










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.3 Santo André set,/dez. 2021
https://doi.org/10.36311/jhgd.v31.12609
ORIGINAL ARTICLE
DOI: 10.36311/jhgd.v31.12609
Effects of the social isolation generated by Covid-19 on the quality of life of the population in Rio Branco -Acre and Santo André - São Paulo, Brazil
Francisco Naildo Cardoso LeitãoII, III; Carlos Roberto Teixeira FerreiraI, II; Katiuscia Larsen de AbreuII, III; Maura Bianca Barbary de DeusI, II; Hugo Macedo JuniorIII; Mauro José de Deus MoraisI, II
ICentro de Ciências da Saúde e do Desporto. Campus Rio Branco. Universidade Federal do Acre (UFAC) - Rio Branco, Acre, Brazil
IILaboratório Multidisciplinar de estudos e Escrita Científica das Ciências da Saúde-LaMEECCS, UFAC - Acre, Brazil
IIIPós-Graduação em Ciências da Saúde do Centro Universitário Saúde do ABC (FMABC), São Paulo, Brasil
ABSTRACT
INTRODUCTION: COVID-19 is a highly transmissible virus that is causing very serious problems in the world's health, generating major political and financial problems. There are numerous risk factors related to this disease, ranging from morbidities to social and family issues.
OBJECTIVE: to evaluate the effects of the social isolation generated by Covid-19 on the quality of life in the population of two Brazilian cities.
METHODS: cross-sectional study. This survey with an online platform uses the drive's Google Forms tool to assess the population's quality of life through the SF-36 protocol. The research was carried out in two different cities of the Brazilian confederation. One in Santo André in São Paulo and Rio Branco in Acre State. The selection was carried out randomly in both groups (Acre and São Paulo), with 109 and 62 participants respectively in this first moment.
RESULTS: regarding gender, women are in greater numbers participating in the city of Santo André, than in Rio Branco, with (80.6% and 48.6%), respectively. Likewise, Santo André has an average age younger than in Rio Branco in relation to the age group. When we compared the dimensions between the two states, performing a Mann-Whitney statistical analysis, statistical differences appeared in three dimensions: functional capacity, pain, and vitality, with better quality of life in these three domains for the city of Rio Branco.
CONCLUSION: the city of Rio Branco, has a positive score compared to the city of Santo André, in most of the domains analyzed.
Keywords: quality of life, COVID-19, social isolation, SARS-CoV-2.
Authors summary
Why was this study done?
The proposed and implemented intervention plan had a positive outcome. During the study period, an increase in the vaccination coverage of the 2020 National Measles Vaccination Campaign and the 2020 National Multivaccination Campaign was observed in the territory covered by the FHS São Cristóvão in the city of Vitória, ES, Brazil. The vaccination coverage of the two Campaigns was significantly expanded, despite all challenges of the COVID-19 pandemic.
What did the researchers do and find?
We evaluated the effects of the social isolation generated by Covid-19 on the population's quality of life of two Brazilian cities: Santo André, in São Paulo State and and Rio Branco in Acre State. The selection was carried out randomly in both groups (Acre and São Paulo), with 109 and 62 participants, respectively, at this first moment. When we compared the dimensions between the two cities using the Mann-Whitney statistical analysis, a statistical difference emerged in three dimensions: functional capacity, pain, and vitality, presenting in these three domains a better quality of life for the city of Rio Branco.
What do these findings mean?
These demonstrate that the activities of large centers when they are faced with a situation of isolation, decrease the quality of life. What makes us rethink to develop better programs that develop aspects of a better quality of life for residents of large cities.
INTRODUCTION
Known as SARS-CoV-2 (acute severe respiratory syndrome coronavirus 2), it has spread globally rapidly to the present day, without until the present moment, we do not have a concrete and definitive solution1,2. Although the virus genome has been sequenced, which has allowed for the development of various diagnostic tests and the initiation of vaccines and data around clinical features grow daily, the clinical spectrum of the disease remains to be defined (including the potential for spread asymptomatic)3.
The quarantine and isolation currently imposed throughout the world due to COVID-19, which acts to separate and restrict both symptomatic and asymptomatic people, seeking to avoid a potentially greater exposure to the virus, thus reducing the risk of infecting other people as well as being infected, is often an unpleasant experience for those who go through it. Separation from loved ones, loss of freedom, uncertainty about the status of the illness, and boredom can occasionally create dramatic effects. The successful use of quarantine as a public health measure requires us to reduce the negative effects associated with it as much as possible. Given the evolving situation with coronavirus, policymakers urgently need evidence synthesis to produce guidance for the public. In the circumstances like these, rapid tests are recommended by the World Health Organization (WHO)4.
According to the WHO, the infection cases by COVID-19 are only increasing worldwide, where a globalized pandemic has already been characterized. There are countless works carried out by scientists looking for a definitive cure (in principle, a vaccine). Research is as varied as possible, in the clinical area and epidemiological, social, human aspects, etc. Because the population is being reached in all its dimensions1.
Research on quality of life (QOL) is a growing research topic in health studies7. Since the mid-twentieth century, the Health and QOL of populations, with and without a clinical diagnosis, have been discussed together, often taking place with a conceptual understanding of one by the other5,6. The study of QOL has assumed importance in several aspects in recent years, particularly regarding its assessment and measurement, either individually or collectively8.
The QOL theme is one of the great questions and challenges for the health area at the beginning of this century. Much has been said about QOL, and there are many attempts to find the best definition for the term, approached from the most different perspectives, whether from the perspective of science or individuals9. Given the need to formulate a concept focused on the health perspective, the WHO in 1994 defined QOL as the individual's perception of their position in life in the context of the culture and value system in which they live and in concerning your goals, expectations, standards and concerns4.
Health-Related Quality of Life (HRQOL) is a subset of the term QOL, often used to distinguish QOL in a more general sense and QOL related to medical and clinical parameters. HRQOL addresses relevant aspects that may vary from study to study. Still, in general, they include health, physical symptoms, physical, emotional, cognitive and sexual functions, functional status, and the possible consequences of these factors10.
The health-related quality of life (HRQOL) assessment has been an increasingly frequent practice in medicine today. This assessment aims to monitor the health of a given population, diagnose the nature, severity, and prognosis of the disease, in addition to evaluating the effects of treatment11.
Within this perspective, the HRQOL assessment is a tool capable of verifying the impact of the disease, health, and treatment, consisting of multidimensional indicators, allowing the assessment of different people who have the same problem and different levels of health physical well-being and emotional12. Although there is no consensus on the meaning of the term QOL, as it deals with concepts related to subjective and individual perception, it is possible to measure it through standardized and validated instruments used in each population13-15.
Although there are several definitions, the main concept is the definition of quality of life proposed by the WHO16. QOL is not only related to the resolution of basic survival problems, it must also include the guarantee of conditions of comfort and psychological, physical, individual and family satisfaction of individuals. It must be understood as the sense of well-being of each one, that is, it must be understood about objective material aspects and subjective emotional aspects17.
HRQOL is the value attributed to lifetime when changed by the perception of physical and psychological limitations, social functions and opportunities influenced by the disease, treatment and other health problems, becoming the main indicator for evaluative research on the outcome of interventions18.
The assessment of the HRQOL and aspects surrounding it is paramount to understand the citizen in the aspects associated with illnesses or linked to therapeutic interventions. This type of assessment maintains a multidimensional character, even though the emphasis is on symptoms, disabilities, or limitations caused by illnesses19.
Taking into account the above about quarantine and its possible side effects, as well as that the North region (Acre) is considered the neediest in the country, where there are many difficulties in conditions ranging from housing, sanitation, financial and social issues, government assistance and support, how is the QOL of this population affected by COVID-19 in the State of Acre? What are the main epidemiological and clinical characteristics of this population? How will the quality of life of the population of Acre be compared to another population of another state in Brazil?
Given the described context, we aimed to evaluate the effects of the social isolation generated by COVID-19 on the quality of life of the population of two Brazilian states.
METHODS
Cross-sectional study. The research was carried out in two different cities of the Brazilian confederation. In Santo André, São Paulo and Rio Branco, Acre, both in Brazil. This is a survey with an online platform, using DRIVE's Google Forms tool to assess the quality of life of the population, the selection was carried out randomly in both groups, with 109 and 62 participants respectively at this first moment.
This study was carried out following the guidelines that regulate research on human beings, in Resolution No. 466/12 of the National Health Council. The research was approved by the Ethics Committee of the Centro Universitário FMABC/Fundação do ABC, under number 4,184,251. All participants who agreed to participate in the research signed the free and informed consent form.
Inclusion criteria
Participants aged over 18, literate of both sexes and in full mental health. People who were in social isolation caused by COVID-19.
Exclusion criteria
Minors, indigenous and illiterate people, and people with mental disabilities could not participate in the research. Also people who were not in social isolation.
Instrument used
The SF-36 assesses the QOL of the population, where we have the "Brazilian Version of the Quality-of-Life Questionnaire - SF-36". This protocol works with eight dimensions, as follows: physical functioning (10 items), limitations caused by physical health problems (4 items), limitations caused by emotional health problems (3 items), social function (2 items), well- emotional being (5 items), pain (2 items), energy/fatigue (vitality) (4 items), general health perception (5 items) and an item about the current health status compared to a year ago which is computed to part. In general terms, to evaluate the results, a score is given for each item (or question), later transformed into a scale from 0 to 100, in which the value 0 reflects a worse QOL and the value 100 reflects a better QOL. The internal consistency estimated by the SF-36 exceeded 0.80 (range 0.61 to 0.90). The SF-36 is considered a generic measure and is supplemented with multi-item type scales.
In this study, the scores of the dimensions present will be distributed into ranges: 1st range - scores from 0% to 25%; 2nd range - scores from 25.001% to 50%; 3rd range - scores from 50.001% to 75%; 4th range - scores from 75.001% to 100%. To analyze the prevalence of participants in the different dimensions, the 1st and 2nd ranges will represent low QOL and the 3rd and 4th ranges, good QoL.
The SF-36 was developed to measure HRQOL, satisfying two essential properties: the assessment of the dimensions that are important for the health condition and the integration of information from the domains, enabling a more complete analysis. The scoring procedure is done by dimension and is therefore analyzed separately. Thus, there is no single value resulting from the global assessment of the health-related quality of life, but average scores for each dimension. This analysis makes it possible to identify the real health-related problems of the participants and verify which ones impact the QOL.
Statistical analysis
Data were analyzed using the Statistical Package for Social Science (SPSS), version 23.0. Descriptive analysis was performed for all variables. Data were expressed as mean ± standard deviation or median (interquartile range), when appropriate. To compare each group's initial and final values, the paired t-test and the Wilcoxon test were performed for non-parametric data. Comparisons between groups were performed using the unpaired t-test or the Mann-Whitney test, when appropriate. In this sense, we carried out both evaluations of the same sample group and compared two related samples as much as possible. For comparison between groups, the Mann-Whitney test for non-parametric distributions was applied. Statistical significance was considered at the level of p < 0.05 (or 5%). Sample distribution was tested with the Shapiro-Wilk test. The data collected were analyzed: a) descriptive: frequency tables, with position measurements (mean, median, minimum and maximum) and standard deviation; Cronbach's alpha coefficient: checks the internal consistency of KDQOL-SF. Good reliability is considered for alpha values equal to or greater than 0.6020.
RESULTS
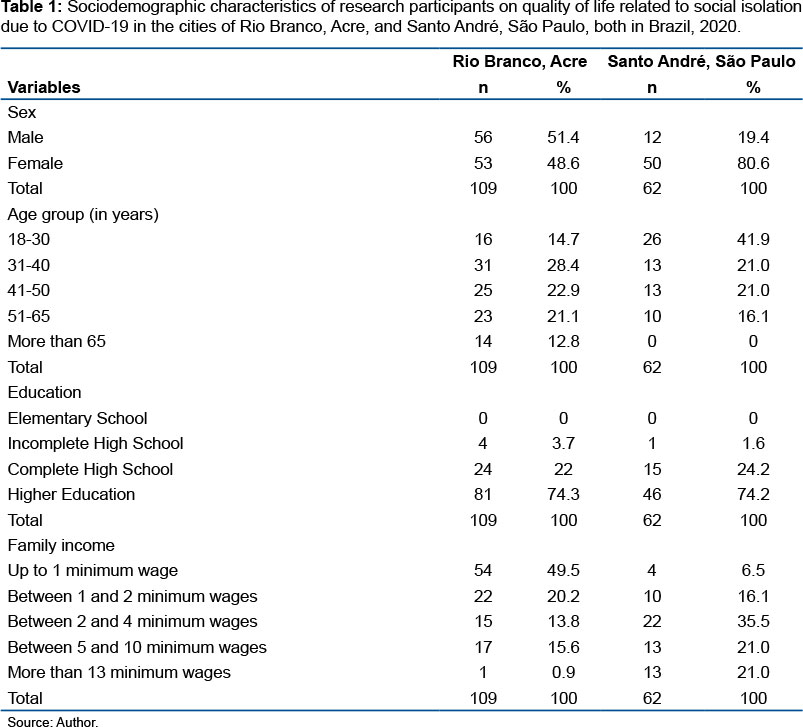
The sociodemographic characteristics found in this study are described in table 1. Regarding sex, proportionally, participants from Santo André have a much higher number of women than in the city of Rio Branco (80.6% and 48.6%) respectively. Also at a proportional level, the age group in Santo André, is much younger than the city of Rio Branco, having, for example, no participants in the age group above 65 years old. In terms of education, the averages are equal. A very interesting fact is about family income, as the state of Acre has almost 50% of participants with income up to the minimum wage. On the contrary, São Paulo has only a percentage of 6.5% in this range.
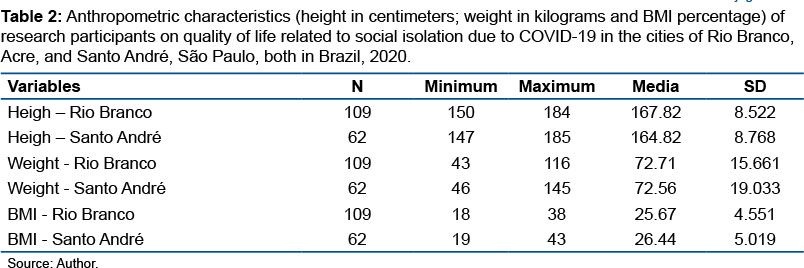
Table 2 shows the anthropometric characteristics of the participants from both states, the average of all variables being equal (height, weight, and Body Mass Index (BMI)), and the assessment of the BMI in Santo André is slightly above the ideal classification according to the literature.
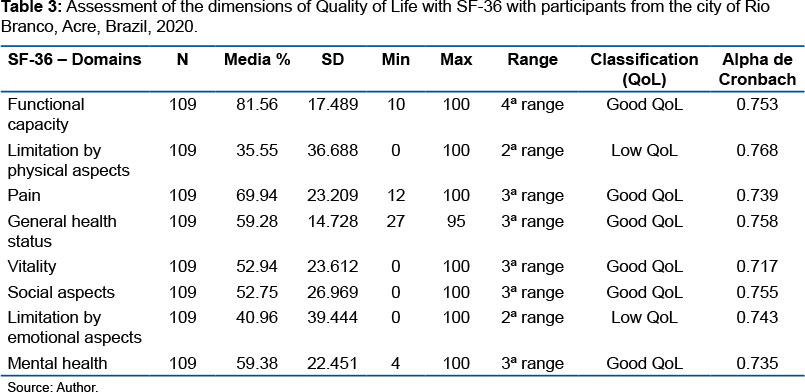
With table 3, which shows the eight dimensions of the SF-36 for the State of Acre, we identified only two domains considered as "Low QOL", which were those of limitation by physical aspects and limitation by emotional aspects with averages of 35.55 and 40.96 respectively. We recall that the dimensions "General health status", "Vitality", "Social Aspects" and "Mental Health", despite having been classified as good quality of life, their values were close to the 50% average. As for the internal consistency of the SF-36, the dimensions obtained satisfactory Cronbach's Alpha values (≥0.60).
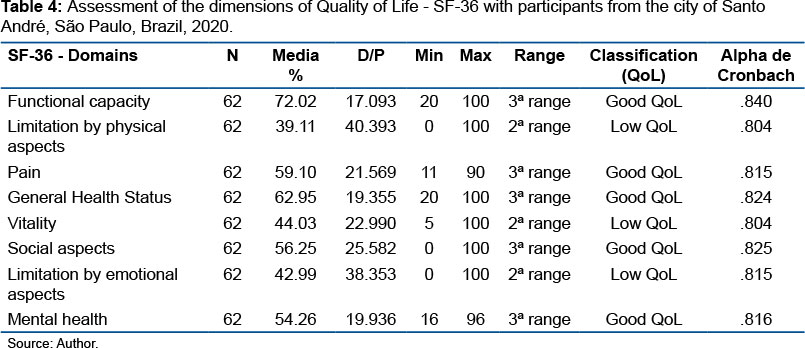
In table 4, where the SF-36 dimensions of the participants from São Paulo were evaluated, three domains were classified as "Low QOL", which were "Limitation by Physical Aspects", "Vitality" and "Limitation by Emotional Aspects", with means 39.11; 44.03 and 42.99 respectively. Also, when evaluating the internal consistency of the SF-36, the dimensions obtained satisfactory Cronbach's Alpha values (≥0.60).
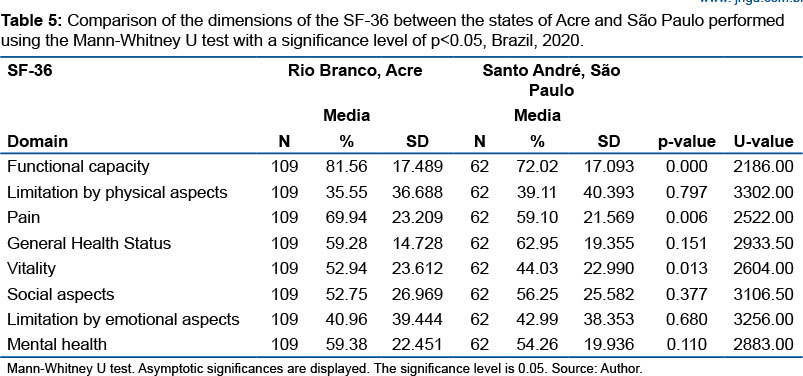
In table 5, when we compared the dimensions between the two cities, performing a Mann-Whitney statistical analysis, statistical differences appeared in three dimensions, which were functional capacity, pain, and vitality, presenting in these three domains better quality of life for the state of Acre. The Mann-Whitney test showed that the position of the functional capacity domain in the State of Acre is better than in the State of São Paulo (U = 2186.00; p<0.01) in Pain (U = 2522.00; p<0.01) and in vitality (U = 2604.00; p<0.01), but not in the other dimensions.
DISCUSSION
In general, the population in isolation due to COVID-19 in the city of Rio Branco, Acre has a better QOL than the population of the city of Santo André, São Paulo when evaluated from the domains of SF-36 protocol. The dimensions with low QOL in Rio Branco, were "limitation by physical aspect" and "limitation by emotional aspect", with an average score of 35.55 and 40.96 respectively. While the city of Santo André obtained as low QOL in the dimensions "Limitation by physical aspects", "Vitality" and Limitation by emotional aspect" with an average score of 39.11; 44.03 and 42.99 respectively.
By carrying out a comparative analysis between the two cities, Rio Branco obtained better results in terms of QOL. Three dimensions had a statistically significant difference, all being positive with good QOL for the city of Rio Branco compared to Santo André, which were: "functional capacity", "Pain" and "Vitality". The other domains had no statistical difference, although in an overall score, the means were better for the state of Acre compared to the state of São Paulo.
The sociodemographic characteristics concerning sex, proportionally, participants in São Paulo have a much higher number of women than in Acre. Also at a proportional level, the age group in Santo André is much younger than the city of Rio Branco, having, for example, no participants in the age group above 65 years. In terms of education, the averages are homogeneous. A very interesting fact is about family income, as the state of Acre has a percentage of almost 50% of participants with income up to the minimum wage, while on the contrary, São Paulo has only a percentage of 6.5% in this range, showing with that, a much greater purchasing power. The body mass index of Santo André is higher, slightly above the classification recommended by the scientific literature.
SARS-CoV-2 is reaching all age groups, social classes and ethnic groups around the world, without distinction21. A large part of this population is recovering at home, and are often in isolation with the virus without knowing it, as it goes unnoticed21,22. Another specific audience, such as the elderly, pre-existing diseases have a higher risk of developing serious illnesses and even death21, including pregnant women who may also be more susceptible to COVID-19, as they are generally vulnerable to respiratory infection23. A large part of this population is in social isolation. This is what our research demonstrates, having two groups from different places in Brazil.
An interesting data to be analyzed in our research was the dimension "limitation by physical aspect", where in the two analyzed states they gave a low score classified as "Low QOL", leaving the city of Rio Branco, Acre with 35.55 and Santo André, São Paulo with 39.11. Which means that they are not taking proper care to exercise in any way, thus affecting this dimension. Corroborating these results, the dimension "Vitality" in the result for São Paulo is also found with Low quality of life, with a score of 44.03, what correlates with the first domain cited.
Well-oriented and developed physical activity can benefit the whole body, even helping to prevent diseases24,25 and defend the body26,27. The social isolation caused by the COVID-19 pandemic can cause various body functions, consequently affecting possible aspects of quality of life28. Thus, the great importance of developing some sport, even if adapted in this isolation, can help benefit other dimensions of QOL that go hand in hand in this isolation phase, such as psychological and cognitive issues, among others29, as well. as in the improvement in physical aspects30.
Corroborating the studies by Li Z, et al.31, when evaluating health professionals who were in contact with patients with Covid-19, they had great emotional problems, anguish and anxiety because they were insecure about the disease, as well as because they were in direct contact with infected patients. The emotional dimensions in both cities (Rio Branco and Santo André) had a low QOL, demonstrating the high impact that the concern with being in isolation is causing psychologically. Another factor to be taken into account with these professionals is knowing that there is still no definitive cure and little information on the subject32.
In their study, CHEN Q, et al.33 with a medical team, identified many professionals who demonstrated a poor general health status due to the possibility of being transmitters of the disease to other people and the lack of protective material and inefficiency against the patients. Differently, in our case, the domain "General Health Status" had a good QOL. This may be because the circumstances are averse to the hospital environment regarding social isolation.
The fear of dying, the insecurity due to the lack of a vaccine to cure the disease caused by the pandemic in Italy has caused great psychological impacts on the population34. Although our studies have provided a good QOL in both cities (Rio Branco and Santo André), in both cases the scores in the Social Aspect domains were similar, with 52.75 and 56.25 respectively, demonstrating that there is also insecurity in the population that is in social isolation on the subject.
Conversely, studies showed cases of suicide among health professionals who were infected by COVID-19 in India and Italy. In the mental health aspect of our study, the means were considered as having good QOLin both states, which demonstrates that this population is enduring the moment of social isolation in their homes. Possible psychiatric problems intensify with psychological wear, thus increasing the suicide rate35-37.
Ornell F, et al.36 considers that there will be changes in the daily lives of families, in their work, cultural environments, among others. Our studies demonstrate that despite the changes in daily life due to isolation, in social aspects in both states, people continue to maintain active social relationships, even if it is with other mechanisms such as lives, virtual conversations, etc. this domain was classified as good QOL.
Many areas of knowledge consider the quality-of-life component important to know how we can identify, assess, and treat the so-called silent diseases. In this phase that the world is going through, all aspects must be considered to alleviate the population's life in a moment of social isolation. In our case, Rio Branco, had a better QOL on average than the city of Santo André. Several aspects can be considered, such as housing aspects, where in Acre most of the houses are houses with land and not apartments like São Paulo. Thus, people have more mobility, which was demonstrated in the domains "functional capacity", "pain" and "vitality", where these three variables even gave significant positive differences to the State of Acre compared to the State of São Paulo. All related by aspects of larger physical spaces.
CONCLUSION
The results indicate that both cities have their QOL compromised due to social isolation. Rio Branco, had better QOL than the city of Santo André, in the domains of functional capacity, pain and vitality. Both cities showed similar results in the rest of the domains.
Author's contribuitions
Francisco Naildo Cardoso Leitão - writing the manuscript, following the guidelines of the magazine; Maura Bianca Barbary of God - Manuscript Writing; Carlos Roberto Teixeira Ferreira - data collection, experiments and manuscript writing; Ocilma Barros de Quental - data collection, carrying out the experiments and writing the manuscript; Mauro José de Deus Morais - data collection, carrying out the experiments and writing the manuscript.
Acknowledgments
We appreciate the partnership between the Federal University of Acre and the University of São Paulo. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. The financial viability of the article is due to the Acre - Health Project in the Western Amazon (multi-institutional agreement process no. 007/2015 SESACRE-UFAC-FMABC).
Conflicts of interest
We declare no potential conflicts of interest.
REFERENCES
1.de Macedo Júnior AM. Covid-19: calamidade pública. Medicus. 2020; 2(1): 1-6. [ Links ]
2.del Rio C, Malani PN. Covid-19-new insights on a rapidly changing epidemic. JAMA. 2020; 323(14): 1339-40. [ Links ]
3.del Rio C, Malani PN. 2019 Novel coronavirus-important information for clinicians. Jama. 2020; 323(11): 1039-40. [ Links ]
4.Saúde OMd. CID-10: Classificação Estatística Internacional de Doenças com disquete Vol. 1: Edusp; 1994. [ Links ]
5.Hubanks L, Kuyken W, Organization WH. Quality of life assessment: an annotated bibliography. 1994. [ Links ]
6.Guyatt GH, Feeny DH, Patrick DL. Measuring health-related quality of life. Annals of internal medicine. 1993; 118(8): 622-9. [ Links ]
7.Moreno AB, Faerstein E, Werneck GL, Lopes CS, Chor D. Propriedades psicométricas do Instrumento Abreviado de Avaliação de Qualidade de Vida da Organização Mundial da Saúde no estudo pró-saúde. Cadernos de Saúde Pública. 2006; 22: 2585-97. [ Links ]
8.Costa PBd, Vasconcelos KFdS, Tassitano RM. Life quality: patients with chronic renal failure in the city of Caruaru, PE. Fisioterapia em Movimento. 2010; 23(3): 461-71. [ Links ]
9.Bittencourt ZZLdC. Qualidade de vida e representações sociais em portadores de patologias crônicas: estudo de um grupo de renais crônicos transplantados. 2003. [ Links ]
10.Diniz DP, Schor N. Qualidade de Vida-Guia de Medicina Ambulatorial e Hospitalar. Unifesp. Barueri: Manole; 2006. [ Links ]
11.Pagani TCdS, Pagani Junior CR. Instrumentos de avaliação de qualidade de vida relacionada à saúde. Ensaios e Ciência. 2006; 1(1): 32-7. [ Links ]
12.Ciconelli RM. Tradução para o português e validação do questionário genérico de avaliação de qualidade de vida Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36). 1997. [ Links ]
13.Duarte PS. Tradução, adaptação cultural e validação do instrumento de avaliação de qualidade de vida para pacientes renais crônicos em programa dialítico-Kidney Disease and Quality of Life-Short Form (KDQOL-SFTM1. 3). 2003. [ Links ]
14.Hays RD, Kallich JD, Mapes DL, Coons SJ, Amin N, Carter WB, et al. Kidney Disease Quality of Life Short Form (KDQOL-SF), Version 1.3: a manual for use and scoring. Santa Monica, CA: Rand. 1997; 39. [ Links ]
15.Hays RD, Kallich JD, Mapes DL, Coons SJ, Carter WB. Development of the kidney disease quality of life (KDQOL TM) instrument. Quality of life Research. 1994; 3(5): 329-38. [ Links ]
16.Matias AB, Oliveira-Cardoso ÉAd, Mastropietro AP, Voltarelli JC, Santos MAd. Qualidade de vida e transplante de células-tronco hematopoéticas alogênico: um estudo longitudinal. Estudos de Psicologia (Campinas). 2011;28(2):187-97. [ Links ]
17.Silva RBGd, Almeida LPd. Próteses auditivas por idosos: aspectos psicossociais, adaptação e qualidade de vida. Interações (Campo Grande). 2016; 17(3): 463-74. [ Links ]
18.Filgueiras Júnior, N. Qualidade de vida dos atletas da terceira idade do município de Ponta Porã, MS. Universidade Católica Dom Bosco, Campo Grande, 2013. [ Links ]
19.Morais MJD, de Abreu LC, Santana de Oliveira F, Pinheiro Bezerra IM, Raimundo RD, Paulo Martins Silva R, et al. Is aerobic exercise training during hemodialysis a reliable intervention for autonomic dysfunction in individuals with chronic kidney disease? A prospective longitudinal clinical trial. J Multidiscip Healthc. 2019; 12: 711-8. [ Links ]
20.Hair JF, Black WC, Babin BJ, Anderson RE, Tatham RL. Análise multivariada de dados: Bookman Editora; 2009. [ Links ]
21.Isah MB, Abdulsalam M, Bello A, Ibrahim MI, Usman A, Nasir A, et al. Corona Virus Disease 2019 (COVID-19): Knowledge, attitudes, practices (KAP) and misconceptions in the general population of Katsina State, Nigeria. medRxiv. 2020. [ Links ]
22.Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The lancet. 2020; 395(10223): 497-506. [ Links ]
23.Liu H, Wang L-L, Zhao S-J, Kwak-Kim J, Mor G, Liao A-H. Why are pregnant women susceptible to viral infection: an immunological viewpoint? Journal of reproductive immunology. 2020: 103122. [ Links ]
24.Kyu HH, Bachman VF, Alexander LT, Mumford JE, Afshin A, Estep K, et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. bmj. 2016; 354:i3857. [ Links ]
25.WHO W. Global recommendations on physical activity for health. 2010. [ Links ]
26.Collao N, Rada I, Francaux M, Deldicque L, Zbinden-Foncea H. Anti-Inflammatory Effect of Exercise Mediated by Toll-Like Receptor Regulation in Innate Immune Cells-A Review: Anti-inflammatory effect of exercise mediated by Toll-like receptor regulation in innate immune cells. International reviews of immunology. 2020; 39(2): 39-52. [ Links ]
27.Nieman DC, Wentz LM. The compelling link between physical activity and the body's defense system. Journal of sport and health science. 2019; 8(3): 201-17. [ Links ]
28.Weyh C, Krüger K, Strasser B. Physical activity and diet shape the immune system during aging. Nutrients. 2020; 12(3): 622. [ Links ]
29.Herold F, Törpel A, Schega L, Müller NG. Functional and/or structural brain changes in response to resistance exercises and resistance training lead to cognitive improvements-a systematic review. European Review of Aging and Physical Activity. 2019; 16(1): 10. [ Links ]
30.Winett RA, Ogletree AM. Evidence-Based, High-Intensity Exercise and Physical Activity for Compressing Morbidity in Older Adults: A Narrative Review. Innovation in Aging. 2019; 3(2): igz020. [ Links ]
31.Li Z, Ge J, Yang M, Feng J, Qiao M, Jiang R, et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain, behavior, and immunity. 2020. [ Links ]
32.Smith GD, Ng F, Li WHC. COVID-19: Emerging compassion, courage and resilience in the face of misinformation and adversity. Journal of clinical nursing. 2020; 29(9-10): 1425. [ Links ]
33.Chen Q, Liang M, Li Y, Guo J, Fei D, Wang L, et al. Mental health care for medical staff in China during the COVID-19 outbreak. The Lancet Psychiatry. 2020; 7(4): e15-e6. [ Links ]
34.Fernandes CA, da Cunha AM, Hemkemaier ECRC, do Carmo KdS, Moraes TVP, dos Santos TP, et al. Desafios e recomendações para o cuidado intensivo de adultos críticos com doença de coronavírus 2019 (COVID-19). Health Residencies Journal-HRJ. 2020;1(1):21-47. [ Links ]
35.Goyal K, Chauhan P, Chhikara K, Gupta P, Singh MP. Fear of COVID 2019: First suicidal case in India! Asian journal of psychiatry. 2020; 49: 101989. [ Links ]
36.Ornell F, Schuch JB, Sordi AO, Kessler FHP. "Pandemic fear" and COVID-19: mental health burden and strategies. Brazilian Journal of Psychiatry. 2020; 42(3): 232-5. [ Links ]
37.Abreu LC, Elmusharaf K, Siqueira CEG. A time-series ecological study protocol to analyze trends of incidence, mortality, lethality of COVID-19 in Brazil. J Hum Growth Dev. 2021; 31(3):491-495. DOI: 10.36311/jhgd.v31.12667 [ Links ]
 Correspondence:
Correspondence:
mauro.morais@ufac.br
Manuscript received: january 2021
Manuscript accepted: june 2021
Version of record online: november 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}