










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.1 Santo André jan./abr. 2022
https://doi.org/10.36311/jhgd.v32.12969
ORIGINAL ARTICLE
doi: 10.36311/jhgd.v32.12969
Association between excess peripheral, central and general adiposity with high blood pressure in adolescents in southern Brazil
Leandro Narciso Santiago; Priscila Custódio Martins; Diego Augusto Santos Silva
Federal University of Santa Catarina, Sports Center, Research Center in Kinanthropometry and Human Performance, Florianópolis, Santa Catarina, Brazil
ABSTRACT
INTRODUCTION: Excess adiposity is one of the main risk factors for cardiovascular diseases, including high blood pressure. Children and adolescents with obesity and hypertension are at greater risk of morbidity and mortality in adulthood
OBJECTIVE: To analyze the association between excess peripheral, central and general adiposity with high blood pressure in adolescents in southern Brazil
METHODS: This is a cross-sectional study with 1,132 adolescents (16.50 ± 1.14 years) of both sexes. Measurements were performed with the oscillometric method using digital sphygmomanometer, considering high systolic and diastolic blood pressure, values above the 95th percentile for sex and age. Peripheral adiposity (triceps skinfold) and central adiposity (subscapular skinfold) were classified as high from the 90th percentile of the Centers for Disease Control and Prevention reference distribution. For excess general adiposity, triceps and subscapular skinfold above the 90th percentile were simultaneously considered. Logistic regression was used with 5% significance level
RESULTS: Male adolescents with high peripheral, central and general adiposity were, respectively, 2.43 (95% CI: 1.14; 5.19), 3.50 (95% CI: 1.66; 7.41) and 2.47 (95% CI: 1.01; 6.18) times more likely of having high SBP. Male adolescents with excess general adiposity were more likely of developing high diastolic blood pressure (OR: 3.31; 95% CI: 1.41; 7.70). Female adolescents with excess central and general adiposity were 4.15 (95% CI: 1.97; 8.77) and 3.30 (95% CI: 1.41; 7.77) times more likely of developing high diastolic blood pressure, respectively
CONCLUSION: Male adolescents with excess peripheral, central and general adiposity were more likely of having high systolic blood pressure and high diastolic blood pressure when presenting high general adiposity. In addition, female adolescents with high excess central and general adiposity were more likely of having high diastolic blood pressure
Keywords: anthropometry, cardiovascular diseases, risk factors.
Authors summary
Why was this study done?
Excess adiposity is a risk factor for chronic diseases such as obesity and systemic arterial hypertension. When initiated in the adolescence phase, the greater the chances of cardiovascular, renal and nervous system complications throughout life. Thus, it was possible to estimate the chances of high blood pressure in adolescents with excess adiposity.
What did the researchers do and find?
This school-based cross-sectional study was collected from 1.132 adolescents. Systolic and diastolic blood pressure were measured considering them normal or high. Peripheral adiposity (triceps skinfold) and central adiposity (subscapular skinfold) were classified as high starting at the 90th percentile. For excess general adiposity was verified when triceps and subscapular skinfold were above the 90th percentile simultaneously. The main findings of the present study were: male adolescents with excess peripheral, central and general adiposity had higher chances of high systolic blood pressure and higher chances of high diastolic blood pressure when they had excessively high general adiposity. Female adolescents with excess central and general adiposity are more likely to have high diastolic blood pressure.
What do these findings mean?
Overweight and obesity may be the main risk factors for high systolic and diastolic blood pressure in adolescents of both sexes. These results exposes excess adiposity and high blood pressure as public health problem among adolescents and the present research can be useful to identify risk subgroups and improve the planning of technologies aimed at combating and preventing health problems.
INTRODUCTION
From 1975 to 2016, the number of obese children and adolescents in the world increased eight times in females and 8.6 times in males and the forecast is that by 2022, there will be more obese young people than those with malnutrition1. In Brazil, the prevalence of excess weight (overweight and obesity) in adolescents increased from 6.2% between 1974 and 1985 to 25% between 2008 and 2009 in adolescents aged 10-19 years, showing an alarming scenario for this population in the country2. Weight gain during childhood and adolescence will possibly lead to excess adiposity in adulthood, increasing the risk of developing diseases such as dyslipidemia, diabetes and cardiovascular diseases such as atherosclerosis and systemic arterial hypertension during all stages of life3.
Systemic arterial hypertension is the increase in blood vessel tension levels, leading to changes in blood pressure4. As it is an asymptomatic disease in its early stages, the prevalence of SAH has been increasing worldwide5. If not controlled, systemic arterial hypertension can cause stroke, myocardial infarction, heart failure, dementia, kidney failure, presenting greater risks of morbidity and mortality in adulthood. Early diagnosis and treatment are directly associated with reducing these risks6.
Studies have shown prevalence of high blood pressure of approximately 10% in overweight adolescents in several countries between 2007 and 20137,8. In Brazil, in 2013, the prevalence of high blood pressure in adolescents with excess adiposity was 9.6%, the lowest being found in the Northern region (8.4%), and the highest in the Southern region of Brazil (12.5 %)7.
Most of these studies used body mass index (BMI) to measure excess adiposity in adolescents7,8. There is scarcity of studies using the anthropometric method of skinfolds, which enables investigating body adiposity in different body regions separately, as they have different prediction patterns. Thus, subgroups with the highest risk can be identified, contributing to the planning of interventions to prevent and treat this health problem9. Subscapular skinfold is an indicator of central adiposity and is directly associated with other health outcomes such as metabolic syndrome and cardiovascular events10. Peripheral adiposity can be verified through triceps skinfold and is directly associated with other health risk factors, such as low cardiorespiratory fitness and hyperglycemia11.
There are studies that have associated blood pressure with excess adiposity, considering excess general adiposity as the sum of both skinfolds12. However, the present study analyzed this variable when both skinfolds remain above the 90th percentile of the reference distribution for sex and age of the Centers for Disease Control and Prevention (CDC) curve11, allowing more precise inferences on the subject. Thus, the aim of the present study was to analyze the association between excess peripheral, central and general adiposity with high blood pressure in adolescents in a city in southern Brazil.
METHODS
Study design
This cross-sectional school-based study was part of the "Brazilian Guide for Assessing Physical Fitness Related to Health and Life Habits - Stage I" macroproject, approved by the Ethics Committee for Research with Humans of the Federal University of Santa Catarina under Protocol No. 746.536 and developed between August and November 2014. All participants signed the Assent Form. For adolescents aged <18 years, parents / guardians signed the Free and Informed Consent Form and adolescents aged ≥ 18 years signed the Free and Informed Consent Form themselves.
Participants
The sampling process was carried out in two stages: the first formed by school density stratification (size: small, with less than 200 students; medium, with 200-499 students; and large, with 500 or more students) and the second considering the study shift and the school grade. Eligibility was considered as to be enrolled in the state school system, to be aged 14-19 years, to be in classroom at the time of data collection and to agree to participate in the study.
To determine sample size, confidence level of 1.96 was adopted (95% confidence interval - 95% CI), tolerable error of five percentage points, prevalence of 50% and design effect of 1.5, adding 20 % for losses and refusals and another 20% to control possible confounding variables. Since 5.182 students were enrolled in high schools in the city of São José, SC in 2014, the sample size was estimated at 751 adolescents. However, due to cluster sampling, all students present were invited to participate in the survey, resulting in 1.132 students.
Dependent variable
Dependent variables were: blood pressure, systolic blood pressure and diastolic blood pressure measured by digital oscillometric method using Omron device (Kyoto, Japan) model HEM 742, validated for use with Brazilian adolescents12. After being informed about procedures, adolescents were instructed to remain at rest for five minutes, with empty bladder, without performing physical activity 90 minutes before the test and without eating, drinking alcohol or caffeine-based beverages at least 30 minutes before data collection. Two measurements with five-minute interval were performed using the average of the two measurements following protocol of the Brazilian Guidelines on Arterial Hypertension4. High blood pressure is defined when adolescents up to 18 years had systolic blood pressure / diastolic blood pressure ≥ 95th percentile according to the reference table of "The Fourth Report on the Diagnosis, Evaluation and Treatment of High Blood Pressure in Children and Adolescents"13. For adolescents aged over 18 and 19 years, high blood pressure was considered for systolic blood pressure ≥ 140 mmHg and / or diastolic blood pressure ≥ 90 mmHg.
Independent variables
Peripheral (triceps skinfold), central (subscapular skinfold) and general (triceps and subscapular skinfold) adiposity was evaluated. Triceps and subscapular skinfolds were collected using scientific Cescorf® adipometer (Porto Alegre, Brazil). Measurements were performed by evaluators certified by the International Society for the Advancement of Kinanthropometry (ISAK) using the same protocol14.
Peripheral and central adiposity was classified as high from value corresponding to the 90th percentile of the reference distribution for sex and age of the Centers for Disease Control and Prevention (CDC) curve11. Values below the 90th percentile were considered as normal adiposity. CDC curves have no reference values for general body adiposity through skinfolds. However, this study analyzed this variable according to Silva et al.15, considering with high general body adiposity adolescents who simultaneously presented skinfold thickness values in the triceps and subscapular region above the 90th percentile11.
Control variables
Sexual maturation was self-assessed according to criteria proposed by Tanner, composed of five development stages for each secondary sexual characteristic (breast and genital development)16. The indication of stages was performed by self-assessment after individual and prior explanation of the instrument by the researcher, always of the same sex as the adolescent. Students marked the number corresponding to the stage they were in relation to breast development (female sex) and genital development (male sex) after observing the corresponding photographs. Stage 1 represents the infantile stage characterized as pre-pubertal. Stages 2, 3 and 4 represent the maturation process, categorized in this study as "pubertal" and stage 5 indicates the mature adult stage, classified as "post-pubertal"16. Due to the low frequency of adolescents who declared themselves as pre-pubertal (0.2%), this variable was categorized into: "pre-pubertal / pubertal" and "post-pubertal".
The level of physical activity was verified using the Youth Risk Behavior Surveillance System (YRBSS) questionnaire developed in the United States, translated and validated for Brazil17. The following question was performed: "During the past 7 days, on how many days have you been physically active for at least 60 minutes a day? (Consider the time you spent on any type of physical activity that increased your heart rate and made your breathing faster for a while). The response options were: "No day"; "One day"; "Two days"; "Three days"; "Four days"; "Five days"; "Six days"; "Seven days". Adolescents who practiced moderate to vigorous physical activity seven days a week for 60 minutes or more were classified as "physically active" and the remaining adolescents who did not reach this recommendation were classified as "little physically active"18.
Age was collected as a discrete quantitative variable (full years) and used continuously, guaranteeing the identification of specific aspects of each age due to transformations from the adolescence phase. To define the economic level, the questionnaire proposed by the Brazilian Association of Research Companies was used, which estimates the purchasing power of families19. Economic level was characterized in a decreasing way according to the purchasing power, accumulation of material goods, housing conditions, number of domestic employees and educational level of the family head. This variable was dichotomized into "High" ("A1"; "A2"; "B1"; "B2") and "Low" ("C1"; "C2"; "D") economic level.
Statistical treatment
Analyses were performed stratified by sex. Descriptive statistics (mean, standard deviation, absolute and relative frequency) were used for sample characterization. In inferential statistics, the independent T test was used for continuous variables and the Chi-square test for categorical variables with analysis of the Cohen'D and Cramérs' effect size. Binary logistic regression was used to examine associations between outcome (blood pressure, systolic and diastolic blood pressure) and exposure (peripheral, central and general adiposity) by estimating the odds ratio (OR) and 95% confidence interval. In the adjusted analysis, all variables (age, economic level, sexual maturity, level of physical activity) were introduced into the model, regardless of p-value in the crude analysis. The significance level was set at 5%. Analyses were performed using the Statistical Package for the Social Sciences software (IBM SPSS Statistics, Chicago, United States), version 22.0.
RESULTS
Of the 1,132 students analyzed, 202 were excluded from the analysis because they did not perform anthropometric measurements, resulting in 930 students. Female adolescents had higher mean SBP values compared to male adolescents (p <0.01). Regarding skinfolds, female adolescents had higher mean triceps and subscapular skinfold values compared to male adolescents (p <0.01). Male adolescents had higher prevalence of high systolic blood pressure when compared to female adolescents (p <0.01). For the prevalence of central adiposity, no significant difference between genders was observed; however, female adolescents had higher prevalence of peripheral (p <0.04) and general (p <0.01) adiposity when compared to male adolescents (Table 1).
The crude analysis showed that male adolescents with excess peripheral (OR: 1.37; 95% CI: 1.40; 4.71), central (OR: 1.82; 95% CI: 1, 23; 2.83) and general adiposity (OR: 1.37; 95% CI: 1.04; 2.88) were more likely of having high blood pressure. In the age-adjusted analysis, male adolescents were also more likely of having high blood pressure when they had excess peripheral (OR: 1.51; 95% CI: 1.22; 4.66), central (OR: 1.81; 95% CI: 1.22; 2.93) and general adiposity (OR: 1.37; 95% CI: 1.47; 2.93). In the crude analysis, female adolescents with excess peripheral (OR: 1.02; 95% CI: 1.38; 2.75), central (OR: 1.13: 95% CI: 1.45; 2.84) and general adiposity (OR: 1.47; 95% CI: 1.54; 4.02) were more likely of having high blood pressure. In the adjusted analysis, female adolescents with excess peripheral (OR: 1.03; 95% CI: 1.37; 2.82), central (OR: 1.04; 95% CI: 1.40; 2.69) and general adiposity (OR: 1.41; 95% CI: 1.50; 3.93) were more likely of having high blood pressure (Table 2).
The crude analysis showed that male adolescents with excess peripheral adiposity were more likely of having high systolic blood pressure (OR: 2.39; 95% CI: 1.22; 4.66). In the adjusted analysis, male adolescents were 2.43 (95% CI: 1.14; 5.19) times more likely of developing high systolic blood pressure (Table 3).
Male adolescents with excess central adiposity were more likely of having high systolic blood pressure in the crude analysis (OR: 3.89; 95% CI: 2.01; 7.55) and adjusted analysis (OR: 3.51; 95% CI: 1.66; 7.41). Male adolescents with excess general adiposity were more likely of having high systolic blood pressure in the crude analysis (OR: 2.51; 95% CI: 1.12; 5.61) and adjusted analysis (OR: 2.47; 95% CI: 1.01; 6.18). Male adolescents with excess general adiposity were more likely of developing high diastolic blood pressure in the adjusted analysis (OR: 3.31; 95% CI: 1.41; 7.70) (Table 3).
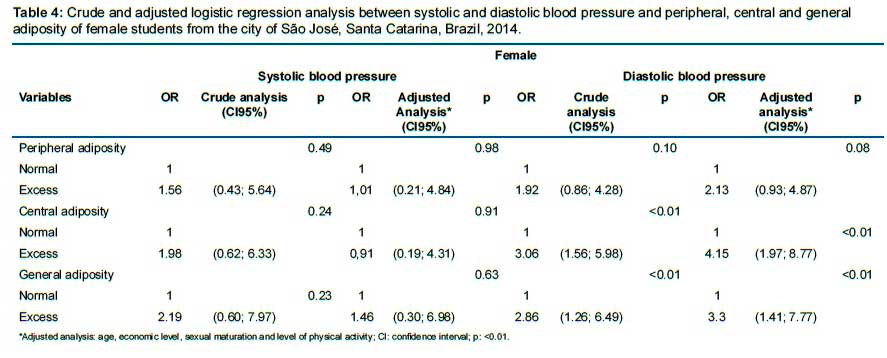
Female adolescents with excess central adiposity were more likely of having high diastolic blood pressure in the crude analysis (OR: 3.06; 95% CI: 1.56; 5.98) and adjusted analysis (OR: 4.15; 95% CI: 1.97; 8.77). Female adolescents with excess general adiposity were more likely of having high diastolic blood pressure in the crude analysis (OR: 2.86; 95% CI: 1.26; 6.49) and adjusted analysis (OR: 3.30; 95% CI: 1.41; 7.77) (Table 4).
DISCUSSION
The main findings of the present study were: 1) Male adolescents with excess peripheral, central and general adiposity were more likely of having high systolic blood pressure; 2) Male adolescents with excess general adiposity were more likely of having high diastolic blood pressure; 3) Female adolescents with excess central and general adiposity were more likely of having high diastolic blood pressure.
The research presents that, male adolescents with excess peripheral, central and general adiposity were more likely of having high systolic blood pressure. Male adolescents with excess general adiposity were more likely of having high diastolic blood pressure. These results corroborated other studies that associated males with anthropometric indicators of obesity and high blood pressure5,7. A possible explanation is related to excess central adiposity. The main physiological aspects involved are: intra-abdominal fat increases the amount of pro-inflammatory cytokines that can lead to high blood pressure; excess sympathetic activity leading to increased sodium reabsorption, causing increase in peripheral vascular resistance and consequently in blood pressure20. During sexual maturation, increased plasma testosterone levels may contribute to a pro-hypertensive effect21.
Female adolescents with excess central and general adiposity were more likely of having high diastolic blood pressure in the present study. A study conducted in the United States of America in 2008 with children aged 7-12 years, which analyzed cross-sectional associations between addition of sugar, and salt shown high consumption of sugars was associated with high DBP, as well as high fat percentage in females22. Another hypotheses is the age of the subjects, given that isolated diastolic hypertension is much more common in younger mostly in dealing of overweight adolescents23. High diastolic blood pressure levels represents a risk factor for cardiovascular disorders when high systolic blood pressure exists simultaneously though23.
Even though is already known the cause of high systolic and diastolic blood pressure is multifactorial, overweight and obesity is the mainly risk factor for this disease in adolescence, adulthood and elderly3. Body fat distribution is more important than total fat mass to determinate health hazards of excess adiposity. Other studies in southtern Brazil shown prevalence of high blood pressure and excess central adiposity in adolecents24,25. Manly excess central adiposity connotes accumulated fat intra-abdominal around and inside vital organs and its harmful to health in general. Physical activity, healthy eating habits and sufficient hours sleep seem to be the key to the prevention and treatment of risk factors such as overweight and consequently high blood pressure and cardiovascular diseases24-26.
The present study has the following limitations: blood pressure levels were measured on a single occasion. Following The Brazilian Guidelines on Arterial Hypertension recommendations, national and international studies that used two or more measures showed reductions in blood pressure levels between the first and the third measurement4. The justification may be the effect of regression to the average due to familiarization with collection procedures, reducing anxiety in the second moment7. Although systolic and diastolic blood pressure values observed in the present study are susceptible to overestimation, they are analogous to most epidemiological studies that have used the same method allowing their use as a reference of systemic arterial hypertension in adolescents.
The doubly indirect method of skinfolds is another limitation to be considered. Since there is a team of evaluators and not only one for all collections, there is possibility of systematic and random errors, underestimating or overestimating the results. The dual-energy X-ray absorptiometry (DXA) technique is shown to be accurate for estimating body fat from the entire body or segments27. A survey of American adolescents aged 11-17 compared BMI and skinfolds vs DXA and the relationship with cardiovascular risk factors, showing similar results between the two techniques (anthropometry and DXA)28. In addition, the skinfold method is validated for this type of study and is easy to apply, with relatively low operating cost compared to other techniques.
The cross-sectional characteristic of the study, which does not allow establishing cause-effect relationships, resulting in possible reverse causalities between associations. Consequently, makes impossible to confirm whether high blood pressure was before or after exposure to the excess adiposity factor.
Positive points such as data collection in different schools should be highlighted, providing greater representativeness as well as standardized procedures and training by the researcher team for data collection. In this sense, actions relevant to healthy habits during adolescence can be implemented in schools, reducing the risk of hypertension in adulthood.
CONCLUSION
It could be concluded that adolescents with excess peripheral, central and general adiposity are more likely of having high blood pressure. When presenting excess central, peripheral and general adiposity, males were more likely of having high systolic blood pressure and more likely of having high diastolic blood pressure in the presence of excess general adiposity. Female adolescents with excess central and general adiposity are more likely of having high diastolic blood pressure.
REFERENCES
1.Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. The Lancet. 2017;390(10113):2627-42. DOI: https://doi.org/10.1016/S0140-6736(17)32129-3 [ Links ]
2. Instituto Brasileiro de Geografia e Estatística (IBGE). Antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil 2008-2009. Rio de Janeiro: IBGE; 2010. [ Links ]
3. World Health Organization (WHO). Consideration of the evidence on childhood obesity for the Commission on Ending Childhood Obesity: report of the ad hoc working group on science and evidence for ending childhood obesity. Geneve: WHO; 2016. [ Links ]
4. Nobre F, Sp A, Saad CI, Sp R, Marcelo D, Giorgi A. VI Diretrizes brasileiras de hipertensão. Arq Bras Cardiol. 2010;95(1):1-51. DOI: https://doi.org/10.1590/S0066-782X2010001700001 [ Links ]
5.Ferreira JS, Aydos RD. Prevalência de hipertensão arterial em crianças e adolescentes obesos. Cien Saude Colet. 2010;15(1):97-104. DOI: https://dx.doi.org/10.1590/S1413-81232010000100015 [ Links ]
6.World Health Organization (WHO). Global status report on noncommunicable diseases 2014. Geneve: WHO; 2014. [ Links ]
7. Bloch KV, Klein CH, Szklo M, Kuschnir MCC, Abreu G de A, Barufaldi LA, et al. ERICA: prevalences of hypertension and obesity in Brazilian adolescents. Rev Saude Publica. 2016;50:9s. DOI: https://doi.org/10.1590/s01518-8787.2016050006685 [ Links ]
8. Parker ED, Sinaiko AR, Kharbanda EO, Margolis KL, Daley MF, Trower NK, et al. Change in weight status and development of hypertension. Pediatrics. 2016;137(3):e20151662. DOI: https://doi.org/10.1542/peds.2015-1662 [ Links ]
9. Duquia RP, Dumith S de C, Reichert FF, Madruga SW, Duro LN, Menezes AMB, et al. Epidemiology of elevated triciptal and subscapular skinfolds in adolescents. Cad Saude Publica. 2008;24:113-21. DOI: https://doi.org/10.1590/S0102-311X2008000100011 [ Links ]
10. Mukhopadhyay A, Bhadra M, Bose K. Regional adiposity, body composition and central body fat distribution of 10-16 years old Bengalee boys of Nimta, North 24 Parganas, West Bengal, India. Coll antropol. 2005;29(2):487-92. [ Links ]
11. Addo OY, Himes JH. Reference curves for triceps and subscapular skinfold thicknesses in US children and adolescents. Am J Clin Nutr. 2010;91(3):635-42. DOI: https://doi.org/10.3945/ajcn.2009.28385 [ Links ]
12. Christofaro DG, Fernandes RA, Gerage AM, Alves MJ, Polito MD, Oliveira AR. Validation of the Omron HEM 742 blood pressure monitoring device in adolescents. Arq Bras Cardiol. 2009;92(1):10-15. DOI: https://doi.org/10.1590/S0066-782X2009000100003 [ Links ]
13. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pedriatrics. 2004;114(2 III):555-76. [ Links ]
14. Marfell-Jones MJ, Stewart AD, Ridder JH, International standards for anthropometric assesment. Wellington: International Society for the Advancement of Kinanthropometry; 2012. [ Links ]
15. Silva DAS, Pelegrini A, de Lima e Silva JMF, Petroski EL. Epidemiology of whole body, peripheral, and central adiposity in adolescents from a Brazilian state capital. Eur J Pediatr. 2011;170(12):1541-50. DOI: https://doi.org/10.1007/s00431-011-1460-3. [ Links ]
16. Tanner JM. Growth at adolescence. Oxford: Blackwell Scientific; 1962. [ Links ]
17. Guedes DP, Lopes CC. Validation of the Brazilian version of the 2007 Youth Risk Behavior Survey 2007. Rev Saude Publica. 2010;44(5):840-50. DOI: https://doi.org/10.1590/S0034-89102010000500009. [ Links ]
18.World Health Organization. Global recommendations on physical activity for health. Geneve: World Health Organization; 2010. [ Links ]
19. Brazilian Association of Research Companies [Internet]. Brazilian Economic Classification Criterion. 2010 [cited 2020 Apr 28]. Available from: http://www.abep.org/. [ Links ]
20. Vaněčková I, Maletínská L, Behuliak M, Nagelová V, Zicha J, Kuneš J. Obesity-related hypertension: possible pathophysiological mechanisms. J endocrinol. 2014;223(3):R63-78. DOI: https://doi.org/10.1530/JOE-14-0368. [ Links ]
21. Denton KM, Hilliard LM, Tare M. Sex-Related differences in hypertension: seek and ye Shall find. Hypertension. 2013;62(4):674-77. DOI: https://doi.org/10.1161/HYPERTENSIONAHA.113.00922. [ Links ]
22. Kell KP, Cardel MI, Bohan Brown MM, Fernández JR. Added sugars in the diet are positively associated with diastolic blood pressure and triglycerides in children. Am J Clin Nutr. 2014;100(1):46-52. DOI: https://doi.org/10.3945/ajcn.113.076505. [ Links ]
23. Kannel, WB. Historic perspectives on the relative contributions of diastolic and systolic blood pressure elevation to cardiovascular risk profile. American heart jornal.1999; 138(3): S205-S210. DOI: https://doi.org/10.1016/S0002-8703(99)70311-X. [ Links ]
24. Schommer VA, Barbiero SM, Cesa CC, Oliveira R, Silva AD, Pellanda LC. Excess weight, anthropometric variables and blood pressure in schoolchildren aged 10 to 18 years. Arq Bras Cardiol. 2014; 102(4):312-8. DOI: https://doi.org/10.5935/abc.20140038. [ Links ]
25. Bergmann ML de A, Graup S, Bergmann GG. Pressão arterial elevada em adolescentes e fatores associados: um estudo de base escolar em Uruguaiana, Rio Grande do Sul, 2011. Rev Bras Saude Mater Infant. 2015;15(4):377-87. DOI: https://doi.org/10.1590/S1519-38292015000400002 [ Links ]
26. Lima TR, Sousa, GR, Castro, JA, Silva, DA. Simultaneous presence of excess weight and insufficient hours of sleep in adolescents: prevalence and related factors. Journal of Human Growth and Development.2017; 27(2):148-157.DOI: https://doi.org/10.1038/sj.ijo.0803026 [ Links ]
27. Monteiro AB, Filho JF. Análise da composição corporal: uma revisão de métodos. Ver Bras Cineantropom Desempenho Hum. 2002;4(1):80-92. [ Links ]
28. Steinberger J, Jacobs DR, Raatz S, Moran A, Hong C-P, Sinaiko AR. Comparison of body fatness measurements by BMI and skinfolds vs dual energy X-ray absorptiometry and their relation to cardiovascular risk factors in adolescents. Int J Obes. 2005;29(11):1346-52. DOI: https://doi.org/10.1038/sj.ijo.0803026 [ Links ]
 Correspondence:
Correspondence:
Diego Augusto Santos Silva
diegoaugustoss@yahoo.com.br
Manuscript received: May 2020
Manuscript accepted: May 2020
Version of record online: January 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}