










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.2 Santo André maio/ago. 2022
http://dx.doi.org/10.36311/JHGD.V32.13365
EDITORIAL
Complexity theory in the management of patients with pain
Mauro AndreuI, II; Pablo PolicastroIII, IV; Tatiana Dias de CarvalhoI; Yolanda PardoV, VI, VII
IUniversidad Nacional De La Matanza (UNLaM), Departamento de Salud, San Justo, Buenos Aires, Argentina
IIFacultad de Ciencias de la Salud, Universidad de las Américas (UDLA), Quito, Ecuador
IIIKINÉ- Kinesiología Deportiva y Funcional, Buenos Aires, Argentina
IVUnidad de Kinesiología, Hospital Durand, Buenos Aires, Argentina
VConsorcio de Investigación Biomédica en Red, Epidemiología y Salud Pública, Barcelona, España
VIInstituto Hospital del Mar de Investigaciones Médicas, Barcelona, España
VIIUniversidad Autónoma de Barcelona, Barcelona, España
ABSTRACT
Nonlinear systems are not susceptible to being investigated with reductionist methods. In this sense, complexity theory offers an alternative approach to quantify the importance of contextual factors (CFs) in the patient with pain. The result of the positive (placebo) or negative (nocebo) use of CFs in the therapeutic setting could be responsible for a large part of a non-specific component of the efficacy of the treatment, directly affecting the quality of the results related to the patient's health (for example, pain, disability, or satisfaction). In recent years, understanding of the value of these effects has increased. Despite growing interest, knowledge, and awareness of them is currently limited and heterogeneous among health professionals, reducing their translational value in the field of health.
Keywords: complexity, contextual factors, pain, health professionals, placebo, nocebo.
Medicine is ever-changing and this conceptual and material dynamism of diseases should not be regarded merely as a bio-scientific process, but also involves a broad range of human and social experiences1. Recent studies have shown that complexity originates from the interaction between the patient's own factors and other contextual factors (CFs)2. However, like many other scientific fields, medicine is founded upon the classical Cartesian method of reductionism, where a problem is broken down into its smallest components, examined, and then the information gleaned used to draw conclusions about the nature of the larger reality3. Fundamental to this approach is the requirement that the problem being examined is a linear system3,4. When this is the case, the reductionist approach is highly successful, and the health professional can rightly feel confident in predicting the outcome of an intervention. However, frustrations arise when the problem we wish to examine is not a simple linear system but exhibits nonlinear behavior. This problem of our inability to predict the outcome in these situations gave birth to the science of complexity theory3.
Pain is a subjective experience modulated by a variety of cognitive and emotional factors, as well as by a series of sensory signals, which arise from the context surrounding the painful experience5,6. Capturing the complexity of the pain patient is one of the most challenging yet largely underexplored issues, as current health systems still focus on individual diseases and are not equipped to handle complexity7.
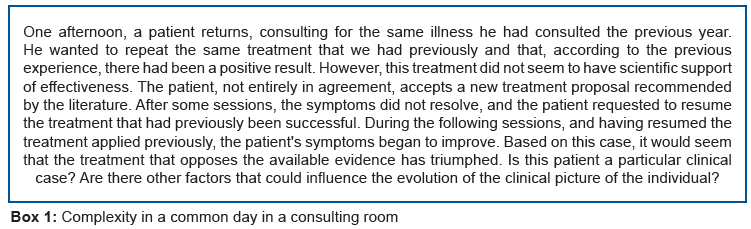
A complex system (CS) can be defined as a network of individual factors whose dynamic interaction emerges from new properties of the system itself, and where the observable results are different from the sum of their individual parts2,8. In other words, it is a collection of agents free to act in a way that is not always predictable, and whose actions are interconnected so that the actions of an agent change the context for other agents8. In this sense, the patient with pain and his/her interaction with the therapeutic environment during the professional consultation can also be considered as a CS, characterized by a high degree of biological variability, negative entropy, and emergent order. In a complex system, agents respond to their environment using a set of internalized rules that drive action. In a biochemical system, the "rules" are a series of chemical reactions. At the human level, rules can be expressed as instincts, constructions, and mental models. "Exploring the patient's previous experiences, expectations and preferences" is an example of an internalized rule that could drive the actions of a professional (Box 1)8.
Many times, we find ourselves challenged by complex situations during the approach to the pain of our patients. With the objective of solving these scenarios, we pursue and apply the recommendations of the scientific literature. However, many times the clinical evolution has outcomes that are difficult to understand. Symptoms can improve or worsen for many reasons not related to treatment9. The understanding of the characteristics of this CS can contribute to the approach of the patient from another perspective, more satisfactory for both the patient and the professional who assists him. These CSs can be better understood by analyzing their characteristics2,3,8.
The determinants of clinical evolution are a phenomenon of emerging interest among professionals and researchers. The complexity approach recognizes patients as a whole, their social, cultural and environmental context, which shapes the individual response to the disease; in essence, a patient-centered health system10. On the other hand, the CS understands health and illness as subjective and disease as objective; emergent states of top-down and bottom-up interactions between the restrictive environmental, socio-cultural, and economic-political context and the recursive physiological and psychological interactions of networks of cellular and organ functions11.
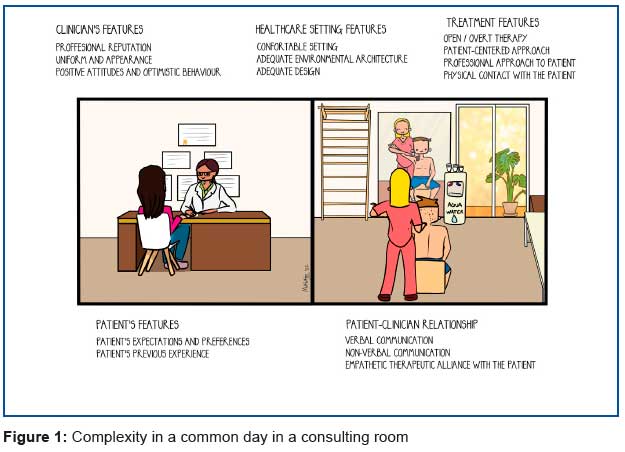
Pain is a subjective experience that cannot be solely attributed to incoming nociceptive information. In fact, pain is modulated by a variety of cognitive and emotional factors, and also by a series of sensory signals6,12. That is, the cognitive, emotional and sensory processes that affect pain arise from the context surrounding the painful experience. Contextual factors (CF) are physical, psychological and social elements involved in the clinical encounter between the patient and the professional (figure 1)13,14.
In the clinical context, the interaction between the specific component of a treatment and the surrounding CF influence the subjective therapeutic experience (for example, pain) triggering effects related to placebo or nocebo15; specifically, positive CF can improve clinical outcomes, while negative CF can amplify the patient's symptoms, preventing their recovery16. The placebo and nocebo effects incorporate complex and different phenomena in which behavioral, neurophysiological, perceptual, and cognitive changes occur during the therapeutic encounter between the professional and the patient. For example, comfortable environment (low noise, music, fragrances, temperature), proper architecture (private cabinets, modern equipment, spacious, windows), carefully planned environmental design (decorations, trims, and colors) are aspects that can affect the therapeutic result. These effects can also occur when an active and therapeutically effective treatment is administered: in fact, any treatment (active or inert) that is administered in any context of care can trigger effects related to this context. CF can be identified related to the characteristics of the professional and the patient, with the patient-professional interaction, with the characteristics of the treatment and with the treatment environment13.
Evidence-based medicine has traditionally focused on the effect of pharmacological agents, underestimating those psychological and environmental factors that contribute significantly to improving the therapeutic outcome with our patients17. For this reason, it is important to consider the approach to the patient with pain as a CS since it will offer additional therapeutic opportunities to manage pain and could be essential to improve the therapeutic efficacy of different interventions. In this approach, the Journal of Human Growth and Development (JHGD) brings to each edition discussions18-35, which can be enriched with this debate about CF and CS in different health conditions and epidemiological contexts.
It is important to reflect on the importance of CS in the therapeutic result, instead of minimizing them or labeling them exclusively as confounding factors1. From an educational perspective, complexity is still underestimated in most undergraduate and postgraduate health courses. To ensure adequate competence, knowledge, and ethical use, it should be included in the study programs.
CONCLUSION
The determinants of clinical evolution are a phenomenon of emerging interest among professionals and researchers. Interest in CFs has grown and is widely identified in the literature. To deal with complexity in pain patient care, we must abandon linear models, accept unpredictability, respect (and use) autonomy and creativity, and respond flexibly to emerging patterns and opportunities.
As long ago as 400 BC, Hippocrates wrote of how "the patient, though conscious that his condition is perilous, may recover his health simply through his contentment with the goodness of the physician". Balint added that what mattered was "not only the medicine . . . or the pills . . . but the way the doctor gave them to the patient-in fact the whole atmosphere in which the drug was given". (Di Blasi Z, et al.).
Funding
This article was part of the program entitled "Formando UNLaM" (edition 2021), which aims at awarding grants to UNLaM professors (Buenos Aires, Argentina) so they can develop and complete their post-graduate research. The grant was awarded to Mauro Andreu, the corresponding author of this article.
REFERENCES
1.Jones DS, Podolsky SH, Greene JA. The burden of disease and the changing task of medicine. N Engl J Med. 2012 Jun 21;366(25):2333-8. DOI: 10.1056/NEJMp1113569 [ Links ]
2.Corazza GR, Formagnana P, Lenti MV. Bringing complexity into clinical practice: An internistic approach. Eur J Intern Med. 2019 Mar; 61: 9-14. DOI: 10.1016/j.ejim.2018.11.009 [ Links ]
3.Tuffin R. Implications of complexity theory for clinical practice and healthcare organization. BJA Educ. 2016;16(10):349-52. DOI: 10.1093/bjaed/mkw013 [ Links ]
4.Lipsitz LA, Goldberger AL. Loss of 'complexity' and aging. Potential applications of fractals and chaos theory to senescence. JAMA. 1992 Apr 1;267(13):1806-9. [ Links ]
5.Wiech K, Ploner M, Tracey I. Neurocognitive aspects of pain perception. Trends Cogn Sci. 2008 Aug;12(8):306-13. DOI: 10.1016/j.tics.2008.05.005 [ Links ]
6.Bushnell MC, Ceko M, Low LA. Cognitive and emotional control of pain and its disruption in chronic pain. Nat Rev Neurosci. 2013 Jul;14(7):502-11. DOI: 10.1038/nrn3516 [ Links ]
7.Plsek PE, Wilson T. Complexity, leadership, and management in healthcare organisations. BMJ. 2001 Sep 29;323(7315):746-9. DOI: 10.1136/bmj.323.7315.746 [ Links ]
8.Plsek PE, Greenhalgh T. Complexity science: The challenge of complexity in health care. BMJ. 2001 Sep 15;323(7313):625-8. DOI: 10.1136/bmj.323.7313.625 [ Links ]
9.Kamper SJ. Engaging With Research: Linking Evidence With Practice. J Orthop Sports Phys Ther. 2018 Jun;48(6):512-513. DOI: 10.2519/jospt.2018.0701 [ Links ]
10.Sanders T, Foster NE, Bishop A, Ong BN. Biopsychosocial care and the physiotherapy encounter: physiotherapists' accounts of back pain consultations. BMC Musculoskelet Disord. 2013 Feb 19; 14: 65. DOI: 10.1186/1471-2474-14-65 [ Links ]
11.Sturmberg JP, Picard M, Aron DC, Bennett JM, Bircher J, de Haven MJ, Gijzel SMW, Heng HH, Marcum JA, Martin CM, Miles A, Peterson CL, Rohleder N, Walker C, Olde Rikkert MGM, Melis RJF. Health and Disease-Emergent States Resulting from Adaptive Social and Biological Network Interactions. Front Med (Lausanne). 2019 Mar 28; 6: 59. DOI: 10.3389/fmed.2019.00059 [ Links ]
12.Wiech K, Ploner M, Tracey I. Neurocognitive aspects of pain perception. Trends Cogn Sci. 2008 Aug;12(8):306-13. DOI: 10.1016/j.tics.2008.05.005 [ Links ]
13.Testa M, Rossettini G. Enhance placebo, avoid nocebo: How contextual factors affect physiotherapy outcomes. Man Ther. 2016 Aug; 24:65-74. DOI: 10.1016/j.math.2016.04.006 [ Links ]
14.Di Blasi Z, Harkness E, Ernst E, Georgiou A, Kleijnen J. Influence of context effects on health outcomes: a systematic review. Lancet. 2001 Mar 10;357(9258):757-62. DOI: 10.1016/s0140-6736(00)04169-6 [ Links ]
15.Carlino E, Frisaldi E, Benedetti F. Pain and the context. Nat Rev Rheumatol. 2014 Jun;10(6):348-55. DOI: 10.1038/nrrheum.2014.17 [ Links ]
16.Wager TD, Atlas LY. The neuroscience of placebo effects: connecting context, learning and health. Nat Rev Neurosci. 2015 Jul;16(7):403-18. DOI: 10.1038/nrn3976 [ Links ]
17.Carlino E, Benedetti F. Different contexts, different pains, different experiences. Neuroscience. 2016 Dec 3; 338: 19-26. DOI: 10.1016/j.neuroscience.2016.01.053 [ Links ]
18.Garcia-Niebla J, Pérez-Riera AR, Barbosa-Barros R, Muñoz D, Nikus K. Brugada syndrome unmasked by fever and paradoxical lower degree of dromotropic disturbance in the right ventricular outflow tract. J Hum Growth Dev. 2022;32(2):187-191. DOI: 10.36311/jhgd.v32.13319 [ Links ]
19.Zequinão MA, MedeirosP, Oliveira WA, Santos MA, Lopes LCO, Pereira B. Body dissatisfaction and bullying among underweight schoolchildren in Brazil and Portugal: a cross-cultural study. J Hum Growth Dev. 2022; 32(2):192-201. DOI: 10.36311/jhgd.v32.9943 [ Links ]
20.Zambaldi MPM, Bisi Molina MC, Martinelli KG, dos Santos-Neto ET. Children, maternal and socioeconomic characteristics influence oral hygiene habits in schoolchildren. J Hum Growth Dev. 2022; 32(2):202-213. DOI: 10.36311/jhgd.v32.13163 [ Links ]
21.Alemu YM, Gobena MG. Determinants of age at first birth among women in Ethiopia using cox proportional hazards model. J Hum Growth Dev. 2022; 32(2):214-222. DOI: 10.36311/jhgd.v32.13145 [ Links ]
22.Pontes CFR, Chamié LP, Aguiar M, Silva EJC, Leite DFB, de Carvalho Silva SAL, Figueiredo JL. Deep endometriosis: clinical and epidemiological findings of diagnosed women according to the criteria of the international deep endometriosis analysis group (IDEA) group. J Hum Growth Dev. 2022; 32(2):223-231. DOI: 10.36311/jhgd.v32.13312 [ Links ]
23.Cunha AC, Santos Neto ET, Cattafesta M, Salaroli LB. Factors associated with the leisure pratice of individuals on hemodialysis. J Hum Growth Dev. 2022; 32(2):232-241. DOI: 10.36311/jhgd.v32.13321 [ Links ]
24.Pereira RGV, Souto RP, Longo PL, Fernandes CE, Filho IC, Felizi RT, Veiga MG, de Oliveira E. Evaluation of the g473a polymorphism in the lysyl oxidase gene as a risk factor related to the occurrence of breast cancer in Brazilian women. J Hum Growth Dev. 2022; 32(2):242-247. DOI: 10.36311/jhgd.v32.13317 [ Links ]
25.Alonso BD, Niy DY, Aguiar CA, Fonseca EL, Sandall J, Diniz CSG. Measuring harm-free care in childbirth: a pilot application of the maternity safety thermometer in Brazil. J Hum Growth Dev. 2022; 32(2):248-257. DOI: 10.36311/jhgd.v32.13228 [ Links ]
26.Barcelos MRB, Lima EFA, Dalla MDB, Vargas TB, Barroso JAM, Souza MP, Barbosa CA, Primo CC. Evaluation of actions to address acquired syphilis between 2016 and 2019, in a southeast brazilian state capital city. J Hum Growth Dev. 2022; 32(2):258-267. DOI: 10.36311/jhgd.v32.12955 [ Links ]
27.Pinasco GC, de Mattos Farina EMJ, Barcellos Filho FN, Fiorotti WF, Ferreira MCM, Souza Cruz SC, Colodette AL, Loureiro LR, Comério T, Farias DCS, Lima EFA, Manhambusque KV. An interpretable machine learning model for COVID-19 screening. J Hum Growth Dev. 2022; 32(2):268-274. DOI: 10.36311/jhgd.v32.13324 [ Links ]
28.Pastori BG, Colmanetti AB, Aguiar CA. Perceptions of sex workers about the care received in the health care context. J Hum Growth Dev. 2022; 32(2):275-282. DOI: 10.36311/jhgd.v32.10856 [ Links ]
29.Lima JKT, Lima SRT, de Lima Júnior AL, Abreu ACG, Corrêa JA. Vascular accesses for hemodialysis in Ceará-Brazil. J Hum Growth Dev. 2022; 32(2):283-293. DOI: 10.36311/jhgd.v32.13318 [ Links ]
30.Barnes C, Adamson-Macedo EN. Understanding the impact of newborn touch upon mothers of hospitalized preterm neonates. J Hum Growth Dev. 2022; 32(2):294-301. DOI: 10.36311/jhgd.v32.13322 [ Links ]
31.Silva AP, Ribeiro MA, Emídio MP, Daboin BEG, Morais TC, de Oliveira Abreu CIP, Bezerra IMP, Abreu LC. COVID-19 in the municipalities of Botucatu and Serrana, São Paulo, Brazil, the effects of lethality and mortality. J Hum Growth Dev. 2022; 32(2):302-314. DOI: 10.36311/jhgd.v32.13225 [ Links ]
32.Duarte DFB, Libório JR, Cavalcante GME, de Aquino TL, Bezerra LC, Martin ALAR, Lacerda JVR, Friary V, de Paula JA. The effects of mindfulness-based interventions in COVID-19 times: a systematic review. J Hum Growth Dev. 2022; 32(1):315-326. DOI: 10.36311/jhgd.v32.13313 [ Links ]
33.Cavalcanti MPE, Siqueira E, Moraes TC, Guerrero Daboin BE, Portugal IBM, Pimentel RMM, da Silva HMR, Jacintho LC, Elmusharaf K, Abreu LC. Trends in COVID-19 lethality and mortality rates in the State of Pernambuco, Brazil: a time series analysis from april 2020 to june 2021. J Hum Growth Dev. 2022; 32(2):327-338. DOI: 10.36311/jhgd.v32.13323 [ Links ]
34.Tobar CF, Michels M, Franco SC. Self-Compassion and positive and negative affects in medical students during the COVID-19 pandemic. J Hum Growth Dev. 2022; 32(2):339-350. DOI: 10.36311/jhgd.v32.11909 [ Links ]
35.Neves SAVM, SilvaLLS, Patzina RA, Ponce CC, Cordeiro JS, Araújo AO, Lima EL, Matos IS, Furtado JJD, Pussi LV, Cavalcante EA, Silva MV. Post COVID-19 Disseminated Mucormycosis in a 55-year-old patient in Western Amazon: Case report J Hum Growth Dev. 2022; 32(2):351-356. DOI: 10.36311/jhgd.v32.13369 [ Links ]
 Correspondence:
Correspondence:
Mauro Andreu
mfandreu@gmail.com


{kind=link}
{kind=link}