










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282On-line version ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.1 Santo André Jan./Apr. 2022
http://dx.doi.org/10.36311/jhgd.v32.12675
ORIGINAL ARTICLE
doi: 10.36311/jhgd.v32.12675
Motor learning in visual impaired individuals during a coincident timing task in a non-immersive virtual reality
Mariana Caramore FavaI; Maria Georgina Marques TonelloII; Renata Martins RosaII; Tania Brusque CrocettaII; Íbis Ariana Peña de MoraesII; Carlos Bandeira de Mello MonteiroII; Talita Dias da SilvaII; Daniel dos SantosI
IPrograma de Graduação em Promoção da Saúde da Universidade de Franca, São Paulo, Brasil
IIEscola de Artes, Ciências e Humanidades da Universidade de São Paulo (EACH-USP), São Paulo, Brasil
ABSTRACT
INTRODUCTION: virtual reality (VR) is used nowadays as an assessment and intervention tool in rehabilitation. One of the skills that can be assessed through VR is coincident timing (perceptual-motor ability to execute a motor response in synchrony with an external stimulus). Visually impaired (VI) people require this synchronization of movements with external objects in their daily and leisure activities
OBJECTIVE: to investigate the performance of VI individuals in a VR coincident timing task
METHODS: sixty individuals over 18 years of age participated in this study: 20 with VI, 20 without VI but blindfolded and 20 individuals without VI that used visual feedback (without blindfold). A semi-structured interview and a virtual coincident timing task were used
RESULTS: although VI individuals started the task with the worst performance (Absolute error = VI group 945ms x blindfolded group 591ms x without blindfold group, 557ms), they improved performance throughout the task, as did the other groups, reducing the number of errors (mean absolute error= 698ms to 408ms). Furthermore, all groups presented increased task speed (mean variable error= last acquisition block 408ms x immediate transfer 227ms x late transfer 247ms
CONCLUSION: individuals with VI had difficulties at the beginning of the proposed task, but with practice they were able to adapt to the task with an improved of performance (observed by the decrease in error time). The auditory feedback was sufficient to allow adaptation to the task which improved participant performance with VI
Keywords: learning, visual disability, virtual reality.
Authors summary
Why was this study done?
Considering that Virtual reality is a possibility of intervention to individuals with disabilities. This study verified if a timing coincident non-immersive virtual task, using auditory feedback, is adaptable for people with visual impairment (VI).
What did the researchers do and find?
This study was developed in São Paulo, Brazil, with 60 participants: 20 with visual impairment that used only auditory feedback and 40 individuals without visual impairment as control group (20 blindfolded during the task and 20 without blindfold and able to use the auditory and visual feedback). A semi-structured interview and a non-immersive virtual coincident timing task were used. Although VI group started with worst performance, all groups improved with the task practice.
What do these findings mean?
Even with difficulties at the beginning of the protocol, individuals with VI adapted to the task with auditory feedback and improved their performance with practice. These findings show that the use of a non-immersive virtual reality task with auditory feedback is a possibility of intervention for individuals with VI.
INTRODUCTION
According to the World Health Organization, visual impairment (VI) is characterized by low vision or blindness and by a sensory impairment, which includes blind people and those with low vision. It is estimated that approximately 2.2 billion people have severe or moderate loss of vision, with 90% of these individuals living in developing countries1.
Tseng et al.2 states that VI affects both the daily activities and motor skills of affected individuals and, therefore, they present difficulties in practically all tasks of social participation. On the other hand, Götzelmann et al.3 mention that people with VI need to experience the environment through auditory and tactile skills, which enables them to "compensate" for the disability and have a good quality life.
Precisely to allow a person with VI to achieve more functionality in daily tasks, it is essential for studies to investigate new functional possibilities, considering the needs and specificities of the disability. One promising possibility is the use of technology through computational tasks.
Considering technological advances, Virtual Reality (VR) represents a possibility for a computational intervention in disabilities, to improve social inclusion. The use of VR in rehabilitation is a modern concept of treatment based on the use of games and tasks in virtual environments to stimulate physical and cognitive functions in people with different types of disabilities4, in which the user interacts with the environment through remote devices, such as a keyboard or mouse, or through using more advanced devices, such as a camera, glasses, and/or special gloves. VR has begun to be used as an assessment and intervention tool for people with disabilities, especially considering its good acceptance, accessibility, safety, and efficiency5.
In addition to their high level of accessibility, VR leisure activities also offer a safe and innovative way to have fun that is not limited by the weather or lack of activity partners, encouraging participation. These activities are also an effective way to practice physical exercise, helping to promote the physical health of practitioners6.
It is important to emphasize that the main feature of a virtual environment is the visual stimulus. However, people with VI, and even with complete blindness, also could experience and benefit from technological advances and adaptations in virtual tasks, especially using tactile and sound stimuli. The use of VR based on tactile and audio games is an efficient skill training strategy for people with VI because the development of navigation skills is based on alternative remaining sensory modalities, such as hearing and touch7.
Still considering the use of VR for people with VI, Lahav et al.8 and Merabet et al.9 verified benefits in spatial orientation and mobility using virtual environment simulators, whereas Morin-Parent et al.10 using sound stimuli, observed differences in reaction time. Balan, Moldoveanu and Moldoveanu7, through analysis of audio-based navigation games, stated that VR plays an important role in the development of mental structures of people with VI, as it increases learning, helps in solving problems of communication, and stimulates motivation, in addition to improving creativity, orientation, mobility, and problem-solving skills.
Considering the new technological possibilities and the need to verify whether virtual environments are adaptable for people with VI, the current work aims to evaluate the performance of people with VI during the practice of a task in a virtual environment (all participants in the experimental group performed the task blindfolded - without any visual information) and compare their performance with people without visual impairment divided into two groups: a group of people without VI who practiced the task with the visual, tactile, and sound stimuli characteristic of the virtual environment, and another group of people without VI who practiced the task blindfolded (without visual stimuli). This protocol aimed to verify if people with VI were able to use auditory stimuli to achieve the same performance as people without VI in a virtual task.
Thus, the participants practiced a motor learning protocol in a virtual coincident timing (CT) task on a computer, where a bubble falls to a target and the participant is required to press the computer keyboard at the exact moment that the bubble hits the target (the game provides visual and auditory feedback of missing and hitting the target). We opted for a CT task, as motor actions that require the performer to produce movements that coincide with an external moving object or event11, 12 are observed in various daily and sports activities11, 12.
Some studies to assess performance in a CT task in a virtual environment observed improvement in performance with practice in individuals with Down Syndrome and Cerebral Palsy13-15. However, no studies were found using CT in people with VI, and, in general, there are not many studies dedicated to understanding how the behavior of people with VI in motor tasks affects motor function16.
Considering the above deliberations, we hypothesized that all groups would present improved performance with practice, but the group of people without visual impairment (with the possibility of visualizing the task) would perform better in all protocols. We also hypothesized that the worst performance will be from the group without VI, but who practiced the task blindfolded, that is, this group should not have the benefit of visual feedback practicing a virtual task and does not have the experience of people with VI to adapt to the environment.
METHODS
Ethical and Legal Aspects of the Research
This study is duly registered in the Brazilian Registry of Clinical Trials and approved by the Research Ethics Committee under number 3,397,895.
Study Location
The study was developed at an Institution of Instruction and Work for the Blind in a city in São Paulo and at the Laboratory of Studies in Leisure, Education and Active Lifestyle for people with disabilities (ProLeva) at the University of Franca, São Paulo, Brazil.
Study Population and Eligibility Criteria
This research is characterized by a convenience sample. Twenty people with VI of both sexes participated in this study, attending an institution for people with VI. These people were invited by the coordination of the institution via telephone or in person and were selected based on the eligibility criteria, which will be described below. Even though all participants with VI were blind, they were asked to wear a blindfold when performing the task.
In addition, 40 people without disabilities were invited through social media and selected for pairing with each participant in the group with VI, that is, for each person with VI, two without VI were paired by sex and age, one directed to the blindfolded group and the other to the group unblindfolded, randomly. One participant in the control group (no VI) was allocated to the group that used the blindfold and the other to the control group that performed a task without the blindfold. Thus, among people without VI (control group), 20 wore blindfolds when participating in the study (only with auditory feedback) and 20 practiced the task with visual and auditory feedback. All participants were taken individually to a room where they performed the protocol. To carry out this study, a notebook computer and CT assessment software were used.
The criteria for participation in the research were: agreement to participate in the research; aged over 18 years; sign the Informed Consent Form; have a diagnosis of VI (in the case of participants with VI); and understand the virtual task. The criteria for non-inclusion in the study included withdrawal during the protocol and functional and cognitive disabilities that prevented performance of the virtual task.
Assessment Protocol
To characterize the sample, a semi-structured interview was used, with questions such as age, sex, time of vision loss, level of visual loss classification, profession, and previous contact with technology.
Task: Coincident timing
For the data collection, we used a software game created by the Information Systems Department at the School of Arts, Sciences and Humanities of the University of São Paulo4. This is a coincidence synchronization task based on the Bassin Anticipation Timer that aims to analyze motor learning through performance, verified by the variability of errors, such as constant error, absolute error, and variable error17-19.
The game (Figure 1) offers a coincident timing task in which the participants are instructed to "intercept" a falling virtual bubble as it reaches the target by pressing the keyboard space button on the computer (i.e., the game presents a sequence of 10 spaces until reaching the target positioned in the final space). The magnitude and direction of error of each participant in anticipating or delaying the arrival of the bubble to the target were recorded by the software in milliseconds. The objective was to evaluate the time difference between the execution of the participant's response and the arrival of the bubble at the target location and the global temporal precision and therefore the coincidence-anticipation timing ability20- 22.

Protocol
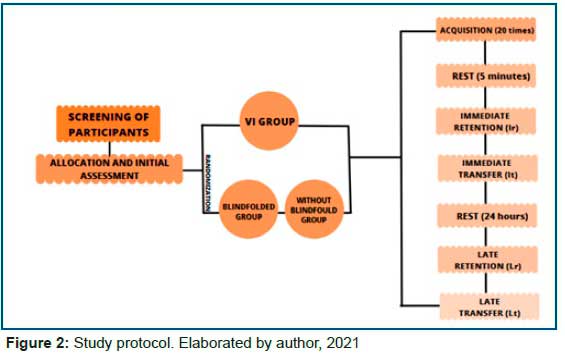
We used a motor learning protocol20, 21, 23-25 organized through blocks of 5 attempts. All participants performed two stages of the protocol. In the first stage, 30 attempts were used, divided into 20 acquisition attempts (task practice), 5 retention attempts (immediate retention - Ir), performed after 5 minutes without contact with the task, and 5 transfer attempts (immediate transfer - It), with an increase in speed. For the second stage, after 24 hours without contact with the task, the participants performed the retention (late retention - Lr) and transfer (late transfer - Lt) phases of the first stage again, totaling 10 more repetitions (Figure 2). Thus, each participant performed 40 repetitions in total.
Data analysis
The dependent variables used were timing errors: constant error (CE), absolute error (AE), and variable error (VE). Timing error was defined as the time difference between the moment the target sphere was turned on (time of arrival) and the moment the keyboard button tap was registered. The dependent variables were submitted to a MANOVA with factor 3 (Groups: with VI, without VI blindfolded, without VI and without blindfold) by 2 (Blocks) with repeated measures (RM) in the last factor (Blocks). For the Blocks factor, separate comparisons were made for acquisition (first acquisition block A1 versus final acquisition block A4), immediate and delayed retention (A4 versus immediate retention block - Ir; and A4 versus late retention block - Lr), and immediate transfer and late transfer (A4 versus immediate transfer block - It and A4 versus late transfer block - Lt). The partial eta squared (Ƞp2) was then used to calculate the effect size, where Ƞp2= 0.01 was considered a small effect, Ƞp2 = 0.06 moderate, and Ƞp2 = 0.14 large (Lakens, 2013). The observed power (op) was also reported. Post hoc comparisons were performed using the Least Significance Difference - LSD test.
To establish whether age and sex could have influenced the results, a linear regression was performed, using the difference between the last and first blocks of the acquisition phase as the dependent variable (A4 - A1). Values of p < 0.05 were considered significant. The statistical package used was the Statistical Package for the Social Sciences (SPSS; IBM, Chicago, Illinois, USA), version 26.0.
RESULTS
Sociodemographic Results
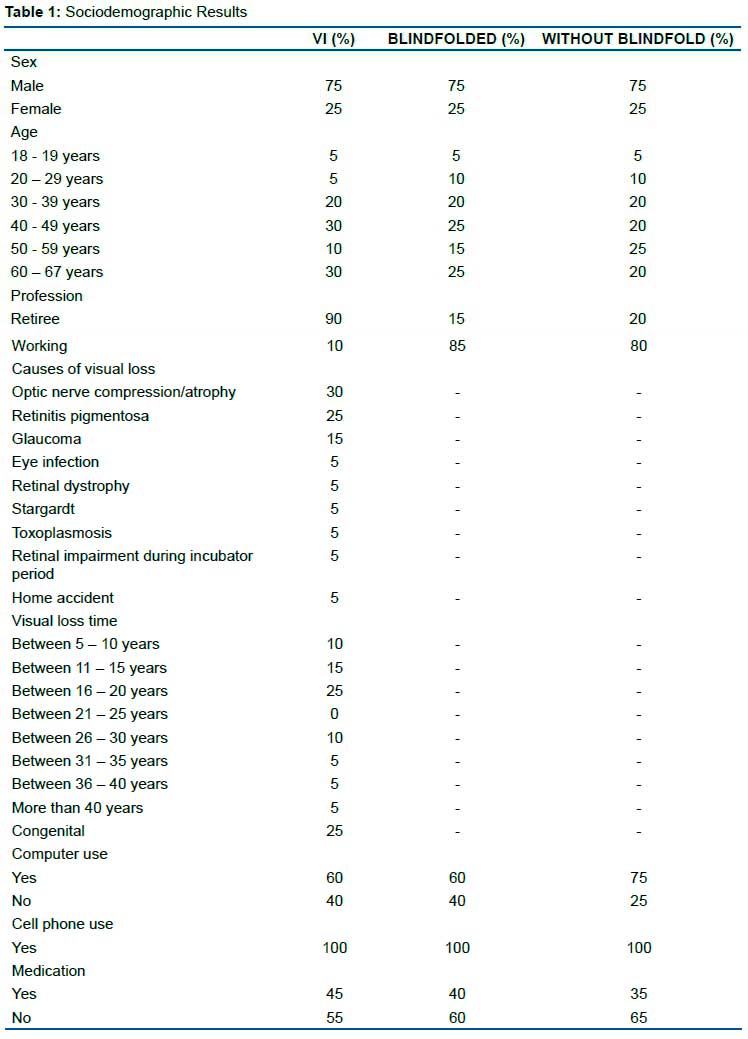
Groups were paired and there were no differences between them, regarding age and sex. Ages ranged between 18 and 67 years, and 15 men and 5 women participated in each group. The causes of visual loss ranged from: compression/atrophy of the optic nerve, eye infection, retinitis pigmentosa, retinal dystrophy, glaucoma, stargardt, toxoplasmosis, retinal impairment during incubation period, and home accident.
Data Analysis Results
Constant Error - CE
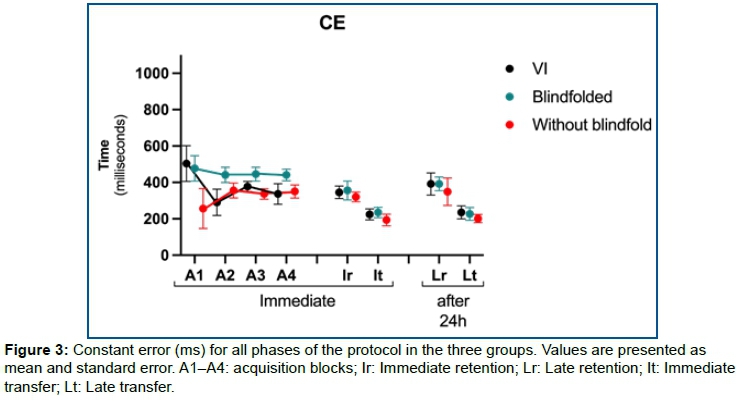
Figure 3 presents the CEs during acquisition, showing that all participants tended to anticipate movement in all phases of the protocol. There were no significant effects or interactions for Groups and Blocks.
Acquisition
MANOVA analyses revealed significant effects for Groups [Wilks' λ = 0.694, F6, 94 = 3.14, p = 0.008, Ƞp2 = 0.17, op = 0.90], Blocks [Wilks' λ = 0.410, F3, 47 = 22.5, p < 0.001, Ƞp2 = 0.59, op = 1.00], and interaction between Groups and Blocks [Wilks' λ = 0.680, F6, 94 = 3.33, p = 0.005, Ƞp2 = 0.18, op = 0.92]. The separate ANOVAs are described below:
Absolute Error - AE
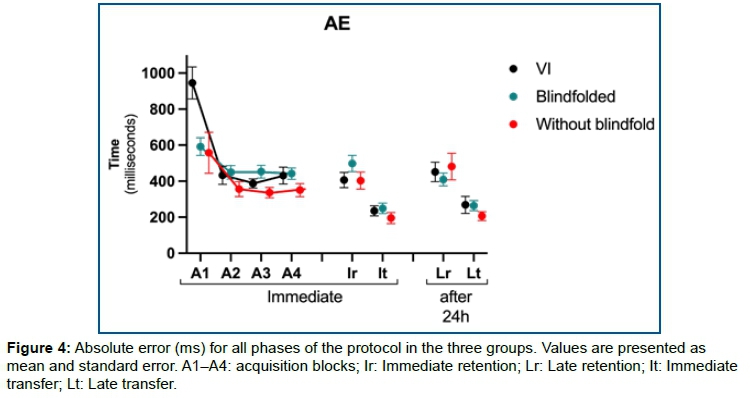
The pattern of absolute errors is illustrated in Figure 4. There was a significant effect for Groups [F2, 49 = 5.63, p = 0.006, Ƞp2 = 0.19, op = 0.83] and interaction between blocks and groups [F2, 49 = 6.70, p = 0.003, Ƞp2 = 0.22, op = 0.90]. The post-hoc test showed that the VI group had higher AE (mean = 945 ms) than the other two control groups (with blindfold - mean 591 ms, p = 0.002; and without blindfold - mean 557 ms, p = 0.003). There was no significant difference between the control groups with and without blindfold, only in the first acquisition block (A1), while in the last acquisition block there was no significant difference between the three groups.
An effect for Blocks [F1, 49 = 39,5, p <0.001, Ƞp2 = 0.45, op = 1.00] was also found. This result means that all participants decreased the EA (improved performance) from the first to the last acquisition block (mean = 698 ms to 408 ms, respectively).
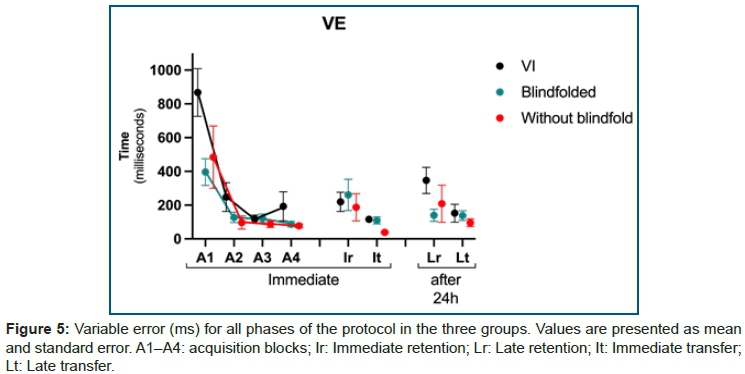
Variable Error - VE
The variable error during acquisition is illustrated in Figure 5. There was an effect for Groups [F2, 49 = 4.85, p <0.001, Ƞp2 = 0.17, op = 0.78] and although the ANOVA did not show a significant interaction, the post-hoc test demonstrated that, similar to the AE, the VI group had a higher VE (mean = 867 ms) than the other two control groups (with blindfold - mean 396 ms, p = 0.009; and without blindfold - mean 484 ms, p = 0.050), with no significant difference between the control groups with and without blindfolds. However, this result only occurred for the first acquisition block (A1), with no significant difference between the three groups in the last block (A4 ).
There was also a significant effect for Blocks [F1, 49 = 33.0, p <0.001, Ƞp2 = 0.40, op = 1.00], which showed that all participants decreased their VE from A1 (mean = 583 ms ) to A4 (average = 119 ms).
Retention
Immediate (Ir) and late (Lr - after 24h) retention
Figures 3, 4, and 5 also show the timing errors during retention. For both immediate and late retention (after 24 hours), there were no distinct differences between the errors in the final block of acquisition. Consequently, the MANOVA and ANOVAs did not reveal any significant main effect or interaction for Blocks when comparing the final acquisition block (A4) and the retention blocks (immediate retention - Ir and late retention - Lr) for constant, absolute, and variable errors, showing that the performance acquired in the last acquisition block was maintained during both retention tests.
Transfer
Immediate (It) and late (Lt - after 24h) transfer
For both immediate and late transfers, MANOVA found a significant effect for Blocks [Ti: Wilks' λ = 0.315, F3, 47 = 33.9, p <0.001, Ƞp2 = 0.69, op = 1.00; Tt: Wilks' λ = 0.284, F3, 42 = 35.3, p <0.001, Ƞp2 = 0.72, op = 1.00], with no effect for Groups or interactions. The ANOVAs will be shown separated only for the absolute errors in the next section, since the constant error presented the same anticipation pattern of the acquisition and retention phases, and no effects or interactions were found for the variable error.
Absolute Error - AE
There were significant effects for Blocks for immediate transfer [F1, 49 = 60.8, p <0.001, Ƞp2 = 0.55, op = 1.00] and late transfer [F1, 44 = 63.8 p <0.001, Ƞp2 = 0.59, op = 1.00]. These results showed that for the transfer phase with increasing speed, the participants demonstrated improved performance, that is, they decreased the AE from the last acquisition block (average = 408 ms) to the immediate transfer block (average = 227 ms) and to the late transfer block (average = 247 ms). See figures 3, 4, and 5.
Regression Analysis
It was found that age influenced the improvement in performance during the acquisition phase: the greater the improvement in performance, the younger the age [r2 = 0.14, F = 7.79, p = 0.007, beta = -8,4]. Sex did not influence performance.
DISCUSSION
The aim of the present study was to evaluate coincident timing performance through a non-immersive virtual task in people with VI. Our hypotheses that all groups would present improved performance with practice and that people without visual impairment that had visual and auditory feedback would performance better were partially confirmed.
Regarding the ability of individuals with VI to adapt to the environment using hearing3, 16, we hypothesized that the auditory feedback would provide better performance when compared to blindfolded individuals (deprived of sight at the time of the task). However, the group with the worst performance was the group of individuals with VI.
In other words, the group with VI started the task with more absolute and variable errors than the other groups. This is an interesting result, as the ability to perform all day-to-day tasks without vision did not provide any advantage for individuals with VI during a non-immersive VR task on the computer, even compared to the group without VI, but who practiced the task blindfolded.
Although the VI group showed worse performance, it is important to note that this difference appears only in the first acquisition block (i.e, at the beginning of the practice). Thus, after 5 attempts (first block) the group with VI was able to adapt to the task and had the same performance in relation to the other groups. We can only speculate that the auditory feedback generated automatically by the computer when the participant hits or misses the target was responsible for the lower performance in the first block for the DV group. Positive and negative auditory feedbacks influence task performance26 and participants in the DV group had to pay attention to identify computer feedback, which probably impaired performance during the beginning of practice.
Moreover, all groups showed a tendency to anticipate the movement and the first attempts were the farthest from ground zero, however they presented improved performance over the course of practice. We can associate this information with the characteristics of learning, which leads to improvement in a task with practice, enhancing performance27.
Another important aspect of motor learning is retention and transfer, which happens when the performance of a certain acquired motor skill can be verified at later times or in new situations or contexts28. In the retention phases (after 5 minutes without contact with the task) and transfer (with task speed increase). According to Oppici et al29, Monteiro et al20, 21 the practice is not only intended to facilitate performance, but to provide a lasting learning observable in the retention and transfer phases.
As seen before, practice is not only intended to facilitate performance, but to make it a lasting learning, hence the importance of retention and transfer29. In the case of this research, all participants maintained their performance in the retention and transfer phases, which can infer motor learning. Matins et al.25 and Monteiro et al.20 who performed a similar task in children with cerebral palsy, and Prumes et al.30, in people with muscular dystrophy, also obtained results in which the computer task with non-immersive VR proved to be a good learning tool.
Although this study is considered an initial proposal for the use of VR with VI individuals, some limitations should be presented. 1- the task used was in a non-immersive virtual environment and offered only auditory feedback to participants with VI, probably the use of a task with auditory and tactile feedback (vibration) could offer more sensory information and provide improvement with task performance; 2- the participant performance pattern could be better analyzed with a greater number of participants and, mainly, a longer task practice time (longitudinal protocol); 3- a non-immersive virtual task developed for laboratory tests was used, but most likely a game with greater possibilities and dynamic interactions could offer results that represent the daily tasks for participants.
CONCLUSION
Based on the findings, individuals with VI had difficulties at the beginning of the proposed task, but with practice they were able to adapt to the task and improve performance (observed by the decrease in error times). Thus, auditory feedback games in practice are sufficient to provide adaptation and improved performance for participants with VI.
Conflicts of Interest:
The authors declare no conflict of interest.
REFERENCES
1.World Health Organization (WHO). World report on vision. 2019. [ Links ]
2.Tseng YC, Liu SHY, Lou MF, & Huang GS. Quality of life in older adults with sensory impairments: a systematic review. Qual. Life Res. 2018;27(8):1957-1971. [ Links ]
3.Götzelmann T. Visually augmented audio-tactile graphics for visually impaired people. ACM Trans. Access. Comput. 2018;11(2):1-31. [ Links ]
4.Crocetta TB, de Araújo LV, Guarnieri R, Massetti T, Ferreira FHIB, De Abreu LC, de Mello Monteiro CB. Virtual reality software package for implementing motor learning and rehabilitation experiments. Virtual Real. 2018;22(3):199-209. [ Links ]
5.Yanovich E and Ronen O. The Use of Virtual Reality in Motor Learning: A Multiple Pilot Study Review. J. Adv. Phys. Edu. 2015;(5):188-193. [ Links ]
6.Ng YL, Ma F, Ho FK, Ip P, Fu KW. Effectiveness of virtual and augmented reality-enhanced exercise on physical activity, psychological outcomes, and physical performance: A systematic review and meta-analysis of randomized controlled trials. Comput. Hum. Behav. 2019;(99):278-291. [ Links ]
7.Balan O, Moldoveanu A, Moldoveanu F. Navigational audio games: an effective approach toward improving spatial contextual learning for blind people. Int. J. Disabil. Hum. Dev. 2015;14(2):109-118. [ Links ]
8.Lahav O, Schloerb DW, Srinivasan MA. Virtual environments for people who are visually impaired integrated into an orientation and mobility program. J. vis. impair. blind. 2015;109(1):5-16. [ Links ]
9.Merabet LB, Connors EC, Halko MA, Sánchez J. Teaching the blind to find their way by playing video games. PloS one. 2012;7(9). [ Links ]
10.Morin-Parent F, de Beaumont L, Théoret H, Lepage JF. Superior non-specific motor learning in the blind. Sci. Rep. 2017;7(1):1-6. [ Links ]
11.Bezerra IMP, Crocetta TB, Massetti T, da Silva TD, Guarnieri R, de Miranda Meira Jr C et al. Functional performance comparison between real and virtual tasks in older adults: a cross-sectional study. J. Med. 2018;97(4). [ Links ]
12.Crocetta TB, de Araújo LV, Guarnieri R, Massetti T, Ferreira FHIB, de Abreu LC et al. Virtual reality software package for implementing motor learning and rehabilitation experiments. Virtual Real. 2018;22(3):199-209. [ Links ]
13.Martins FPA, Massetti T, Crocetta TB, Lopes PB, da Silva AA, Figueiredo EF et al. Analysis of motor performance in individuals with cerebral palsy using a non-immersive virtual reality task-a pilot study. Neuropsychiatr. Dis. Treat. 2019;(15):417, 2019. [ Links ]
14.de Mello Monteiro CB, da Silva TD, de Abreu LC, Fregni F, de Araujo LV, Ferreira FHIB, Leone C. Short-term motor learning through non-immersive virtual reality task in individuals with down syndrome. BMC Neurol.2017;17(1):71. [ Links ]
15.Torriani-Pasin C, Bonuzzi GM, Soares MA, Antunes GL, Palma GC, de Mello Monteiro CB et al. Performance of Down syndrome subjects during a coincident timing task. Int. Arch. Med. 2013;6(1):1-6. [ Links ]
16.Morin-parent F, Beaumont L, Théoret H, Lepage JF. Superior non-specific motor learning in the blind. Sci Rep. 2007;6003. [ Links ]
17.Shea CH, Ashby AA. Modifications to the Bassin anticipation timer. Res Q Exerc Sport. 1981;52(2):278-280. [ Links ]
18.Williams L, Jasiewicz J, Simmons R. Coincidence timing of finger, arm, and whole-body movements. Percept Mot Skills. 2001;92(2):535-547. [ Links ]
19.Crocetta TB, Guarnieri R, Massetti T, da Silva TD, de Almeida Barbosa RT, de Lima Antão JYF et al. Concurrent validity and reliability of alternative computer game for the coincidence-anticipation timing task. Meas Phys Educ Exerc Sci, 2019. [ Links ]
20.de Mello Monteiro CB, Massetti T, da Silva TD, van der Kamp J, de Abreu LC, Leone C, Savelsbergh GJ. Transfer of motor learning from virtual to natural environments in individuals with cerebral palsy. Res Dev Disabil. 2014;35(10):2430-2437. [ Links ]
21.de Mello Monteiro CBM, Silva TD, Abreu LC, Fregni F, Araujo LV, Ferreira FHIB, Leone C. Short-term motor learning through non-immersive virtual reality task in individuals with down syndrome. Bmc Neurology. 2017; 17(1):1-8. [ Links ]
22.de Moraes IAP, de Mello Monteiro CB, Silva TDD, Massetti T, Crocetta TB, de Menezes LDC. Motor Learning and Transfer Between Real and Virtual Environments in Young People with Autism Spectrum Disorder: A Prospective Randomized Cross Over Controlled Trial. Autism Res. 2019:1-13. [ Links ]
23.Prado MTA, Fernani DCGL, da Silva TD, Smorenburg AR, de Abreu LC, de Mello Monteiro CB. Motor learning paradigm and contextual interference in manual computer tasks in individuals with cerebral palsy. Res Dev Disabil. 2017;(64):56-63. [ Links ]
24.Possebom WF, Massetti T, da Silva TD, Malheiros SRP, de Menezes LDC, Caromano FA et al. Maze computer performance in Down syndrome. J. Hum. Growth Dev. 2016;26(2):205-210. [ Links ]
25.Martins FPA, Massetti T, Crocetta TB, Lopes PB, da Silva AA, Figueiredo EF et al. Analysis of motor performance in individuals with cerebral palsy using a non-immersive virtual reality task-a pilot study. Neuropsychiatr Dis Treat. 2019;(15):417. [ Links ]
26.Mitani K and Kashino M. Auditory feedback assists post hoc error correction of temporal reproduction, and perception of self-produced time intervals in subsecond range. Front. Psychol. 2018;(8):2325. [ Links ]
27.Christiansen L, Madsen MJ, Bojsen-Møller E, Thomas R, Nielsen JB, Lundbye-Jensen J. Progressive practice promotes motor learning and repeated transient increases in corticospinal excitability across multiple days. Brain Stimul. 2018;11(2):346-357. [ Links ]
28.Sattelmayer M, Elsig S, Hilfiker R, Baer G. A systematic review and meta-analysis of selected motor learning principles in physiotherapy and medical education. BMC Medical Educ. 2016;16(1):1-22. [ Links ]
29.Oppici L, Panchuk D. Specific and general transfer of perceptual-motor skills and learning between sports: A systematic review. J Sport Exerc Psychol. 2022;(59):102-118. [ Links ]
30.Prumes M, Silva TDD, Alberissi CADO, Capelini CM, Menezes LDCD, Rocha JBFD et al. Motor learning through a non-immersive virtual task in people with limb-girdle muscular dystrophies. J. Hum. Growth Dev. 2020;30(3):461-471. [ Links ]
 Correspondence:
Correspondence:
Renata Martins Rosa
renata.martinsr@hotmail.com
Manuscript received: may 2021
Manuscript accepted: december 2021
Version of record online: january 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}