










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.1 Santo André jan./abr. 2022
http://dx.doi.org/10.36311/jhgd.v32.12618
ORIGINAL ARTICLE
doi: 10.36311/jhgd.v32.12618
Spatial Clusters of Chronic Childhood Conditions in the State of Paraíba, Brazil
Malu Micilly Porfírio Santos PintoI; Luciana Moura Mendes de LimaII; Rackynelly Alves Sarmento SoaresII; Simone Elizabeth Duarte CoutinhoIII; Ana Tereza de MedeirosIV; Ronei Marcos de MoraesIV
IMaster in Decision and Healthcare models, Universidade Federal da Paraíba, João Pessoa, Paraíba, Brazil
IIPhD in Decision and Healthcare models, Universidade Federal da Paraíba, João Pessoa, Paraíba, Brazil
IIIProfessor of the Department of Nursing in Collective Health, Universidade Federal da Paraíba, João Pessoa, Paraíba, Brazil
IVProfessor of The Graduate Program in Decision and Healthcare Models, Universidade Federal da Paraíba, João Pessoa, Paraíba, Brazil
ABSTRACT
INTRODUCTION: chronic conditions are complex health problems that require continuous and multidisciplinary care. When they affect children/adolescents, they require hospitalizations and periodic and long-term follow-up. Understanding the geographical distribution of these conditions will provide greater visibility to the problem and support the decision-making process
OBJECTIVE: detect the spatial clusters of chronic health conditions affecting children and adolescents in the state of Paraíba, Brazil
METHODS: ecological, retrospective, study employing secondary data from the Information System of Children and Adolescents with Chronic Disease from a reference hospital in the state of Paraíba, Brazil, covering the period from 2015 to 2017. The Spatial Incidence Ratio and the Spatial Scan statistic were used for the data analysis
RESULTS: a concentration of spatial clusters was observed in the Mata Paraibana mesoregion, an area where the public hospital service is located, which functions as a reference in the recurrent hospitalizations of this population with chronic conditions
CONCLUSION: the detection of spatial clusters can help public managers to recognize the priority areas for the monitoring of chronic conditions in children and adolescents
Keywords: chronic condition, child, adolescent, spatial analysis.
Authors summary
Why was this study done?
The recognition of spatial clusters helps to identify and visualize priority areas for monitoring children's chronic conditions, helping management in the decision-making process regarding the care of this population, as well as subsidizing the maintenance or expansion of access to health services and in the elaboration of effective public policies.
What did the researchers do and find?
This study aimed to detect the spatial clusters of chronic health conditions that affect children and adolescents in the state of Paraíba, Brazil, that does not have, to date, scientific research that address the geographic distribution of these cases. There was a greater concentration of spatial clusters in the mesoregion of the forest in the city, where the public hospital service is located, which acts as a state reference in the recurrent hospitalizations of this population in chronic condition.
What do these findings mean?
Perhaps this fact has contributed to the greater concentration of spatial clusters in this specific mesoregion, which leads to a reflection on the complexity of the problem of chronic childhood illness and its demand for health services that provide complex and resolving care. The proximity of the family to the specific health service favors the continuity of child care, however, this option is not always valid for families of children who reside in another municipality or even mesoregion, highlighting the need for quality care in all its levels, from primary to the tertiary referral service, in order to ensure that the specific needs of the child/adolescent are addressed both in the municipality/mesoregion of origin of the patient and in the referral services.
INTRODUCTION
Chronic conditions are complex health problems that require continuous, multidisciplinary treatment and prolonged care management, which could involve years or even decades. Such conditions are, above all, characterized by not being limited to health problems and by the persistence and recurrence of long-lived health problems1. In children and adolescents, these chronic conditions usually have a duration of more than three months or a clinical picture that recurs more than three times2. In addition, they require hospitalizations and periodic follow-up by specialized health teams3.
Regarding the epidemiological profile of these conditions, there has been an increase in the number of cases4,5 according to the National Household Sample Survey (Pesquisa Nacional por Amostra em Domicílios, PNAD), which revealed that 9.1% of children from 0 to 5 years, 9.7% from 6 to 13 years and 11% of adolescents from 14 to 19 years among the general population have some chronic condition6. Concomitantly, the number of new cases of hospital admissions has trended upwards, with Brazil registering a rate of 331 per 100,000 inhabitants in 2013. Among children under one year of age, in particular, this figure is greater than 1,000 per 100,000 inhabitants5.
This epidemiological situation of childhood chronicity and consequent recurrent hospitalizations also implies a strong impact on the family dynamics of these individuals, whose daily routines involve difficulties in understanding the diagnosis, in dealing with prejudices, in addition to facing obstacles in the search for adequate care on which the child will depend for years to come in order to have a better quality of life7.
As such, the development ofeffective public policies is necessary to provide better health conditions to the mother-child binomial. Spatial information contribute to this requirement by supporting the decision-making process and furthering our understanding of how these individuals are distributed geographically8.
A spatial analysis enables the identification of characteristics related to these events in the territory in order to plan prevention and control measures through specific public policies. In this sense, the geopolitical and social context can influence the determination of health/disease processes1.
Few studies in the literature address the geographical distribution of chronic childhood condition cases in Brazil. In addition, no scientific research was found that contemplated the northeastern state of Paraíba or regions with similar characteristics. As such, the objective of this study is to detect the spatial clusters of chronic health conditions affecting children and adolescents in the state of Paraíba.
METHODS
This study is characterized by an ecological, retrospective, quantitative approach, employing secondary-type data of the Information System of Children and Adolescents with Chronic Disease (Sistema de Informação de Crianças e Adolescentes com Doença Crônica, SICADC) from a reference hospital for this condition in the state of Paraíba in the period from 2015 to 2017.
The state of Paraíba is one of the 27 Federative Units of Brazil, located in the east of the northeast region of the country. The city of João Pessoa is its capital. The state has 223 municipalities distributed in four mesoregions, as can be seen in figure 1 Its mesoregions are: Mata Paraibana, Agreste Paraibano, Borborema and Sertão Paraibano, divided according to their characteristics and forms of socio-economic and political organization6.
The following measures were used in the data analysis: Spatial Incidence Ratio (SIR) and the Spatial Scan statistic in order to detect the spatial clusters of chronic conditions in childhood.
SIR is a spatial measure that allows for the standardization of information according to the population of a given area, enabling more consistent comparative analyses8,9. To this end, two important entities must be understood: geo-object and geographical region. The geographical region refers to a delimited geographical area of study where the events of interest occur. It can be represented by a collection of distinct and geographically locatable objects within it, called geo-objects10. In the current study, the aggravation of chronic conditions among children/adolescents in the state of Paraiba was used, as acquired from the total number of recorded chronic disease cases in each municipality. As such, Paraíba refers to the geographical region and each municipality to a geo-object.
Formally, a geographical region A is formed by a set N of geo-objects, i.e., ai ϵ A, i=1,..., N. X is a random variable that corresponds to the total number of cases recorded in a given time interval within a geo-object in ai, in the geographical region A. And finally, G is the population at risk in geographical region A. The SIR in each geo-object ai is given by the following equation:

That is, the SIR of the geo-object ai is given by an incidence ratio, in which the numerator corresponds to the incidence of an epidemiological event in the geo-object and the denominator to the incidence in the entire geographical region.
The SIR is interpreted by dividing it into class intervals in which one color is associated with each pre-established interval so that the areas on the map are colored according to their class. Its values are explained as follows: an SIR equal to zero means there is no incidence of the epidemiological event in the geo-object ai; values greater than 0 and less than 0.5 mean that the SIR in the geo-object ai is less than half of the global incidence in the geographical region; values greater than or equal to 0.5 and less than 1.0 mean that the SIR in the geo-object ai is more than half, but less than the overall incidence in the geographical region; values greater than or equal to 1.0 and less than 1.5 mean that the SIR in the geo-object ai is greater than the global incidence and less than 1.5 of the global incidence in the geographical region; values greater than or equal to 1.5 and less than 2.0 mean the SIR in the geo-object ai is more than 1.5 times of the global incidence, but less than 2.0 of the global incidence in the geographical region; finally, values greater than or equal to 2.0 mean the SIR in the geo-object ai is more than 2.0 times the global incidence in the geographical region8,11.
The spatial clusters were detected through the Spatial Scan statistic. This statistic was proposed in 1995 by Kulldorff and Nagarwalla and corresponds to a method that aims to detect and identify spatial clusters; that is, it performs a search for the entire region to find areas where the occurrence of a phenomenon is significantly more likely. It is used in data that does not require a distribution that is close to normal. Among the possible probabilistic models to be used with the Spatial Scan statistic, the Poisson model was adopted12 because we're dealing with count data13.
In this method, an association of the information of the area is made with a single point within a polygon, be it a circle,14 an ellipse,15 a rectangle16, or another geometric shape17. This point is called the centroid and represents the center of each area of the region. In this study, the circular format was used since it facilitates the observation of the functionality of the methods.
The Circular Scan statistic generates a Z window in each centroid of the subregions, where a window consists of the circle created from the centroid. For any of these centroids, the radius of the circle varies continuously from zero to a percentage of the population at risk to be covered, established by the user. If a window contains the centroid of a subregion, therefore, the radius of the circle will grow to encompass the established percentage of the population in this region18.
There is no standardization in the literature regarding the percentage of the population at risk, in which the search radius increases until including a maximum percentage of the population. It is only recommended that it does not exceed 50% of the population19. For this study, the percentages of 0.1%, 0.2%, 0.3%, 0.4%, 0.5%, 0.7%, 1%, 3%, 5%, 7% and 10% of the population at risk were analyzed on the Scan statistic maps for each year of the study, using the SIR maps as reference.
The data were stored in a spreadsheet and analyzed in the R software. The project was approved by the Research Ethics Committee under the number 2.729.054 (CAEE No. 91161118.3.0000.5188), respecting the criteria established in Resolution No. 466 of December 12, 2012 which regulates research in human beings.
RESULTS
There were 116 chronic disease cases in children/adolescents registered in the SICADC of a reference hospital in the period from 2015 to 2017 in the state of Paraíba. The main diagnoses of chronic conditions in children and adolescents in this period were: asthma, type I diabetes mellitus, neuropathies, nephropathies, heart disease, and systemic lupus erythematosus. The predominant age group was children up to one year of age.
Figure 2shows the SIR and Circular Scan statistic of the chronic condition in children and adolescents in the year 2015. The SIR of the chronic condition varied between 0 and 39.78 per thousand inhabitants, with the largest record occurring in the municipality of Santo André located in the Borborema mesoregion. In the State, 27 cities had a non-zero SIR, mostly involving a SIR that was 2,0 times greater or more than the global incidence in the geographical region of the geo-object ai. With regard to the Circular Scan statistic, 0.3% of the population at risk was used, detecting ten spatial clusters with a greater concentration in the east of the state of Paraíba in the Mata Paraibana mesoregion.
The SIR and Circular Scan statistic of chronic conditions in children and adolescents in year 2016 in the state of Paraíba can be seen in figure 3 The SIR with the highest record occurred in the city of Poço Dantas, located in the Sertão Paraibano mesoregion. Of the 223 municipalities, 32 had a non-zero SIR with a greater concentration in the east of the state. The Circular Scan statistic with the percentage of 0.3% of the population at risk identified eight spatial clusters with a greater concentration in the east of the state, in the Mata Paraibana mesoregion.
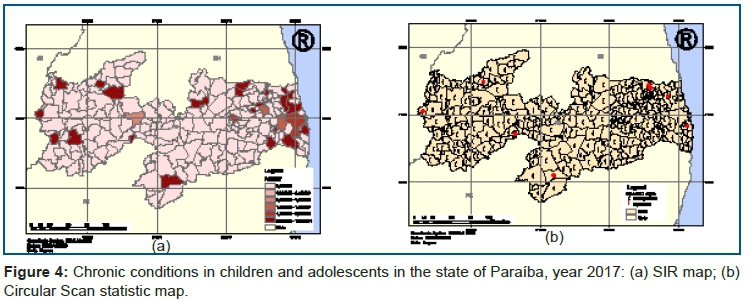
Figure 4 (a) shows the SIR map of chronic conditions in children and adolescents in the state of Paraíba in 2017, whose values varied from 0 to 19 per thousand inhabitants. In the state of Paraíba, 29 municipalities had a SIR different from zero and, of these, 23 had a SIR equal to or greater than 2.0 times the geographical region. These municipalities were mostly concentrated in the east of the state in the Mata Paraibana mesoregion. The Circular Scan statistic detected nine spatial clusters with a population at risk of 0.2% and a higher concentration in the aforementioned mesoregion.
DISCUSSION
The current study investigated chronic condition cases in children and adolescents in the state of Paraíba from 2015 to 2017. Through the Circular Scan statistic, it was possible to identify and detect that the spatial clusters had a higher concentration in the Mata Paraibana mesoregion in the three years of the study and that this coincided with the highest SIRs. The aforementioned mesoregion harbors a public hospital that functions as a reference for Paraíba regarding the care, diagnosis, and treatment of children and adolescents with chronic conditions. This fact could have contributed to the higher concentration of spatial clusters in this particular mesoregion.
This geographical coincidence between the spatial clusters of children/adolescents affected by chronic conditions and the hospital refers to a reflection on the complexity of the chronic childhood illness issue and the demand for healthcare services that provide complex and resolving care. The proximity of the family to the specific healthcare service favors the continuity of care to the child, but this option is not always available for the families of children who reside in another municipality or even mesoregion, sometimes leading to difficulties in accessing the service and even the discontinuity of care.
In this context, the need for quality care at all levels should be emphasized, from primary care to tertiary reference services, through an effective system of reference and counter-reference within the health care network, ensuring that the specific needs of the child/adolescent-family binomial are taken into account at both the municipality/mesoregion of origin of the patient and in the reference service20.
Studies have shown that children and adolescents with chronic conditions need periodic, routine consultations in the various specialties, in addition to recurrent hospital admissions3. In general, hospitalizations are prolonged and frequent, limiting the social and family relations of the child/adolescent-family binomial. It is an unpleasant, exhausting, tiring experience with psychological consequences due to the constant tension of expectations, marked by frequent examinations and several invasive procedures, which are necessary to safeguard the child from harm and worsening of the condition21. It is a therapeutic trajectory characterized by the search for a solution to the health situation, in which reference hospitals or university services are points of care in search of a resolution22.
As such, this study sheds light on the spatial distribution of chronic childhood illness in the state of Paraíba, mainly by indicating the mesoregions that should be prioritized in its monitoring. This knowledge can help managers in maintaining or expanding access to health services and in developing effective public policies for the prevention and/or management of these conditions. In the scientific literature, spatial analyses in healthcare have become an important research tool in the field of epidemiology due to their ability to provide a detailed investigation of the spread of diseases and indicate new forms of support for the planning and evaluation of healthcare actions. Spatial analysis techniques enable the simultaneous statistical analysis of social, economic, and environmental variables that act on a given population, and they are useful to detect vulnerable areas where health problems occur more frequently, as well as the influence of each variable in determining the occurrence of the event23,24.
Spatial cluster methods, therefore, can assist managers in the adoption of effective measures to prevent and control diseases with the identification of these priority areas23. The Spatial Scan statistic has been used in health research in order to understand the spatial distribution of several diseases that are considered relevant in the field of public health, such as acute myocardial infarction19, hematological diseases24, leprosy25, dengue18,26, tuberculosis27, among others. With regard to chronic conditions, there are still few studies that seek to identify, describe and understand the importance of the spatial component in relation to the development of the health-disease process, especially when it is restricted to the period of childhood and adolescence.
One limitation found in this study refers to the secondary data source used from the SICADC. This is a local database, which may not have included all chronic condition cases in children and adolescents in the state of Paraíba. In addition, the total population for the years of 2015 to 2017, provided by the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística, IBGE) and necessary for the implementation of the methods - is divided by age group categories (0 to 19 years) and not by age. SICADC, on the other hand, uses a division by age (from 0 to 17 years).
CONCLUSION
The current study made it possible to detect spatial clusters of child and adolescent patients with chronic conditions in the state of Paraíba in the period from 2015 to 2017. The employed methodology proved to be adequate and easy to understand, especially for the health manager.
The recognition of these clusters helps identify and visualize the priority areas for the monitoring of chronic conditions. It can therefore assist in the planning, maintenance, and/or expansion of the health services of this population, which requires special attention. It can also provide support to public health policy actions.
REFERENCES
1.Goodman RA, Posner SF, Huang ES, Parekh AK, Koh HK. Defining and measuring chronic conditions: Imperatives for research, policy, program, and practice. Preventing Chronic Disease [Internet]. 2013 [cited 2021 Jul 1]; 10(4): 1-16. Available from: https://pubmed.ncbi.nlm.nih.gov/23618546/ [ Links ]
2.Moreira MCN, Gomes R, Sá MRC de. Doenças crônicas em crianças e adolescentes: Uma revisão bibliográfica. Vol. 19, Ciencia e Saude Coletiva. Associacao Brasileira de Pos - Graduacao em Saude Coletiva; 2014. p. 2083-94. [ Links ]
3.Nóbrega VM, Silva ME de A, Fernandes LTB, Viera CS, Reichert AP da S, Collet N. Chronic disease in childhood and adolescence: Continuity of care in the Health Care Network. Revista da Escola de Enfermagem [Internet]. 2017 Jun 12 [cited 2021 Jul 1]; 51. Available from: http://dx.doi.org/10.1590/S1980-220X2016042503226 [ Links ]
4.Alves Pereira R, Alves-Souza RA, De Sousa Vale J. O PROCESSO DE TRANSIÇÃO EPIDEMIOLÓGICA NO BRASIL: UMA REVISÃO DE LITERATURA [Internet]. Vol. 6, Revista Científica da Faculdade de Educação e Meio Ambiente. 2015 Jul [cited 2021 Jul 1]. Available from: http://www.faema.edu.br/revistas/index.php/Revista-FAEMA/article/view/322 [ Links ]
5.Moura EC, Moreira MCN, Menezes LA, Ferreira IA, Gomes R. Condições crônicas complexas em crianças e adolescentes: Internações no Brasil, 2013. Ciencia e Saude Coletiva. 2017; 22(8): 2727-34. [ Links ]
6.IBGE Censo 2010 [Internet]. [cited 2021 Jul 1]. Available from: https://censo2010.ibge.gov.br/sinopse/index.php?uf=13%26dados=4 [ Links ]
7.Bolla BA, Fulconi SN, Baltor MRR, Dupas G. Cuidado da criança com anomalia congênita: a experiência da família. Escola Anna Nery. 2013 Jun; 17(2): 284-90. [ Links ]
8.Lima LMM, de Toledo Vianna RP, de Moraes RM. Spatial and spatio-temporal analysis of congenital malformations of nervous system in the state of Paraiba from 2010 to 2016. Journal of Human Growth and Development [Internet]. 2019 [cited 2021 Jul 1]; 29(2): 169-76. Available from: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S0104-12822019000200005&lng=pt&nrm=iso&tlng=en [ Links ]
9.ANÁLISE COMPARATIVA DE MÉTODOS DE AGLOMERAÇÃO ESPACIAL PARA ESTUDOS EPIDEMIOLÓGICOS / COMPARATIVE ANALYSIS OF SPATIAL CLUSTERING METHODS FOR EPIDEMIOLOGICAL STUDIES | Pinto | Revista Espaço e Geografia [Internet]. [cited 2021 Jul 1]. Available from: http://www.lsie.unb.br/espacoegeografia/index.php/espacoegeografia/article/view/618 [ Links ]
10.Goodchild MF. Geographical data modeling. Computers and Geosciences. 1992 May 1; 18(4): 401-8. [ Links ]
11.De Lima LMM, De Sá LR, Dos Santos MacAmbira AFU, De Almeida Nogueira J, De Toledo Vianna RP, De Moraes RM. A new combination rule for Spatial Decision Support Systems for epidemiology. International Journal of Health Geographics [Internet]. 2019 Nov 9 [cited 2021 Jul 1]; 18(1): 25. Available from: https://doi.org/10.1186/s12942-019-0187-7 [ Links ]
12.Kulldorff M, Nagarwalla N. Spatial disease clusters: Detection and inference. Statistics in Medicine [Internet]. 1995 [cited 2021 Jul 1]; 14(8): 799-810. Available from: https://pubmed.ncbi.nlm.nih.gov/7644860/ [ Links ]
13. A Spatial Scan Statistic [Internet]. [cited 2021 Jul 1]. Available from: https://www.satscan.org/papers/k-cstm1997.pdf [ Links ]
14.Kulldorff M, Huang L, Pickle L, Duczmal L. An elliptic spatial scan statistic. Statistics in Medicine [Internet]. 2006 Nov 30 [cited 2021 Jul 1]; 25(22): 3929-43. Available from: https://onlinelibrary.wiley.com/doi/full/10.1002/sim.2490 [ Links ]
15.Detecting Elongated Disease Clusters [Internet]. [cited 2021 Jul 1]. Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/su5401a43.htm [ Links ]
16.Duczmal L, Assunção R. A simulated annealing strategy for the detection of arbitrarily shaped spatial clusters. [cited 2021 Jul 1]. Available from: http://www.est.ufmg.br/~duczmal/Simulated_Annealing.pdf [ Links ]
17.Tango T, Takahashi K. A flexibly shaped spatial scan statistic for detecting clusters. International Journal of Health Geographics [Internet]. 2005 May 18 [cited 2021 Jul 1]; 4(1): 1-15. Available from: http://www.ij-healthgeographics.com/content/4/1/11 [ Links ]
18.Melo JCS, Melo ACO, Moraes RM. (2016) Comparação dos Métodos Scan Circular e Flexível na Detecção de Aglomerados Espaciais de Dengue. In: Escola de Informática Teórica e Métodos Formais (ETMF 2016); 2016 Nov 22-23; Natal, Brasil, p. 11-19. [ Links ]
19.Kjærulff TM, Ersbøll AK, Gislason G, Schipperijn J. Geographical clustering of incident acute myocardial infarction in Denmark: A spatial analysis approach. Spatial and Spatio-temporal Epidemiology. 2016 Nov 1; 19: 46-59. [ Links ]
20. Vaz EMC, Brito T da S, Dos Santos MCS, Lima PMV de M, Pimenta EAG, Collet N. Referral and counter-referral of children in chronic condition: Perception of mothers and secondary care professionals. Revista Enfermagem [Internet]. 2020 Oct 16 [cited 2021 Jul 1]; 28(0): 1-7. Available from: http://dx.doi.org/10.12957/reuerj.2020.51186 [ Links ]
21. Silva TP da, Silva MM da, Silva LJ da, Silva ÍR, Leite JL. Especificidades contextuais do cuidado de enfermagem à criança em condição crônica hospitalizada/Contextual specificities of nursing care to hospitalized children with chronic condition. Ciência, Cuidado e Saúde [Internet]. 2015 Jun 11 [cited 2021 Jul 1]; 14(2): 1075. Available from: https://periodicos.uem.br/ojs/index.php/CiencCuidSaude/article/view/23814 [ Links ]
22.Souza LA de, Rafael R de MR, Moura ATMS de, Neto M. Relações entre a atenção primária e as internações por condições sensíveis em um hospital universitário. Revista gaucha de enfermagem. 2018 Aug 2; 39: e20170067. [ Links ]
23.Ribeiro Barbosa I, Pereira L, Gestor S. INFLUÊNCIA DOS DETERMINANTES SOCIAIS E AMBIENTAIS NA DISTRIBUIÇÃO ESPACIAL DA DENGUE NO MUNICÍPIO DE NATAL-RN Influence of environmental and social determinants in spatial distribution of Dengue Fever in Natal, RN-Brazil [Internet]. Vol. 1, Revista Ciência Plural. 2015 [cited 2021 Jul 1]. Available from: https://periodicos.ufrn.br/rcp/article/view/8583 [ Links ]
24.Narimatsu H, Kohno K, Shiono Y, Kato Y, Suzuki I, Fukao A, et al. Applying spatial epidemiology to hematological disease using R: a guide for hematologists and oncologists. Journal of Blood Medicine [Internet]. 2014 Mar [cited 2021 Jul 1]; 5: 31. Available from: https://pubmed.ncbi.nlm.nih.gov/24624001/ [ Links ]
25.Barreto JG, Bisanzio D, de Guimarães LS, Spencer JS, Vazquez-Prokopec GM, Kitron U, et al. Spatial Analysis Spotlighting Early Childhood Leprosy Transmission in a Hyperendemic Municipality of the Brazilian Amazon Region. PLoS Neglected Tropical Diseases [Internet]. 2014 [cited 2021 Jul 1]; 8(2): e2665. Available from: http://www.censo2010.ibge.gov.br/cnefe/ [ Links ]
26.ANÁLISE DO DESEMPENHO DOS MÉTODOS SCAN E BESAG E NEWELL PARA IDENTIFICAÇÃO DE CONGLOMERADOS ESPACIAIS DO DENGUE NO MUNICÍPIO DE JOÃO PESSOA ENTRE OS MESES DE JANEIRO DE 2004 E DEZEMBRO DE 2005 | DE FIGUEIRÊDO LUCENA | Boletim de Ciências Geodésicas [Internet]. [cited 2021 Jul 1]. Available from: https://revistas.ufpr.br/bcg/article/view/15518 [ Links ]
27.Sá LR de, Nogueira J de A, Moraes RM de. Modelo de decisão sobre o perfil demográfico para o controle da tuberculose usando lógica Fuzzy. Revista Eletrônica de Enfermagem [Internet]. 2015 Jun 30 [cited 2021 Jul 1]; 17(2): 223-60. Available from: http://dx.doi.org/10.5216/ree.v17i2.27643 [ Links ]
 Correspondence:
Correspondence:
Malu Micilly Porfírio Santos Pinto
malu.porfirio@ifpb.edu.br
Manuscript received: april 2021
Manuscript accepted: june 2021
Version of record online: january 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}