










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.31 no.3 Santo André set,/dez. 2021
https://doi.org/10.36311/jhgd.v31.12183
CASE REPORT
DOI: 10.36311/jhgd.v31.12183
Guillain-Barre syndrome related to COVID-19: muscle and nerve biopsy findings
Dandara Costa Lima de SouzaI; Rafael Basílio GuimarãesII; Alzira Alves de Siqueira CarvalhoI
IDepartment of Neurosciences - Neuromuscular Service, Centro Universitário Saúde ABC, Santo André, SP, Brazil
IIDepartment of Neurosurgery - Centro Hospitalar do Município de Santo André, Santo André, SP, Brazil
ABSTRACT
BACKGROUND: the involvement of the peripheral nervous system (PNS) in COVID-19 is rare and, to date, morphological aspects from muscle and nerve biopsies have not been reported. Here, we describe a case of Guillain-Barré Syndrome (GBS) related to COVID-19 and demonstrate findings from peripheral nerve and skeletal muscle biopsies. A 79-year-old man presented with progressive weakness in both legs over one-week, evolving to both arms and urinary retention within 6 days. Four days earlier, he had a cough, febrile sensation and mild respiratory discomfort. On admission, his was afebrile, and without respiratory distress. A neurological examination disclosed asymmetric proximal weakness, diminished reflexes and no sensitive abnormalities. Three days later, the patient presented with bilateral facial weakness and proximal muscle strength worsened. Deep tendon reflexes and plantar responses were absent. Both superficial and profound sensitivity were decreased. From this point, oxygen saturation worsened, and the patient was placed on mechanical ventilation. CSF testing revealed one cell and protein 185 mg/dl. A chest CT showed the presence of ground-glass opacities and RT-PCR for SARS-CoV-2 was positive. The muscle biopsy revealed moderate neuromyopathic findings with positive expression for MHC-class I, C5b9, CD8 and CD68. The nerve biopsy showed inflammatory infiltrates predominantly with endoneurial compound formed by CD45 and CD68. The patient was treated with Oseltamivir for 9 days followed by IVIG for 5 days and died three days later of septic shock.
DISCUSSION: this is the first documented case of GBS associated with COVID-19 with a muscle and nerve anatomopathological study. A systematic review about neurological complications caused by COVID-19 described 11 patients with GBS. The morphological features reported in our patient showed signs of involvement of the immune system, suggesting that direct viral invasion could have played a role in the pathogenesis of peripheral nerve injury. Hereafter, further research will be necessary to understand the triggers for these cells migrating into the peripheral nerve.
Keywords: COVID-19, Peripheral nervous system, biopsies, Guillain-Barré Syndrome.
RESUMO
INTRODUÇÃO: O envolvimento do sistema nervoso periférico (SNP) na COVID-19 é raro e, até o momento, os aspectos morfológicos de biópsias de músculo e nervo não foram relatados. Descrevemos um caso de Síndrome de Guillain-Barré (SGB) na vigência de COVID-19 destacando os achados na biopsia de músculo e nervo. Um homem de 79 anos apresentou fraqueza progressiva em ambas as pernas ao longo de uma semana, evoluindo para ambos os braços e retenção urinária em 6 dias. Quatro dias antes, apresentou tosse, sensação febril e leve desconforto respiratório. Na admissão, apresentava-se afebril e sem alteração respiratória. O exame neurológico mostrou fraqueza proximal assimétrica, reflexos diminuídos e sensibilidade preservada. Três dias após, o paciente evoluiu com fraqueza facial bilateral e piora da força muscular proximal. Reflexos tendinosos profundos e cutâneo plantar ausentes bilateralmente. A sensibilidade superficial e profunda estavam diminuídas. Evoluiu com piora na saturação de oxigênio sendo colocado sob ventilação mecânica. O exame de liquor revelou uma célula e aumento de proteína (185 mg / dl). A TC de tórax revelou a presença de opacidades em vidro fosco e o RT-PCR para SARS-CoV-2 foi positivo. A biópsia muscular mostrou achados neuromiopáticos moderados com imunoexpressão positiva para MHC classe I, C5b9, CD8 e CD68. A biópsia de nervo revelou infiltrado inflamatório inflamatórios predominantemente endoneural composto por CD45 e CD68. O paciente foi tratado com Oseltamivir por 9 dias seguido de IVIG por 5 dias indo a óbito após três dias por choque séptico.
DISCUSSÃO: Este é o primeiro caso documentado de SGB associada a COVID-19 com estudo anatomopatológico de músculo e nervo. Uma revisão sistemática de complicações neurológicas associadas à COVID-19 descreveu 11 pacientes com SGB. As características morfológicas em nosso paciente mostrando sinais de envolvimento do sistema imunológico sugere que a invasão viral direta pode ter colaborado no processo patogênico da lesão neuromuscular. A partir daí, mais pesquisas serão necessárias para entender os gatilhos para essas células migrarem para o nervo periférico.
Palavras-chave: COVID-19, Sistema nervoso periférico, biópsias, Síndrome de Guillain-Barré.
Authors summary
Why was this study done?
The primary manifestation of COVID-19 is respiratory, but neurological features are also being reported in the literature as case reports and case series.
What did the researchers do and find?
We describe a case of Guillain-Barré Syndrome (GBS) related to COVID-19 and present the findings from nerve and muscle biopsies.
What do these findings mean?
Identifying the manifestation of Guillain-Barré Syndrome (GBS) related to COVID-19 and through biopsy findings indicates that it is necessary to further investigate the potential outcomes related to COVID-19 infection.
BACKGROUND
The primary manifestation of COVID-19 is respiratory, but neurological features are also being reported in the literature as case reports and case series. However, the mechanism involved in the induction of neurological manifestations is not well known1. Peripheral nervous system (PNS) involvement is notably scarce and morphological aspects from muscle and nerve biopsies have been scarcely reported2,3. Here, we describe a case of Guillain-Barré Syndrome (GBS) related to COVID-19 and present the findings from nerve and muscle biopsies.
REPORT OF A CASE
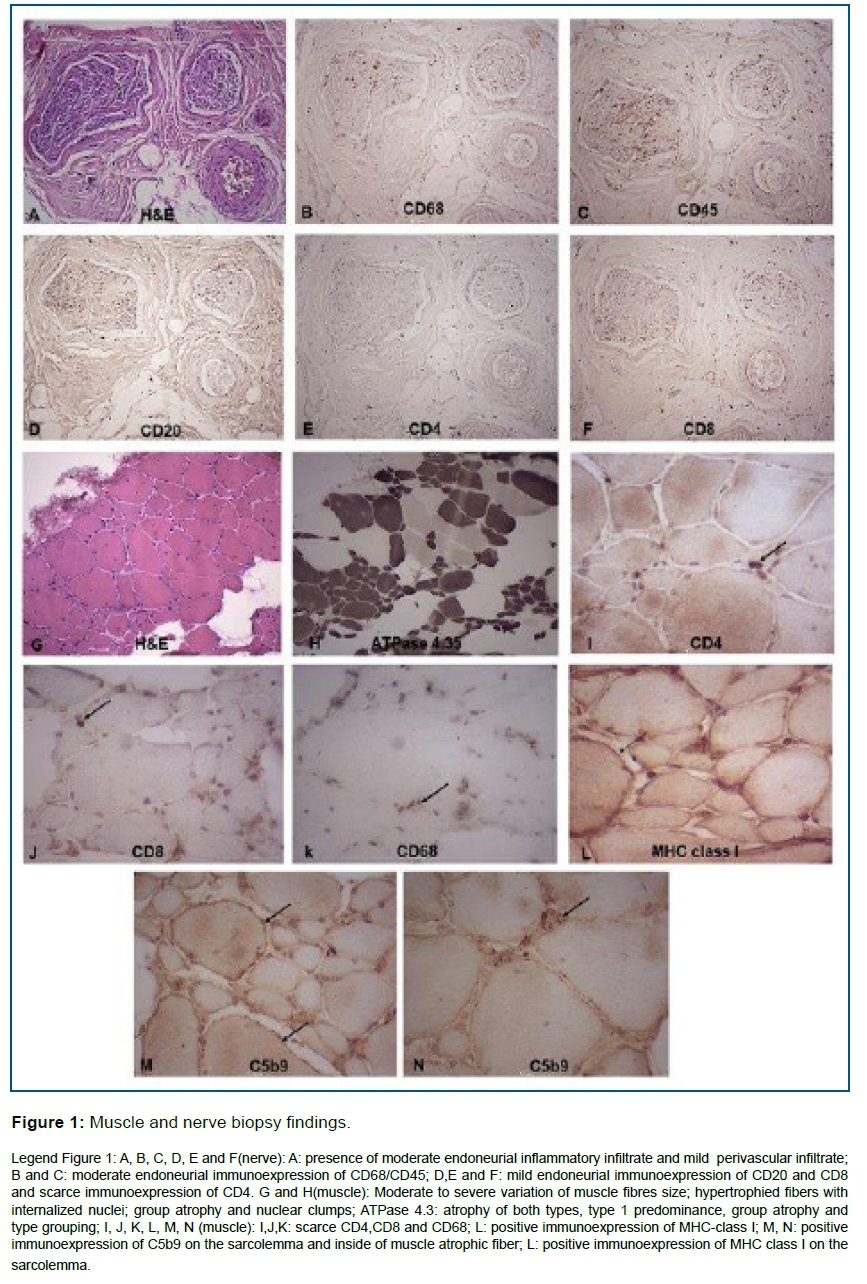
A 79-year-old man presented with progressive weakness in both legs evolving over one-week to both arms, and urinary retention within 6 days. Four days earlier he had cough, febrile sensation and mild respiratory discomfort. Relevant conditions of his medical history included hypertension, hypothyroidism and controlled type 2 diabetes. No previous neurological history was reported. On admission, he was afebrile, oxygen saturation was 96% and the respiratory rate was 16 breaths per min. Neurological examination disclosed asymmetric proximal weakness (3/5 right upper limb and left lower limb; 2/5 left upper limb and 1/5 right lower limb) and diminished reflexes. There were no sensitive abnormalities. Three days later, the symptoms progressed, presenting with bilateral facial weakness, and proximal muscle strength worsened. Deep tendon reflexes and plantar responses were absent. Superficial and profound sensitivity were decreased. From this point, oxygen saturation worsened (under 94%), the patient was placed on mechanical ventilation and transferred to an intensive care unit. Laboratory results, including creatine kinase, were normal except for an increased erythrocyte sedimentation rate of 60 mm. CSF testing revealed one cell, protein 185 mg/dl, glucose 60 mg/dl, with normal cytology and sterile cultures. Recent infection of CMV, HIV, HTLV, syphilis and hepatitis were also negative. Conduction studies and EMG were not done due the peak of this pandemic. Brain computed tomography (CT) was normal and a chest CT showed the presence of ground-glass opacities with severe pulmonary involvement. Oropharyngeal and nasopharyngeal swabs were positive for SARS-CoV-2 on the RT-PCR assay. A muscle fragment from tibialis anterior revealed moderate to intense variation in muscle fibre size; hypertrophied fibres with internalised nuclei, nuclear clumps, small group atrophy and atrophy of both types. Immunohistochemical results showed positive immune expression for MHC-class I and C5b9, and scarce CD8 lymphocytes and CD68 macrophages. A sural nerve biopsy showed an inflammatory infiltrate, predominantly endoneurial, formed mainly by CD45 leucocytes and CD68; CD4, CD8, CD20 lymphocytes were rare. (Figure 1). The patient was treated with Oseltamivir for 9 days followed by IVIG administration (0.4 g/kg) for 5 days. Although the pulmonary condition remained unchanged, the patient presented improvement in his neurological condition. Three days after IVIG administration, he died of septic shock.
DISCUSSION
To our best of knowledge, this is the first case of GBS associated with COVID-19 together with a muscle and nerve anatomopathological study. PNS manifestations are rare, with the most common being hypogeusia (5.6%) and hyposmia (5.1%), while skeletal muscle complaints were report in 10.3% of patients2-4.
Recently, a systematic review about neurological complications caused by COVID-19 reported 6 publications about GBS, totalling 11 patients and only 2 cases of rhabdomyolysis5. Patients infected with COVID-19 showed significantly higher blood levels of cytokines and chemokines6.
The morphological features described in our patient showed signs of involvement of the immune system, suggesting that direct viral invasion could have a role in the pathogenesis of peripheral nerve injury. However, one previous article analysed nerve biopsies from 35 autopsies who died with COVID-19 and demonstrated that Covid-19 immunohistochemistry was negative in muscle and nerve in all patients2. Both tissues, nerve and muscle showed inflammatory and immune-mediated damaged probably associated to cytokines activation2,3.
The inflammatory cell infiltrate, characterised mainly by the presence of CD45 and CD68, confirmed the activation of phagocytosis and cytokine production which play an essential role as regulator of macrophages or T(Th) cells7. Also, the predominant cell infiltrate in endoneurial regions drew our attention to the similarities observed in nerve biopsies from patients with HIV, including polyneuropathy which shows inflammatory cell infiltrates affecting endoneurial and/or epineurial small vessels8.
The muscle biopsy findings also favour the participation of the immune system in the pathogenesis of muscle lesions. Although the infiltrated cells were scarce (CD4, CD8, CD68, CD20), the expression of MHC-class I on the sarcolemma and C5b9 on the sarcolemma and sarcoplasm point to the activation of cytotoxic T cells and complement pathway, respectively. Lately, Aschman et al, studied muscle and myocardial inflammation in patients with COVID-19 in a series of 43 patients who died after COVID-19 . Most saples showed signs od myositis ranging from mild to severe grade. The inflammatory process in skeletal muscle was related to duration of illness suggesting that the disease could be associated with a immune-mediated myopathy, postinfectious3. In our case, the muscle and nerve alterations was found from the beginning of the disease.
Hereafter, further research will be necessary to understand the triggers for these cells migrating into the peripheral nerve.
REFERENCES
1.Ahmad I, Rathore FA. Neurological manifestations and complications of COVID-19: A literature review. J Clin Neurosci. 2020; S0967-5868(20)31078-X. doi: 10.1016/j.jocn.2020.05.017 [ Links ]
2.Suh J, Mukerji SS, Collens SI, Padera RF Jr, Pinkus GS, Amato AA, Solomon IH. Skeletal Muscle and Peripheral Nerve Histopathology in COVID-19. Neurology. 2021 Aug 24;97(8):e849-e858. doi: 10.1212/WNL.0000000000012344. Epub 2021 Jun 7. PMID: 34099523. [ Links ]
3.Aschman T, Schneider J, Greuel S, Meinhardt J, Streit S, Goebel HH, Büttnerova I, Elezkurtaj S, Scheibe F, Radke J, Meisel C, Drosten C, Radbruch H, Heppner FL, Corman VM, Stenzel W. Association Between SARS-CoV-2 Infection and Immune-Mediated Myopathy in Patients Who Have Died. JAMA Neurol. 2021 Aug 1;78(8):948-960. doi: 10.1001/jamaneurol.2021.2004. PMID: 34115106. [ Links ]
4.Mao L, Jin H, Wang M, et al. Neurologic Manifestations of Hospitalized Patients with Coronavirus Disease 2019 in Wuhan, China [published online ahead of print, 2020 Apr 10]. JAMA Neurol. 2020; e201127. doi:10.1001/jamaneurol.2020.1127 [ Links ]
5.Munhoz RP, Pedroso JP, Nascimento FA et al. Neurological complications in patients with SARS-CoV-2 infection: a systematic review. Arq Neuropsiquiatr: 2020; 1-11; https://doi.org/10.1590/0004-282X20200051 [ Links ]
6.Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020; 109:102433. doi: 10.1016/j.jaut.2020.102433. [ Links ]
7. Iwasaki A, Medzhitov R. Control of adaptive immunity by the innate immune system. Nat Immunol. 2015;16(4):343-353. doi:10.1038/ni.3123 [ Links ]
8.Robinson-Papp J, Simpson DM. Neuromuscular diseases associated with HIV-1 infection. Muscle Nerve. 2009;40(6):1043-1053. Doi:10.1002/mus.21465. [ Links ]
 Correspondence:
Correspondence:
neurogenetica@fmabc.br
Manuscript received: november 2020
Manuscript accepted: may 2021
Version of record online: november 2021


{kind=link}