










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.3 Santo André set,/dez. 2021
https://doi.org/10.36311/jhgd.v31.12611
ORIGINAL ARTICLE
DOI: 10.36311/jhgd.v31.12611
Evolution of COVID-19 during the epidemiological week 16 to 53 of 2020 in the state of Acre Western Amazonia, Brazil
Edimilson Lima de AssisI, III; Mauro José de Deus MoraisII, III; Jorge de Oliveira EichembergI, II; Valéria Rigamonte Azevedo de AssisIII; Hugo Macedo JuniorII; Maura Bianca Barbary de DeusIII; Luiz Carlos de AbreuI, II, III, IV, V
IPós-Graduação em Ciências da Saúde do Centro Universitário Saúde do ABC (FMABC), São Paulo, Brasil
IILaboratório de Delineamento de Estudos e Escrita Cientifica (FMABC), São Paulo, Brasil
IIILaboratório Multidisciplinar de estudos e Escrita Científica das Ciências da Saúde-LAMEECCS, UFAC, Acre, Brasil
IVEscola Superior de Ciências da Santa Casa de Misericórdia de Vitória (EMESCAM), Espírito Santo, Brazil
VCardiorespiratory Research Group, Department of Biological and Medical Sciences, Faculty of Health and Life Sciences, Oxford Brookes University, Headington Campus, Oxford, OX3 0BP, United Kingdom
ABSTRACT
INTRODUCTION: coronavirus is part of a group of RNA viruses belonging to the Coronaviridae family, widely distributed in humans and other mammals. Currently, it has been seriously affecting the whole world, without a definitive cure yet.
OBJECTIVE: to analyse the association between the HDI and confirmed cumulative cases of COVID-19 that occurred during epidemiological week 16 to 53 of 2020, in the State of Acre.
METHODS: this is an ecological study of descriptive time series, evaluating the State of Acre and its 22 municipalities affected by COVID-19, in the period corresponding to the epidemiological weeks 16 to 53 of 2020. The State of Acre and its municipalities are aggregated by five regions with a total of approximately 881 thousand inhabitants, with an HDI of 0.663. Rio Branco is the state capital with 407,000 inhabitants. The 22 municipalities were analyzed, relating the HDI variables, confirmed cases per day and number of inhabitants to each other.
RESULTS: it was observed that the population evaluated, affected by COVID-19 during SE 16 to 53 of 2020, in the State of Acre, had as predominant general characteristics brown skin color, male sex, and the evolution to death from the disease was related with older age and comorbidity. Acre had a mortality rate (deaths per 100,000 inhabitants) of 90.9 and a lethality rate of 1.9%, with the highest mortality rate observed in the municipality of Rio Branco (121.3/100,000 inhabitants) and lethality in Rodrigues Alves (2.9%). The incidence of COVID-19 in Acre was 4,759.9 cases per 100,000 inhabitants, the municipalities of Assis Brasil and Xapuri had the highest incidences in the state with 10273.7 and 9330.8 new cases per 100,000 inhabitants, respectively.
CONCLUSION: although the accumulated numbers of cases are different for the same day, the behavior is very similar, that is, the curves vary in the same way over time, regardless of the municipality observed.
Keywords: COVID-19, SARS-CoV-2, epidemiology, pandemic, health surveillance.
Authors summary
Why was this study done?
COVID-19 is a highly transmissible disease that has been causing serious health problems around the world, generating major political and financial problems. There are numerous risk factors related to this disease, ranging from morbidity to social and family issues. The State of Acre, being one of the poorest in Brazil, needs studies on the subject, making it interesting to carry out an analysis of the incidence of cases in the State.
What did the researchers do and find?
We evaluated the State of Acre and its 22 municipalities affected by COVID-19 during the Epidemiological Week (SE) 16 to 53 of 2020. The State of Acre is made up of 22 municipalities, aggregated by five regions with a total of approximately 881 thousand inhabitants, having an HDI of 0.663. Rio Branco is the state capital with 407,000 inhabitants. The 22 municipalities were analyzed, relating the HDI variables, confirmed cases per day and number of inhabitants to each other. Acre has a mortality rate (deaths per 100,000 inhabitants) of 90.9 and a lethality rate of 1.9%, with the highest mortality rate being found in the municipality of Rio Branco (121.3/100,000 inhabitants) and of lethality in Rodrigues Alves (2.9%).
What do these findings mean?
This demonstrates that the state is at a high risk of cases of COVID when considering the HDI and when compared to other states in the confederation. Served as an alert to health authorities as well as the population.
INTRODUCTION
Coronavirus is part of a group of RNA viruses belonging to the Coronaviridae family, widely distributed in humans and other mammals1. They cause illnesses ranging from the common cold to more serious illnesses such as pneumonia2.
The coronavirus, since 2002, has caused several important Public Health events that have resulted in global epidemics, such as: the Severe Acute Respiratory Syndrome (SARS) caused by the coronavirus SARS-CoV-1; Middle East Respiratory Syndrome (MERS) caused by MERS-CoV and Coronavirus Disease 2019 (COVID-19) caused by SARS-CoV-2, named as such by the World Health Organization (WHO) on January 12, 20201,3. COVID-19 was initially identified as a pneumonia virus in Wuhan. SARS-CoV-2 is a new strain that has not been previously identified in humans4, and which has greater transmissibility than the two previous ones5.
In 2002, the first reports of severe acute respiratory syndrome (SARS) took place in Guangdong province, China6. The main clinical manifestations are fever, fatigue, headache, muscle and joint fatigue, systemic symptoms such as pain and respiratory symptoms such as dry cough, chest tightness and dyspnea. Some people may have gastrointestinal symptoms such as diarrhea7. The epidemic caused by SARS-CoV-1 spread rapidly to become a pandemic in 29 countries, according to WHO statistics, 774 of the 8,096 infected people died, with a mortality rate of 9.6%, before the global SARS epidemic be controlled in 20038. After this outbreak, microbiologists and infectious disease specialists focused on investigating the pathogenicity of the disease and found that this infection was caused by a new form of Corona Virus9.
In 2012, another coronavirus was identified, different from the one that caused SARS. This new coronavirus causes the "Middle East Respiratory Syndrome" (MERS), unknown as an agent of human disease until its identification, starting in Saudi Arabia and later in other countries in the Middle East, Europe, and Africa. The symptoms observed are fever, cough, sore throat or chest pain, diarrhea or vomiting10. Of 2494 people infected with MERS worldwide, there were 858 deaths, with a mortality rate of 34.4%. MERS-CoV causes more deaths from pneumonia than SARS11. The evolution of this virus has shown that the coronavirus is not a stable virus and can adapt to become more virulent and even lethal to humans.
The third human zoonotic coronavirus of the century, known as SARS-CoV-2 is a Betacoronavirus (Subgenus sarbecovirus and Subfamily Orthocoronavirinae subfamily), appeared on December 1, 201912,13, causing COVID-19, a disease detected for the first time in Wuhan, Hubei Province, China14, and has become a serious infectious disease affecting human health and expanding worldwide. The source of COVID-19 is unknown, although initial cases have been linked to the Seafood Market in Wuhan, China, which also sold live animals4.
Currently, Brazil has more than 5 million people infected by SARS-CoV-2, ranking third among the countries with the highest number of infected, the first place is occupied by the United States, with more than 8 million people, followed by India with more than 7 million cases15.
Regarding mortality, Brazil ranks second with more than 154,000 deaths, and the USA, in addition to the highest number of infected, has the highest number of deaths15.
Acre - State of the Western Brazilian Amazon - is one of the states in the North region. In the native language of the Apurinãs, the first inhabitants of the state, Acre means "Aquiri" - "river of alligators". The territory of Acre belonged to Bolivia and Peru, being little by little occupied by Brazilians. It borders Peru, Bolivia, Amazonas and Rondônia. It has 164,123,737 km2 of extension and 22 municipalities16, since the last change made by Law No. 1 034, of April 28, 1992, creating the city of Jordão. Acre is the third Brazilian state with the lowest number of municipalities, losing to Roraima (15) and Amapá (16) and followed by Rondônia (52). The state is officially subdivided into five micro-regions (Brasileia, Cruzeiro do Sul, Rio Branco, Sena Madureira and Tarauacá) and two mesoregions (Vale do Acre and Vale do Juruá).
In 2010, Acre was ranked 21st in Brazil with a Human Development Index (HDI) of 0.663. According to the last sense (2010), the estimated population was 733,559 people and 894,470 for 2020, being considered the third least populous federative unit in Brazil. It has a demographic density (2010) of 4.47 inhabitants/km2 and the population over 60 years of age is 46,926 people, representing 6.40% of the population16.
The state of Acre notified its first confirmed case of infection by COVID-19 on March 15, 2020. As of 04/09/2020, the Department of Health Surveillance considered that in cities where confirmed cases were registered of COVID-19 are in the stage of community or sustained transmission, as it was not possible to establish an epidemiological link between the cases17. Temporary measures were adopted from March 16, 202018, to face the Public Health emergency resulting from the COVID-19 disease. Government Message No. 1,649, of March 19, 2020, forwards to the Legislative Assembly of the State of Acre the request for recognition of a state of public calamity, lasting until December 31, 2020, due to the pandemic. Decree No. 5.496, of March 20, 2020, established new measures to face the Public Health emergency (ACRE, 2020)16.
In June 2020 the State of Acre launched "The Acre Pact without Covid"17. It was a strategy outlined by the State Government for the gradual and responsible resumption of economic and commercial activities at the state level, to achieve harmony between economic development, the right to health protection and the social values of work. According to data from October 23, 2020, Acre registered 30,121 cases of people infected by COVID-19, with a total of 686 deaths according to the Bulletin of the Secretary of Health of Acre.
It is true that there are obvious differences in the spread of this pandemic and in mortality rates between regions, but the factors related to these spatial differences are unclear. In this context, ecological time-series studies18 are beneficial for studying each region's specificities and its associated factors. Given the above, our objective was to analyze the evolution of COVID-19 from epidemiological week (SE) 16 to SE 53 of 2020 in the State of Acre.
METHODS
Study design
This is an ecological study of descriptive time series, evaluating the State of Acre and its 22 municipalities affected by COVID-19 during SE 16 to 53 of 2020. The State of Acre consists of 22 municipalities, aggregated by five regions with a total of approximately 881 thousand inhabitants, with an HDI of 0.663. Rio Branco is the state capital with 407,000 inhabitants. The 22 municipalities were analyzed, relating to each other the HDI variables, confirmed cases per day (accumulated) and number of inhabitants.
Due to the necessary readjustments of the protocols and information system in the country and in the States, new cases of COVID-19 were not publicly available in the system, but in epidemiological reports and bulletins produced by the municipal secretariats of the State of Acre, the State Secretary of Health and by the Ministry of Health of Brazil. In this context, the cases registered in our study involved from (SE) 16 to 53, that is, from April 17 to December 31, 2020.
For the epidemiological situation, the period between April 17th and December 31st, 2020 (final date of extraction of our data) was considered. We used data on cases and deaths confirmed by the disease, by place of residence and aggregated by macro-region of the State, made available by the COVID-19 Panel of the Health Department of the State of Acre in a public, grouped, and non-nominal way.
Tables of confirmed cases per day accumulated for the twenty-two municipalities of the State of Acre were prepared. For the survey of historical facts, the website of the Health Department of Acre was consulted.
Finally, the incidence and mortality rates for the municipalities of the state were calculated, multiplying by 100,000 inhabitants. This multiplication factor was used to allow national and international comparisons. The population estimates used as denominators of Brazil were produced by the Brazilian Institute of Geography and Statistics (IBGE) and refer to the year 2019. To calculate rates per SE, the accumulated values of cases related to the last day of collection were considered.
Data analysis
Data were analyzed using the Statistical Package for Social Science (SPSS), version 23.0. Descriptive analysis was performed for all variables. Data were expressed as mean ± standard deviation or median (interquartile range), when appropriate.
We calculated the absolute number of new cases of COVID-19, per epidemiological week, for the year 2020. To assess the effect of the entry of COVID-19 in Acre on hospitalization notifications, a descriptive analysis was performed in the R software, version 3.6.3 (http://www.r-project.org).
The confirmed case per day variable can be understood as the speed or speed that infections occur, obtained from the cumulative series of cases by municipality.
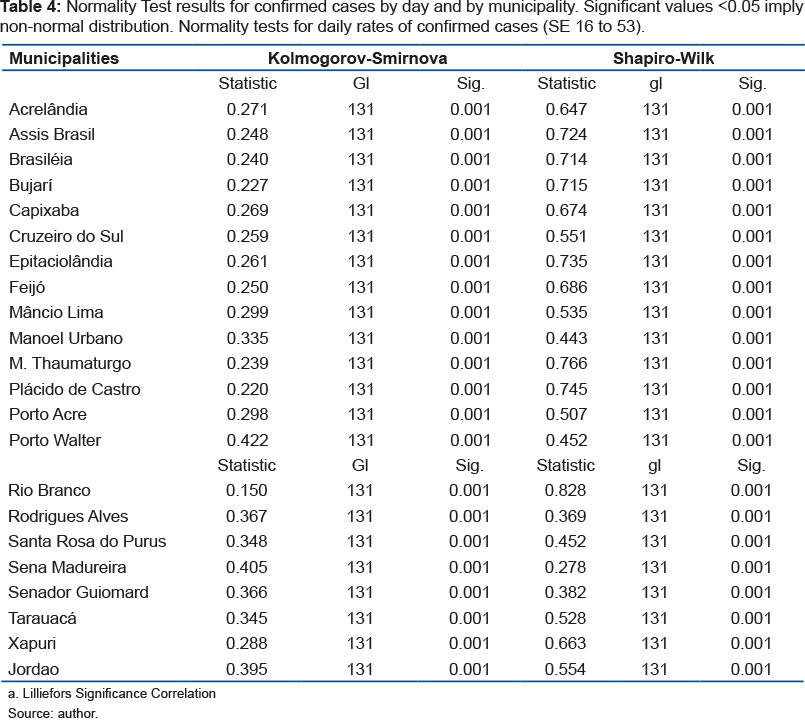
Due to problems in confirming the accumulated cases, some days the accumulated was lower than the day before, generating negative values for the variable confirmed cases per day. Therefore, these negative values were excluded from the analysis. Using the Shapiro-Wilk (SW) and Kolmogorov-Smirnov (KS) normality test, it was observed that all cases confirmed per day are not normally distributed, since in all municipalities the p-value < 0.001 for both tests.
The association between confirmed cumulative cases per 10,000 inhabitants per municipality among all 22 municipalities in the state of Acre was studied. The association was performed using Pearson's correlation coefficients (r), constructing two correlation matrices of 22 lines by 22 columns, generating 484 correlation coefficients for each type of correlation, having as reference the value of p<0.05.
To analyze the relationship between the number of accumulated cases and the HDI, the simple linear regression test was used. Analyzes were performed using SPSS 23.0 statistical software.
RESULTS
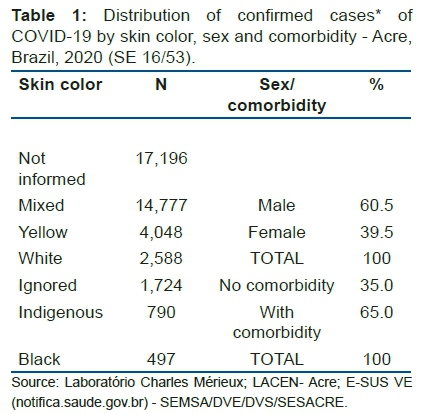
The epidemiological data in tables 1, 2 and 3 refer to general data issued in the bulletin dated 31-12-2020 referring to (SE 53) by the Health Department of the State of Acre. The intention is to demonstrate general data as close as possible to the closing of this work. The following tables refer to the data tabulated statistically during the expected period of this research, which was from (SE) 16/53, starting on April 17th and ending on August 31st, 2020.
According to the skin color variable, the largest proportion of positive cases is of mixed-race people (35.5%). However, it appears that 45.4% of confirmed cases do not have the record of this information. According to gender, 481 (60.5%) deaths occurred in males and 314 (39.5%) in females. Among the 795 deaths, 517 (65.0%) of them had some comorbidity, but it appears that 278 (35.0%) of the people who progressed to death had no history of comorbidities (table 1).
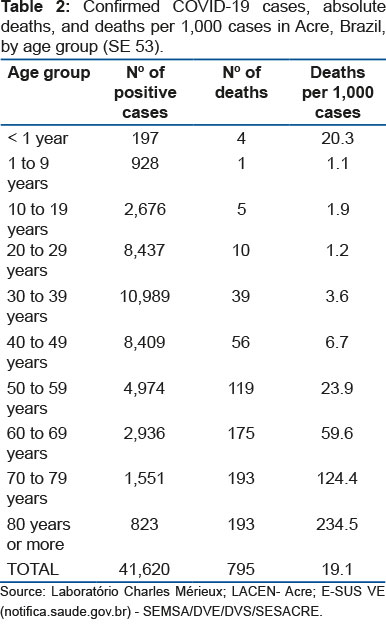
According to age group, there is a direct relationship between age and deaths: the older the age, the greater the lethality of the disease. Regarding the number of positive cases, it is observed that, despite most cases being in the age group of 20 to 49 years, lethality is found in the older age groups (table 2).
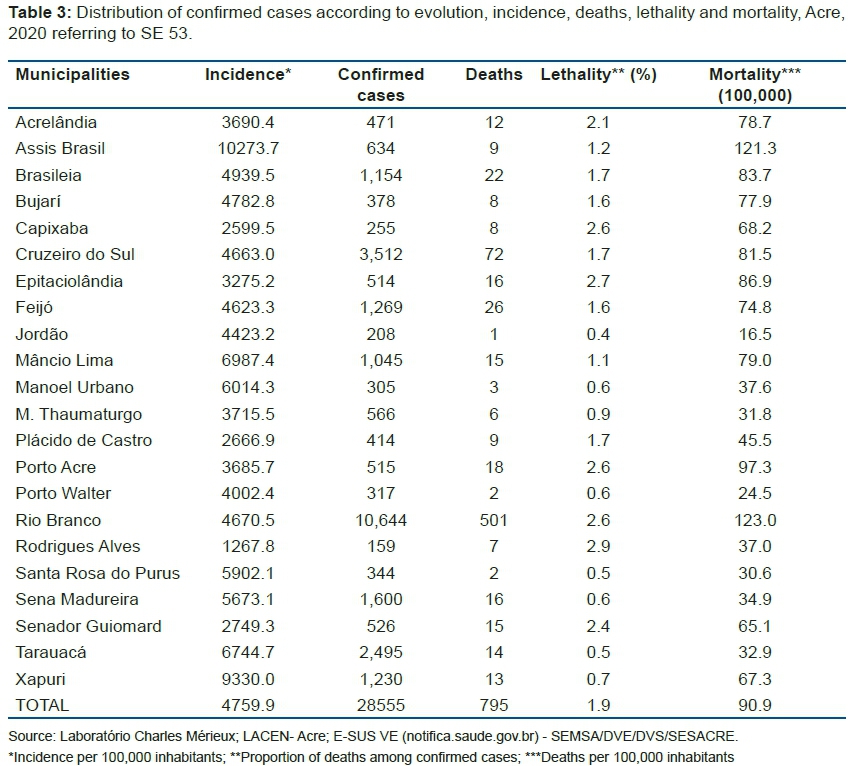
As of April 9, 2020, the Department of Health Surveillance of the State of Acre considers that municipalities with confirmed cases of COVID-19 are in the stage of community or sustained transmission, as it is no longer possible to establish an epidemiological link among cases. Most positive cases are evolving without complications, not requiring hospitalization, with only indication of home isolation for 14 days for treatment and recovery. So far, 33,670 were discharged, having completed the 14 days, and no longer showing symptoms of the disease. In table 3, however, 795 deaths were registered in the state, the municipality of Rio Branco had the highest number, 501 deaths. Acre has a mortality rate (deaths per 100,000 inhabitants) of 90.9 and a lethality rate of 1.9%, with the highest mortality rate being observed in the municipality of Rio Branco (121.3/100,000 inhabitants) and of lethality in Rodrigues Alves (2.9%). The incidence of COVID-19 in Acre is 4,759.9 cases per 100,000 inhabitants, the municipalities of Assis Brasil and Xapuri have the highest incidences in the state with 10,273.7 and 9,330.8/100,000 inhabitants, respectively (table 3).
Table 4 shows that all distributions of confirmed cases per day are NOT normal for all regions, that is, the respective p-values are always less than the significance α=0.05.
The respective p-values were lower than the significance,α = 0.05, and the correlation coefficients were always close to 1, suggesting a strong positive correlation for all accumulated cases from all municipalities with each other.
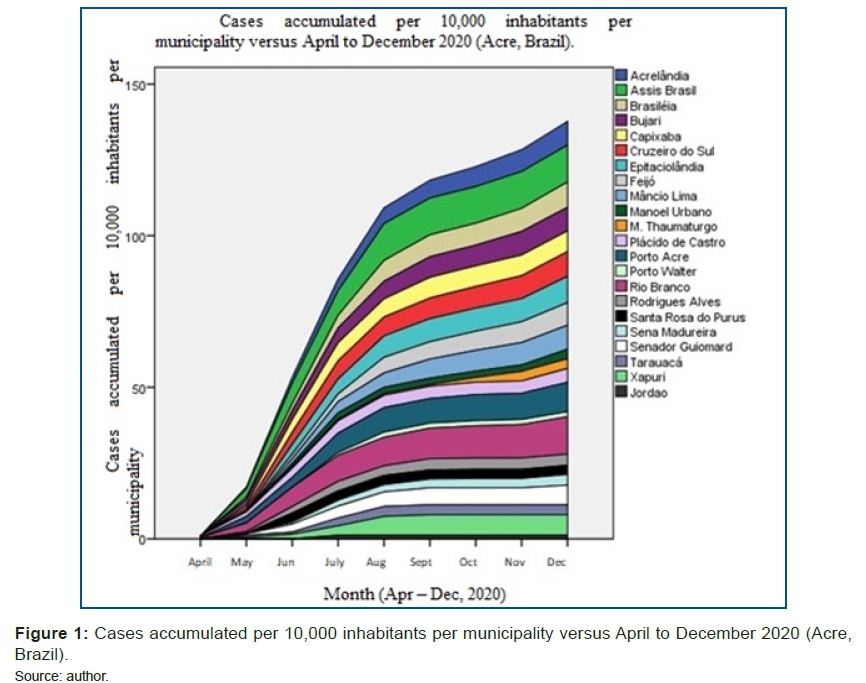
Therefore, although the accumulated numbers of cases are different for the same day, the behavior is very similar, that is, the curves vary in the same way over time, regardless of the municipality observed. The graph in figure 1 shows the cases accumulated per 10,000 inhabitants and per municipality in the period from April to December 2020.
Figure 1 shows a strong positive dependence (increasing) between the HDI and the frequency of accumulated cases of COVID-19 for the state of Acre. The rate is 39.16 cases accumulated per 10,000 inhabitants per HDI.
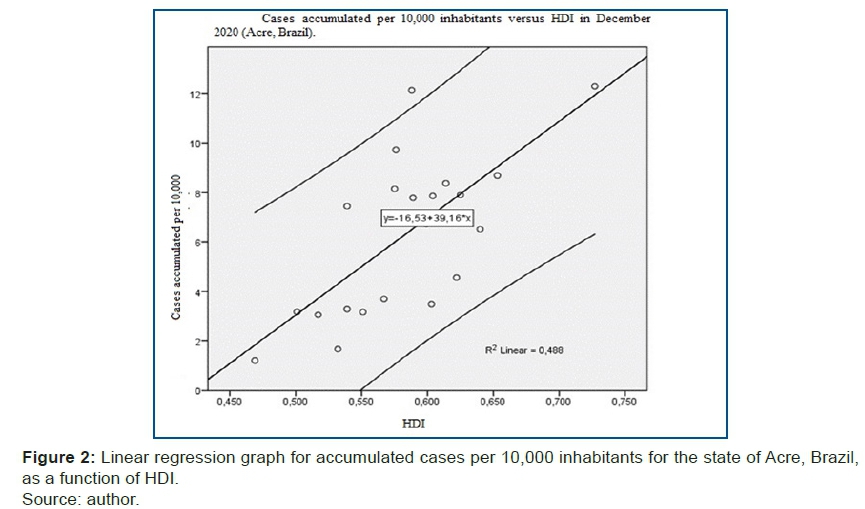
The study of the association between the variables accumulated cases confirmed per 10,000 inhabitants for the state of Acre and the month was carried out using linear regression, according to the graph in figure 2.
A positive linear regression is observed for cases accumulated per 10,000 inhabitants in the state of Acre as a function of the HDI, showing that this rate shows an upward trend, as shown in figure 2.
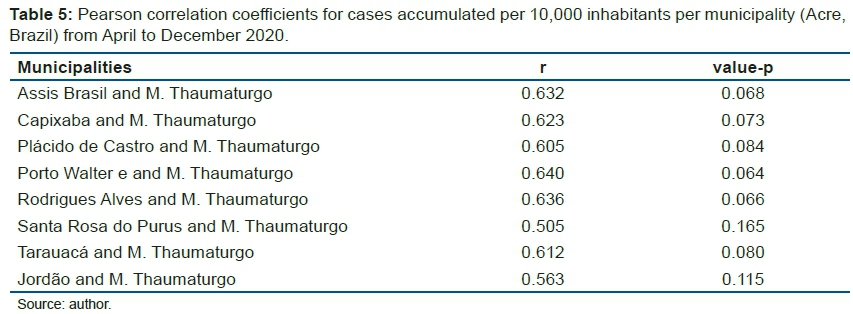
Table 5 shows that there is no significance in the correlation of cases by the municipalities analyzed, showing that even though the rate is growing, it is not possible to observe this result individually in the municipalities.
Through table 5, it is possible to observe that the frequent municipality is M. Thaumaturgo in all significant correlations because the "r" values are a little above 0.500. However, the correlations between the other municipalities were higher than r=0.800 and their respective p-values were <0.001, that is, much lower than the 0.05 significance. Therefore, we can consider a different behavior from other municipalities for its curve of accumulated cases over time for the municipality of M. Thaumaturgo that needs to be investigated.
DISCUSSION
As the main findings of our research, the population evaluated from SE 16/53 2020 of the State of Acre on COVID-19 had brown skin color as main characteristics in relation to the general data, the majority affected were male, and prevailed that the majority that progressed to death was related to age and some comorbidity.
Acre has a mortality rate (deaths per 100,000 inhabitants) of 90.9 and a lethality rate of 1.9%, with the highest mortality rate being found in the municipality of Rio Branco (121.3/100,000 inhabitants) and of lethality in Rodrigues Alves (2.9%). The incidence of COVID-19 in Acre is 4,759.9 cases per 100,000 inhabitants, the municipalities of Assis Brasil and Xapuri have the highest incidences in the state with 10273.7 and 9330.8/100,000 inhabitants, respectively.
By evaluating the cumulative data among the 22 municipalities, we identified that, despite the accumulated numbers of cases being different for the same day, the behavior is very similar, that is, the curves vary in the same way over time, regardless of the municipality observed. It was also identified that there is no significance in the correlation of the cases by the analyzed municipalities, showing that even though the rate is growing, it is not possible to observe this result individually in the municipalities. A positive linear regression is observed for cases accumulated per 10,000 inhabitants in the state of Acre as a function of the HDI, showing that this rate shows an increasing trend in confirmed cases per day and number of inhabitants, finding a strong positive correlation between confirmed cases per day. day with number of inhabitants, which also showed a correlation between the HDI and the number of inhabitants. Which leads us to say that, in fact, the number of confirmed cases per day is proportional to the number of inhabitants and HDI per region, that is, that the cases of COVID-19 in Acre are growing, proportionally per region.
Brazil is at an earlier stage of the epidemic when compared to other countries in the world, but with high incidence and mortality rates when looking at its macro-regions and states. In studies by Cavalcante et al.19, they show that absolute numbers of cases were concentrated in the Southeast region, however, the North region of the country had the highest incidence rate of the disease up to SE 20, where, according to the author, the reasons are obstacles to adherence by the population to social isolation19. Our findings corroborate those mentioned above, as the State of Acre has a high incidence rate of 4,759.9, considering the number of the existing population.
Mortality in the State of Acre is also a worrying number, as we have 90.9 per million inhabitants, with the main municipalities with high rates being Rio Branco and Rodrigues Alves. These values are above the national average, which is 67.3 per million inhabitants according to data from the Ministry of Health20.
Reports from China and Italy suggest that risk factors for serious illnesses include old age and the presence of at least one of several underlying health conditions. Older adults in the United States, including those ≥65 years and particularly those ≥85 years, also appear to be at increased risk for serious outcomes associated with COVID-19, however, data describing underlying health conditions among patients affected by COVID-19 have not yet been reported. The percentage of patients with COVID-19 with at least one underlying health condition or risk factor was higher among those who required admission to the intensive care unit (ICU) and those who required admission (no admission to the ICU), than among those who were not hospitalized. The most reported conditions were diabetes mellitus, chronic lung disease, and cardiovascular disease21-24. These international studies are reflected in our results, as most of the population evaluated from SE 16/53 2020 in the State of Acre on COVID-19 had as main characteristics, the predominance of males, and it prevailed that the majority that progressed to death it was related to advanced age above 60 years, and with one or more associated comorbidities. These preliminary findings translate that comorbidity problems associated with COVID-19 infection are at greater risk than people without these comorbidities at first.
The lethality data in the State of Acre are at the end of this study with 1.9%, considered high for the region, being distributed in all municipalities. According to world data25, which state that Brazil and other countries are facing an increasing trend of lethality.
The number of cases with COVID in Ceará, Brazil, grow in geometric progression, as in 7 days the number of cases jumped from 11 to 164 in two weeks, later, in 3 weeks the number more than doubled, as there were already 382 cases, a fact that only evidences the speed of growth to more than double. Among the results, Ceará is the third state in number of cases. On the State scale, the highest concentration occurs in the capital, in neighborhoods with a higher HDI, where middle- and upper-class people live, with the other cases in the metropolitan region and the interior of the State, with a tendency for diffusion speed less concentrated in the State's municipalities26. In our findings, the notified cases followed the same evolution as in the State of Ceará as the high number was in the municipalities with the highest HDI and quickly evolved to the interior.
In a comparison of the State of Acre with Amazonas, proportionally, Acre has a higher average in the incidence of cases per 100,000 inhabitants with 4,759.9 against 2,808 in Amazonas27. In this case, we evaluated among all municipalities in Acre against the macro-regions of Amazonas.
Studies show that confirmed cases with their evolution are directly linked to the HDI with the number of inhabitants, leading to an increase in cases proportionally to each municipality. This corroborates with studies by Dias et al., where in a recent national-level survey relating Brazilian states, they identified that the population and number of inhabitants in each location are directly related to the pandemic28.
The results showed that there is a significant difference in the number of cases per day variable depending on the region. These are the pairs of municipalities that have different values of the confirmed cases per day variable, that is, the speed of cases is different between these municipalities. In a study carried out by Li et al.29, at the beginning of the pandemic, they identified among the first 425 patients with confirmed Coronavirus Infected Pneumonia (NCIP), the mean age was 59 years and 56% were male. Most cases (55%) starting before January 1, 2020, were linked to the Huanan Seafood Wholesale Market, compared to 8.6% of subsequent cases. The mean incubation period was 5.2 days (95% confidence interval [CI], 4.1 to 7.0), with the 95th percentile of the distribution at 12.5 days. In the early stages, the epidemic doubled in size every 7.4 days. With a mean series interval of 7.5 days (95% CI, 5.3 to 19), the basic reproductive number was estimated at 2.2 (95% CI, 1.4 to 3.9). This demonstrates that the evolution of cases among the municipalities in the interior followed the same path as the studies by the author, as the interior of the State of Acre still has a lot of physical contact between fishermen and residents in municipal markets.
For Mocelin30, human infection caused by the new Coronavirus (SARS-CoV-2) or COVID-19 is a Public Health emergency of international importance, whose clinical spectrum is diverse, ranging from mild symptoms to severe acute respiratory syndrome. The lethality varies according to each country, but it is evident that the elderly and people with chronic comorbidities are the ones with the most complications. Currently, no vaccines or drugs with proven scientific evidence have been developed for their definitive treatment and, currently, clinical management is aimed at support and control of symptoms31.
The number of people infected with SARS-CoV-2 in the world is impressive. As of August 30, 2020, approximately 25 million cases and 800,000 deaths have been reported since the start of the outbreak32. The mortality rate is between 0.2% and 0.4% for the age groups between 10 and 49 years, 1% for the elderly between 50 and 59 years, 3.6% for people between 60 and 69 years and 8% for over 70s.
It points to the need for actions aimed at Public Health Policies33 that contribute to the promotion of the population's quality of life in this pandemic period, to collaborate with the promotion of occupational health. It is known that health in general is a topic that needs to be widely discussed and that the care provided to this population should focus from prevention and promotion actions to actions aimed at the control and treatment of the health problems that affect. It also emphasizes the importance of research that can contribute to new paths in achieving Public Health in the population, as well as the transfer of knowledge34,35.
Thus, during this difficult time that the world is going through due to the COVID-19 pandemic, the State of Acre is very vulnerable to this disease. A state with 894.470 thousand inhabitants, with a demographic density of 4.47 inhabitants/km2, distributed in 22 municipalities and an HDI of 0.663. A place with many contrasts and peculiar local characteristics, mainly in the interior, where we have a simple life and what prevails is hunting and fishing and local agriculture. These characteristics contributed to a faster dissemination of COVID-19, as the lack of structure and knowledge of the disease meant that many were not properly cared for.
On the other hand, we observe that the prevention problems are slowly being solved, making the population start to be more careful. Even so, the pandemic has already reached 22 municipalities, reaching indigenous villages and rubber tappers, which causes even greater concern due to the lack of structures in these places.
CONCLUSION
We conclude that the state of Acre is not different from the rest of the country in terms of increasing positive cases of COVID-19. Although the accumulated numbers of cases are different for the same day, the behavior is very similar, that is, the curves vary in the same way over time, regardless of the municipality observed.
We also identified that cases multiply quickly and continue to grow throughout the state, even though there is no correlation between individual confirmed cases. Which leads us to a general conclusion: the pandemic has infiltrated all parts of Brazil, without distinction, not separating regions, places, society, and culture.
Authors' contributions
Edimilson Lima de Assis, writing of the manuscript, following the guidelines of the journal; Mauro José de Deus Morais, data collection, conducting experiments and writing the manuscript; Valéria Rigamonte Azevedo de Assis, writing of the manuscript; Francisco Naildo Cardoso Leitão, Jorge de Oliveira Eichemberg and Maura Bianca Barbary de Deus writing of the manuscript, following the guidelines of the magazine; Maura Bianca Barbary de Deus, manuscript writing; Italla Maria Pinheiro Bezerra, data collection, conducting experiments and writing the manuscript; Luiz Carlos de Abreu, data collection, conducting experiments and writing the manuscript.
Acknowledgments
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. The financial viability of the article is due to the Acre - Health Project in the Western Amazon (multi-institutional agreement process no. 007/2015 SESACRE-UFAC-FMABC).
Conflicts of interest
We declare no potential conflicts of interest.
REFERENCES
1.Richman, Douglas D. “Antiviral Drug Discovery To Address the COVID-19 Pandemic.” Mbio. 2020; 11(5): e02134-20.
2.Wang HJ, Du SH, Yue X, Chen CX. Review and Prospect of Pathological Features of Corona Virus Disease. Fa yi xue za zhi. 2020; 36(1): 16-20. [ Links ]
3.Novel CPERE. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua liu xing bing xue za zhi= Zhonghua liuxingbingxue zazhi. 2020; 41(2): 145. [ Links ]
4.Shigemura J, Ursano RJ, Morganstein JC, Kurosawa M, Benedek DM. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiatry and clinical neurosciences. 2020; 74(4): 281. [ Links ]
5.Luo C, Yao L, Zhang L, et al. Possible transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in a public bath center in Huai'an, Jiangsu Province, China. JAMA network open. 2020; 3(3): e204583-e204583. [ Links ]
6.Silva LJ da. A Globalização da doença. Rev Saúde Pública. junho de 2003; 37 (3): 273-4. [ Links ]
7.Gärtner A, Pereira T, Simões MJ, et al. Use of hybrid chitosan membranes and human mesenchymal stem cells from the Wharton jelly of umbilical cord for promoting nerve regeneration in an axonotmesis rat model. Neural regeneration research. 2012; 7(29): 2247. [ Links ]
8.王慧君, 杜思昊, 岳霞, 陈传香. 冠状病毒肺炎的病理学特征回顾与展望. Journal of Forensic Medicine. 2020; 36(1). [ Links ]
9.Al-Osail AM, Al-Wazzah MJ. The history and epidemiology of Middle East respiratory syndrome corona virus. Multidisciplinary respiratory medicine. 2017; 12(1): 20. [ Links ]
10.Algaissi A, Agrawal AS, Hashem AM, Tseng C-TK. Quantification of the middle east respiratory syndrome-coronavirus RNA in tissues by quantitative real-time RT-PCR. In: MERS Coronavirus. Springer; 2020: 99-106. [ Links ]
11.Doucleef M. Scientists go deep on genes of SARS-like virus. September. 2012; 26: 2012. [ Links ]
12.Zhu N, Zhang D, Wang W. China Novel Coronavirus Investigating and Research Team. A novel coronavirus from patients with pneumonia in China, 2019 [published January 24, 2020]. N Engl J Med. [ Links ]
13.Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. Um novo coronavírus de pacientes com pneumonia na China, 2019. New England Journal of Medicine. 20 de fevereiro de 2020; 382 (8): 727-33. [ Links ]
14.Du Z, Wang L, Cauchemez S, et al. Risk for transportation of coronavirus disease from Wuhan to other cities in China. Emerging infectious diseases. 2020; 26(5): 1049. [ Links ]
15.Zar HJ, Dawa J, Fischer GB, Castro-Rodriguez JA. Challenges of COVID-19 in children in low-and middle-income countries. Paediatric Respiratory Reviews. 2020. [ Links ]
16.Brasil I. Instituto Brasileiro de geografia e Estatística. Censo demográfico. 2010; 2010. [ Links ]
17.Rocha de Souza I. PORTARIA Nº 122/2020/DG-Manaus, 22 de junho de 2020. [ Links ]
18.Abreu LC, Elmusharaf K, Siqueira CEG. A time-series ecological study protocol to analyze trends of incidence, mortality, lethality of COVID-19 in Brazil. J Hum Growth Dev. 2021; 31(3):491-495. DOI: 10.36311/jhgd.v31.12667 [ Links ]
19.Bufulin AP, da Cunha Braz MB, da Vitória FM. Coronavírus e direito de família: as implicações do enfrentamento da emergência de saúde pública de importância internacional decorrente do surto de Covid-19 no regime de convivência familiar. civilistica com: revista eletrônica de direito civil. 2020; 9(1): 1-15. [ Links ]
20.Cavalcante JR, Cardoso-dos-Santos AC, Bremm JM, et al. COVID-19 en Brasil: evolución de la epidemia hasta la semana epidemiológica 20 de 2020. Epidemiologia e Serviços de Saúde. 2020; 29(4). [ Links ]
21.da Silva WNT, Rosa MFP, de Oliveira SV. Produção de boletins epidemiológicos como estratégia de Vigilância em Saúde no contexto da pandemia de COVID-19. Vigilância Sanitária em Debate: Sociedade, Ciência & Tecnologia (Health Surveillance under Debate: Society, Science & Technology)-Visa em Debate. 2020; 8(3): 171-177. [ Links ]
22.Control CfD, Prevention. Severe outcomes among patients with Coronavirus Disease 2019 (COVID-19)-United States, February 12-March 16, 2020 [punlished online March 18, 2020]. Morb Mortal Wkly Rep. [ Links ]
23.Covid C, COVID C, COVID C, et al. Preliminary estimates of the prevalence of selected underlying health conditions among patients with coronavirus disease 2019-United States, February 12-March 28, 2020. Morbidity and Mortality Weekly Report. 2020; 69(13): 382. [ Links ]
24.de Oliveira JJM, de Melo Soares K, da Silva Andrade K, et al. O impacto do coronavírus (covid-19) na prática odontológica: desafios e métodos de prevenção. Revista Eletrônica Acervo Saúde. 2020(46): e3487-e3487. [ Links ]
25.Zagato L. Vírus, imperialismos, estratégias: entre meta-complôs inventados (quase todos) e complôs reais. Universidade Nômade.154. [ Links ]
26.de Moraes Bernal H, Siqueira CE, Adami F, de Sousa Santos EF. Trends in case-fatality rates of covid-19 in the world, between 2019-2020. Journal of Human Growth and Development. 2020; 30(3): 344-354. DOI: https://doi.org/10.7322/jhgd.v30.11063 [ Links ]
27.Silva JBd, Muniz AMV. Pandemia do Coronavírus no Brasil: Impactos no Território Cearense. Espaço e Economia Revista brasileira de geografia econômica. 2020. [ Links ]
28.Gomes, CA et al. Situação epidemiológica da COVID - 19 nos municípios da Regional de Saúde Rio Negro e Solimões - Amazonas. Coari, AM: Universidade Federal do Amazonas, 2020. [ Links ]
29.Dias GN, Pamplona VMS, Rodrigues AE, et al. Análise matemática e estatística da doença COVID-19 e implicações em projeções futuras. Research, Society and Development. 2020; 9(10): e4169108826-e4169108826. [ Links ]
30.Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. New England Journal of Medicine. 2020. [ Links ]
31.Mocelin HJS, Primo CC, Laignier MR. Visão geral das recomendações para a amamentação e COVID-19. JHGD. 15 de outubro de 2020; 30 (3): 335-43. DOI: 10.36311/jhgd.v31.12230 [ Links ]
32.OPAS O. OMS Brasil-Folha informativa-COVID-19 (doença causada pelo novo coronavírus)| OPAS/OMS [Internet]. Pan American Health Organization/World Health Organization. 2020. [ Links ]
33.Mocelin HJS, Primo CC, Laignier MR. Overview on the recommendations for breastfeeding and COVID-19. Journal of Human Growth and Development. 2020; 30(3): 335-343. DOI: https://doi.org/10.7322/jhgd.v30.11060 [ Links ]
34.de Abreu LC. Integrated actions and strengthening of public health system in Brazil in a time of pandemic. Journal of Human Growth and Development. 2020; 30(1): 05-08. DOI: https://doi.org/10.7322/jhgd.v30.9980 [ Links ]
35.Neves LAT. Contributions in the field of Public Health for decision-making in health. Journal of Human Growth and Development. 2017; 27(2): 128-131. DOI: https://doi.org/10.7322/jhgd.137515 [ Links ]
 Correspondence:
Correspondence:
maurodedeus@outlook.com
Manuscript received: august 2021
Manuscript accepted: september 2021
Version of record online: november 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}