










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.2 Santo André mayo/ago. 2022
http://dx.doi.org/10.36311/jhgd.v32.13319
ORIGINAL ARTICLE
Brugada syndrome unmasked by fever and paradoxical lower degree of dromotropic disturbance in the right ventricular outflow tract
Javier Garcia-NieblaI; Andrés Ricardo Pérez-RieraII; Rodrigo de Souza AbreuIII; Raimundo Barbosa-BarrosIV; Díaz MuñozV; Kjell NikusVI
IProfesor colaborador Escuela Universitaria de Enfermería. Hospital Universitario de La Candelaria en Universidad de La Laguna. Valle del Golfo Health Center, Servicio Canario de Salud, El Hierro, Spain
IILaboratório de Delineamento de Estudos e Escrita Científica. Faculdade de Medicina do ABC, Santo André, São Paulo (SP) Brasil e Disciplina de Clínica Médica, Centro Universitário Uninove, Mauá, Brasil
IIILaboratório de Delineamento de Estudos e Escrita Científica. Universidade Federal do Espírito Santo. Vitória, Espírito Santo, Brasil
IVCentro Coronário, Hospital Messejana Dr. Carlos Alberto Studart Gomes, Fortaleza, Ceará, Brasil
VServicios Sanitarios del Área de Salud de El Hierro, Valle del Golfo Health Center, Islas Canarias, Spain
VIHeart Center, Tampere University Hospital and Faculty of Medicine and Life Sciences, University of Tampere, Finland
ABSTRACT
Brugada syndrome (BrS) is an inherited clinical-electrocardiographic arrhythmic entity with an autosomal dominant genetic pattern of inheritance or de novo variant. The syndrome has low worldwide prevalence, but is endemic in Southeast Asian countries (Thailand, Philippines and Japan). The BrS is a subtle structural heart disease (SHD), and the diagnosis is only possible when the so-called type 1 Brugada ECG pattern is spontaneously present or induced for example with fever. Repolarization-depolarization disturbances in BrS patients can be caused by genetic mutations, abnormal neural crest cell migration, low expression of connexin-43 gap junction protein, or connexome disturbances. A recent autopsy study revealed increase in biventricular collagen with myocardial fibrosis when compared with control subjects although the main affected cardiac territory is the right ventricular outflow tract (RVOT). In this location, there is abnormally low expression of significant connexin-43 gap junction responsible for the electro-vectorcardiographic manifestations of terminal QRS conduction delay in the right standard precordial leads (V1-V2), high right precordial leads (V1H-V2H), as well as in the unipolar aVR lead ("the forgotten lead"). Based on their location, these leads reflect the electrical activity of the RVOT.
Keywords: Brugada syndrome, fever, dromotropic disturbance, right ventricular outflow tract.
RESUMO
A síndrome de Brugada (SBr) é uma entidade arrítmica clínico-eletrocardiográfica hereditária com padrão genético autossômico dominante de herança ou variante de novo. A síndrome tem baixa prevalência mundial, porém sendo endêmica no Sudeste Asiático (Tailândia, Filipinas e Japão). A SBr é uma doença cardíaca minimamente estrutural, sendo o diagnóstico só possível na presença do chamado padrão ECG de Brugada tipo 1 espontâneo ou induzido, por exemplo, a febre. Os distúrbios de repolarização-despolarização em pacientes com SBr podem ser causados por mutações genéticas responsáveis pela migração anormal de células da crista neural, baixa expressão "gap junctions" conexina-43 ou distúrbios do conexoma. Um estudo recente de autópsia revelou aumento do colágeno biventricular com fibrose miocárdica quando comparado aos controles, embora o principal território cardíaco afetado seja a via de saída do ventrículo direito (VSVD). Nessa área, há menor expressão da conexina-43, o que se traduz no ECG-VCG por atraso final de condução do QRS nas derivações precordiais direitas (V1-V2), precordiais direitas altas (V1H-V2H), bem como na derivação unipolar aVR ("a derivação esquecida"). Com base em sua localização, esses eletrodos refletem a atividade elétrica da VSVD.
Palavras-chave: Síndrome de Brugada; febre; distúrbio dromótropo; via de saída do ventrículo direito.
Authors summary
Why was this study done?
Because the tracings demonstrate terminal conduction delay in the right ventricular outflow tract (RVOT) during the febrile state (ECG2), confirming by the simple ECG the existence of lower gap junction expression in this area (conexin-43).
What did the researchers do and find?
We found that fever affects ventricular conduction, mainly in the RVOT, signaling a worsening of sodium entry in phase 0 of the monophasic action potential: thermo-sensitive sodium channel.
What do these findings mean?
Electrocardiographic evidence means that Brugada syndrome is an entity that preferentially affects the RVOT, confirming recent biopsy findings, as demonstrated by Nademanee et al (Koonlawee Nademanee, et al. Fibrosis, Connexin-43, and Conduction Abnormalities in the Brugada Syndrome J Am Coll Cardiol. 2015 Nov 3;66(18):1976-1986. doi: 10.1016/j.jacc.2015.08.862)
INTRODUCTION
Brugada syndrome (BrS) is a genetic disorder transmitted in an autosomal dominant pattern. Patients with the BrS have an increased risk of ventricular tachyarrhythmia/ventricular fibrillation (VF) causing syncope and/or sudden cardiac death (SCD), predominantly at rest or during sleep. The hallmark diagnostic is the type 1 Brugada ECG pattern.
Fever is a trigger for ECG changes and SCD in BrS. Patients with syncope at rest or during sleep have the highest risk.
CASE REPORT
A 77-year-old Caucasian male, former smoker with chronic obstructive pulmonary disease. Dyslipidemia was treated by statin.
He reported syncopal episodes at rest, without prodromal, since the age of 67, related to fever. He had been asymptomatic since April 2014. As his ECGs showed a type 2 Brugada pattern at the time of syncopal episodes, he was instructed to use antipyretics to keep the body temperature at ≥37ºC. Additionally, we provided a list of drugs to avoid (BrugadaDrugs.org).
Family background: The patient had no family history of syncope or SCD. He has three children, whose ECGs were negative for the type 1 Brugada pattern, also when recorded superiorly on the chest. One of his young adult sons had atrial fibrillation without structural heart disease (SHD). He underwent successful electrical cardioversion prior to anticoagulation, and subsequently presented a negative Brugada challenge test with flecainide.
Normal physical and echocardiogram.
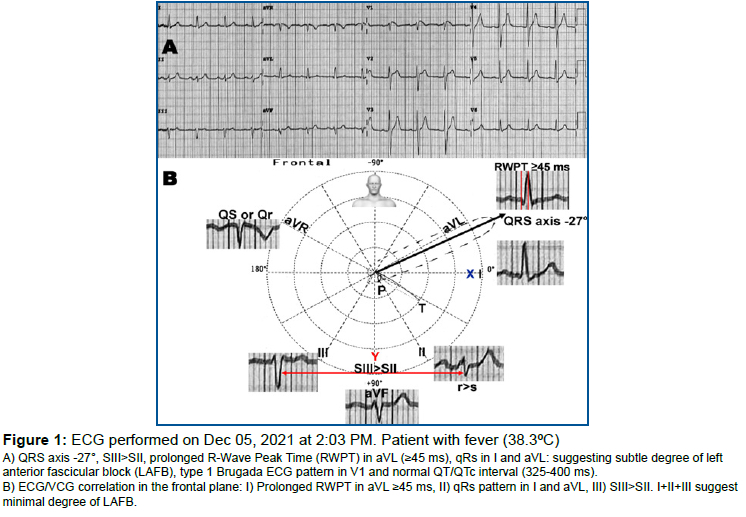
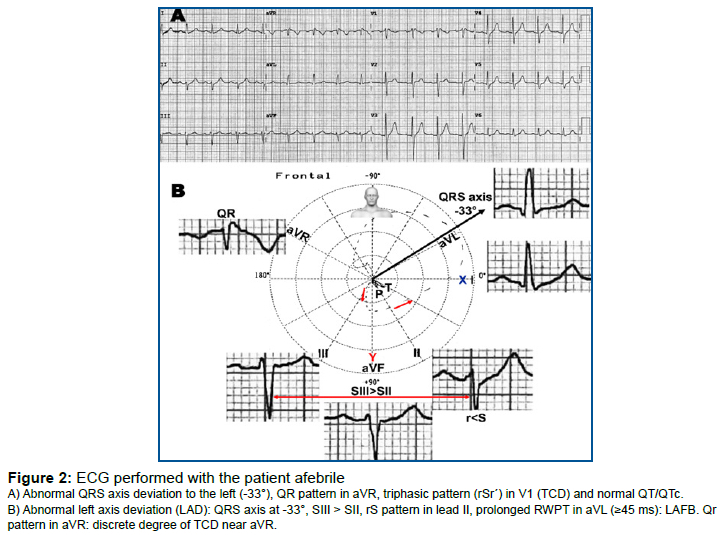
On December 5, 2021, the patient had fever and an ECG was performed (figure 1). A few hours later, when the patient was afebrile, the ECG in figure 2 was performed.
An exercise stress test, and a CT coronary angiogram were normal. We recommended genetic testing of the proband and first-degree family members.
DISCUSSION
Dumaine et al.1 hypothesized that at more physiological temperatures, the missense mutation may change the gating of the sodium channel such that the net outward current is dramatically augmented during the early phases of the right ventricular action potential. The authors tested this hypothesis by expressing Thr1620Met in a mammalian cell line, using the patch-clamp technique to study the currents at 32°C. Their results indicated that Thr1620Met current decay kinetics are faster when compared with the wild type at 32°C. Recovery from inactivation was slower for Thr1620Met at 32°C, and steady-state activation was significantly shifted. These findings explain the features of the ECG of BrS, illustrating for the first time a cardiac sodium channel mutation, in which the arrhythmogenicity is revealed only at temperatures approaching the physiological range, and suggest that some patients may be more at risk during febrile states
Then, fever is considered as a trigger of polymorphic ventricular tachycardia (PVT) and/or VF in the BrS, jointly with other factors capable of worsening the ventricular repolarization, such as: antimalarial, tricyclic antidepressants, Class Ia (ajmaline and procainamide) and Class 1c sodium channel blockers, cocaine, α-agonists, β-blockers, nitrates, cholinergic stimulation, hyperglycemia, vagal predominance, alcohol, mental stress, ischemia, hypokalemia, hypothermia and direct-current cardioversion2.
Repolarization versus depolarization hypothesis and eclectic possibility
The "repolarization" hypothesis postulates a gradient of expression of the Ito current across the RVOT myocardium, and reduced sodium current facilitates the occurrence of afterdepolarizations originating from the RVOT epicardium and of Phase 2 reentry (P2R) PVT/VF. P2R is a local arrhythmogenic phenomenon, where electrotonic current propagates from a spike-and-dome action potential (AP) region to re-excite a loss-of-dome AP region. Reduced INa may lead to the formation of an arrhythmogenic substrate due to dromotropic disturbance, but may also result in a propensity for P2R-induced premature ventricular contractions (PVCs) by decreasing the inward current available to counteract Ito. P2R is not the sole arrhythmogenic pathway in BrS and/or Ito-induced AP divergence. The dispersion in repolarization due to Ito heterogeneity in itself forms an arrhythmogenic substrate with an increased propensity for unidirectional conduction block by a closely coupled PVC, not necessarily P2R-induced.
The "depolarization" hypothesis points to slowed and delayed areas of conduction in the RVOT as the substrate for BrS arrhythmias. This latter hypothesis challenges the definition of BrS as a pure electrical heart disease, and is supported by microscopic SHD with less expression of connexin 43 gap junction and fibrotic infiltrates localized at the RVOT3-6.
Figure 3 shows the AP/ECG correlation in the repolarization versus depolarization.
We analyzed an extensive series of 140 ECGs/VCGs from BrS patients with a spontaneous or induced type 1 Brugada ECG pattern. In all cases, the ECG/VCG explored a terminal conduction delay (TCD) located in the upper right quadrant in the frontal plane, and in the right posterior quadrant in the horizontal plane7,8.
Possible explanation for the conduction delays in the present patient case
In the present case, the ECG changes seem paradoxical. In ECG # 1, recorded during fever, there is a spontaneous type 1 Brugada pattern, but only minor signs of TCD represented by a final r wave in lead aVR. On the other hand, in ECG # 2, recorded when the patient had normal body temperature, there is more evident TCD represented by a QR pattern in lead aVR despite the absence of the Brugada pattern in lead V1. In addition, there is LAFB. Consequently, we have to consider the possibility that the predominant operative mechanism stems from the repolarization hypothesis.
CONCLUSION
We present a case, where the ECG during fever showed the typical Brugada type 1 pattern, but only minor evidence of QRS TCD, while the ECG when the patient was afebrile showed more evident TCD without the type 1 Brugada pattern. We discuss possible mechanisms for the ECG manifestations of the BrS.
Conflict of interest
The authors declare no conflicts of interest.
REFERENCES
1.Dumaine R, Towbin JA, Brugada P, Vatta M, Nesterenko DV, Nesterenko VV, et al. Ionic mechanisms responsible for the electrocardiographic phenotype of the Brugada syndrome are temperature dependent. Circ Res. 1999; 85: 803-9. DOI: 10.1161/01.res.85.9.803 [ Links ]
2.Ortega-Carnicer J, Benezet J, Ceres F. Fever-induced ST-segment elevation and T-wave alternans in a patient with Brugada syndrome. Resuscitation. 2003; 57: 315-7. DOI: 10.1016/s0300-9572(03)00057-1 [ Links ]
3.Catalano O, Antonaci S, Moro G, Mussida M, Frascaroli M, Baldi M, et al. Magnetic resonance investigations in Brugada syndrome reveal unexpectedly high rate of structural abnormalities. Eur Heart J. 2009; 30: 2241-8. DOI: 10.1093/eurheartj/ehp252 [ Links ]
4.Cerrone M. Editorial commentary: Non-invasive tools for risk stratification and treatment in Brugada syndrome: Less is more? Trends Cardiovasc Med. 2021; 31: 330-1. DOI: 10.1016/j.tcm.2020.06.010 [ Links ]
5.Andrés Ricardo Pérez-Riera, Raimundo Barbosa Barros, Rodrigo Daminello-Raimundo, Luiz Carlos de Abreu, Kjell Nikus. Transient high-degree right bundle branch block masking the type 1 Brugada ECG pattern associated with possible transient early repolarization syndrome. Ann Noninvasive Electrocardiol. 2020 Jan;25(1):e12673. doi: 10.1111/anec.12673. [ Links ]
6.Andrés Ricardo Pérez-Riera, Raimundo Barbosa-Barros, Marianne Penachini da Costa de Rezende Barbosa, Rodrigo Daminello-Raimundo, Luiz Carlos de Abreu. Transient left septal and anterior fascicular block associated with type 1 electrocardiographic Brugada pattern. J Electrocardiol. Jan-Feb 2018;51(1):145-149. doi: 10.1016/j.jelectrocard.2017.07.015. [ Links ]
7.Perez-Riera AR, Barbosa-Barros R, Thomaz de Andrade A, Pontes Rodrigues R, Yanowitz F, Daminello Raimundo R, et al. Relevance of the vectorcardiogram in the Brugada syndrome with "northwest QRS axis". J Electrocardiol. 2021; 66: 125-8. DOI: 10.1016/j.jelectrocard.2021.04.009 [ Links ]
8.Perez-Riera AR, Yanowitz F, Barbosa-Barros R, Daminello-Raimundo R, de Abreu LC, Nikus K, et al. Electrocardiographic "Northwest QRS Axis" in the Brugada Syndrome: A Potential Marker to Predict Poor Outcome. JACC Case Rep. 2020; 2: 2230-4. DOI: 10.1016/j.jaccas.2020.07.037 [ Links ]
 Correspondence:
Correspondence:
Andrés Ricardo Pérez-Riera
riera@uol.com.br
Manuscript received: may 2021
Manuscript accepted: december 2021
Version of record online: june 2022


{kind=link}
{kind=link}
{kind=link}