










Servicios Personalizados
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.1 Santo André ene./abr. 2022
http://dx.doi.org/10.36311/jhgd.v32.12616
ORIGINAL ARTICLE
doi: 10.36311/jhgd.v32.12616
Outcome Measure Epidemiological of Female Inmates in West Amazon, Brazil
Vitor Djannaro Eliamen da CostaI; Italla Maria Pinheiro BezerraII; Carlos Eduardo SiqueiraIII; Francisco Naildo Cardoso LeitãoI; Leonardo Gomes da SilvaII; Blanca Elena Guerrero DaboinI; Khalifa ElmusharafIV; Luiz Carlos de AbreuI, IV
IDesign of Studies and Scientific Writing Laboratory at the ABC ABC University Health Center, Santo André, São Paulo, Brazil
IIHigher School of Sciences of Santa Casa de Misericórdia de Vitória, ES - Brazil
IIIAssociate Professor. School for the Environment. Associate Professor in the School for the Environment (SFE) at UMass Boston
IVAdjunct Professor in Public Health at Graduate Entry Medical School. University of Limerick
ABSTRACT
INTRODUCTION: the prison system in the Brazilian state of Acre, located in the Western region of the Amazon, is a branch of the criminal justice system that has been suffering from issues such as overcrowding and growth in internal organized crime. The prevalence of these matters directly affects the resocialization of prisoners and inhibits the successful re-engineering of their social values and beliefs
OBJECTIVE: to analyze the epidemiological profile of jailed women in the State of Acre, Brazil
METHODS: in a cross-sectional descriptive study, 129 participants were recruited from female penitentiaries in the state of Acre. Conducted between August and December of 2017, data was collected through a validated questionnaire, divided into modules, using both open and closed-ended items
RESULTS: we found that most women who participated in the study were single (n = 86, 66.7%), had brown skin (n = 93, 72.1%), had children (n=102, 79.1%), resided in the state of Acre (n=117, 90.5%). The mean age of the sample was 27.69 years. Among those participants who reported having partners (n = 40, 31%), we found that half had partners who were also incarcerated (n = 20, 50%). The study results also indicate that drug trafficking (n = 86, 66.7%) was the major cause for female incarceration, followed by homicide crime (n = 16, 12.4%). Over half of the participants were in prison for the first time (n = 75, 58.1%), with a high recidivism rate observed in the total sample (n = 54, 41.9%). A majority of the participants (n = 97, 75.2%) kept in touch with members of their families and a smaller portion (n = 15, 11.6%) received conjugal visits. With regard to social activities, slightly more than half (n = 75, 58.1%) worked and the majority (n = 114, 88.4%) did not study while jailed
CONCLUSION: the difficulties associated with accessing inmate data and the lack of peer-reviewed studies on inmate health in Brazil suggests that the public policies recommended by the PNSSP and the National Policy for Comprehensive Health Care for Women should be reevaluated
Keywords: inmates, health profile, Acre
Authors summary
Why was this study done?
Considering the scarcity of research on the topic of women deprived of their freedom in the Western Amazon and the importance of these findings for public health, the researchers decided to describe the epidemiological profile of this population.
What did the researchers do and find?
A descriptive, cross-sectional study was conducted with 129 women deprived of liberty in the three female prison units in Acre. The study resulted in a predominance of single women, mothers, and an average age of 27 years. It is noteworthy that the crime of drug trafficking is the largest factor of female incarceration, followed by the crime of homicide.
What do these findings mean?
It highlights a reality unassisted by public policies, effectiveness of the actions recommended in the National Policy for Full Health Care of People Deprived of Liberty in the Prison System, and because it is an institution with restricted access, research on this topic is scarce.
INTRODUCTION
The prison system in Acre, Brazil, is a branch of the criminal justice system that has suffered from overcrowding and a growth of organized crime inside prisons, thus impeding the resocialization of inmates. This is an issue that is opposed to the intent of the Criminal Enforcement Law, which states in Article 14 that "The health care of the prisoner over the age of eighteen is preventive and curative and must include medical, pharmaceutical and dental care and it is the duty of the state to ensure this assistance"1.
Prisoners within the National Correction System are exposed to a number of health risks, exemplified by the significant prevalence of sexually transmitted diseases (STD), AIDS, tuberculosis, pneumonia, dermatitis, mental disorders, hepatitis, trauma, infectious diarrhea, hypertension, and diabetes mellitus. Taking this into consideration, the need for prisoner populations to have accessible health care is evident. This could be achieved through both the implementation of basic health care within prisons, and medium to high complexity care, with a guarantee of meeting the specific needs of female prisoners within the scope of the Unified Health System2.
In 2017, the Inter-Ministerial Decree Nº. 1 instituted the aforementioned policy by establishing the National Policy for Integral Health Care of Persons Deprived of Freedom in the Prison System (PNAISP). The PNAISP governs the objectives, guidelines, and responsibilities of the Ministry of Health, the Ministry of Justice, the states, and the Federal District represented by the Health Secretariat, the Justice Secretariat, and the municipalities1.
The PNAISP also established certain goals regarding the health of the Brazilian prison population1. These goals aim at promoting access of the persons deprived of freedom to the health care network, primarily for integral care; to ensure the autonomy of health care professionals for the integral care of persons deprived of their freedom; to improve and humanize health care in the prison system through joint actions with the health and justice sectors; to promote inter-sectoral relations with basic human rights, affirmative and social policies, and criminal justice; and to foster and strengthen social participation and control3.
The population directly affected by the PNAISP are those who are protected by the state in the provisional regime, whether sentenced or under a security protocol. Article 8 of the Inter-Ministerial Decree Nº. 1, written in January of 2014, states that "workers in criminal services and other persons who deal with persons deprived of their liberty will be involved in promotion actions and disease prevention within the framework of the PNAISP"1. Thus, apart from the people deprived of their liberty, an expanded network that assists in the health promotion and disease prevention of this population would also be involved3.
With confinement and the restriction of freedom, the process of adapting to a prison environment, and conflicts among the different actors, there is a tendency by officials to neglect health-related issues. This comes from the habit of prioritizing the problems related to security and immediate survival of security guards and prisoners4.
Additionally, the prisons and penitentiaries have become overcrowded as a result of a significant increase in the prison population. This is an important trend to consider, as the growth of the female has been higher than the male population, a trend that continued in the last four years. The rate of incarcerated women is around 37.4%, which represents an average annual growth rate of approximately 12%5.
Compared to other countries, Brazil has the world's fifth largest female population in prison; a statistic only topped by Thailand, Russia, China, and the United States. A majority (68%) of these prisoners' cases involve drug trafficking5.
Brazilian jails are a hub for social exclusion, treating unfavorably vulnerable individuals in many spaces. It's been found that women's units harbor more violations of prisoners' sexual and reproductive rights, with lack of access to specialized healthcare personnel, such as gynecologists, as one of the main violations observed6. There is hardly any possibility for victims to seek care or treatment that is offered outside of the criminal justice system7.
This study aims at describing the epidemiological profile of female inmates in Acre, Brazil, to compare with observed trends in Brazilian penitentiaries.
METHODS
This study utilized a cross-sectional, quantitative, descriptive design to ascertain the epidemiological profile of the identified female inmates. The survey was conducted between August and December of 2017. 129 out of 305 women agreed to participate in the survey. The sample and target population were recruited under the Penitentiary Administration Institute (IAPEN/AC) in the state of Acre, Brazil.
A validated semi-structured questionnaire with closed and open-ended questions was used to collect data. The questionnaire was divided into five different sections: identification, occupational and criminal history, smoking behavior, health perceptions, and reported morbidity. The researcher who led the study was an employee of the Acre prison system and duly authorized by the Institute of Penitentiary Administration, which is the government body that manages the prison system in the state of Acre.
The inclusion criteria for the study required that participants be above the age of 18, sentenced to the closed system, and had communication abilities that allowed for the administration of the survey instrument. To be excluded from the study, individuals must have been sentenced to the semi-open regime, provisional regime, or been electronically monitored.
Variables such as sociodemographic conditions and crime type were taken into account while the database was double typed in Microsoft Excel® 2016. In order to conduct the statistical analysis, the research team utilized version 24 of the software Statistical Package for the Social Sciences® (SPSS).
All research protocol was approved by the Research Ethics Committee of the University of Juazeiro do Norte (FJN) on October 31, 2016, under number 1,802,277. The study was also compliant with resolution 196/96 of the National Health Council (CNS) to safeguard the anonymity of participants. Individuals were free to participate and withdraw from the study at any time without harm. Informed consent was also obtained via a signed form from each participant before they enrolled in the study.
RESULTS
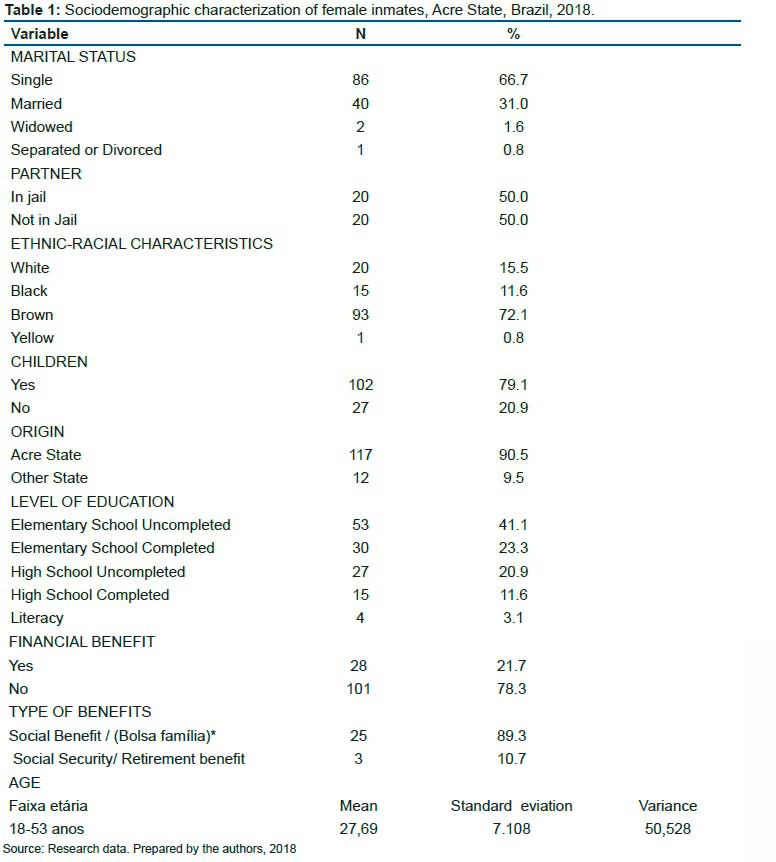
Table 1 shows that most female inmates were single (n = 86; 66.7%), had brown skin (n = 93; 72.1%) and had children (n = 102, 79.1%). A majority of them were from the state of Acre (n = 117, 90.5%), with an average age of 27.69 years. Among those who reported having a partner (n = 40; 31%), half reported that their partner (n = 20; 50%) were also in prison. Less than half of the participants did not finish elementary school and only 15 prisoners (11.6%) completed high school. The majority of the sample did not receive any social welfare benefits (n = 101; 78.3%) and of those had an income (n = 28; 21.7), most received cash transfers from the federal government program called "Bolsa Familia."
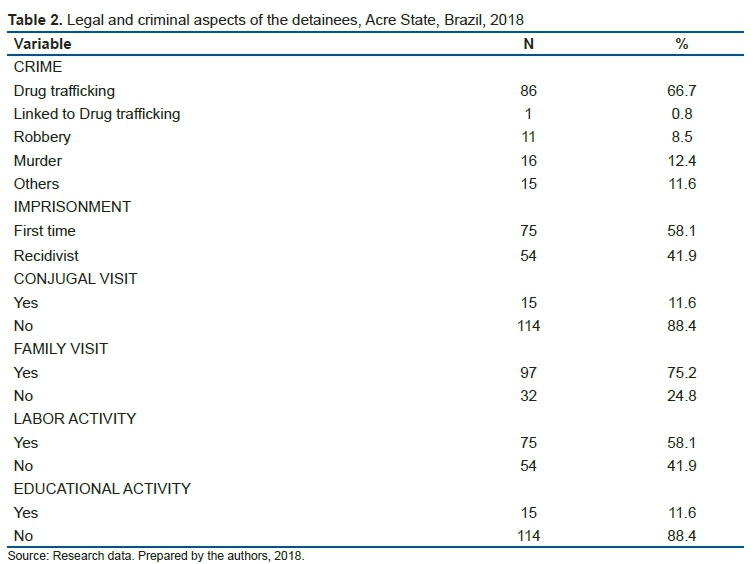
Drug trafficking (n= 86; 66.7%) was found to be the major cause of female incarceration. This can likely be attributed to the geographical location of Acre, which shares international borders with Bolivia and Peru. This border consists of forests, rivers, and streams that make it very difficult to monitor trafficking activity. Drug trafficking is followed by homicide (n = 16, 12.4%) as the leading causes of incarceration.
Slightly more than half of the female inmates reported being in prison for the first time (n = 75; 58.1%); the recidivism rate (n = 54; 41.9%) was high. The majority of the participants (n = 97, 75.2%) had contacts with their family. Conjugal visits were rare (n = 15, 11.6%) as many of the inmates were abandoned by their male partners after incarceration. Regarding re-socialization activities, just over half (n = 75, 58.1%) worked and the majority (n = 114, 88.4%) did not study while in jail.
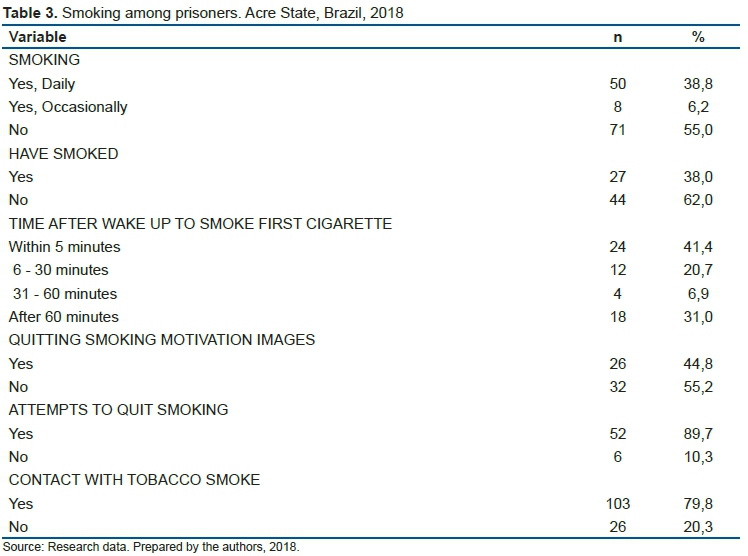
Table 3 demonstrates that more than half of the inmates did not smoke regularly. However, approximately 80% of participants reported being passive smokers. 41.4% of the smokers smoked within five minutes after waking up and 89.7% reported attempting to quit smoking. Less than half of the sample claimed that warning photos about smoking health effects encouraged them to quit.
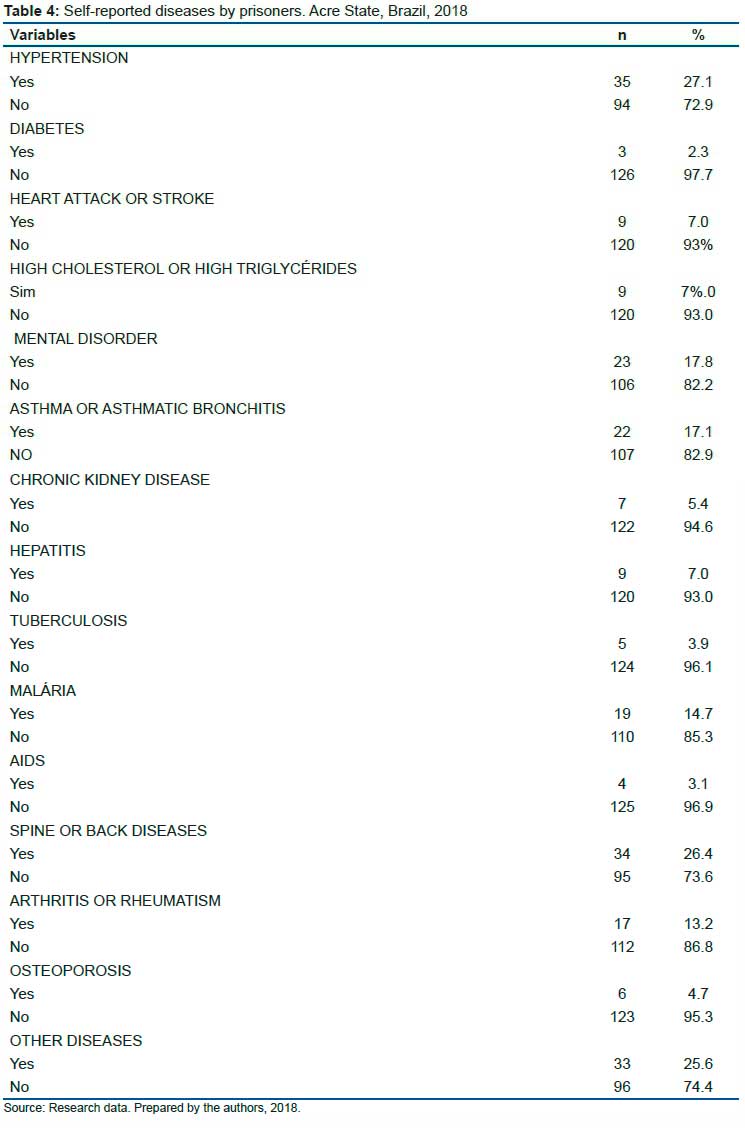
Table 4 shows that conditions such as hypertension (27.1%), mental disorders (17.8%), asthma or asthmatic bronchitis (17.1%), and spine or back diseases (26.4%) were prevalent among inmates. Other diseases were also reported, although they were not included in the questionnaire. We want to emphasize the prevalence of malaria reported by the sample (n = 19, 14.7%), given the geographical location of the state of Acre in West Amazon, which has a large number of rivers and streams.
DISCUSSION
Socio-demographic characteristics of female inmates in Acre indicate a young population, with many being single mothers. A study realized in California found results similar to those found in this study, with a similar sample. In the Californian study, authors reported that 64.5% of the participants were young, 41.3% were single, and 94.5% had children8. There were, however, dissimilar education levels between the studies. The Californian sample had 37% of its participants report finishing high school, while the Acre sample only had 11.6% of participants report similar education level.
Diniz and Paiva reported from a 2012 survey carried out in the Federal Penitentiary of the Federal District (PDF) that 51% of females interviewed were under 30 years old, 67% were black or brown, and 71% had incomplete elementary or less than first-grade elementary education. 70% were domestic or informal workers, 80% had at least one child, 52% had a partner who was also arrested, and 69% were arrested on a case-by-case basis as a result of drug trafficking. This profile indicates some important determinants of social exclusion and access to goods and services, such as health services. Regarding the crimes committed by the inmates, 66.7% of the crimes were attributed to drug trafficking. This was the highest percentage, followed by homicide (12.4%)9.
A study conducted by Oliveira et al, in the state of Paraiba found that drug trafficking crimes were committed by 28.4% of the participants, while homicide had a rate of 6.2% and was the fourth leading cause for incarceration. Although Oliveira's study found different rates for the types of crimes, both studies found drug trafficking as the most prevalent cause of incarceration. The authors also explained the reasons for the involvement of those women in crime. Most participants in that study claimed to have been primarily affected by their partner's incarceration, which influenced their choice to get involved in illicit activities as a method of supporting their families. Those drug-related offenses were what ultimately led to their imprisonment10.
Some female prisoners received financial assistance, most of which comes from the Bolsa Família Program. Our data is also supported by Oliveira et al study, which observed the same financial situation among inmates and concluded that minimal schooling, as well as a lack of employment, were contributing factors for the involvement of those inmates in criminal activities10.
While more than half of the inmates were primary offenders, there were some that were repeat offenders. This pattern was also reported by Melo and Gauer, who noticed an increase in female crime during recent decades and a high rate of recidivism in the prison system11.
As far as re-socialization is concerned, our results show that a minority of participants attended school while in the prison. However, with respect to work, more than half of the inmates were involved in some kind of work, with handicraft being the most common activity. Offering concrete opportunities for social reintegration may allow for reformative paths for the victims, although there must be a reevaluation of the recovery and re-education goals of the prison system's administration12. In our case, the prison system offered work and/or education opportunities but did not mandate inmate participation in them. This flexibility contributed to the reduced number of individuals involved in these re-socializing activities, while others reported not being able to study for lack of personal documentation.
A great prompt for re-socialization is contact with family members, which serves as motivation for the inmate to seek a return to society. During this study there was evidence of great family participation on family visit days, though some inmates did not receive family visits due to their family living a long distance away. Conjugal visits, however, were low in frequency, which confirms abandonment by the inmates' partners after incarceration. A separate but related study also found the same pattern in Italian prisons, where 85.5% of female inmates did not engage in sexual activity13.
In our study, most inmates did not smoke and many reported that they had never smoked. In two of the three female prisons where the study was conducted, smoking was prohibited and forced inmates to stop smoking. Participants that occasionally smoked explained that a cigarette would calm and relax them. However, this result differs from the Antonetti et al., study that showed high consumption rates of tobacco (87.3%) among inmates in the Italian prisons, with a daily average of 19 cigarettes smoked by participants13.
Spaulding et al, found in a meta-analysis that 60.9% of Pakistani women in prison smoked, and they noticed that women in that community constituted only 3.7% of the inmate population14.
Most participants reported that they did not consider their health as regular, good, or excellent. This trend was also observed in a separate study of 23 prisoners in Zambia, which showed that every participant reported anxiety about access to health care, while 18 (78.3%) reported being HIV positive15.
Health care service provision within the Acre prison system ensures that while the largest prison has a health unit within the building complex, the smaller ones have a nurse technician who works in the prison unit controlling the distribution of medicines and providing the first level of care. When it is required, inmates are referred to public health care services outside the prison perimeter, duly escorted by prison officers. Vaccination and health promotion campaigns are carried out by health care managers or the Institute of Penitentiary Administration (IAPEN), which works daily to guarantee all necessary care.
This situation can be compared to a study conducted by Van Hout and Mhlanga-Gunda, who established that the provision of health care for incarcerated women in sub-Saharan Africa was inadequate and failed to meet their needs, whether sexual or reproductive16. This is not in accordance with human rights requirements and international recommendations, and thus contrasts with the situation found in Acre.
In Brazil, the implementation of the National Health Plan in the Penitentiary System (PNSSP) in 2003, guaranteed the citizenship rights of the prison population, especially in areas related to health. The guidelines of the PNSSP were: to provide continuous and good quality, comprehensive care to the penitentiary population; to contribute to the control and / or reduction of frequent diseases that affect the inmate population; and to define and implement actions and services consistent with the principles and guidelines of the Unified Health System (SUS). Further, the guidelines intend to provide for the establishment of partnerships through the development of inter-sectoral actions; to contribute to the democratization of knowledge about the health/disease process; to organize services and the social production of health; to promote the recognition of health as a right of citizenship, and to stimulate the effective exercise of social participation17.
The full implementation of the principles proclaimed by the PNSSP faces certain impasses, such as funding, the difficulty of making security compatible with public health, and contracting all members of health teams in the penitentiary system. It is important to emphasize that the implementation of prison health units should meet the population criteria of one health unit for every 100 inmates. In prisons where this criterion has not been met, health services must be provided by the SUS through the networks of the Family Health Strategy Program20.
In situations where health problems are not treated or are postponed, pathologies tend to evolve, requiring complex treatments that result in higher costs, which could have been minimized if treatment was offered sooner18. Therefore, it is very important to evaluate health care services not only from the perspective of the users, but also from the providers' in order to integrate knowledge with better care to the population. Thus, specific measures are taken that reinforce the decrease in public spending19.
Canazaro and Argimon in a study of the frequency and factors associated with mental disorders in prisoners, concluded that the prevalence was significant due to experiences related to inmates' previous life and the remoteness of family members. Their data also highlighted mental disorders, which deserves special attention20.
A study in England showed that women suffered from mental and emotional problems after being deprived of their liberty, although some suffered from such problems before incarceration. However, the mental health of these women was severely impacted by the arrest. After interventions with plants at an Iowa prison in the United States, and analysis of the results, the authors suggest that interventions with elements of nature can complement traditional mental health therapies. The results from the interventions were associated with the fact that women improved their relationships while carrying out the proposed activities to contribute significantly to the prison space21.
Prisons can offer educational and disease prevention programs, focusing on mental health, substance abuse, and help to those inmates who are disadvantaged due to limited access to health care22. Access to health care is a problem, evidenced by there being only one health unit in the Acre prison system. Often, inmates must be moved to a SUS unit, which requires dedicated logistics and human resources.
In order to implement public policies in prisons aimed at providing health care for persons deprived of their freedom, it is necessary to overcome the difficulties imposed by confinement, which hinders access to health care services, especially for women who demand specialized care due to their living conditions and building environments. Many women who are incarcerated have resorted to prostitution, experienced various types of violence, and abused drugs. As a result, they carry the physical and psychological repercussions of a life exposed to multiple risk factors.
CONCLUSION
There are the difficulties in accessing inmate data and the lack of peer-reviewed studies on inmate health in Brazil suggests that public policies recommended by National Policy for Comprehensive Health Care for Women should be re-evaluated.
Acknowledgments
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. The financial viability of the article is due to the Acre - Health Project in the Western Amazon (multi-institutional agreement process no. 007/2015 SESACRE-UFAC-FMABC).
Conflicts of Interest
The authors declare that there is no conflict of interest.
REFERENCES
1.Ministério da Saúde. GABINETE DO MINISTRO PORTARIA INTERMINISTERIAL Nº 1, DE 2 DE JANEIRO DE 2014 [Internet]. Disponível em: https://central3.to.gov.br/arquivo/370304/. [ Links ]
2.Brazil, organizador. Política nacional de atenção integral à saúde da mulher: princípios e diretrizes. 1a. ed. Brasília, DF: Editora MS; 2004. 80 p. (Série C Projetos, programas e relatórios). [ Links ]
3.Pereira ÉL. Famílias de mulheres presas, promoção da saúde e acesso às políticas sociais no Distrito Federal, Brasil. Ciênc saúde coletiva. julho de 2016; 21 (7): 2123-34. [ Links ]
4.Lhuilier D, Lemiszewska A. Le choc carcéral: survivre en prison. Bayard; 2001. 309 p. [ Links ]
5.Infopen - levantamento nacional de informações penitenciárias - ministério da justiça e segurança pública [Internet]. [citado 29 de setembro de 2021]. Disponível em: http://dados.mj.gov.br/dataset/infopen-levantamento-nacional-de-informacoes-penitenciarias [ Links ]
6.Braga AGM. Dar à luz na sombra: exercício da maternidade na prisão. 2019. [ Links ]
7.Marques S. A gravidez no cárcere Brasileiro: uma análise da Penitenciária Feminina Madre Pelletier. [citado 29 de setembro de 2021]; Disponível em: http://revistaseletronicas.pucrs.br/ojs/index.php/fadir/article/download/571/401 [ Links ]
8.Kelly PJ, Peralez -Dieckmann Esther, Cheng A-L, Collins C. Profile of women in a county jail. Journal of Psychosocial Nursing and Mental Health Services. 48 (4): 38-45. [ Links ]
9.Diniz D, Paiva J. Mulheres e prisão no Distrito Federal: itinerário carcerário e precariedade da vida. Revista brasileira de ciências criminais. 2014; (111): 313-29. [ Links ]
10.Oliveira LV, Costa GMC, Medeiros KKAS, Cavalcanti AL. Perfil epidemiológico de presidiárias no estado da Paraíba-Brasil: estudo descritivo. Online braz j nurs. 19 de dezembro de 2013; 12 (4): 892-901. [ Links ]
11.Mello DC, Gauer G. Vivências da maternidade em uma prisão feminina do estado Rio Grande do Sul (Experiences of motherhood in a women's prison Rio Grande do Sul State). Saúde & Transformação Social / Health & Social Change. 31 de maio de 2011; 2 (2): 113-21. [ Links ]
12.Cunha EL da [UNESP. Ressocialização: o desafio da educação no sistema prisional feminino. Resocialization: the challenge to educate women in the detention system. 1o de agosto de 2010; 157. [ Links ]
13.The health needs of women prisoners: an Italian field survey. Disponível em: http://www.annali-iss.eu/article/view/615. [ Links ]
14.Spaulding AC, Eldridge GD, Chico CE, Morisseau N, Drobeniuc A, Fils-Aime R, et al. Smoking in correctional settings worldwide: prevalence, bans, and interventions. Epidemiologic Reviews. 1o de junho de 2018; 40 (1): 82-95. [ Links ]
15.Topp SM, Moonga CN, Mudenda C, Luo N, Kaingu M, Chileshe C, et al. Health and healthcare access among Zambia's female prisoners: a health systems analysis. Int J Equity Health. dezembro de 2016; 15 (1): 157. [ Links ]
16.Van Hout MC, Mhlanga-Gunda R. Contemporary women prisoners health experiences, unique prison health care needs and health care outcomes in sub Saharan Africa: a scoping review of extant literature. BMC Int Health Hum Rights. dezembro de 2018; 18 (1): 31. [ Links ]
17.Gois SM, Santos Junior HP de O, Silveira M de F de A, Gaudêncio MM de P. Para além das grades e punições: uma revisão sistemática sobre a saúde penitenciária. Ciênc saúde coletiva. maio de 2012; 17: 1235-46. [ Links ]
18.Saúde atrás das grades: o Plano Nacional de Saúde no sistema penitenciário nos estados de Minas Gerais e Piauí | Sumários.org [Internet]. [citado 29 de setembro de 2021]. Disponível em: https://www.sumarios.org/artigo/sa%C3%BAde-atr%C3%A1s-das-grades-o-plano-nacional-de-sa%C3%BAde-no-sistema-penitenci%C3%A1rio-nos-estados-de [ Links ]
19.Barajas-Martinez H, Hu D, Baranchuk A. Genetics bases of cardiac sodium channel mutations linked to inherited cardiac arrhythmias. J Hum Growth Dev. 28 de novembro de 2016; 26 (3): 277. [ Links ]
20.Canazaro D, Argimon II de L. Características, sintomas depressivos e fatores associados em mulheres encarceradas no Estado do Rio Grande do Sul, Brasil. Cad Saúde Pública. julho de 2010; 26: 1323-33. [ Links ]
21.Caulfield LS. Counterintuitive findings from a qualitative study of mental health in English women's prisons. IJPH. 19 de dezembro de 2016; 12 (4): 216-29. [ Links ]
22.Van den Bergh BJ, Gatherer A, Møller LF. Women's health in prison: urgent need for improvement in gender equity and social justice. Bull World Health Organ. junho de 2009; 87: 406-406. [ Links ]
 Correspondence:
Correspondence:
Vitor Djannaro Eliamen da Costa
adm.vitor@outlook.com
Manuscript received: december 2020
Manuscript accepted: may 2021
Version of record online: january 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}