considered, using the International Classification of Diseases, 10th edition (ICD-10), of "U07.1 COVID-19, identified virus", associated with the diagnosis of the disease, confirmed by clinical and/or laboratory diagnosis.
The collected data were distributed in an Excel spreadsheet. Incidences (cases/population x 100,000) and mortality rates (deaths/population x 100,000) expressed per 100,000 inhabitants, and lethality (total deaths/total cases x 100), expressed as a percentage, were calculated. Mortality rates were also calculated throughout the period, stratified by sex and age.
For trend analysis, the periods were divided into first wave (1st wave - March to November 2020) and second wave (2nd wave - December 2020 to June 2021), to define the end of the first wave, the month with the lowest rate of mortality was considered, which suggested the end of a first wave in the curve.
Trends were analyzed using the methodological guidelines of Antunes and Cardoso15. The Prais-Winsten regression model for population mortality rates was used to construct time series, which allowed the correction of first-order autocorrelation in the analysis of the values of the organized time series. The following values were estimated: probability (p) and Daily Percentage Change - DPC, considering a significance level of 95%. This procedure allowed for the classification of mortality and lethality, assessing whether it increased, decreased or was flat.
Statistical analyzes were performed using STATA 14.0 software (College Station, TX, U.S. 2013).
Due to the use of public domain data, there was no need to submit the work to the National Research Ethics Commission (CONEP) and to analyze the Research Ethics Committee (CEP) system.
RESULTS
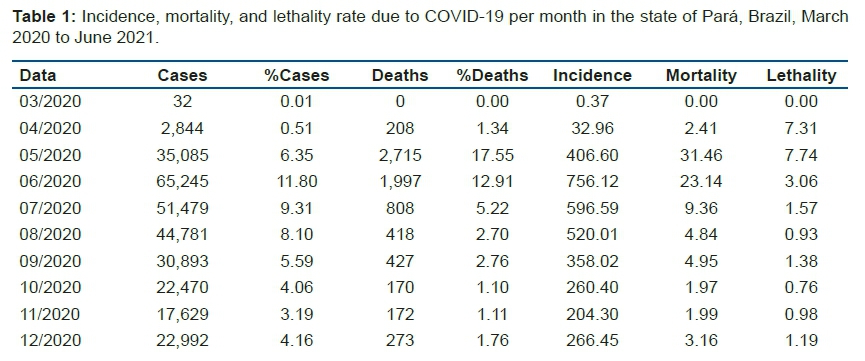
The total number of confirmed cases and deaths from COVID-19 in the state of Pará was 552,937 and 15,469, respectively, in the period from March 2020 to June 2021. The months with the highest frequencies of confirmed cases for COVID-19 were June 2020 (65,245/11.8%), April 2020 (54,036/9.77%) and March 2021 (52,880/9.56%). Regarding death, they were May 2020 (2,715/17.55%), April 2021 (2,555/16.52%) and June 2021 (1,997/12.91%). The incidence and mortality rates for the period from March 2020 to June 2021 were, respectively, 6,407.9 and 179.3 per 100,000 inhabitants and the lethality was 43.3% (table 1).
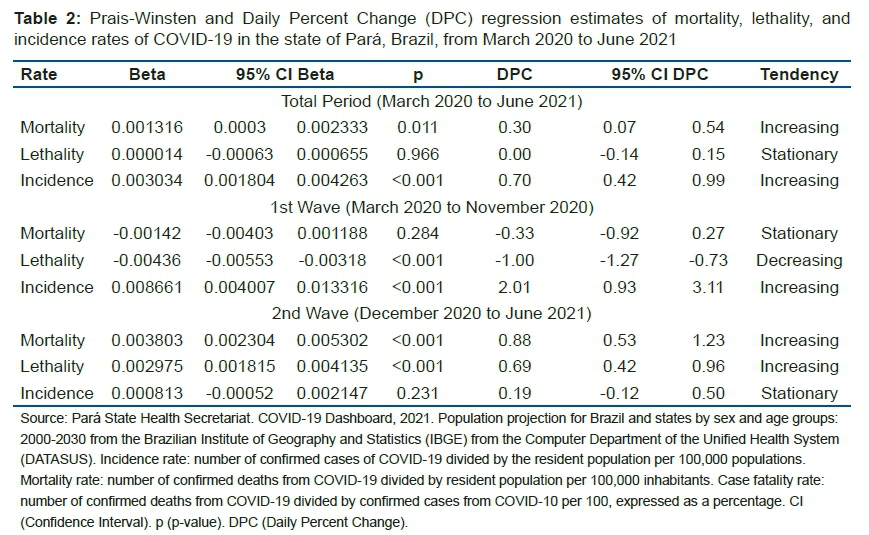
Regarding the analysis of the daily trend of rates in the period from March 2020 to June 2021, both mortality and incidence increased. With the division into two periods, it was found that the incidence remained increasing and the lethality decreasing in the first wave and in the second wave the mortality rate and lethality increasing (table 2).
DISCUSSION
In the state of Pará, 552,937 confirmed cases and 15,469 deaths were reported from COVID-19 from March 2020 to June 2021. There was a characterization of two waves of disease incidence (classified by 1st and 2nd wave). The months with the highest frequencies of confirmed cases for COVID-19 were June 2020 (65,245/11.8%), April 2020 (54,036/9.77%) which coincides with the first wave and the next highest increase was in the second wave in March 2021 (52,880/9.56%).
Regarding death, there was a higher frequency in the first period, which was in May 2020 (2,715/17.55%) and in the second period it was concentrated in the months of April 2021 (2,555/16.52%) and June 2021 (1.997/12.91%). The behavior of the trend of rates in the first period was that the incidence remained increasing and the lethality decreasing and in the second period it presented an aggravation, both the mortality rate and the lethality were increasing.
Recent studies have been carried out observing the incidence of COVID-19 in Brazilian municipalities and verified specific flows in each region16-20. And possibly, these variations can be influenced by aspects related to socioeconomic, cultural and health inequalities, thus, it can be understood that COVID-19 has a syndemic nature21. The term syndemic means the biological and social interaction so that a prognosis, treatment, public policy, and social protection can be established, and these determinants can interfere with the incidence of COVID-19, and this characterizes how this disease behaves in Brazil22,23.
In Northern Brazil, the most affected states on May 5, 2020, in reported cases of COVID-19 and mortality per 1 million inhabitants, were Amazonas (2,327.5 and 251.7) and Pará (627.4 and 49 .5). The capital of Pará has the highest incidence (1,816.4/1,000,000 inhabitants) and mortality (240/1,000,000 inhabitants) with a mortality rate of 9.9% such rates remain after one year of the pandemic in the state of Pará, corroborating the present study11.
Regarding the spatial distribution of incidence and mortality, the north and northeast are among the regions with the highest rates. Both regions had cities with incidence rates two to 10 times higher than the incidence rates of cities in the Midwest, South and Southeast regions, and this heterogeneity of the disease corroborates to validate the hypothesis that the incidence and mortality from COVID-19 are associated with a combination of geographic, economic, social, and cultural factors that express the way of life of the population24.
In the Northern region, the high mortality rate may be linked to the presence of the indigenous population25. All people are immunologically susceptible to COVID-19, however, this population is more vulnerable to epidemics due to worse social, economic and health conditions, increasing the spread of diseases26. In addition, the difficulty of accessing health services, geographic distance, scarcity of human resources in the areas of health and language, and a lifestyle that allows them to be more exposed to infectious diseases, such as living in collective houses and sharing personal utensils are all favorable factors. Many indigenous people have already been victims of COVID-19, but the difficulty in diagnosing and notifying the inhabitants of indigenous areas contributes to the underreporting of the number of cases and deaths25-27.
The rates of intensive care unit beds in the Brazilian territory per 10,000 inhabitants is another factor in relation to the capacity of the health system, which the northern region has a much lower rate than other regions, with 0.9 beds27. The high incidence of mortality can be justified by conditions related to health care, socioeconomic and demographic conditions, and factors peculiar to the population (age, presence of comorbidities and lifestyle habits)28-31.
To minimize the increase in new cases and mortality, and the spread to the interior, the government of Pará instituted a blockade decree in the capital and nine other municipalities. This measure aimed to impose social isolation as there were municipalities that had a higher incidence than the Capital11.
The insufficiency in the capacity of hospital care and emergency care units, health professionals and adult beds, ICU beds and ventilators, and the lack of rapid testing possibly contributed to the advancement of COVID-19 in the state of Pará for both increase in cases and deaths11,32.
The state of Pará started vaccination on January 19, 2021, and until September 24, 2021, there is a total of 7,036,152 applied doses, which represents 46.04% of vaccination coverage for the first dose and 29.02% for second or single dose33. It is known that vaccination will take more time to reach most of the population, which is why social distancing, isolation, the use of face masks and quarantine are still the best ways to prevent transmission of the virus.
This study had some limitations: the methods and analyzes applied cannot infer causality; secondary data analysis may be limited by incompleteness of the dataset34; do not consider individual-level variables such as age/gender/race and therefore limit conclusions.
CONCLUSION
It was found that the behavior of the trend of rates in the first period was increasing in the incidence of confirmed cases and the lethality decreasing, and in the second period both mortality and lethality rates were increasing. The contribution of this analysis supports preventive actions, control and treatment, reduction of mortality and definition of priorities within the area of public health.
Authors' Contributions
All authors participated in all stages of the work, study design and manuscript design. All authors agreed with the final version of the manuscript.
Acknowledgments
We thank the Acre State Health Secretariat (SESACRE), Acre, Brazil, the Federal University of Acre (UFAC), Acre, Brazil, and the Centro Universitário FMABC (FMABC), Santo André, São Paulo, Brazil. All researchers, undergraduate, master's and doctoral students from the Study Design and Scientific Writing Laboratory of the FMABC University Center, Santo André, São Paulo.
Conflict of Interest
There are no conflicts of interest.
REFERENCES
1.Nalla AK, Casto AM, Huang M-LW, Perchetti GA, Sampoleo R, Shrestha L, et al. Comparative performance of sars-cov-2 detection assays using seven different primer-probe sets and one assay kit. J Clin Microbiol. 26 de maio de 2020; 58(6): e00557-20. DOI: 10.1128/JCM.00557-20 [ Links ]
2.Who coronavirus (COVID-19) dashboard [Internet]. [citado 3 de abril de 2021]. Disponível em: https://covid19.who.int [ Links ]
3.Marinho PRD, Cordeiro GM, Coelho HFC, Brandão SCS. Covid-19 in Brazil: A sad scenario. Cytokine Growth Factor Rev. 2021 Apr; 58: 51-54. DOI: 10.1016/j.cytogfr.2020.10.010. Epub 2020 Nov 5. PMID: 33199180. [ Links ]
4.Ministério da Saúde (BR). Painel coronavirus [Internet]. Brasília: Ministério da Saúde; 2020 [citado 28 de agosto de 2021]. Disponível em: https://covid.saude.gov.br/ [ Links ]
5.Marquitti FMD, Coutinho RM, Ferreira LS, Borges ME, Portella TP, Silva RLP da, et al. Brazil in the face of new SARS-CoV-2 variants: emergencies and challenges in public health. Rev bras epidemiol. 2021; 24: e210022. DOI: https://doi.org/10.1590/1980-549720210022 [ Links ]
6.Bezerra ÉCD, Santos PSD, Lisbinski FC, Dias LC. Spatial analysis of Brazil's COVID-19 response capacity: a proposal for a Healthcare Infrastructure Index. Cien Saude Colet. dezembro de 2020; 25(12): 4957-67. DOI: 10.1590/1413-812320202512.34472020 [ Links ]
7.Orellana JDY, Marrero L, Horta BL. Excesso de mortes por causas respiratórias em oito metrópoles brasileiras durante os seis primeiros meses da pandemia de COVID-19. Cad Saúde Pública. 2021; 37(5): e00328720. DOI: https://doi.org/10.1590/0102-311X00328720 [ Links ]
8.Muniz ÉS. A interiorização da covid-19 na Amazônia: reflexões sobre o passado e o presente da saúde pública. Hist cienc saude-Manguinhos. 30 de julho de 2021; 28: 875-8. DOI: https://doi.org/10.1590/S0104-59702021005000007 [ Links ]
9.Coronavírus Brasil [Internet]. [citado 7 de abril de 2021]. Disponível em: https://covid.saude.gov.br/ [ Links ]
10. Escobar, G.J. et al. Disparidades raciais nos testes e desfechos do COVID-19: estudo de coorte retrospectivo em um sistema integrado de saúde. Anais de medicina interna, 2021. [ Links ]
11.Silva, F.L.; Pita, J.D.; Gomes, M.D.A.; Silva, A.P.L.; Silva, G.l.P. (2021). Intraregional propagation of Covid-19 cases in Pará, Brazil: assessment of isolation regime to lockdown. Epidemiology and infection, 149, e72, p.1-15. DOI: https://doi.org/10.1017/S095026882100039X [ Links ]
12.Abreu LC, Elmusharaf K, Siqueira CEG. A time-series ecological study protocol to analyze trends of incidence, mortality, lethality of COVID-19 in Brazil. J Hum Growth Dev. 2021; 31(3):491-495. DOI: 10.36311/jhgd.v31.12667 [ Links ]
13.2011 - portal embrapa [Internet]. [citado 7 de abril de 2021]. Disponível em: https://www.embrapa.br/dia-de-campo-na-tv/2011 [ Links ]
14.Pina-Costa, A. et al. Malária no Brasil: o que acontece fora da região endêmica da Amazônia. Memórias do Instituto Oswaldo Cruz, v. 109, p. 618-633, 2014. [ Links ]
15.Ibge | portal do ibge | ibge [Internet]. [citado 7 de outubro de 2021]. Disponível em: https://www.ibge.gov.br/ [ Links ]
16.Antunes, J.L.F., Cardoso, M.R.A. (2015) 'Uso da análise de séries temporais em estudos epidemiológicos', Epidemiologia e Serviços de Saúde, 24(3), 565-576. DOI: 10.5123/S1679-49742015000300024. [ Links ]
17.Cavalcante JR, Abreu A de JL de. COVID-19 no município do Rio de Janeiro: análise espacial da ocorrência dos primeiros casos e óbitos confirmados. Epidemiologia e Serviços de Saúde [Internet]. 29(3). DOI: https://doi.org/10.5123/S1679-49742020000300007 [ Links ]
18.Andrade LA et al. (2020) Surveillance of the first cases of COVID-19 in Sergipe using a prospective spatiotemporal analysis: the spatial dispersion and its public health implications. Revista da Sociedade Brasileira de Medicina Tropical [Internet] 53, e20200287. DOI: https://doi.org/10.1590/0037-8682-0287-2020 [ Links ]
19.Fortaleza CMCB et al. (2020) Taking the inner route: spatial and demographic factors affecting vulnerability to COVID-19 among 604 cities from inner São Paulo State, Brazil. Epidemiology & Infection [Internet] 148, e118. DOI: 10.1017/S095026882000134X [ Links ]
20.Pedrosa NL. Análise Espacial dos Casos de COVID-19 e leitos de terapia intensiva no estado do Ceará, Brasil [Internet]. Disponível em: http://www.cienciaesaudecoletiva.com.br/artigos/analise-espacial-dos-casos-de-covid19-e-leitos-de-terapia-intensiva-no-estado-do-ceara-brasil/17556?id=17556&id=17556 [ Links ]
21.Dornels Freire de Souza C, Silva de Paiva JP, Cavalcanti Leal T, Feitosa da Silva L, Gomes Santos L. Spatiotemporal evolution of case fatality rates of COVID-19 in Brazil, 2020. J Bras Pneumol. 2020; 46(4): e20200208-e20200208. DOI: https://doi.org/10.36416/1806-3756/e20200208 [ Links ]
22.de Souza CDF et al. (2020) Spatiotemporal evolution of coronavirus disease 2019 mortality in Brazil in 2020. Revista da Sociedade Brasileira de Medicina Tropical [Internet] 53, e20200282. DOI: https://doi.org/10.1590/0037-8682-0282-2020 [ Links ]
23.Horton R (2020) Offline: COVID-19 - a reckoning. The Lancet [Internet] 395, 935. DOI: 10.1016/S0140-6736(20)30669-3. [ Links ]
24. Lana RM et al. (2020) Emergência do novo coronavírus (SARS-CoV-2) e o papel de uma vigilância nacional em saúde oportuna e efetiva. Cadernos de Saúde Pública [Internet] 36(3), e00019620. DOI: https://doi.org/10.1590/0102-311X00019620 [ Links ]
25.Castro, R. R., Santos, R., Sousa, G., Pinheiro, Y. T., Martins, R., Pereira, M., & Silva, R. (2021). Spatial dynamics of the COVID-19 pandemic in Brazil. Epidemiology and infection, 149, e60. DOI: https://doi.org/10.1017/S0950268821000479 [ Links ]
26.Santos RV, Pontes AL and Coimbra CEA Jr (2020) Um "fato social total": COVID-19 e povos indígenas no Brasil. Cadernos de Saúde Pública [Internet] 36(10), e00268220. DOI: https://doi.org/10.1590/0102-311X00268220 [ Links ]
27.Power T et al. (2020) COVID-19 and indigenous peoples: an imperative for action. Journal of Clinical Nursing [Internet] 29, 2737-2741. DOI: https://doi.org/10.1111/jocn.15320 [ Links ]
28.Díaz de León-Martínez L et al. (2020) Critical review of social, environmental and health risk factors in the Mexican indigenous population and their capacity to respond to the COVID-19. Science of the Total Environment [Internet] 733, 139357. DOI: https://pubmed.ncbi.nlm.nih.gov/32416536/#:~:text=10.1016/j.scitotenv.2020.139357 [ Links ]
29.Associação de Medicina Intensiva Brasileira (2020) AMIB apresenta dados atualizados sobre leitos de UTI no Brasil. Associação de Medicina Intensiva Brasileira [Internet]. Avaliable at: https://www.amib.org.br/fileadmin/user_upload/amib/2020/abril/28/dados_uti_amib.pdf [ Links ]
30.de Cobre AF et al.. (2020) Risk factors associated with delay in diagnosis and mortality in patients with COVID-19 in the city of Rio de Janeiro, Brazil. Ciência & Saúde Coletiva [Internet] 25, 4131-4140. DOI: https://doi.org/10.1590/1413-812320202510.2.26882020 [ Links ]
31.Garnelo L, Sousa ABL and Silva C de O da (2017) Regionalização em Saúde no Amazonas: avanços e desafios. Ciência & Saúde Coletiva [Internet] 22, 1225-1234. DOI: https://doi.org/10.1590/1413-81232017224.27082016 [ Links ]
32.da Silva JB and Muniz AMV (2020) Pandemia do Coronavírus no Brasil: impactos no Território Cearense. Espaço e Economia [Internet] 9(17), 1-20. doi: https://doi.org/10.4000/espacoeconomia.10501 [ Links ]
33.Mendonça FD, Rocha SS, Pinheiro DLP, Oliveira SV. Região Norte do Brasil e a pandemia de COVID-19: análise socioeconômica e epidemiológica. J Health NPEPS. 2020; 5(1): 20-37). [ Links ]
34.Pará. State of Pará Public Health Secretary (SESPA). Coronavirus in Pará. Available at http://www.saude.pa.gov.br/vacinometro/ (Accessed 24 September 2021). [ Links ]
 Correspondence:
Correspondence:
celiaguarnieris@gmail.com
Manuscript received: july 2021
Manuscript accepted: september 2021
Version of record online: november 2021


{kind=link}
{kind=link}
{kind=link}