










Servicios Personalizados
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.1 Santo André ene./abr. 2022
http://dx.doi.org/10.36311/jhgd.v32.12615
ORIGINAL ARTICLE
doi: 10.36311/jhgd.v32.12615
Judicialization of health care in the Western Amazon: collective decisions of the jurisdictional court of justice in the State of Acre, Brazil
José Luiz Gondim dos SantosI, II; David Wilson de Abreu PardoIII; Paulo André Stein MessettiII; Sandra Dircinha Teixeira de Araújo MoraesII; Alan Patricio da SilvaII; Francisco Naildo Cardoso LeitãoII; Blanca Elena Guerrero DaboinII; Italla Maria Pinheiro BezerraIV; Luiz Carlos de AbreuI, II, IV
IMaster's Degree in Health Sciences from the Faculdade de Medicina do ABC (FMABC) - Santo André (SP), Brazil;
IILaboratory of Study Design and Scientific Writing. University Center FMABC, Santo André (SP), Brazil;
IIICenter of Legal Sciences of the Federal University of Acre - UFAC, Rio Branco (AC) and Federal University of Brasília - UnB, Brasília (DF);
IVPostgraduate Program in Public Policies and Local Development. EMESCAM - School of Sciences of Santa Casa de Misericórdia de Vitória / ES, Brazil
ABSTRACT
INTRODUCTION: the judicialization of health is an alternative to the health services in Brazil, despite criticism of judicial decisions and control of public health policy. The large number of actions that demand health services is a health problem that characterizes the political, social, ethical, legal, and health systems of the Public Health Policy
OBJECTIVE: to analyze the judicialization of health care in the Acre State, Brazil, from 2010 to 2016
METHODS: it is a documentary and cross-sectional study of collegiate decisions, with final judgments, in the period from 2010 to 2016, issued by the Court of Justice of the State of Acre
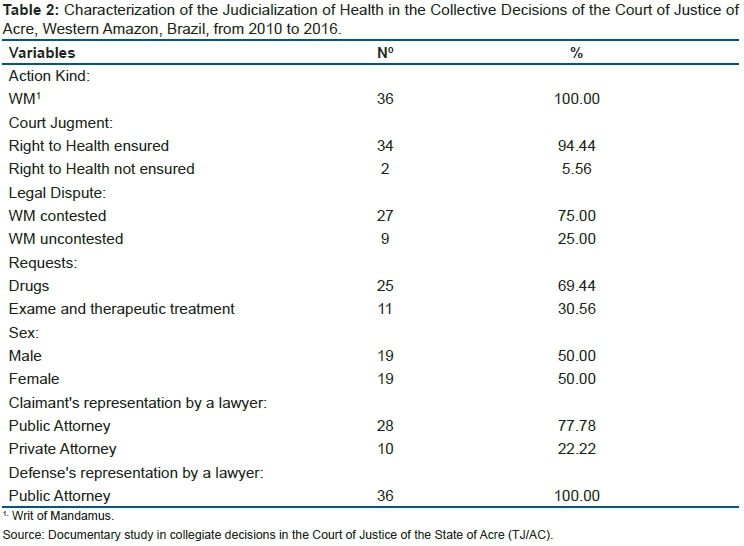
RESULTS: all proposed actions were Writ of Mandamus. The use of preliminary injunction was the most common strategy (n = 34; 94.44%). One third of the respondents were not questioned by the State of Acre (n = 9; 25%) as decisions of the Court of Justice on health concern medicines, examinations, and procedures, in these cases, it only manages interests, with no litigation per se. (n = 25, 69.44%). Men and women demanded in the same proportion, all of them characterized by living in poverty (n = 28; 77.78%
CONCLUSION: the collective health decisions handed down by the State Court of Justice Acre, Brazil, guarantee access to health goods and services to the claimants, with emphasis on preliminary injunctions and grounds based on the principle of human dignity, physical integrity and life, and on medical prescriptions in each specific case and, in a third of the cases, serving as a mere administration of interests
Keywords: public health policy, judicial decisions, legal procedural law, health judicialization.
Authors summary
Why was this study done?
Analyze the main issues concerning the judicialization of health in collegiate decisions in the State of Acre from 2010 to 2016.
What did the researchers do and find?
The authors analyzed 36 (thirty-six) collegiate decisions at the Court of Justice of the State of Acre and examined the interests under discussion, with their motivating factors, circumstances, and outcomes. The analyzed writs of mandamus had the objective to access medicines, examinations, and the referral of the plaintiffs to the treatment of care outside the home.
What do these findings mean?
Contribute to the understanding of the judicialization profile of health care in Brazil. The judicialization of health in the State of Acre means access to medicines and services based on the medical prescription of each particular case, regardless of the complexity of diagnosis or treatment.
INTRODUCTION
The judicialization of health is the search for the judicial system as the ultimate alternative to obtain the drug prescription or service denied by the public or private health provider, either for out of stock or budgetary issues. It reflects a flawed health system, which can not fully satisfy the protection of this fundamental right1.
Since 1990, the judicialization process has been present in South and Central America. Still, in Brazil, it exhibits many demands attended by the Judiciary, involving discussions among managers and health professionals, politicians, lawyers, in the most varied political, social, ethical and legal contexts2.
The scope and social repercussion of the theme caused the Federal Supreme Court (STF) to categorize the judicialization of health as a public health problem present in all Brazilian states3,4.
The Unified Health System (SUS) is responsible for the creation and implementation of public health policies. It is administered, executed, and controlled by the Executive Branch at all three levels of government (Federal, State, and Municipal), with established hierarchy and decentralization of actions and responsibilities, promoting health for all in the national territory, regardless of the requirement5.
Brazil recorded 1.346,931 processes in the health area as of December 2016, with 214,947 lawsuits related to medical-hospital treatment or medicine supply by the SUS6. In the same year, the State of Acre presented 320 legal actions, 82 related to hospital medical treatment or supply of medical drugs (SUS)7.
The structuring of the right to health through public policy makes the Executive Branch responsible for creating infrastructure and human resources to guarantee a good quality health service to the citizen. It is the responsibility of the Judiciary to control it without prejudice to all criticisms regarding the capacity technique and social effectiveness of judicial decisions8,9 affecting SUS management and financing systems.
It is evident that the search for judicial intervention for access to medicines, services, treatments reflects a mismatch between public health needs and the provision of universal, integral, and equitable care to citizens10.
In the context of judicial control of the public health policy by the Judiciary, the Executive Branch's challenge is the reduction of the number of judicial litigation. Hence, it is essential to understand the causes and effects of judicialization in the public health policy system8, mainly due to the regional diversity of the Brazilian states, such as Distrito Federal11, Pernambuco, Rio Grande do Sul, and Minas Gerais12-14.
In this way, the Executive Branch must adopt approaches to the political and collective construction of the right to health, distinguishing the legitimate interests of each actor involved, establishing an effective institutional dialogue in resolving public health conflicts15,16. In addition ethical commitment, must be adopted to ensure the balanced performance of each actor, governmental organization, and social organization involved in guaranteeing the right to health17.
Regional approaches to the judicialization of health are necessary to understand the problems of access to health in Brazil and adopt an efficient and effective public health policy.
The present study is based on the premise that collegiate decisions on Health Judicialization are legal and constitutional. Moreover, understanding that the apparent divergence between Public Authorities and users is the result of a conflict directed at the resilience of the Judiciary, aiming at the realization of Brazilian SUS principles and human dignity above all.
Thus, the objective of this study is to analyze the collegiate decisions on the of health's judicialization in the State of Acre, Brazil, from 2010 to 2016.
METHODS
Study Design
It is a cross-sectional documentary study18 with secondary data collected in the judgments of the Court of Justice of the State of Acre (TJ / AC), Western Amazon, Brazil, whose decisions were related to health services in the SUS from 2010 to 2016. It defined legal terms for this data collection as follows:
- Monocratic decisions: they are judicial decisions pronounced by a single magistrate;
- Infringing embargoes: it is an appeal filed against a monocratic decision of the rapporteur and is intended to review the decision19;
- Amendment of Judgment: refers to a legal instrument (appeal) whereby a party to a judicial process asks the judge (or Court) to clarify particular aspect (s) of a decision given when there is any doubt, omission, or contradiction in judgments20;
- Writ of Mandamus: are lawsuits that seek to protect a clear legal height; being this the right whose proof of the factual support is pre-constituted, when there is no need to demonstrate the facts that sustain it by the instruction of the process21;
- Out-of-home treatment: these are situations in which the State can not guarantee health treatment in its locality, needing to be referred from its locality to centers referenced within or outside the State, at the discretion of the Acre medical committee22;
- Plaintiff: it is the part of the process that holds a right or interest and seeks, by legal action, to obtain a good, to ensure protection and others19;
- Defendant: it is the part of the process that is legally responsible for the safeguard and guarantee of a right19;
- Interest: it is the condition for filing the lawsuit qualified by the necessity and utility, since the actual situation of the plaintiff admits the service of a need in a helpful and timely manner by judicial means19;
- Claim: it is the request of the satisfaction of an interest (a right) of the plaintiff with the Judiciary Power;
- Dispute: it is the defendant's resistance resistance to the satisfaction of an interest (a right) of the plaintiff sought from the Judiciary Branch19.
Study Location and Period
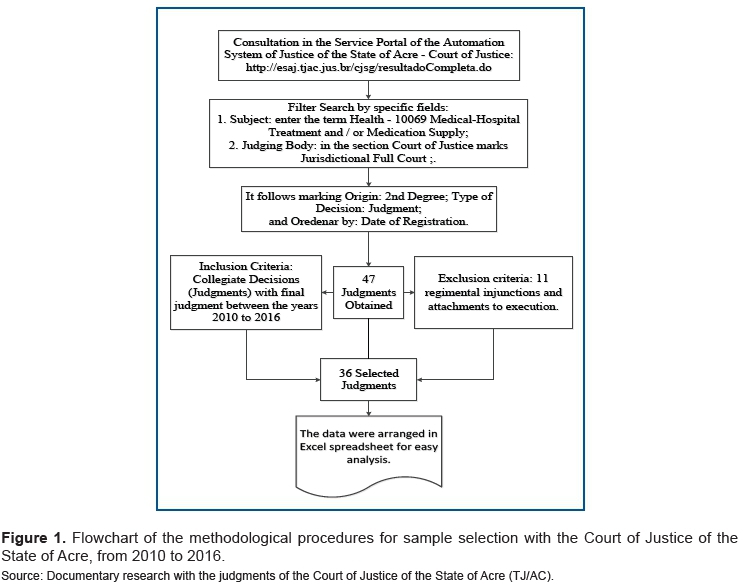
The data were collected in the Service Portal of the Judicial Automation System (e-SAJ) of the State of Acre, (http://esaj.tjac.jus.br/cjsg/resultadoCompleta.do), for the period 2010-2016.
Study Population and Eligibility Criteria
The e-SAJ portal is an automation system that promotes the integration of information among institutions of the justice ecosystem and brings the justice of all citizens closer together, adopted by the Court of Justice of the State of Acre (TJ / AC) to exchange information and streamline procedures through online services for use by lawyers, citizens, and court officials.
The data extraction was performed using the following descriptors: Health - Medical-Hospital Treatment 10069 and / or Drug Supply. In the following, the operating system of the Court of Justice of the State of Acre, Brazil offers the following fields: judicial body (Court of law), origin (second degree), type of publication (judgment), order by date of publication.
Data Collection
The information of 47 judgments were found during the examined period. After applying the inclusion and non-inclusion criteria, 11 decisions were excluded because they were monocratic. Subsequently, thirty-six (36) decisions were considered on judicializing the right to health.
The criteria for inclusion were judgments (decisions of collegiate courts) delivered by the Full Court of the Court of Justice of the State of Acre. A collegiate decision does not allow further discussion in higher Court in medical treatment and / or supply of medicines. The exclusion criteria were: internal appeal by a court (infringing liens) and declaration liens.
Data Analysis
The data were tabulated in Microsoft Excel, and the descriptive statistic was applied to consider the percentage of the judicialization of health requirements.
Ethical and Legal Aspects of the Research
CEP CEA CAAE approval: 60249316.0.0000.5624, Opinion no. 1.802.271.
RESULTS
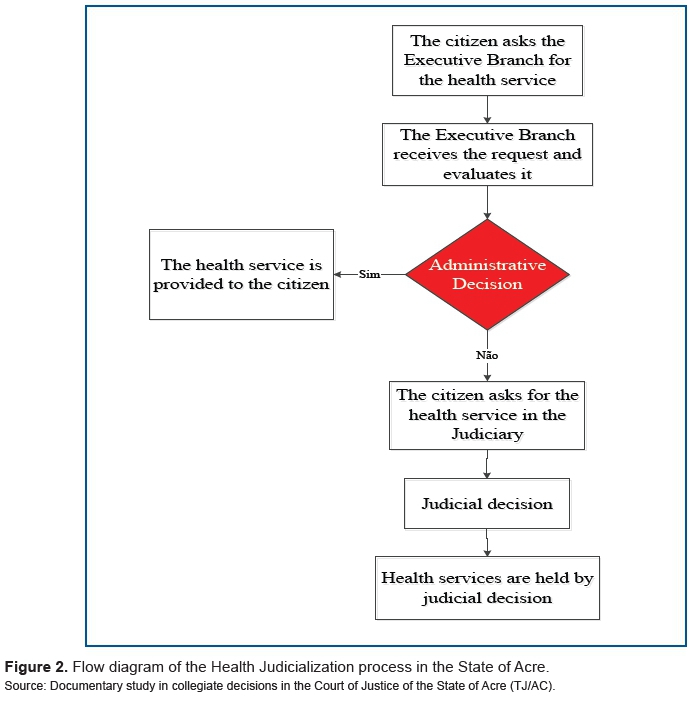
Judicial decisions on a writ of mandamus are preceded by the failure or omission of the State of Acre to provide essential health services to the citizens, who seek in the Judiciary to meet their needs and fulfill their health rights (figure 2).
Thirty-six (36) collegiate decisions were found to analyze and evaluate the legal steps to assure their right to health. They identify the factors and circumstances that motivated the demand, the profile of the plaintiff and the nature of his judicial representation (public or private), the legal principles used by magistrates, and the outcome.
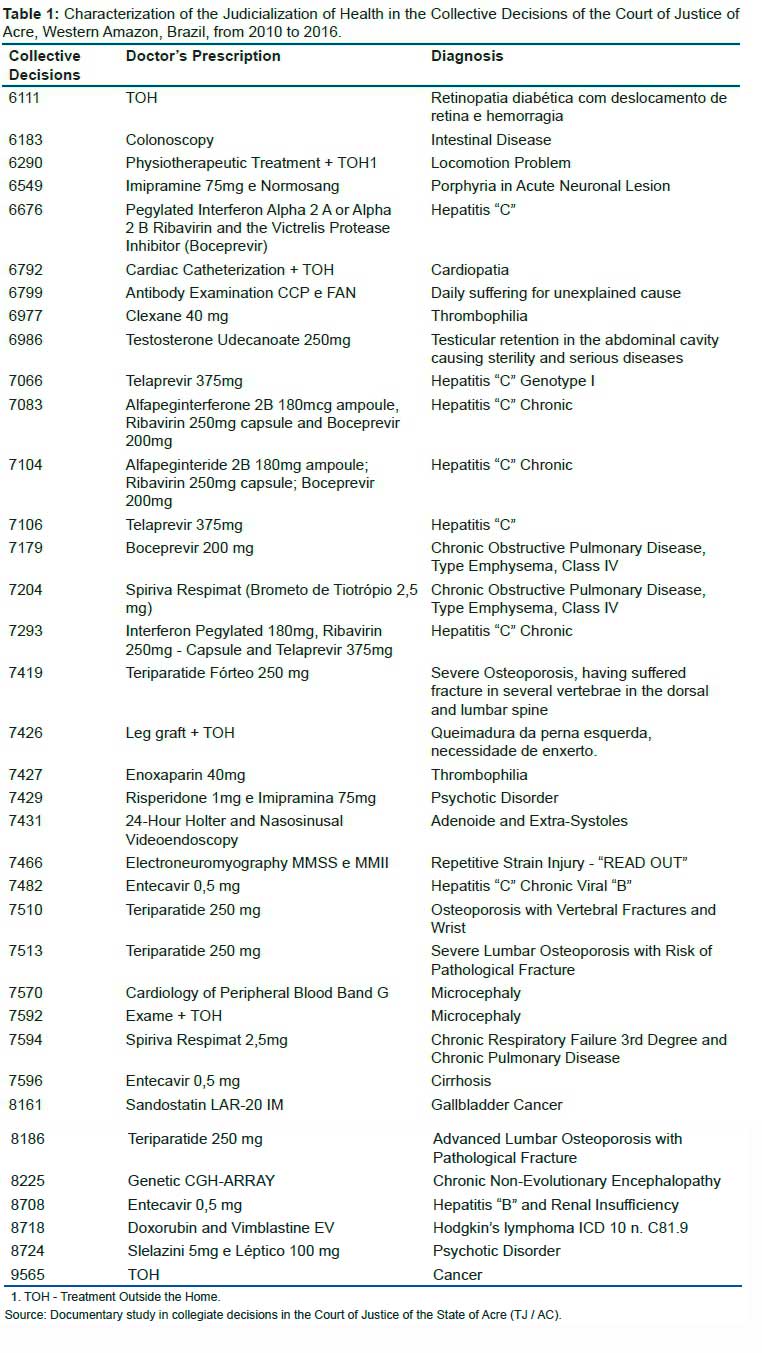
The analyzed writs of mandamus had the objective to access medicines, examinations, and the referral of the plaintiffs to the treatment of care outside the home. The most frequent diagnoses are viral hepatitis B or C. The most requested applications are pegylated interferon-alpha two or alpha 2 b, ribavirin, protease inhibitor Victrelis (Boceprevir), Telaprevir 375 Entecavir 0.5 mg. In contrast, the second most frequent diagnosis was osteoporosis, which had Teriparatide Fortéo 250 mg (table 1).
All the actions proposed in the period under study were imposed by writ of mandamus (MS). Most of the cases supported the right to health of the plaintiffs by injunctions, duly confirmed in a final merits decision (table 2).
Nine lawsuits were not contested by the State, which contemplated the sale of medicines, followed by examinations and treatments.
DISCUSSION
In the analysis of the collective health judicial decisions issued by the Court of Justice of the Acre State, from the Full Jurisdictional Court, the results report that all actions proposed in the period under study were writ of mandamus (WM). And, 94, 4% (n = 34) of the requests were granted by injunctions, duly confirmed on merits in these same cases (table 1).
There is evidence of a high level of legal health demands, such as those reported by Travassos12 (91.2%) and Gomes8 (93.6%), noting that judicial measures are urgent and emerging, requiring rapid action the Judiciary to safeguard the plaintiff's physical integrity and life.
The study reveals a regional peculiarity that a quarter of the demands, 25% (n = 9), have not been contested by the State of Acre. There are no similar records in the literature, and in this case, despite the possibility of interfering with the judicial action of the State of Acre. It is possible that the Executive Branch uses judicial channels for the purpose of granting the health service or input under the scrutiny of legality, but without due administrative proceedings for public procurement, a time-consuming and laborious procedure, especially in the case of medicines.
The absence of litigation in health actions transforms the Judiciary into a mere administrator of public-private interests, which distorts the judicial function and reveals the need for a new mechanism of state action to resolve public health litigation. In this context, the judicialization of health legitimizes the expenses in front of the control organs, allowing the purchase of medicines and the solicitation of medical exams without bidding.
The absence of litigation in health demands induces the adoption of institutional arrangements that favor conciliation and / or mediation23.
The health demands, in most cases, are about the judicial discussion of access to medicines, observing this situation in other States of the Federation, motivated by the divergence between the medical prescription and the indications contained in the Clinical Protocols and Therapeutic Guidelines (PCDT) of the SUS11-13.
The divergences of PCDT from SUS and medical prescriptions, which are always prevalent over those in the cases studied, bring as possible consequences the risk to the health of the applicant because there is no scientific proof as to the suitability and efficacy of the drug and / or service and / or procedure for the treatment of the health need of the petitioner. A clear example of this situation was the granting of 13,000 preliminary injunctions for the supply of synthetic phosphoethanolamine24, an experimental drug, at the time considered a remedy by the Judiciary, without the protection of CPTGs, violating the principles of bioethics25,26 and endangering of thousands of people.
In order to provide greater legal certainty to judicial decisions on health, the National Council of Justice (CNJ) issued Recommendation No. 31 of October 30, 2010, establishing to the Courts the adoption of measures aimed at better subsidizing judges and other to ensure greater efficiency in the resolution of lawsuits involving health care, including the adoption of technical assistance centers in health27 and that the basis of the decisions consider scientific evidence27,28.
The judicialization of health can not be a prejudicial factor to society29 and the judicial granting of health services, inputs and procedures with observance of the PCDTs of the SUS, with the assistance of health technical assistance centers and based on scientific evidence are objective and firm criteria for provide the universality, completeness and equity of SUS.
The resolution of the difficulties regarding the incorporation of technologies in the SUS goes through legal, administrative and technological evolution issues, noting that advances in Brazilian legislation have sought to reduce the time of evaluation and incorporation of services and inputs30, but the time of management never will be the time of need and urgency of health care.
It is also worth noting that the health court in the State of Acre concerning requests for services of examinations and procedures, which occurred in 30.56% (n = 11), emphasizing that in six cases the request was associated with the referral of the petitioner to the treatment of care outside the home. This association is not observed in other states such as Brasília11, and Rio Grande do Sul13.
Five were associated with receiving treatment outside the home in the eleven cases concerning the requests for examinations and services (TOH). The TOH associated with judicial health claims is a peculiar condition deriving from the geographical location of the State of Acre in the westernmost part of the Amazon Brazilian population, with 54.19% (397,521 inhabitants) settled in distant areas from urban centers. The main urban centers are Rio Branco, capital of the State of Acre, and Cruzeiro do Sul, where the main health centers are located31.
Most of the population of the State of Acre lives in the forest. However, the largest urban concentrations are in the cities of Rio Branco (336,038 inhabitants), and Cruzeiro do Sul (78,507 inhabitants)31. If not completely isolated, remote locations sometimes present transit difficulties during rainy periods, which hampers public health interventions in the vast majority of the 22 municipalities of the State of Acre.
A strategy to solve the problem can be itinerant health and video medicine, for example, that can mitigate conflicts and adequately meet social needs, especially regarding primary health care, efficiently meet health demands, as a fundamentally guaranteed constitutional right32.
It is also important to note that CCE cases considerably increase health costs for public claimants because they are associated with the services and expenses, such as housing and food. In 2017, the State of Acre spent more than R$ 12 million (the US $ 5 million) on TOH33.
It is noticed that 16.66% (n = 6) of the processes involve vulnerable population: children, older adults, pregnant women, and people with disabilities. They request medicines already included in the National List of Essential Medicines (RENAME), for example, Rispiridone and Imipramine, to treat mental disorders; Teriparatide 250mg, for osteoporosis treatment; and the G. Band Peripheral Blood Cardiotype test.
The concept of vulnerability in health is shaped by a dynamic of reciprocal interdependencies that express multidimensional values - biological, existential, and social34. This research reports the health vulnerability in six analyzed cases that show that the violation of fundamental rights is aggravated when there is an absence or delay in health care, as well as when their vulnerable condition have been neglected, directly violating equity, one of the basic principles of SUS.
It is perceived that the situation of vulnerability in the health of the claimants is transferred to their capacity of exercise of postulation in Court, which is treated like the other petitioners of the other cases analyzed.
The socioeconomic profile of the prosecutors of the health judiciary in the State of Acre is poor since in 77.78% (n = 28) of the actions, the prosecution of these cases is performed by the Public Defender, acting in view of the urgency and necessity of the judicial measure in health. The Court, considering the factual support of the case, deferred gratuitousness for presumption, whereas the law requires objective proof of the insufficiency of financial resources of the author postulation in court35.
The judicialization of health is a means of accessing health services and inputs through the most varied social levels. The demands are related to high-cost drugs, hospitalizations, and procedures from the most complex to the simplest8,36. The characteristics of poverty and extreme need for health care are also observed in other regions of Brazil, such as Rio Grande do Sul, Minas Gerais, and the Federal District11,12,37,38.
The research data also show the dynamic performance of the Public Defender's Office and the judicial manifestations of the Public Ministry in the health demands of Acre State, frequently in favor of the defendants of the demands as observed in the judgments analyzed. Note that the hypo- sufficiency of the claimants is evidenced by a signed self-declaration of poverty35. In contrast, the health need of the impetrates is proved by medical prescription, seen in the cases analyzed as the primary evaluation parameter of the judgment.
When the Judiciary considers medical prescription as the main evaluation parameter for the judgment of health demands brings out the intense controversy about the concept of essential medicine in the face of that available to the World Health Organization (WHO).
It is noticed in the analyzed demands that essential medicine is one that the patient needs, prescribed by a qualified doctor, which conflicts with the definition of essential medicine from the WHO, that defines it as that either satisfies the need priority of health of the population39. The judicial position of the TJ/AC conflicts with the collective conception of health concerning essential medicine. Bucci et Duarte (2017)40 criticize the individual concession of treatments for interfering in public health policy management and systematic financing.
The study results showed that the implementation of public health policy requires programming, systematicity, tactics, and management strategy to achieve healthcare, under the principles of universality, completeness, and equity, with a fundamental social right of the citizen.
Even the judicialization serves as an alternative instrument to health access, the resolution of conflicts involving public policies control, requires mechanisms of institutional dialogue between political and legal actors to reduce lawsuits, which may increase even more given the broad concept of health built after the Declaration of Alma-Ata(1978)41 and the Ottawa(1986) Charter42.
An example of an initiative of communicative institutional dialogue was carried out in the Municipality of Lages, Santa Catarina State, Brazil, with Conciliation Centers43. In specific cases, the judge promotes the reduction of the health claim litigation through the mediation of conflicts, strengthening the dialogue among the various local actors, despite the resistance of the Court of Justice of that State.
In the State of Acre, a similar initiative was performed in 2012, through the Technical Cooperation Agreement No. 017/2012, which drew technical cooperation between the Executive Branch, Judiciary Branch, Public Prosecutor's Office, and Public Defender's Office, intending to guarantee technical subsidies to the demands and procedures that involve the provision of health services44.
The interactivity between all the organs that are part of the relationship in which the judicialization is established is indispensable for constructing actions that serve the common good, considering the possibility and reality of each of the organs involved in this chain45. The initiative of institutional dialogue in the State of Acre had no practical solutions. It should be re-evaluated and resumed to rationalize relations between the Executive Branch, Judiciary, and users of the health system.
The foundation of institutional arrangements lies in communicative theories and cooperative constitutionalism, which are based on balance and reasonableness in the relationship between power and citizenship as an effective alternative for resolving issues involving the judicialization of public policies26,43. Thus, the conventional judicial model of conflict resolution in public health is dysfunctional to meet social health demands, and tends to aggravate violations of SUS principles and permanent increase in the number of requests in the Judiciary, harming the management of public health and intelligent allocation of scarce resources.
In referring to the thesis on the right to health as a fundamental social right of the citizen, the findings of the research report that the JB / AC bases its decisions on the principle of human dignity, physical integrity and life, affirming that the right to health must be guaranteed, regardless of budget constraints and bureaucratic requirements. But it reinforces the idea of the need for a new resolution mechanism in public health policy, since 25% of the health demands analyzed were not judicially resisted by the State of Acre in meeting the health interest of the user.
Access to healthcare is a fundamental citizen social right materialized by SUS, which serves more than 220 million people, and is characterized by three pillars of support: universality, integrality and equit46.
Universality is bound to guarantee the right to health to all Brazilians, without meaning or discrimination, to access the health services offered by the SUS; while the integrity of care is understood as an articulated and continuous set of preventive and curative actions and services, individual and collective, necessary for each case at all levels of system complexity46.
The main causes of health judicialization in Acre are the divergences between medical prescriptions and the provisions established in the SUS PCDT, with prevailing injunctions as the main strategy of the applicants for access to health.
On the other hand, its main negative effects are the prevalence of individual rights over collective rights to health, with the credible commitment of the normative system of the SUS, and damages to the public order, public economy and systematicity of public health policy, especially consequences of double or triple violation of the fundamental rights of vulnerable groups, who must have differential and priority treatment.
In addition, the effects of the judicialization promote a direct violation of equity in SUS, which is characterized by valuation, fair judgment and virtue (attitude, behavior, fact, etc.) of who or what manifests a sense of justice, impartiality, respect for equal rights. Nevertheless, the judicialization directs the protection of the actions and services of the citizens that must be offered, regardless of the complexity of the service provision, the region in which the individual resides or his / her nationality46.
The work of the Judiciary ensures compliance with SUS principles when the executive branch plans and effectively execute the public health policy. Still, the judicialization of health cannot be a mere administration of judicial interests in cases without conflicts, as was observed in cases not contested in the State of Acre.
The findings show that in the imposition of judicial decisions, there is no judicial evaluation regarding the predictability of the resources needed by the executive for health, and the damage to SUS's management and financing system is a serious consequence in the State of Acre.
According to Borges, mechanisms and/or dialogical approaches of the Judiciary and Executive Branch provide an environment of collaboration and partnerships between different state actors, such as state courts, state attorneys, public defenders, prosecutors, technical assistance centers, and conciliation chambers to reducing or responding better to individual health care disputes47.
There is a lack of administrative and technical-scientific decisions that ensure the fundamental right to health by the Judiciary, and, above all, an instrument of institutional dialogue among the actors involved in litigation is necessary, to enabling a fairness service48.
The institutional dialogue gap for resolving health disputes can be solved by improving the administrative process of incorporating technologies in the National Commission for the Merger of Technology (CONITEC)49.
The institutional dialogue to mitigate the consequences of judicialization on public health policy can be achieved by improving the process of incorporating technologies into SUS, already existing and with legitimacy, competence and technical conditions to decide whether or not to incorporate technology (medication or procedure) to meet social needs in health, based on scientific evidence, efficiency and impersonality.
It is worth noting that preliminary health measures do not allow for an in-depth analysis of patients' health issues, striving for speed and not considering the State's bureaucratic and financial limitations, but promoting interference in the management and programming of public health policy.
However, understanding the factors and consequences of the judicialization of health in a regionalized way is essential for understanding the parts of a whole of Brazilian public health policy, for the collection of data and information that enable a more efficient and effective policy to propose services in terms of meeting health needs and filling health gaps.
CONCLUSION
Thus, collective decisions on the judicialization of health in the State of Acre ensure the right to health for citizens, in most cases (94.44%), through preliminary injunctions based on the principle of human dignity, physical integrity and life, as well as in medical prescriptions in each specific case, regardless of assessments regarding financial, budgetary and bureaucratic constraints of the State.
About a third of cases (25%) go uncontested because the parties have common interests - health is a fundamental, universal and integral right for all. In these cases, health demands are no more than the mere administration of the public interest, where the citizen seeks health and the State grants health, considering the patient's clinical condition, contrary to good health management practices, which are generally silent and non-existent.
On these premises, also, considering the absence of litigation, the reduction of the judicialization of health can be achieved by cooperative procedures between powers and clinical management of diseases with the cooperation and development of due legal process that improves the standardization of patient health and clinical condition.
Author Contributions
All authors participated in all stages of the work, study design and manuscript design. All authors agreed with the final version of the manuscript.
Acknowledgments
My family, friends and professor, as well as the Laboratory of Study Design and Scientific Writing at Centro Universitário FMABC and, especially, I thank Professor Pascoal Muniz, who taught me the constancy and intrepidity that the spirit of research requires. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. The financial viability of the article is due to the Acre - Health Project in the Western Amazon (multi-institutional agreement process no. 007/2015 SESACRE-UFAC-FMABC).
Conflicts of Interest
The authors declare that there are no competing interests.
REFERENCES
1.Alves B/ O/ O-M. DeCS - Descritores em Ciências da Saúde [Internet]. [citado 27 de setembro de 2021]. Disponível em: https://decs.bvsalud.org/ [ Links ]
2.Pandolfo M, Delduque MC, Amaral RG. Aspectos jurídicos e sanitários condicionantes para o uso da via judicial no acesso aos medicamentos no Brasil. Rev salud pública. abril de 2012; 14 (2): 340-9. [ Links ]
3.Lamprea E. The judicialization of health care: a global south perspective. Annu Rev Law Soc Sci. 13 de outubro de 2017; 13 (1): 431-49. [ Links ]
4.Mullachery P, Silver D, Macinko J. Changes in health care inequity in Brazil between 2008 and 2013. Int J Equity Health. dezembro de 2016; 15 (1): 140. [ Links ]
5.Asensi F. Responsabilidade solidária dos entes da federação e "efeitos colaterais" no direito à saúde. Rev Direito Sanit. 30 de dezembro de 2015; 16 (3): 145. [ Links ]
6.ADWS-. Números atualizados da judicialização da saúde no brasil - por clenio jair schulze [Internet]. Empório do Direito. 2017 [citado 27 de setembro de 2021]. Disponível em: http://emporiododireito.com.br/leitura/numeros-atualizados-da-judicializacao-da-saude-no-brasil-por-clenio-jair-schulze [ Links ]
7.E-saj [Internet]. [citado 27 de setembro de 2021]. Disponível em: https://esaj.tjac.jus.br/esaj/portal.do?servico=740000 [ Links ]
8.Gomes DF, Souza CR, Silva FL da, Pôrto JA, Morais I de A, Ramos MC, et al. Judicialization of health and public hearing convened by the Supreme Court in 2009: what has changed since then? Saúde em Debate [Internet]. 2014 [citado 27 de setembro de 2021]; 38 (100). Disponível em: http://www.gnresearch.org/doi/10.5935/0103-104.20140008. [ Links ]
9.Ventura M, Simas L, Pepe VLE, Schramm FR. Judicialização da saúde, acesso à justiça e a efetividade do direito à saúde. Physis. 2010; 20 (1): 77-100. [ Links ]
10.Asensi F, Pinheiro R. Judicialização da saúde e diálogo institucional: a experiência de lages(Sc). Rev Direito Sanit. 25 de outubro de 2016; 17 (2): 48. [ Links ]
11.Diniz D, Machado TR de C, Penalva J. A judicializacao da saude no Distrito Federal, Brasil. Ciênc saúde coletiva. fevereiro de 2014; 19: 591-8. [ Links ]
12.Travassos DV, Ferreira RC, Vargas AMD, Moura RNV de, Conceição EM de A, Marques D de F, et al. Judicialização da Saúde: um estudo de caso de três tribunais brasileiros. Ciênc saúde coletiva. novembro de 2013; 18 (11): 3419-29. [ Links ]
13.Biehl J, Socal MP, Amon JJ. The judicialization of health and the quest for state accountability: evidence from 1,262 lawsuits for access to medicines in southern brazil. Health Hum Rights. junho de 2016; 18 (1): 209-20. [ Links ]
14.Araújo AF da S. Judicialização da saúde em Minas Gerais: novas estratégias de enfrentamento: a criação do Núcleo de Atendimento à Judicialização da Saúde. Cad Ibero Am Direito Sanit. 20 de setembro de 2014; 3 (2): 73-9. [ Links ]
15.Campos Neto OH, Acurcio F de A, Machado MA de Á, Ferré F, Barbosa FLV, Cherchiglia ML, et al. Médicos, advogados e indústria farmacêutica na judicialização da saúde em Minas Gerais, Brasil. Rev Saúde Pública. outubro de 2012; 46: 784-90. [ Links ]
16.Menezes FFJ de, Silva AG da. Poder judiciário e diálogos institucionais: uma perspectiva frente à flexibilização das decisões. 1 [Internet]. 25 de julho de 2014 [citado 27 de setembro de 2021]; Disponível em: http://www.seer.ufu.br/index.php/horizontecientifico/article/view/17921 [ Links ]
17.Falavinha DHS, Marchetto PB, Veiga Junior H. Judicialization of Health: The Brazilian case and a bioethical review. Rev Quaestio Iuris [Internet]. 25 de maio de 2016 [citado 27 de setembro de 2021]; 9 (2). Disponível em: http://www.e-publicacoes.uerj.br/index.php/quaestioiuris/article/view/20085 [ Links ]
18.Zangirolami-Raimundo J, Echeimberg J de O, Leone C. Research methodology topics: Cross-sectional studies. J Hum Growth Dev. 28 de novembro de 2018; 28 (3): 356-60 [ Links ]
19.Direito processual civil esquematizado - 9a edição [Internet]. [citado 27 de setembro de 2021]. Disponível em: https://www.sbs.com.br/direito-processual-civil-esquematizado-9-edicao.html [ Links ]
20.Brasil. Estado do Acre. Lei Complementar Estadual nº 121, de 30 de dezembro de 2010. Disponível em: http://www.migalhas.com.br/arquivos/2016/8/art20160809-05.pdf Acesso em: 28/03/2018. [ Links ]
21.Lenza P. Direito Constitucional Esquematizado - 25a Edição 2021. 25a edição. Saraiva Jur; 2021. [ Links ]
22.Mais de 7,6 mil pessoas foram atendidas pelo TFD no Acre e investimento foi R$ 14,8 milhões no ano passado [Internet]. G1. [citado 27 de setembro de 2021]. Disponível em: https://g1.globo.com/ac/acre/noticia/2018/08/24/mais-de-76-mil-pessoas-foram-atendidas-pelo-tfd-no-acre-e-investimento-foi-r-148-milhoes-no-ano-passado.ghtml. [ Links ]
23.Silva C de A. Diálogos institucionais e ativismo. Curitiba: Juruá Ed.; 2010. [ Links ]
24.Teodoro CR dos S, Caetano R. O caso da fosfoetanolamina sintética e a preocupante flexibilização das normas sanitárias no Brasil. Physis. setembro de 2016; 26: 741-6. [ Links ]
25.Ventura CA, Junior RC, Gutier MS, Mendes IA. Alternatives for the enforcement of the right to health in Brazil. Nurs Ethics. maio de 2016; 23 (3): 318-27. [ Links ]
26.Diniz D, Medeiros M, Schwartz IVD. Consequências da judicialização das políticas de saúde: custos de medicamentos para as mucopolissacaridoses. Cad Saúde Pública. março de 2012; 28 (3): 479-89. [ Links ]
27.Núcleos de assessoria técnica e judicialização da saúde: constitucionais ou inconstitucionais? - technical advice centers and "judicialization of health": constitutional or unconstitutional? | justiça federal - seção judiciária do rio de janeiro [Internet]. [citado 27 de setembro de 2021]. Disponível em: https://www.jfrj.jus.br/revista-sjrj/artigo/nucleos-de-assessoria-tecnica-e-judicializacao-da-saude-constitucionais-ou [ Links ]
28.Natjus - núcleo de apoio técnico [Internet]. [citado 27 de setembro de 2021]. Disponível em: http://wwa.tjto.jus.br/saude/index.php/nat-nucleo-de-apoio-tecnico#:~:text=Em%20aten%C3%A7%C3%A3o%20a%20Recomenda%C3%A7%C3%A3o%20N%C2%BA%2031%2C%20de%2030,relativas%20ao%20SUS%20-%20Sistema%20%C3%9Anico%20de%20Sa%C3%BAde. [ Links ]
29.ConJur - Judicialização da saúde beneficia mercado, diz pesquisador [Internet]. [citado 27 de setembro de 2021]. Disponível em: https://www.conjur.com.br/2018-mar-12/judicializacao-saude-beneficia-mercado-pesquisador?imprimir=1. [ Links ]
30.Caetano R, Silva RM da, Pedro ÉM, Oliveira IAG de, Biz AN, Santana P. Incorporação de novos medicamentos pela Comissão Nacional de Incorporação de Tecnologias do SUS, 2012 a junho de 2016. Ciênc saúde coletiva. agosto de 2017; 22 (8): 2513-25. [ Links ]
31.Lucas D. Acre em números - governo do estado do acre [Internet]. [citado 27 de setembro de 2021]. Disponível em: http://acre.gov.br/acre-em-numeros/ [ Links ]
32.Telemedicina como instrumento de suporte na atenção primária à saúde - latin american journal of telehealth [Internet]. [citado 27 de setembro de 2021]. Disponível em: http://cetes.medicina.ufmg.br/revista/index.php/rlat/article/view/187 [ Links ]
33.Redação D. Governo do Acre investiu mais de R$ 12 milhões em TFD ao longo de 2017 [Internet]. Notícias do Acre. 2018 [citado 27 de setembro de 2021]. Disponível em: https://agencia.ac.gov.br/governo-do-acre-investiu-mais-de-r-12-milhoes-em-tfd-ao-longo-de-2017/ [ Links ]
34.Oviedo RAM, Czeresnia D. O conceito de vulnerabilidade e seu caráter biossocial. Interface (Botucatu). 27 de março de 2015; 19 (53): 237-50. [ Links ]
35.Brasil. Lei nº 1.060, de 5 de fevereiro de 1950. Estabelece normas para a concessão de assistência judiciária aos necessitados. Disponível em:<http://www.planalto.gov.br/cciVil_03/Leis/L1060compilada.htm>. Acessado em: 06/10/2018. [ Links ]
36.Trevisan LM, Nalin T, Tonon T, Veiga LM, Vargas P, Krug BC, et al. Access to treatment for phenylketonuria by judicial means in Rio Grande do Sul, Brazil. Ciênc saúde coletiva. maio de 2015; 20 (5): 1607-16. [ Links ]
37.Biehl J, Petryna A. Tratamentos jurídicos: os mercados terapêuticos e a judicialização do direito à saúde. Hist cienc saude-Manguinhos. março de 2016; 23 (1): 173-92. [ Links ]
38.Medeiros M, Diniz D, Schwartz IVD. A tese da judicialização da saúde pelas elites: os medicamentos para mucopolissacaridose. Ciênc saúde coletiva. abril de 2013; 18 (4): 1089-98. [ Links ]
39.WHO Expert Committee on the Selection and Use of Essential Medicines (12th : 2002 : Geneva S, Organization WH. The selection and use of essential medicines : report of the WHO Expert Committee, 2002 : (Including the 12th model list of essential medicines) [Internet]. World Health Organization; 2003 [citado 27 de setembro de 2021]. Disponível em: https://apps.who.int/iris/handle/10665/42620 [ Links ]
40.Bucci MPD, Duarte CS. Judicialização da saúde - 1a edição de 2017: A visão do poder executivo. 1a edição. Saraiva Jur; 2017. [ Links ]
41.World Health Organization. Declaração de Alma-Ata. Conferência Internacional sobre Cuidados Primários de Saúde. 1978. [cited 2018 Mai 08]. Available: http://cmdss2011.org/site/wp-content/uploads/2011/07/Declara%C3%A7%C3%A3o-Alma-Ata.pdf [ Links ]
42.Brasil. Primeira Conferência Internacional sobre promoção da saúde, novembro de 1986. Declaração de Alma-Ata. 2001: 19. Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/carta_ottawa.pdf. Acesso em: 19/03/2018. [ Links ]
43.Asensi F, Pinheiro R. Judicialização da saúde e diálogo institucional: a experiência de lages(Sc). Rev Direito Sanit. 25 de outubro de 2016; 17 (2): 48. [ Links ]
44.Termo de Cooperação Técnica n. 017/2012 [Internet]. Portal CNJ. [citado 27 de setembro de 2021]. Disponível em: https://www.cnj.jus.br/transparencia-cnj/acordos-de-cooperacao-tecnica/termo-de-cooperacao-tecnica-n-0172012/ [ Links ]
45.Saúde (Brasil) CN de S de. Coletânea Direito à Saúde: dilemas do fenômeno da judicialização da saúde. Coletânea Direito à Saúde: dilemas do fenômeno da judicialização da saúde. 2018; 319-319. [ Links ]
46.Abreu LCD, Pereira VX, Silva RPM, Macedo Jr H, Bezerra IMP. The right to scientific information: one of the main elements of the unified health system. J Hum Growth Dev. 18 de dezembro de 2017; 27 (3): 258. [ Links ]
47.Individual health care litigation in brazil through a different lens: strengthening health technology assessment and new models of health care governance [Internet]. Health and Human Rights Journal. 2018 [citado 27 de setembro de 2021]. Disponível em: https://www.hhrjournal.org/2018/06/individual-health-care-litigation-in-brazil-through-a-different-lens-strengthening-health-technology-assessment-and-new-models-of-health-care-governance/ [ Links ]
48.Critérios definidos pelo STJ trazem pouco avanço na judicialização da saúde [Internet]. Consultor Jurídico. [citado 27 de setembro de 2021]. Disponível em: https://www.conjur.com.br/2018-mai-03/daniel-dourado-tese-stj-avanca-judicializacao-saude. [ Links ]
49.Affonso FM. Uma análise legal do processo de incorporação de tecnologia no sus: um passo para o fortalecimento da justiça administrativa. 1 [Internet]. 2017 [citado 27 de setembro de 2021]; Disponível em: revistacej.cjf.jus.br/cej/index.php/revcej/article/view/2216 [ Links ]
 Correspondence:
Correspondence:
José Luiz Gondim dos Santos
gondim.adv@gmail.com
Manuscript received: july 2020
Manuscript accepted: may 2021
Version of record online: january 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}