










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282On-line version ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.1 Santo André Jan./Apr. 2022
http://dx.doi.org/10.36311/jhgd.v32.11796
ORIGINAL ARTICLE
doi: 10.36311/jhgd.v32.11796
Gastroschisis in Brazil within a Global Context
Virginia Maria MunizI; Antônio Lima NettoII; Luciane Bresciani SalaroliIII; Eliana ZandonadeIV
IPrograma de Pós-Graduação em Saúde Coletiva. Universidade Federal do Espírito Santo (PPGSC/UFES), Vitória, Espírito Santo, Brasil
IINúcleo de Terapia Intensiva Pediátrica e Neonatologia, Hospital Estadual Infantil Nossa Senhora da Glória, Vitória - ES, Brasil
IIIDepartamento de Educação Integrada à Saúde, Programa de Pós-Graduação em Saúde Coletiva, Universidade Federal do Espírito Santo (UFES), Vitória, Espírito Santo, Brasil
IVDepartamento de Estatística, Programa de Pós-Graduação em Saúde Coletiva, Universidade Federal do Espírito Santo, Vitória, Espírito Santo, Brasil
ABSTRACT
INTRODUCTION: global disparity in outcomes of gastroschisis is visible. Survival rates in high-income countries have improved since 1960, and are currently around 100%, due to progress in pediatric surgery and neonatal intensive care. However, in low- and middle-income countries mortality rates can reach all cases
OBJECTIVE: this study aims to map the existing literature on gastroschisis in Brazil within a global context
METHODS: scoping Review. PubMed, Scielo Brazil, Biblioteca Virtual em Saúde (BVS) and Google Scholar, were searched from January 2000 to May 2020
RESULTS: eight studies met the inclusion criteria. The consolidated data of 912 patients were: Mean maternal age of 20.7 years, antenatal diagnosis rate of 80.2%, cesarean section rate of 77.7%. Mean of hospital stay of 40.8 days. Mean mortality rate of 25.3 %. Risk factors associated with death were: prematurity, low birth weight, low APGAR score, reinterventions, sepsis, birth-to-surgery interval greater than 4 hours, fewer prenatal visits, delayed prenatal diagnosis
CONCLUSION: studies on gastroschisis in Brazil were scarce, most of carried out in southeast of country. This study suggests that there are regional contrasts on gastroschisis outcomes in Brazil. The worst results are in regions with low economic resources, a similar situation found in international literature. This review should be validated with future studies to investigate the situation of pregnant women with fetuses with gastroschisis, especially in low-resource regions, in Brazil
Keywords: Brazil, congenital abnormalities, gastroschisis, newborn, pregnancy outcome.
Authors summary
Why was this study done?
There are few publications on results of gastroschisis cohorts in low- and middle-income countries. This scope review aims to map the existing literature on gastroschisis in Brazil and to discuss the body of evidence available in a global context.
What did the researchers do and find?
Studies on gastroschisis in Brazil have been scarce, most of them carried out in southeast of country. The data were consolidated and results suggest that there are regional contrasts in outcomes of gastroschisis in Brazil. Worst results are in regions with few economic resources, a situation similar to that found in the international literature.
What do these findings mean?
It is expected to contribute to the policy makers and professionals involved in assisting patients with gastroschisis in obtaining better results in health care for this population.
INTRODUCTION
Gastroschisis (GS) is a congenital anomaly that consists of abdominal organs externalization through a defect, which in most cases is to the right of the umbilical cord; the organs are not covered by membranes1. Its pathogenesis is related to abnormalities in "physiologic" umbilical herniation, which occurs between the fifth and tenth weeks of gestation2.
A global disparity in outcomes of GS is visible3. Survival rates in high-income countries (HICs) have improved since 1960 and are currently around 100%, due to progress in pediatric surgery and neonatal intensive care3. However, in low-income countries (LICs) mortality rates can reach all cases3. The lack of antenatal diagnosis, inefficiency in pre-hospital care, limited access to neonatal intensive care units (NICU), unavailability of pediatric surgery and total parenteral nutrition (TPN) are factors related to death in regions with low economic resources3.
There are few publications on outcomes of cohorts of gastroschisis in low-and middle-income countries LMICs3. Brazil is an upper-middle-income country with regional contrasts4. Southeast region has higher Human Development Indexes (HDI), more qualified health professionals and NICU beds than those in north and northeast regions of country5,6. This Scoping review aims to map the existing literature on GS in Brazil and within the global context.
METHODS
Study Design
The method of this scoping review was based on the format described by Arksey and O'Malley7 and advanced by Levac et al.8 included the following five main phases: (1) definition of the research question, (2) recognition of relevant studies, (3) selection of the study, (4) data mapping and (5) collating, summarizing and reporting the results. The specific question was: "What is the current state of evidence on the outcomes of patients with gastroschisis in Brazil?"
Data sources
Search was performed in PubMed, Scielo Brazil, Biblioteca Virtual em Saúde (BVS). We limited our search to studies published in English and Portuguese, in the period between January 2000 and May 2020.
Search: The descriptors "Gastroschisis and Brazil" and "Gastrosquise" were adopted, and the inherent operational properties of each database were observed. The search and selection process were carried out independently by two authors (ALN and VMM), who read the title and the summary of the publications.
Study selection
The inclusion criteria were original publications on GS carried out in the NICU in Brazil. The exclusion criteria were studies that included other major congenital malformations, duplicate databases, case reports, unpublished theses or dissertations, editorials, letters from readers, qualitative studies, presentations at scientific events, book chapters, classes, research carried out exclusively with fetuses (fetal medicine) and experimental research on animals.
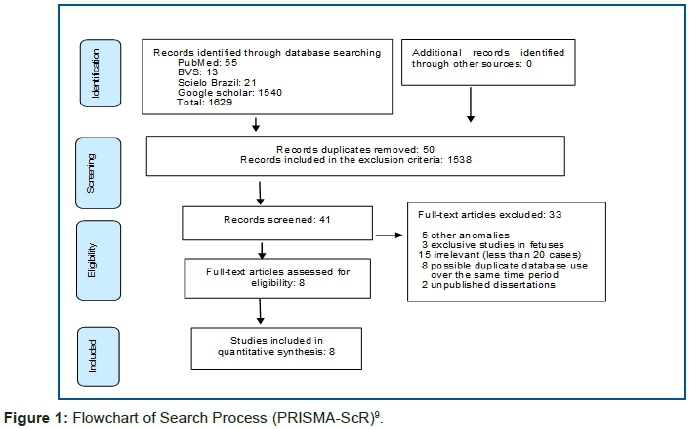
The flowchart of the study was prepared according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) (figure 1)9.
The following data were extracted: geographic region of Brazil, research period, site of study, study design, prenatal and postnatal variables. These two latter variables comprised the following parameters: Prenatal care and delivery variables: maternal age (mean) and antenatal diagnosis (%), route of delivery (vaginal or cesarean section), place of birth (inborn or outborn), gender, birth weight (grams) and gestational age (weeks). Postnatal variables: GS simple or complex gastroschisis (CG) (with atresia, stenosis, volvulus, ischemia, necrosis)10. Type of wall closure (primary closure or silo placement), TPN (mean time or percentage of use), mechanical ventilation "MV" (mean time or percentage of use), sepsis, time to first enteral feeding (mean of days), time to full enteral feeding (mean of days), hospital length of stay (mean of days), mortality rate (%) and total number of patients.
RESULTS
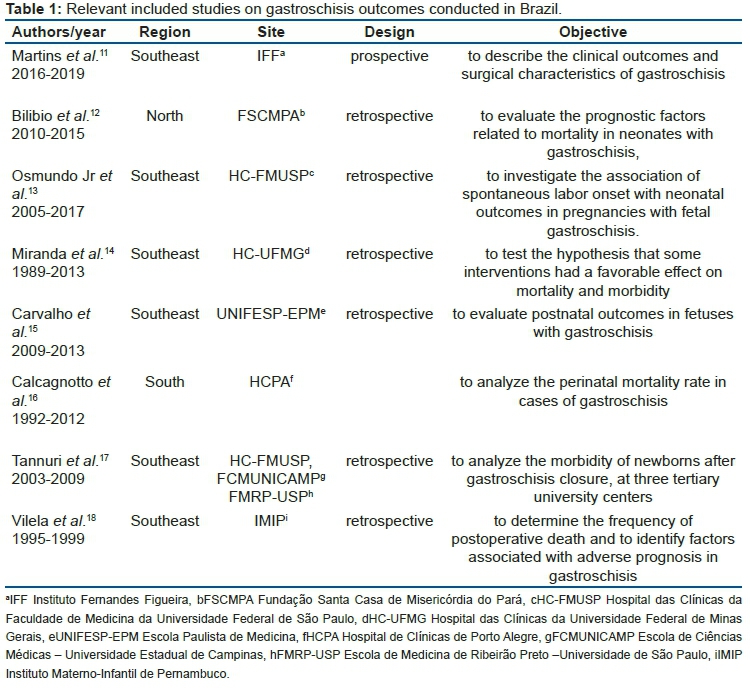
Eight studies met inclusion criteria. Table 1 shows included studies11-18.
Outcomes extracted from included studies
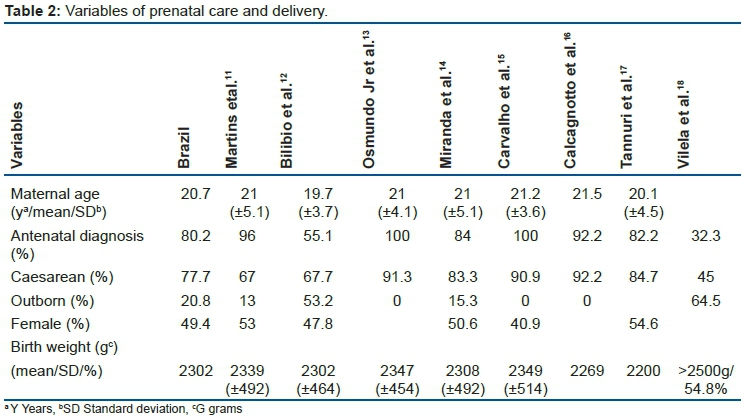
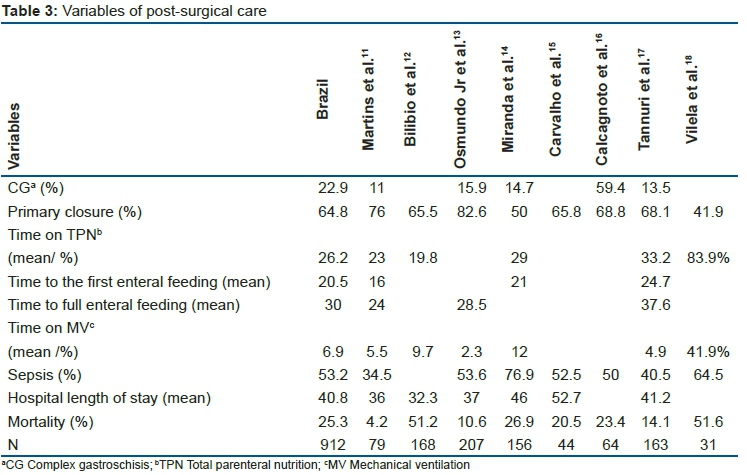
Outcomes of 912 patients were verified. The smallest number of individuals observed was 31 and the largest was 20713,18. Table 2 shows variables of prenatal care and delivery and table 3 variables of post-surgical care.
Risk factors for mortality and other associations
Three studies verified the risk factors associated with death. Calcagnotto et al.16 found prematurity (p=0.03), low weight at birth (p=0.001), low APGAR score (p=0.03), reinterventions (p=0.001) and sepsis (p=0.008). Vilela et al.18 observed birth weight less than 2 500 g (p= 0.03), birth-to-surgery interval greater than 4 hours (p=0.04) and need of mechanical ventilation (p=0.02). Bilibio et al.12 found fewer prenatal visits (p=0.004), delayed prenatal diagnosis (p=0.005), low birth weight (p=0.001), intestinal injury (p=0.001) and sepsis (p=0.001).
Moreover, spontaneous labor in preterm infants was associated with CG (p=0.002) and short bowel syndrome (p=0.013) when compared to preterm indicated deliveries13. Low postoperative serum sodium and albumin levels were associated with prolonged MV time17. CG group had a significantly smaller defect size (p=0.04), more surgical reinterventions (p=0.001), and worse clinical outcomes than simple group, with start of feeding 1.5 times longer (p=0.001), time of total parenteral nutrition use twice as long (p=0.001), and length of hospital stay 2.5 times longer11. Patients who underwent sutureless technique had significantly fewer wound infections (p=0.01) and a decreased duration of MV than sutured patients (p=0.001)11. Results before and after a protocol of care package were measured14. When compared to the previously cohort, patients had higher rates of prenatal diagnosis (p=0.001), delivery at a tertiary center (p=0.001), early closure (p=0.001), primary repair (p=0.01), monitoring of bladder pressure (p=0.001), PICC placement (p=0.001), early initiation of enteral feeding (p=0.001), and lower rates of electrolyte disturbances (p=0.001)14.
DISCUSSION
In this review, mean maternal age was 20.7 years (19.7 to 21.5 years). The lowest mean was reported in a region with the second lowest HDI in country5. In 2013, a Brazilian study showed a trend towards earlier first pregnancy among women from the north region (19.4 years) compared to the ones from the southeast region (21.9 years). These figures indicated a higher prevalence of early pregnancy in the poorest region of country19. By way of comparison, the mean maternal age in this review was lower than ones reported in similar studies from Canada (23.3 years), U.S. (22.2 years) and France (25 years)20-22.
Rates of antenatal diagnosis of GS vary considerably according to the country´s economic status. Whilst in HICs GS is antenatally diagnosed in between 68% to 100% of cases21,23, in LMICs this rate is much lower, ranging from 4.7% to 46%24-26. In our review the antenatal diagnosis total rate was 80.2% (32.2% to 100%). Studies carried out in poorest regions had lower rates of antenatal diagnosis and this indicate failures in the local health system. The antenatal diagnosis allows the proper differentiation with omphalocele, distinction between simple gastroschisis and CG, childbirth planning and family counseling27.
Cesarean rates vary among the Brazilian regions. According to a previous study, in country´s low resource region operative deliveries rates ranged from 35% to 45%, whilst in the high resource region the same rates ranged between 55% and 65%28. In HICs cesarean rates ranged from 31.5% to 68%20,22,23, and in LMICs between 5% and 76.3%24,26,29. In the current study, cesarean rate was 77.7% (45% to 92.2%). However, were higher in studies carried out in high resource settings of Brazil. The best route of birth in fetuses with GS remains controversial27,30. Purported benefits of inducing labor close to term include reducing the exposure of the intestine to amniotic fluid and reducing serious intestinal injuries. On the other hand, this procedure increases the risk of conditions related with prematurity, such as respiratory distress and other comorbidities27.
In this review, mean rate of outborn patients was 20.8% (0% to 64.5%). However, were more frequent in studies carried out in poorest region of the country. The rates of outborn in LMICs ranged from 46.8% to 100%24,26,29, whilst in HICs these rates varied between 2.9% and 62.5%20,22,23. After the diagnosis of GS is confirmed, the pregnant woman should be forwarded to a tertiary referral center for high-risk births, wherein fetal medicine, pediatric surgery, NICU, and nutritional teams are accessible27,30.
Regarding the features related to newborns, the mean of birth weight was 2 302 g (2 200 g to 2 349 g). Studies carried out around the world have found birth weight ranging from 2 232 g to 2 549g20,22,26,29. Female gender rate was 49.4% (40.9% to 54.6%), similar to studies found in the international literature20,22-24,26. The mean gestational age of this review was 36.2 weeks (35.9 to 37.6 weeks); full-term births were more frequent in studies carried out in poorest region of Brazil and were similar to rates found in LMICs26,29. The lower gestational age reflects the use of protocols for monitoring pregnancy during prenatal care, including the induction of delivery close to term in high-income health care systems20,22,23.
CG offers additional challenges to the treatment of this anomaly, since the affected newborns are more prone to multiple surgeries and long-term TPN, more vulnerable to sepsis and death10,30. In this current review, the CG rate of 22.9% (11% to 59.4%) were similar to those reported in studies from other countries22,23,25,29.
The rate of primary wall closure surgery found in this review of 64.8% (41.9% to 76%) was close to studies conducted in HICs22,23,31. This procedure, when performed immediately after birth, offers some advantages such as early positioning of the intestine back to its appropriate location and a reduction of the risk of injuries due to mechanical exposure. However, this technique is not always possible or safe, particularly in the presence of friable, distended intestinal loops or narrow intra-abdominal cavities, due to the risk of compartment syndrome32.
The mean time of TPN use was 26.2 days (19.8 to 33.2 days). Studies carried out in high resource settings of Brazil showed a mean time of TPN use similar to HICs20,22,23 and higher than those observed in MICs26,29. Maintaining a newborn on TPN is a challenge, since this procedure requires a trained team in techniques for the insertion and maintenance of intravenous catheters and handling these solutions3. In regions with few resources, these therapeutic options are not available and this may result in shorter survival times for patients with GS and reflect the shorter duration of TPN use observed in LMICs3.
The mean time to the first enteral feeding in this study was 20.5 days (16 to 24.7 days), and close to that found in the international literature20,25. The mean time to full enteral feeding of 30 days (24 to 37.6 days) was higher than those found in studies performed in HICs (24 to 26 days)22,23. Most patients with simple GS start an enteral diet around the second week of life, whereas cases of CG require prolonged fasting due to intestinal complications32.
The mean time under MV in this review was 6.9 days (2.3 to 12 days), and similar to studies carried out in HICs and MICs (4 to 9.5 days)20,22,23,26,29. Patients in LIC studies did not have access to MV26,33.
The mean sepsis rate observed in this study of 53.2% (34.5% to 76.9%) were higher than in reports from HICs (19% to 36.2%)22,23, and were close to those observed in MICs (54% to 83%)25,26,29.
The mean of length of stay observed in this review of 40.8 days (32.3 to 52.7 days) was higher than studies performed in HICs (34 to 37 days)20,23,31. In LMICs this period ranges from 17 to 34 days24-26,29,34. The long hospital stay reflects the complications of GS, which evolve with the need for several secondary surgeries, prolonged fasting and can delay the motor development of newborns32,35. A short length of stay is related to care failures and high death rates in the first weeks of life3.
The mortality rates observed in this study was 25.3% (4.2% to 51.6%). It was noted that in studies performed in high resource setting, in Brazil, the mortality rates (4% to 26.8%) were close to those observed in MICs (12% to 39.1%)26,29, and were far from those of HICs (1.4% to 3.5%)20,22,31. In low resource setting of the country, these rates (51.6% and 51.2%) were similar to those in LICs (58%)34.
Vulnerabilities in prenatal care, access to health services and postoperative care were risk factors associated with death observed in this review; and these findings are similar to those obtained in LICs3. In HICs, the outcome of death is no longer used as a primary result in cases of simple GS, as these rates negligible20. However, a recent study found birth weight, Apgar score at 5 min, and complex gastroschisis was able to predict mortality23. Another study found no statistically significant trends in the overall mortality for gastroschisis31.
In most recent studies in reference centers of high resource setting in Brazil, the use of protocols for the standardization of conduct in GS has been noted with good results. A research group composed of English and African investigators proposed three levels of intervention in cases of GS that could improve the outcomes in these patients in places with limited resources. At the micro level, educational programs aimed at neonatal resuscitation (pre- and intra-hospital), training of a multidisciplinary team and the involvement of parents in monitoring the provision of care. At the macro level, the incorporation of ultrasound in prenatal care and logistics for the provision of TPN and MV. At the global level, GS has been suggested as a sentinel condition for assessing the capacity of services to provide care in cases of neonatal surgical emergencies in general in LMICs3. The importance of these guidelines has been supported by a recent study in Uganda that achieved a 40% reduction in mortality rates after the implementation of the micro-level intervention protocol34.
In this review notice that publications on GS conducted in Brazil were scarce, most of carried out in southeast of country, with small sample size, heterogeneous methodology, not all variables were present in the included studies and only one study was multicentric. These characteristics are typical of studies on gastroschisis carried out in other countries, which has made it difficult to carry out classic systematic reviews36.
This study has several limitations. Firstly, the variables were studied heterogeneously and not all were present in the included studies. Secondly, all studies reported data on patients who had access to tertiary referral centers and under this aspect, they may not represent the entire population of patients who were born with gastroschisis in Brazil. Finally, in some studies there were periods of achievement with prolonged time differences, which may not reflect the reality of current assistance in those places.
The gaps observed in this review suggest that future studies in Brazil may be carried out with the cooperation between the tertiary reference services in GS with multicentric research and elaboration of consensus protocols on which outcomes should be verified, for better quality of care.
CONCLUSION
In summary, these clinical findings based on this review suggest that there are regionals contrasts in studies conducted on gastroschisis in Brazil. The worst outcomes are in regions with low economic resources, similar situation found in international literature. However, these results should be validated with future studies to investigate the situation of pregnant women with fetuses with gastroschisis, especially in low-resource regions in Brazil.
Contributions
Muniz V.M., Salaroli L.B. and Zandonade E. had the original concept and design of the study. Muniz V.M. and Netto A.L. performed data collection. Muniz V.M. performed data analysis, under supervision of Salaroli L.B. and Zandonade E. Muniz V.M. and Netto A.L. wrote the first draft, which was approved by all of the authors.
Acknowledgments
The authors are grateful to Professor Marcelo Ramos Muniz for the text review. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. The financial viability of the article is due to the Acre - Health Project in the Western Amazon (multi-institutional agreement process no. 007/2015 SESACRE-UFAC-FMABC).
Conflicts of Interest
Nothing to declare.
REFERENCES
1.Ruschkowsk B, Lafreniere A, Demellawy DE, Grynspan D. Gastroschisis Is Associated With Placental Delayed Villous Maturation. Pediatr Dev Pathol [Internet]. 2020 Sep [cited 2021 Aug 12]; 23(3): 197-203. Available from: https://journals.sagepub.com/doi/10.1177/1093526619875877 [ Links ]
2.Opitz JM, Feldkamp ML, Botto LD. An evolutionary and developmental biology approach to gastroschisis. Birth Defects Res [Internet]. 2019 Fev [cited 2021 Aug 12]; 111(6): 294-311. Available from: https://onlinelibrary.wiley.com/doi/10.1002/bdr2.1481 [ Links ]
3.Wright NJ, Sekabira JS, Ade-AJayi N. Care of infants with gastroschisis in low-resource settings. Semin Pediatr Surg [Internet]. Sep 2018 [cited 2021 Aug 12]; 27(5): 321-326. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7116007/ [ Links ]
4.World Bank.Washington (DC): World Bank Country and Lending Groups [Internet]. 2019 [cited 2019 Dec 20]. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups [ Links ]
5.Instituto de Pesquisa Econômica Aplicada (IPEA) Brazilia: Radar IDHM: evolução do IDHM e de seus índices componentes no período de 2012 a 2017, 2019 [Internet]. 2019 [cited 2021 Aug 12] Available from: https://www.ipea.gov.br/portal/images/stories/PDFs/livros/livros/190416_rada_IDHM.pdf [ Links ]
6.Oliveira GS, Lima MCBM, Lyra CO, Oliveira AGRC, Ferreira MAF. Desigualdade espacial da mortalidade neonatal no Brasil: 2006 a 2010. Cien Saude Colet [Internet]. Aug 2013 [cited 2021 Aug 12]; 18(8): 2431-2441. Available from: https://www.scielo.br/j/csc/a/NMCvfFKCnkp5tHKjcHcHbfk/?lang=pt [ Links ]
7.Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol [Internet]. Feb 2007 [cited 2021 Aug 12]; 8(1): 19-32. Available from: https://www.tandfonline.com/doi/abs/10.1080/1364557032000119616 [ Links ]
8.Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci [Internet]. Sep 2010 [cited 2021 Aug 12]; 5:69. Available from: https://implementationscience.biomedcentral.com/articles/10.1186/1748-5908-5-69 [ Links ]
9.Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. Extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med [Internet]. Oct 2018 [cited 2021 Aug 12]; 169(7): 467-473.Available from: https://www.acpjournals.org/doi/full/10.7326/M18-0850?rfr_dat=cr_pub++0pubmed&url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org [ Links ]
10.Bergholz R, Boettcher M, Reinshagen K, Wenke K. Complex gastroschisis is a different entity to simple gastroschisis affecting morbidity and mortality-A systematic review and meta-analysis. J Pediatr Surg [Internet]. Sep 2014 [cited 2021 Aug 12]; 49(10): 1527-32. Available from: https://www.jpedsurg.org/article/S0022-3468(14)00482-5/fulltext [ Links ]
11.Martins BMR, Abreu I, Méio MDB, Moreira MEL. Gastroschisis in the neonatal period: a prospective case-series in a Brazilian referral center. J Pediatr Surg [Internet]. Aug 2020 [cited 2021 Aug 12]; 55(8): 1546-1551. Available from: https://www.sciencedirect.com/science/article/abs/pii/S0022346820302943 [ Links ]
12.Bilibio JP, Beltrão AM, Vargens AC, Gama TB, Lorenzzoni PL. Gastroschisis during gestation: prognostic factors of neonatal mortality from prenatal care to postsurgery. Eur J Obstet Gynecol Reprod Biol [Internet] Apr 2019 [cited 2021 Aug 12]; 237: 79-84. Available from: https://www.ejog.org/article/S0301-2115(19)30179-4/fulltext [ Links ]
13.Osmundo Jr GS, Mohamed SHM, Nishie EN, Tannuri ACA, Gibellia MABC, Francisco RPV, et al. Association of spontaneous labor onset with neonatal outcomes in pregnancies with fetal gastroschisis: A retrospective cohort analysis. Acta Obstet Gynecol Scand [Internet]. Feb 2019 [cited 2021 Aug 12]; 98(2): 154-161. Available from: https://obgyn.onlinelibrary.wiley.com/doi/10.1111/aogs.13473 [ Links ]
14.Miranda ME, Emil S, Paixão RM, Piçarro C, Cruzeiro PCF, Campos BA, et al. A 25-year study of gastroschisis outcomes in a middle-income country. J Pediatr Surg [Internet]. Mar 2019 [cited 2021 Aug 12]; 54(7): 1481-1486. Available from: https://www.jpedsurg.org/article/S0022-3468(19)30137-X/fulltext [ Links ]
15.Carvalho NS, Helfer MT, Serni PO, Terasaka OA, Boute T, Araujo Junior E, et al. Postnatal outcomes of infants with gastroschisis: a 5-year follow-up in a tertiary referral center in Brazil. J Matern Fetal Neonatal Med [Internet]. Mar 2015 [cited 2021 Aug 12]; 29(3): 418-422. Available from: https://www.tandfonline.com/doi/abs/10.3109/14767058.2014.1002764?journalCode=ijmf20 [ Links ]
16.Calcagnotto H, Müller ALL, Leite JCL, Sanseverino MTV, Gomes KW, Magalhães JAA. Fatores associados à mortalidade em recém-nascidos com gastrosquise. Rev Bras Ginecol Obstet [Internet]. Dec 2013 [cited 2021 Aug 12]; 35(12): 549-53. Available from: https://www.scielo.br/j/rbgo/a/bf6tmZc3rg49rqynbBkVm3r/?lang=pt [ Links ]
17.Tannuri ACA, Sbragia L, Tannuri U, Silva LM, Leal AJG, Schmidt AFS, et al. Evolution of critically ill patients with gastroschisis from three tertiary centers. Clinics [Internet]. 2011 [cited 2021 Aug 12]; 66(1): 17-20. Available from: https://www.scielo.br/j/clin/a/WsKpdM7BNtF3jbBWXJrmbTg/?lang=en [ Links ]
18.Vilela PC, Amorim MMR, Falbo GH, Santos LC. Risk Factors for Adverse Outcome of Newborns With Gastroschisis in a Brazilian Hospital. J Pediatr Surg [Internet]. Apr 2001 [cited 2021 Aug 12]; 36(4): 559-564. Available from: https://www.jpedsurg.org/article/S0022-3468(01)69750-1/fulltext [ Links ]
19.Fernandes FCGM, Santos EGO, Barbosa IR. Age of first pregnancy in Brazil: data from the national health survey. J Hum Growth Dev [Internet]. 2019 [cited 2021 Aug 12]; 29(3): 304-312. Available from: https://revistas.marilia.unesp.br/index.php/jhgd/article/view/9523 [ Links ]
20.Youssef F, Laberge JM, Puligandla P, Emil S, Canadian Pediatric Surgery Network (CAPSNet). Determinants of outcomes in patients with simple gastroschisis. J Pediatr Surg [Internet]. Feb 2017 [cited 2021 Aug 12]; 52(5): 710-714. Available from: https://www.jpedsurg.org/article/S0022-3468(17)30051-9/fulltext [ Links ]
21.Overcash RT, DeUgarte DA, Stephenson ML, Gutkin RM, Norton ME, Parmar S, et al. Factors associated with gastroschisis outcomes. Obstet Gynecol [Internet]. Sep 2014 [cited 2021 Aug 12]; 124(3): 551-557. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4147679/ [ Links ]
22.Tosello B, Zahed M, Guimond F, Baumstarck K, Faure A, Michel F, et al. Management and Outcome Challenges in Newborns with Gastroschisis: A 6-year retrospective French study. J Matern Fetal Neonatal Med [Internet]. Dec 2017 [cited 2021 Aug 12]; 30(23): 2864-2870. Available from: https://www.tandfonline.com/doi/abs/10.1080/14767058.2016.1265935?journalCode=ijmf20 [ Links ]
23.Raymond SL, Hawkins RB, St. Peter SD, Downard CD, Qureshi FG, Renaud E, et al. Predicting Morbidity and Mortality in Neonates Born With Gastroschisis. J Surg Res [Internet]. Jan 2020 [cited 2021 Aug 12]; 245: 217-224. Available from: https://www.journalofsurgicalresearch.com/article/S0022-4804(19)30559-1/fulltext [ Links ]
24.Wesonga AS, Fitzgerald TN, Kabuye R, Kirunda S, Langer M, Kakembo N, et al. Gastroschisis in Uganda: Opportunities for improved survival. J Pediatr Surg [Internet]. Aug 2016 [cited 2021 Aug 12]; 51(11): 1772-1777. Available from: https://www.jpedsurg.org/article/S0022-3468(16)30193-2/fulltext [ Links ]
25.Marshall Niles SG, Mitchell-Fearon K, Gill MI, DeSouza CJ, Fearon IC, Abel CA, et al. Mortality-related factors in gastroschisis a Jamaican perspective. J Pediatr Surg [Internet]. Apr 2017 [cited 2021 Aug 12]; 52(4): 530-533. Available from: https://www.jpedsurg.org/article/S0022-3468(16)30506-1/fulltext [ Links ]
26.Zalles-Vidal C, Peñarrieta-Daher A, Bracho-Blanchet E, Ibarra-Rios D, Dávila-Perez R, Villegas-Silva R, et al. A Gastroschisis bundle: effects of a quality improvement protocol on morbidity and mortality. J Pediatr Surg [Internet]. Nov 2018 [cited 2021 Aug 12]; 53(11): 2117-2122. Available from: https://www.jpedsurg.org/article/S0022-3468(18)30387-7/fulltext [ Links ]
27.Haddock C, Skarsgard ED. Understanding gastroschisis and its clinical management: where are we? Expert Rev Gastroenterol Hepatol [Internet]. Apr 2018 [cited 2021 Aug 12]; 12(4): 405-415. Available from: https://www.tandfonline.com/doi/abs/10.1080/17474124.2018.1438890?journalCode=ierh20 [ Links ]
28.Ramires de Jesus G, Ramires de Jesus N, Peixoto-Filho FM, Lobato G. Caesarean rates in Brazil: what is involved? BJOG [Internet]. Apr 2015 [cited 2021 Aug 12]; 122(5): 606-609. Available from: https://obgyn.onlinelibrary.wiley.com/doi/10.1111/1471-0528.13119 [ Links ]
29.Du L, Pan WH, Cai W, Wang J, Wu YM, Shi CR. Delivery room surgery: an applicable therapeutic strategy for gastroschisis in developing countries. World J Pediatr [Internet]. Fev 2014; 10(1): 69-73. Available from: https://link.springer.com/article/10.1007%2Fs12519-014-0455-3 [ Links ]
30.O'Connell RV, Dotters-Katz SK, Kuller JA, Strauss RA. Gastroschisis: A review of management and outcomes. Obstet Gynecol Surv [Internet]. Sep 2016 [cited 2021 Aug 12]; 71(9): 537-544. Available from: https://journals.lww.com/obgynsurvey/Abstract/2016/09000/Gastroschisis__A_Review_of_Management_and_Outcomes.18.aspx [ Links ]
31.Bhatt P, Lekshminarayanan A, Donda K, Dapaah-Siakwan F, Thakkar B, Parat S, et al. Trends in incidence and outcomes of gastroschisis in the United States: analysis of the national inpatient sample 2010-2014. Pediatr Surg Int [Internet] Sep 2018 [cited 2021 Aug 12]; 34(9): 919-929. Available from: https://link.springer.com/article/10.1007%2Fs00383-018-4308-3 [ Links ]
32.Skarsgard ED. Management of gastroschisis. Curr Opin Pediatr [Internet] Jun 2016 [cited 2021 Aug 12]; 28(3): 363-369. Available from: https://journals.lww.com/co-pediatrics/Abstract/2016/06000/Management_of_gastroschisis.17.aspx [ Links ]
33.Apfeld JC, Wren SM, Macheka N, Mbuwayesango BA, Bruzoni M, Sylvester KG, et al. Infant, maternal, and geographic factors influencing gastroschisis related mortality in Zimbabwe. Surgery [Internet] Dec 2015 [cited 2021 Aug 12]; 158(6): 1475-1480. Available from: https://www.surgjournal.com/article/S0039-6060(15)00368-2/fulltext [ Links ]
34.Wesonga A, Situma M, Lakhoo K. Reducing gastroschisis mortality: a quality improvement initiative at a Ugandan pediatric surgery unit. World J Surg [Internet]. May 2020 [cited 2021 Aug 12]; 44(5): 1395-1399. Available from: https://link.springer.com/article/10.1007%2Fs00268-020-05373-w [ Links ]
35.Mota GAO, Shimizu GY, Lahoz ALC, Nicolau CM, Paula LCS, Maristela TCunha MT, Tanaka C. Motor performance evaluation of newborns with gastroschisis after surgical correction. J Hum Growth Dev [Internet]. 2021 [cited 2021 Aug 12]; 31(2): 217-223. Available from: https://revistas.marilia.unesp.br/index.php/jhgd/article/view/12225/7517 [ Links ]
36.Allin BSR, Hall NJ, Ross AR, Marven SS, Kurinczuk JJ, Knight M, et al. Development of a gastroschisis core outcome set. Arch Dis Child Fetal Neonatal Ed [Internet]. Jan 2019 [cited 2021 Aug 12]; 104(1): F76-F82. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6762000/ [ Links ]
 Correspondence:
Correspondence:
Virginia Maria Muniz
vmuniz605@gmail.com
Manuscript received: march 2021
Manuscript accepted: august 2021
Version of record online: january 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}