










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.1 Santo André ene./abr. 2022
http://dx.doi.org/10.36311/jhgd.v32.11323
ORIGINAL ARTICLE
Prevalence of chronic noncommunicable diseases and their associated factors in adults over 39 years in riverside population in the western brazilian amazon region
Antonieta Pereira RelvasI; Juliana de Souza Almeida Aranha CamargoII, III; Sergio de Almeida BasanoIV; Luís Marcelo Aranha CamargoI, III, V, VI, VII
IFederal University of São João Del Rei, Campus Centro-Oeste Dona Lindu, Sebastião Gonçalves Coelho Street, 400, CEP 35501-296, Divinópolis, Minas Gerais, Brazil;
IIOswaldo Cruz Foundation Leônidas and Maria Deane Institute, Rua Teresina 476, CEP 69.057-070 Manaus, Amazonas, Brazil (Post-Graduation Student);
IIIDepartment of Medicine, Afya/São Lucas University, Alexandre Guimarães Street 1929, CEP 76.888-000, Porto Velho, Rondonia, Brazil
IVCentro de Medicina Tropical de Rondônia, Av. Guaporé, 215, CEP 78918-791 Porto Velho, Rondônia, Brazil;
VCoordinator of the Biomedical Science Institute 5, University of São Paulo, CEP 76.888-000, Monte Negro, Rondonia, Brazil
VINational Institute of Science & Technology/CNPq-EpiAmo, Rua da Beira 1930, CEP 76.803-596,Porto Velho, Rondonia, Brazil
VIIDepartment of Medicine,Tropical Medicine Center, Rua da Beira 1930, CEP 76.803-596, Porto Velho, Rondonia, Brazil
ABSTRACT
BACKGROUNG: The prevalence of Chronic Noncommunicable Disease (CND) are rocketting over the world, including in young adults. The WHO estimates that more than half of the deaths in the world are caused by CND
A cross-sectional study was carried out from june to november 2016. The researchers visited 16 communities, with a sample size of 183 adult individuals performed for convenience. The patients went through screening and verified: weight, height, abdominal circumference, blood pressure, clinical-epidemiological history and performed physical and laboratory examination. Prevalence ratios were calculated with confidence intervals of 95% and with statistical significance with p<0.05.
This study aims to estimate the prevalence of CND and its associated factors in the adult riverside population of the Rio Madeira in Humaitá, Amazonas State, Western Brazilian Amazon.
The prevalence of systemic arterial hypertension (SAH) was 44.7%, 52.6% in female. Of the individuals with SAH, 77.5% did not use medication. About 51.5% of them had Grade I SAH. The prevalence of type 2 diabetes mellitus was 16.4%, where no patient used medication and about 40.4% of the studied population fits in the glucose intolerance range. Metabolic syndrome presented a prevalence of 24.0%, with a higher frequency in females (33.8%) (p=0.007). Concerning chronic kidney disease, a prevalence of 12.1% was observed in both sexes. The associated factors found were alcoholism, smoking, sedentary lifestyle and obesity, and more than 45% of the patients had at least two associated factors.
The population had a high prevalence of CND and associated factors, low frequency of medication use, revealing inefficiency of the local health system. Increased coverage of the Governmental Family Health Strategy (GFHS) and the increase in number of trained Community Health Assistants , together with health education actions can increase the population's health standard.
Keywords: chronic noncommunicable disease, riverside population, Brazilian Western Amazon.
RESUMO
INTRODUÇÃO: A prevalência de Doença Crônica Não Transmissível (DCNT) está elevada em todo o mundo, incluindo em adultos jovens. A OMS estima que mais da metade das mortes no mundo são causadas por DCNT
Um estudo transversal foi realizado de junho a novembro de 2016. Os pesquisadores visitaram 16 comunidades, com um tamanho de amostra de 183 indivíduos adultos, realizada por conveniência. Os pacientes passaram por triagem e verificados: peso, altura, circunferência abdominal, pressão arterial, história clínico-epidemiológica, sendo realizado exame físico e laboratorial. Razões de prevalência foram calculadas com intervalos de confiança de 95% e com significância estatística com p<0,05. Este estudo tem como objetivo estimar a prevalência de DCNT e seus fatores associados na população ribeirinha do Rio Madeira em Humaitá, Estado do Amazonas, Amazônia Ocidental, em adultos com mais de 39 anos. A prevalência de hipertensão arterial sistêmica (HAS) foi de 44,7%, 52,6% no sexo feminino. Dos indivíduos com HAS, 77,5% não faziam uso de medicamentos. Cerca de 51,5% deles tinham HAS grau I. A prevalência de diabetes mellitus tipo 2 foi de 16,4%, nenhum paciente fazia uso de medicamentos e cerca de 40,4% da população estudada se enquadra na faixa de intolerância à glicose. A síndrome metabólica apresentou prevalência de 24,0%, com maior frequência no sexo feminino (33,8%) (p = 0,007). Em relação à doença renal crônica, foi observada prevalência de 12,1% em ambos os sexos. Os fatores de risco associados encontrados foram etilismo, tabagismo, sedentarismo e obesidade, sendo que mais de 45% dos pacientes apresentavam pelo menos dois fatores associados. A população apresentou alta prevalência de DCNT e fatores associados, baixa frequência de uso de medicamentos, revelando ineficiência do sistema de saúde local. O aumento da cobertura da Estratégia Saúde da Família (ESF) e o aumento do número de Agentes Comunitários de Saúde capacitados, aliados a ações de educação em saúde, podem elevar o padrão de saúde da população.
Palavras-chave: Doença Crônica Não Transmissível. População Ribeirinha. Amazônia Ocidental Brasileira.
Authors summary
Why was this study done?
Two previous studies, carried out between 2014 and 2015 by the same researchers in the municipality of Monte Negro, urban area of the Brazilian Amazon, colonized by people that migrated in the 1970-1980 from the south and southest of Brazil, pointed for extremely high prevalence's of Chronic Noncommunicable Disease (CND) in the adult. As so, the authors wants to know if the riverine population (most of them with Indian miscegenation that live in the banks of Madeira River for more than 2 centuries), with a different way of life, away from the metropolitan centers, has the same profile of CND.
What did the researchers do and find?
The authors examined and interviewed 183 adults from 16 riverine communities and screened for CND and their associated factors. The authors found a high prevalence of CND and a high prevalence of associated factors among the examined population and the evidence of a weak public health system. Even so, the prevalences of CND are similar or quite lower than in other studies.
What do these findings mean?
Even with a diffente way of life, away from the metropolitan centers and their facilities, the riverine adult has quite the same profile as the adult in the urban areas of the Amazon region and other regions of Brazil. Such results point for the weakness of the local public health system, unable to prevent such disease, promote health and deal with such revelant problem.
INTRODUCTION
The decrease in frequency and the disappearance of certain diseases over the years has led to a process of changing the epidemiological profile of the population. This process is due a dynamic phenomenon and multidimensional process, dependent on socioeconomic, demographic, biological, cultural and technological aspects, described as "Epidemiological Transition"1. This phenomenon is characterized by the progressive evolution of a high mortality profile by infectious and parasitic diseases to another where chronic noncommunicable diseases (CND) predominate. However, these aspects did not impact the whole world equally, although the decrease in mortality was common in mainly all countries2.
In a comprehensive assessment of the state of world health, it was found that communicable, maternal, neonatal and nutritional diseases decreased both in absolute terms and in relation to noncommunicable diseases in the period, except for malaria and HIV3. The burden of CND has increased, with the highest increase associated with Type 2 Diabetes (T2DM) and cardiovascular diseases. The main risk factors for CND also changed substantially between 1990 and 2010, with the main current factors being obesity, disglycemia, high-sodium diet, sedentary lifestyle, low-fiber diets, and permissive marketing of tobacco and alcohol3.
As the aging process advances in Brazil, and the number of premature deaths falls, there is an exponential growth of people affected by CND and consequently, there is an increase in public expenditures4. In crude values, mortality from CND in Brazil increased by 5% between 1996 and 2007, and the prevalence of T2DM and SAH has already reached important numbers and a constant increase5.
There is little information on the health of riverine populations in the Amazon, which represents a mixture of different social groups (Indians and migrants mainly from the northeast)6,7.
Studies on the health situation of the riverine population, mainly related to CND and their associated factors, will allow the mapping of the epidemiological profile and allow the development of intervention strategies to reduce the associated factors. Considering that population aging leads to an increase in CND, the objective of this study was to verify the prevalence of CNDs with their associated factors in remote riverside communities along the Madeira River, in the municipality of Humaitá, Amazonas State, Western Amazon.
METHODS
Study Design
This is an cross-sectional study to measure the prevalence of CND and associated factors, using data collected from the population that lives in riverside areas in the banks of Rio Madeira and data from the Municipality Secretary of Health.
Study Location and Period
The surveyed riverside communities correspond to a total of 16 localities with an estimates population of 531 inhabitants. The studied area extended between latitude 6°59'04.95" South, longitude: 62°49'37.26" West and latitude 6°45'23.14" South, longitude: 62°28'48.58" West on the banks of the Rio Madeira in the municipality of Humaitá, Amazonas State, Western Amazon. The study was carried out from june to november 2016.(Figure 1)

Study Population and Eligibility Criteria
The sample size was estimated to ensure representativeness for the event under study. As the adult population is scarce in these areas, the authors considered as adult the ones older than 39 years. The sample calculation used information from the SIAB (Primary Care Information System) referring to the adult population (age greater than 39 years) living in the studied area in 2016, making a total of 241 adults older than 39 years . To calculate the sample size, the authors used the statistical software OpenEpi, Version 3, with a 95% confidence interval and a 5% margin of error, with a prevalence of unknown CND (therefore, the authors adopted a supposed prevalence of 50%) and an increase of 20% of the sample for possible losses and/or refusals. Thus, the final sample size was 183 adults, or 76% of the population (>39 years). The sampling was performed for convenience, since there is no nominal list of residents, making randomization impossible. Individuals over 39 years of age who had agreed to participate in the study, who had the consent document signed and have fasted for at least 8 hours entered the study.
Data Collection
The participants of the study underwent a screening, in which weight, height, abdominal circumference, and blood pressure were verified. Soon after, they answered the questionnaire regarding characteristics: sex, age, ethnicity and applied a clinical epidemiological questionnaire to verify the history of diseases and associated factors for CND. The researchers evaluated the prevalence of SAH, dyslipidemia and T2DM and their associated factors: sedentary lifestyle, smoking, excessive alcohol consumption, obesity and Chronic Kidney Dysfunction (CKD).
Afterwards, all participants collected blood tests in the Floating Health Unit.
Aneroid sphygmomanometer was used, duly calibrated, based on Brazilian Guidelines for Arterial Hypertension (2016) for the diagnosis and classification of hypertension, where the patients, after 5 minutes of rest, were seated in a chair, had not had coffee, supported their 2 feet on the floor, the back on the back of the chair, had an empty bladder and supported the arm on a table, at heart level. The blood pressure of each limb was measured 3 times, where the first was discarded, and the mean systolic (SBP) and diastolic (DBP) pressures of each limb were measured. The highest blood pressure level of SBP and DBP of each limb was chosen to make up real blood pressure8.
The diagnosis of T2DM and Metabolic Syndrome (MS) was made following the Guidelines of the Brazilian Society of Diabetes (2015)9.
For the evaluation of dyslipidemias, laboratory analyses of lipid parameters were performed in the samples of fasting patients and the lipid profile reference values were adopted for adults, according to the Brazilian Guidelines on Dyslipidemia and Prevention of Atherosclerosis of the Brazilian Society of Cardiology10:
The NCEP-ATP III11 criteria were used to confirm the diagnosis of metabolic syndrome. For the evaluation of CKD, creatinine dosages and the CKD-EPI equation were used for adults and classified according to KDOQI11. CKD was considered when the glomerular filtration rate was less than 60 mL/min/1.73m2
Anthropometric measurements of weight, height and abdominal circumference were obtained to determine the body mass index (BMI) to classify obesity and metabolic syndrome. To evaluate the sedentary lifestyle, an international physical activity questionnaire - IPAQ3, in the short version, was used. The Alcohol Use Identification Test - AUDIT, developed by the Medical School of Ribeirão Preto of the University of São Paulo, was used to evaluate alcoholism. We also used the questionnaire for screening the use of alcohol, tobacco and other substances - ASSIST, developed by WHO (World Health Organization).
Data from the Muncipality Secretary of Health was used in order to estimate the Governmental Family Health Strategy (GFHS) coverage, the number a Health Community Assistants (HCA) and to calculate de sample size.
Data Analysis
The data obtained were compiled in Excel® tables. The calculations of the prevalence of CND and their associated factors were performed with 95% confidence intervals. The Fisher chi-square test was used to calculate the prevalence ratios, comparing possible divergences between the observed frequencies, with a statistical significance of 5%. The researchers used the statistical platform OpenEpi (www.openepi.org).
Ethical and Legal Aspects of the Research
For each individual examined an informed consent form was signed. The study was submited and aproved by the Brazilian Nacional Ethical Committé under number CAAE 51511415.4.0000.0013, report 1.359.182.
RESULTS
One hundred and eighty three adults (79% of the population), aged between 39-84 years, was examinated. There was equilibrium in the frequency between sexes (56.3% male) and higher frequency of the population between 39-49 years (49.2%), with the majority of mulatto inhabitants (79.2%). The average age was 52.5 +- 10.6 years. The family income, much of it, is maintained by the Bolsa da Família Program (governmental budget for people with low income) and varies between 1 and 2 minimum wages/month. The economic activities developed are small trade, fishing, hunting, manioc flour production, subsistence agriculture and mineral extraction of gold (river mining). Few residents have access to electricity generators and difficulty in reaching the urban area. The coverage of the GFHS, is low (~30,6%) as is the number of HCA (3 assitants), a fact that leads, in most cases, for the community to seek the solution of their health problems in the community itself.
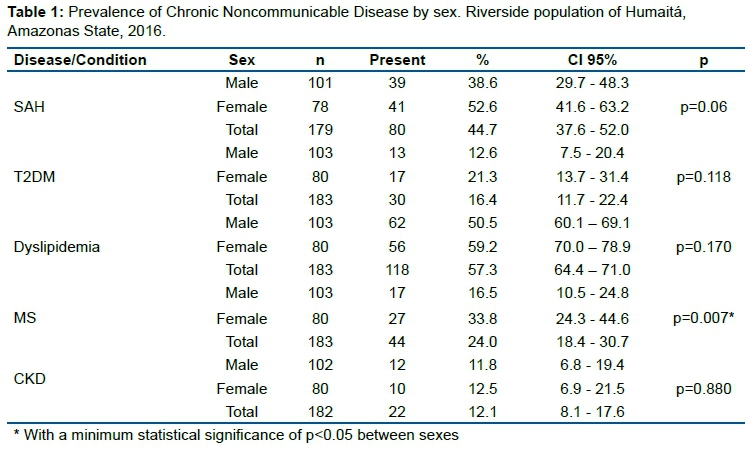
Table 1 shows results regarding the frequency of CND, where it is observed a high prevalence of SAH (SBP > 140 mm Hg and/or DBP > 90 mm Hg). Of the individuals with SAH, 77.5% did not use medication. Approximately 51.5% of the hypertensive individuals were classified with SAH Grade I (PAS 140-159mm Hg and/or PAD 90-99mm Hg). Of the patients with T2DM (fasting blood glucose >125 mg/dL) (16.4%), none used medication to control blood glucose. Also, about 40.4% of the studied population fits in the glucose intolerance range (100-125 mg/dL), being considered pre-diabetic.
Results related to dyslipidemias indicate the prevalence of total cholesterol considered high (>240 mg/dL) frequent in both sexes (57.3%) and 16.9% of the sample are borderline 200-239 mg/dL). In relation to the high triglyceride rate (200-499 mg/dL), we can verify an equal frequency between sexes (46.6%), while emphasizing that 20.2% of the patients sampled are with triglyceride rates considered borderline (150-200mg/dL). HDL cholesterol presented low concentrations in 24.0% of the study participants (<40 mg/dL for men and <50 mg/dL for women), with higher frequency in male participants (32%, p=0.004). High LDL cholesterol levels (160-189 mg/dL) presented a relatively high prevalence (38.7%), with a similar frequency between both sexes (37.5% in females and 39.8% in males).
Obesity prevalence in the population was 20.4%, more prevalent in women (23.7%) (p=0.017). For the diagnosis of MS, a prevalence of 24.0% was verified, with higher frequency in female participants (27.0%) (p=0.007).
For CKD, there was a prevalence of 12.1% with similar frequency in both sexes.
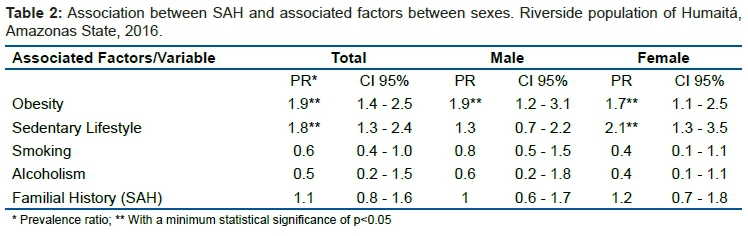
According to the data in Table 2, we can consider that obesity is a associated factor for SAH in both sexes and a sedentary lifestyle only for females.
Despite Table 3, according to the data, we can consider that a sedentary lifestyle is a associated factor for T2DM in both sexes.
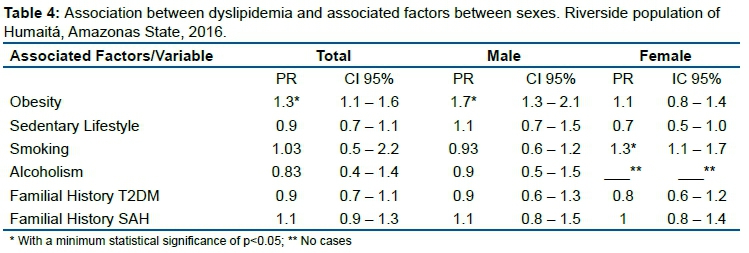
According to the data in Table 4, we can consider that obesity is an associated factor for male dyslipidemia and smoking only for females.
DISCUSSION
Chronic Non-Transmissible Disease (General)
In this study, we observed an average prevalence of general CND of 44.7% among surveyed adults aged 40 to 84 years. The results of this study are similar to a study carried out in Maringá, south of Brazil, in 2012, that showed the presence of CND in 44.8% of those evaluated, aged between 18 and 87 years, being more prevalent in women (77%). The Maringá study (urban area in the south of Brazil) also revealed that the CND were more prevalent in the adult, people with low schooling, that used of tobacco and were obese12. The south of Brazil is more developed, the coverage of the GFSH is greater, and the access to the public health system is easier and the inclusion of young people in the study could explain the quite low prevalence of CND.
Another study, carried ou in Coari (Amazonas State) in 20157 , estimated a prevalence of general CND of 9,5% in the population aged 18 years and greater. As they icluded young peolple in the sample this could reduce the prevalence. On the other hand, the disease were self-reported by the individual, fact that makes the data inaccurate. The Monte Negro Study (urban municipality of Rondonia State, Amazon Region), points for a prevalence of CND around 70,6%16, in people with age greater than 59 years. Another study, run by the Brazilian government, acessed 62.986 households over the contry, and interviewed people older than 17 years (self-reportd information) and detected a prevalence of CND of 45%19.
The riverine life style, with a more difficult access to fast food television and game devices (screen time) and an increase in physical activities linked to agriculture, fishing and mining may contribute to this lower CND prevalence, although the GFSH coverage is low, the number of CHA is inadequated and the access to public health system much more difficult.
SAH
SAH had a prevalence of 44.7% in the studied population. Of the individuals with SAH, about 62 (77.5%) did not use medication to control blood pressure. This is probably due to the previous ignorance of the pathology and/or the difficulty of access to medicine since this population lives in communities far from the urban area and has a precarious coverage of the GFHS and CHA.
In riverside communities located on the banks of the Madeira River, in Porto Velho (Rondonia´s State capitol, Amazon region), a study was conducted with 841 adults (> 19 years) between 2009 a 2011, showing a prevalence of SAH of 25.7%, with a higher prevalence in males (28.7%). The prevalence of SAH showed an increasing trend throughout the age groups, with a higher value among individuals over 60 years of age (58.6%)13.
A study conducted in Nobre, a small municipality, center-west of Brazil, found a prevalence of 30.1% in adults14. In Belém municipality, north of Brazil, a similar study on the prevalence of hypertension and factors associated pointed for a prevalence of 17%15.
In this study SAH was more prevalent in female (23.7%, p= 0.017). Although women traditionally search more frequently for healthcare, the low coverage of the GSHS makes it more difficult. As riverine women takes care of the children, cooks and takes care of the house, they are more obese (23,7%, p=0.017) and have a higher prevalence of MS (27%, p=0.007) than males, probably contributing for the higher prevalence of SAH13. Sedentary lifestyle women also has 1.7 more probability of having SAH, as seen in Table 2. This study reinforces the association of obesity and sedentarism as factors associated with SAH. These results have discrepancies compared to the Monte Negro Study, in individuals aged over 59 years (perhaps an age bias in comparison with this study), that showed a prevalence of SAH of 70.6% of people and that only 60% used medication16.
We can verify that even in urban areas the lack of access to medicine and the low GFHS/CHA coverage occurs similarly compared to riverside areas. The lower age of the population in this study may influence the results, decreasing the SAH prevalence. The riverine life style, as discussed above, may also collaborate to lower SAH prevalence.
T2DM
We can observe that the prevalence of T2DM in the studied population was 16.4%, a value considered according to the national average. According to data from the National Household Sample Survey (NHSS-2013), the prevalence of T2DM in the population over 18 years of age in Brazil is 6.2%17. In the NHSS-2013, there was a prevalence of self-reported T2DM of 6.2%, higher in women (7.0 vs 5.4%), and among older adults, reaching 19.8% of the elderly17,19.
In a study conducted in the city of São Carlos, southeastern Brazil, with individuals in the 30-79 year age group, it verified the occurrence of 16.6% of T2DM, with an increasing prevalence according to increasing age.
In Viçosa, southeast Brazil, 621 older adults were studied, the majority (53.3%) being female. Age ranged between 60 and 98 years, and the prevalence of self-reported T2DM was 22.4%20.
In addition to these studies, we can cite the Monte Negro Study, with people over 59 years of age, in which the prevalence of T2DM was 22%16.
In the cross-sectional study, based on the system of Surveillance of Risk and Protective Factors for CND by Telephone Survey (VIGITEL-2009), 54,369 individuals aged over 18 years were interviewed, the prevalence of T2DM self-reported was 5.3% for the set of municipalities studied, with higher prevalence in females (6.0%)21.
In addition to these studies, we can cite the Monte Negro Study, with people over 59 years of age, in which the prevalence of T2DM was 22%16.
Based on these data, we can verify a positive association between T2DM and increasing age, which has already been argued in the literature5,13. According to the Brazilian Diabetes Association, in the age group above 65 years, the prevalence of T2DM is about one-fifth of the Brazilian population, and can be justified by the changes inherent to the aging process, by the reduction of physical activity, obesity and unhealthy eating habits9.
This study shows a prevalence of T2DM of 16,4%, similar to other studies in Brazil16-20 and emphasizes the relation between the disease and sedentarism, as shown in Table 3.
Dyslipidemia
Studies on the prevalence of dyslipidemia in the general population and in specific regions are scarce in Brazil24. The Monte Negro Study shows dyslipidemia with a prevalence rate of 65.2%, where only 12% are being treated appropriately16. A population-based cross-sectional study with individual data from the VIGITEL-2009, despite methodological limitations, in telephone interviews of individuals of both sexes, aged 18 years or more, living in the state capitols of Brazil, in 2009, showed a prevalence of dyslipidemia of 15%, increasing with age24.
This study points for a prevalence of dyslipidemia of 50,5% in the general population, higher in females (59.2%), but with no statistical association for sex. Table 4 calls attention for the association of obesity with dyslipidemia. In this study, obese people had a proability of 1.3 of dyslipidemia and females have a higher probability of 1.7 times. This association was also observed in other studies24.
Metabolic Syndrome (MS)
The prevalence of the MS risk factor was higher in women (33.8%) as can be seen in Table 1. We found variations in prevalence throughout the literature, due to the profile of the population studied. A study conducted in Novo Hamburgo, south of Brazil, in the elderly (68 ±6 years old) found a prevalence of 56.9% of MS22. A study conducted in Greece observed a prevalence of approximately 12% in both sexes, with age above 70 years23. In the Monte Negro Study, with people over 59 years of age, the prevalence of MS was 45.4%16. This study shows a general prevalence a MS of 24%. Given these data, we can observe a variation in the prevalence of MS in different populations, which indicates the need for local studies that better define these prevalences. As discussed above, the riverine women lifestyle and, may collaborate for this greater prevalence, when compared with men.
CKD
Regarding the glomerular filtration rate less than 60mL/min/1.73m2, we observed a prevalence of 12.1% in both sexes. A study conducted in Juiz de Fora - MG, in adult individuals, identified a prevalence of 9.6% of CKD in the initial stage25. In a study conducted in Rio Branco (Acre State, Amazon Region), involving 1,016 elderly (>60 years), a general prevalence of CKD of 21.4% was verified, associated with the following factors: age, diabetes, MS, hypertension and obesity26. In the Monte Negro Study, the prevalence was 53.4% in older than 59 years16.
The decrease in renal function, which seems to begin early in the second decade of life and the prevalence of CKD increases with advancing age27. The fact that the studied population is neglected in relation to the treatment of comorbidities such as SAH, T2DM and dyslipidemia and their associated factors (obesity, MS and sedentary lifestyle), the prevalence of DRC in this population is as expected. The lower age of the riverine population in this study may have collaborated to find a lower CKD prevalence, when compared with other studies.
Sedentary Lifestyle and Obesity
Among the associated factors evaluated in the study, the most prevalent was a sedentary lifestyle (34.8%), with a higher frequency in females (50%), and the least prevalent was alcoholism (7.3%).
More than 45% of the population studied had at least two risk factors. In a cross-sectional study, through the VIGITEL Telephone Survey, the prevalences was: sedentary lifestyle 16.2% and overweight 50.8%. The presence of associated factors was associated with male sex, older age, and lower schooling19. As a consequence, overweight and obesity reach high levels, as well as increasing the prevalence of CND, such as T2DM and SAH.
Changes were observed in the dietary patterns of the riverine, with the substitution of the consumption of natural products, diet poor in fruits and fibers, by industrialized products, rich in carbohydrates, usually less perishable, considering the lack of electricity and the consequent lack of refrigerated food storage conditions. There are no vegetable gardens in the communities, and the fiber fronts are available only in local fruits (mango, cupuaçu and palm tree nuts as açaí, bacaba and patoá), and the substitution of the habit of rowing by the use of engines in the boats. These situations trigger overweight and obesity.
With the increase in the longevity of the population, there is an aggregation of associated factors, which results in compromising people's quality of life, and population aging increase the probability of involvement of CND5.
The use of a non-randomic sample could have introduced a selection bias in the study by selecting sick people who searched for medical attention or were absent seeking medical assistant in more developed areas. On the other hand, people who were healthy, could not seek for the medical attention subsidized by the research team. Even so, 79% of the target population was examined by the research team.
CONCLUSION
In this study the researchers we were able to verify a high prevalence of CND and their associated factors in the riverine population, and the scarcity of Brazilian studies that measure health conditions in these populations.
The access of these populations to health services is limited, economic conditions are unfavorable, and health problems are often solved in the community itself. The low coverage of the GSHS/CHA reinforces this situation.
The riverine life style, with a more difficult access to fast food television and game devices (screen time) and an increase in physical activities linked to agriculture, fishing and mining, and the younger population studied in this researche project may contribute to this lower CND prevalence when compared with other studies.
Strategic public health measures should be implemented in this region, control, prevention and health promotion, improvement of GFHS/CHA coverage, training of CHA to manage CND, diagnoses and early treatment of diseases are necessary to decrease the high rates of morbidities by CND.
REFERENCES
1.Omram AR. The epidemiological transition: a theory of the epidemiology of population change. Milbank Memorial Fund Quarterly. 1971; 49(4):509-583. [ Links ]
2.Horiuchi S. Epidemiologic transitions in humam history. In: UNITED NATIONS. Health and mortality issues of global concern: proceedings of the Sumposium on Health and Mortality, New York, p. 54-71, 1999. [ Links ]
3.Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015; 386: 743-800. [ Links ]
4.Achutti A, Azambuja MIR. Doenças Crônicas Não-Transmissíveis no Brasil: Repercussões do Modelo de Atenção a Saude Sobre a Seguridade Social. Ciência & Saúde Coletiva, 9 (4): 833-840, 2004. [ Links ]
5.Schmidt MI, Duncan BB, Azevedo e Silva G, Menezes AM, Monteiro CA, Barreto SM et al. Chronic non-communicable diseases in Brazil: burden and current challenges. Lancet. 2011;377:1949-61. [ Links ]
6.Fraxe TJP, Pereira HS, Witkoski AC. Comunidades ribeirinhas amazônicas: modos de vida e uso dos recursos naturais. Manaus: EDUA; 2007. [ Links ]
7.Gama ASM, Fernandes TG, Parente RCP. Secoli SR. Inquérito de saúde em comunidades ribeirinhas do Amazonas, Brasil. Caderno de Saúde Pública. 34(2):e00002817. 2018. [ Links ]
8.7ª Diretriz Brasileira de Hipertensão Arterial. Arquivos Brasileiros de Cardiologia, Volume 107, Nº 3, Suplemento 3. Rio de Janeiro, 2016. [ Links ]
9.Diretrizes da Sociedade Brasileira de Diabetes: 2014-2015/Sociedade Brasileira de Diabetes ; [organização José Egidio Paulo de Oliveira, Sérgio Vencio]. - São Paulo: AC Farmacêutica, 2015. [ Links ]
10.Diretriz Brasileira de Dislipidemias e Prevenção da Aterosclerose. Arq Bras Cardiol 2013; 101 (4 Supl. 1):1-20. [ Links ]
11.K/DOQI. Clinical practice guidelines for chronic kidney disease: evaluation, classification and stratification. Am J Kidney Dis 2002;39 (suppl):S1-S246. [ Links ]
12.Rocha-Brischiliari, et al. Doenças Crônicas não Transmissíveis e Associação de Fatores de Risco. Revista Brasileira de Cardiologia, 2014, 27 (I): 35-42. [ Links ]
13.Oliveira BFA, Mourão DS, Gomes N, Costa JMC, Souza AV, Bastos WR, et al. Prevalência de hipertensão arterial em comunidades ribeirinhas do Rio Madeira, Amazônia Ocidental Brasileira. Cad Saúde Pública 2013; 29:1617-30. [ Links ]
14.Rosário TM, Scala LCN, França GVA, Pereira MR, Jardim PCBV. Fatores associados à hipertensão arterial sistêmica em Nobres - MT. Rev Bras. Epidemiol 2009;12(2):248-57. [ Links ]
15.Borges HP, Cruz NC, Moura EC. Associação entre hipertensão arterial e excesso de peso em adultos, Belém, Pará, 2005. Arq Bras Cardiol 2008; 91:110-8. [ Links ]
16.Coelho, et al. The New Challenge: The Aging Process in the Brazilian Amazonia J Gerontol Geriatr Res: 2015, 4:1 [ Links ]
17.Instituto Brasileiro de Geografia e Estatística. Pesquisa nacional por amostra de domicílios (PNAD 2013): Percepção do estado de saúde, estilo de vida e doenças crônicas. Rio de Janeiro: IBGE; 2014. [ Links ]
18.Leal MO, Jardim ADI. Qualidade da informação sobre diabéticos e hipertensos registrada no Sistema Hiperdia em São Carlos - SP, 2002-2005. Revista de Saúde Coletiva, Rio de Janeiro, 19(2): 405-417, 2009. [ Links ]
19.Malta DC, et al. Fatores associados ao diabetes autorreferido segundo a Pesquisa Nacional de Saúde, 2013. Revista de Saúde Pública. 2017;51 Supl 1:12s. [ Links ]
20.Vitoi NC, et al. Prevalência e fatores associados ao diabetes em idosos no município de Viçosa, Minas Gerais. Revista Brasileira de Epidemiologia. Out.Dez, 2015; 18(6): 953-965. [ Links ]
21.Schmidt MI, Duncan BB, Hoffmann JF, Moura L, Malta DC, Carvalho RM. Prevalence of diabetes and hypertension based on self-reported morbidity survey, Brazil, 2006. Rev. Saúde Pública. 2009 nov;43 Suppl 2:74-82. [ Links ]
22.Rigo J C, Vieira JL, Dalacorte RR, Reichert CL. Prevalência de síndrome metabólica em idosos de uma comunidade: comparação entre três métodos diagnósticos. Arq Bras Cardiol, v. 93, n. 2, p. 85-91, 2009. [ Links ]
23.Guize L, Pannier B, Thomas F, Bean K, Jégo B, Benetos A. Recent advances in metabolic syndrome and cardiovascular disease. Arch Cardiovasc Dis. 2008; 101:577-583. [ Links ]
24.Pereira LP, et al. Dislipidemia autorreferida na região Centro-Oeste do Brasil: prevalência e fatores de risco. Ciência & Saúde Coletiva, 20(6):1815-1824, 2015. [ Links ]
25.Bastos RMR, Bastos MG, Ribeiro LC, Bastos RV, Teixeira MTB. Prevalência da Doença Renal Crônica nos Estágios 3, 4 e 5 em adultos. Rev Assoc Med Bras 2009; 55(1): 40-4. [ Links ]
26.Amaral TLM, Amaral CA, Vasconcellos MTL, Monteiro GTR. Prevalência e fatores associados a doença renal crônica em idosos. Rev Saúde Pública. 2019;53:44. [ Links ]
27.Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, et al. Prevalence of chronic kidney disease in the United Sta¬tes. JAMA 2007; 298:2038-47. [ Links ]
28.Veras R. Envelhecimento populacional contemporâneo: demandas, desafios e inovações. Rev Saúde Pública. 2009; 43(3):548-54. [ Links ]
29.Zangirolami-Raimundo, J.; Echeimberg, J. O.; Leone, C. Research methodology topics: Cross-sectional studies. Journal of Human Growth and Development. 2018; 28(3): 356-360. [ Links ]
 Correspondence:
Correspondence:
Juliana de Souza Almeida Aranha Camargo
spider@icbusp.org
Manuscript received: december 2020
Manuscript accepted: december 2021
Version of record online: january 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}