










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282On-line version ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.2 Santo André May/Aug. 2022
http://dx.doi.org/10.36311/jhgd.v32.13163
ORIGINAL ARTICLE
Children, maternal and socioeconomic characteristics influence oral hygiene habits in schoolchildren
Maiara Paula Malacarne ZambaldiI; Maria del Camem Bisi MolinaII; Katrini Guidolini MartinelliIII; Edson Theodoro dos Santos-NetoIV
IPrograma de Pós-Graduação em Saúde Coletiva, Universidade Federal do Espírito Santo (UFES), Avenida Marechal Campos, 1468, Bonfim, Vitória, Espírito Santo, Brasil
IIPrograma de Pós-Graduação em Saúde Coletiva, Universidade Federal do Espírito Santo (UFES), Avenida Marechal Campos, 1468, Bonfim, Vitória, Espírito Santo, Brasil
IIIDepartamento de Medicina Social, Universidade Federal do Espírito Santo (UFES), Avenida Marechal Campos, 1468, Bonfim, Vitória, Espírito Santo, Brasil
IVPrograma de Pós-Graduação em Saúde Coletiva, Universidade Federal do Espírito Santo (UFES), Avenida Marechal Campos, 1468, Bonfim, Vitória, Espírito Santo, Brasil
ABSTRACT
BACKGROUNG: the prevention of dental caries is basically done by brushing and flossing the teeth. The adoption of these habits, especially in children, is a complex process that depends on factors related to different aspects of life
OBJECTIVE: to determine the association between children's, maternal and socioeconomic characteristics with oral hygiene habits in students aged 7 to 10 years in Vitória, Espírito Santo, Brazil
METHODS: cross-sectional study conducted with probabilistic sample of triple stage with final study population of 1,282 students. Data were collected using a questionnaire applied to children and questionnaire sent to parents to fill out and return. The outcome was the variable summary called "Oral Hygiene Practices" with three possible combinations: less favorable level, intermediate level and more favorable level. The independent variables were children´s, maternal and socioeconomic characteristics. The Multinomial Regression Analysis was performed between the independent variables that showed significance less or equal to 0.10 in the Bivariate Analysis and the summary variable. The significance level for the variables in the final model was p<0.05 and less favorable level was used as reference
RESULTS: most were female (58.0%), aged 8 and 9 (56.1%) and enrolled in public schools (82.8%). The most favorable oral hygiene level showed the highest prevalence (78.0%) among schoolchildren. Remained associated to more favorable level in the final model the variables: living with father and mother in the same home (OR=2,88; IC95%=1,15-7,20), dental appointment (OR=3,01; IC95%=1,32-6,85), cavity experience (OR=2,88; IC95%=1,15-7,20)) and own a toothbrush (OR=4,72; IC95%=1,43-15,66
CONCLUSION: social determinants have a strong influence on the adoption of positive habits. It is necessary for public health a more comprehensive approach to the perspective of health inequalities so that the family and social context should not be overlooked
Keywords: oral hygiene, habits, child, social determinants of health.
Authors summary
Why was this study done?
It is in childhood that the child is more likely to develop oral hygiene habits and assimilate its importance. Therefore, it is recommended to know the factors that influence the adoption of more favorable oral hygiene habits and how much these factors contribute to the acquisition of these habits.
What did the researchers do and find?
A cross-sectional school-based study was carried out with 1,282 schoolchildren aged 7 to 10 years. The oral hygiene habit was classified as less favorable, intermediate, and more favorable, according to the frequency of brushing and flossing. It was found that having their own toothbrush, having had at least one dental appointment in their lifetime, previous experience with caries, adequate birth weight and living with their father and mother were factors that contributed to the children having more healthy oral hygiene habits.
What do these findings mean?
Having contact with the dental service in early childhood is essential for the child to adopt more favorable oral hygiene habits, either through a routine consultation or due to the need caused by the experience of caries in childhood. As well as socioeconomic, maternal and child factors must be considered for the performance of professionals in the field of oral health for the adoption of more favorable oral hygiene habits
INTRODUCTION
Removal of biofilm from dental surfaces occurs mainly through brushing and flossing, which significantly contributes to the prevention of oral diseases1. Although oral hygiene methods are widely disseminated, the actual adoption of health behaviors is a very complex mechanism2. In this context, the general determinants of health related to the physical, social, political, economic and cultural environment in which individuals live become protagonists in the adoption of habits related to health care3.
Children are particularly susceptible to the conditions to which they are exposed, so that their health behaviors are constantly being shaped by the environment, past life history and personal experiences2. Therefore, some factors will contribute to the effective adoption of their oral hygiene habits, such as: individual characteristics4,5; socioeconomic factors related to family income6,7, housing conditions8, maternal education level9-11 and characteristics concerning the social support received by their family and friends5,10,12.
In Brazil, the young population is significant since in 2021 of the 213 million Brazilians, about 30 million were aged between 5 and 14 years13 and almost all of them can be found in the school environment. In addition, the school plays a fundamental role in the formation of attitudes and values by bringing together children at ages that favor the assimilation of preventive measures, such as hygiene habits that are formed in childhood14. The school environment also influences the children's socialization process, as children, when living with teachers and friends, assimilate their behavior and shape attitudes and behaviors related to their own oral health2.
The present study has as its research scenario the municipality of Vitória-Espírito Santo (ES), Brazil, which stands out among Brazilian capitals for presenting favorable socioeconomic characteristics, such as: the third largest Gross Domestic Product (GDP)15 per capita in 2019 and the best SUS Performance Index (IDSUS) in 201216. Given these considerations, the objective of this study was to verify the association between socioeconomic factors, maternal and child characteristics and the performance of oral hygiene practices in schoolchildren with 7 to 10 years.
METHODS
Study Design, Location and Period
This is a cross-sectional study, with data collected between May and December 2007, as part of the Study: "Nutrition and Health of schoolchildren aged 7 to 10 years enrolled in public and private schools in Vitória - ES, Brazil (SAUDES)9.
Study Population and Eligibility Criteria
Study participants were selected in a triple-stage probabilistic sampling process9 so that spatial coverage could generate a representative sample of the city's population, as well as a representative proportion of genders (female and male), ages (7, 8, 9 and 10 years) and education networks (public and private). Thus, the final sample consisted of 1,282 schoolchildren.
Data Collection
Data collection was performed using two instruments: the first applied to children by researchers trained to answer questions and the second sent to those responsible for self-completion. The children's form addressed issues related to feeding practices and oral health, as well as anthropometric data on the child. The questionnaire given to those responsible covered information about the child's mother, socioeconomic aspects and other variables.
In the present study, children's oral hygiene habits and their relationship with child, maternal and socioeconomic characteristics were investigated. In this way, the variables related to the frequency of daily brushing and flossing were synthesized in a summary variable called "oral hygiene practices".
To obtain the summary variable, each possible response was scored according to the "most favorable" to "least favorable" situation, so that the frequency of brushing three or more times a day was classified as +3 points, twice a day equals +2 points, once a day equals +1 point. When brushing did not occur during the day, the score considered was -1 point. Flossing was classified as: sometimes (+1 point), yes (+2 points) and no (-1 point).
For each child participating in the study, the points referring to the frequency of brushing and flossing were added together, determining three possible situations concerning oral hygiene practices: less favorable situation (score -2 and 0), intermediate situation (score 1, 2 and 3), more favorable situation (scores 4 and 5).
The independent variables used were grouped into child characteristics, maternal characteristics and socioeconomic characteristics. Child characteristics included: caries experience, sex, age, type of school, lunch companion, dinner companion, lunch location, dinner location, and birth weight. The maternal characteristics were related to the number of children; schooling; occupation of mothers of children participating in the study; and, the socioeconomic characteristics considered were: joint father and mother residence, human household agglomeration, education of the head of residence, socioeconomic class, dental appointment at least once in a lifetime and possession of the child's own toothbrush.
Data Analysis
Statistical analyzes were performed using the SPSS for Windows 17.0 program. Initially, the existence of an association between the three possible situations of the variable of oral health practices and the factors under study was investigated through exploratory bivariate analyzes with Yates' chi-square test of association. Next, the Multivariate Multinomial Regression analysis was performed between the outcome variable "Oral hygiene practices" and the independent variables that showed a significance level lower than or equal to 0.10 in the bivariate analysis, so that, for each independent variable , the odds ratio and confidence interval were obtained. The least favorable situation was used as the reference category.
The variables related to education of the head of the family and socioeconomic class were not included in the final analysis model because they are strongly associated with each other and with maternal education (p-value<0.05). However, maternal schooling functioned as an adjustment variable, as well as lunch location. The Pseudo-R2 statistic (Cox & Snell and Nagelkerke) was used to choose the best fit of the model, whose value was closer to 1. The significance level adopted for the variables in the final model was p<0.05.
Ethical and Legal Aspects of the Research
The research from which the present study originated was approved by the Research Ethics Committee of the Biomedical Center of the Federal University of Espírito Santo on 10/26/06, under registration number CEP/UFES 089/06. The performance of the study in public schools was officially authorized by the Municipal Department of Education of the Municipality of Vitória and all children participating in the research had the Free and Informed Consent Term signed by their guardians.
RESULTS
Of the 1,282 students participating in the study, most were female (58.0%), enrolled in public schools (82.8%) in the city of Vitória-ES, with a predominant age of 8 and 9 years. Most children were born with normal weight (90.8%) had someone from the family as company during lunch (73.2%) and dinner (81.7%) and had lunch (59.1%) and had dinner (59.4%) watching television. Regarding oral hygiene practices, the following frequencies were identified: 3.5% of the children had a less favorable oral hygiene practice, 15.5% had an intermediate practice and 81.0% had a more favorable oral hygiene practice. In addition, 44.4% of students reported caries experience (table 1).
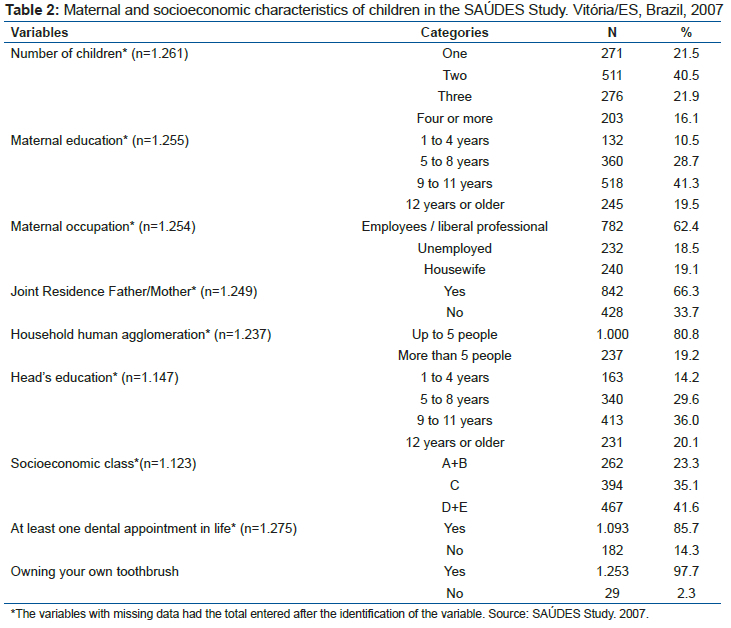
As for the characteristics of the children's mothers, the results showed that most women had studied from 9 to 11 years (41.3%), had two children (40.5%) and worked outside the home and/or were self-employed professionals. (62.4%). Regarding the socioeconomic variables of the families surveyed, there was a predominance of minors who lived with both parents in the same residence (66.3%), families with up to five inhabitants (80.8%), families belonging to the socioeconomic class D+E (41.6%) and families in which the head of household had 9 to 11 years of schooling (36.0%). In addition, 85.7% of the children had already been to the dentist at some point in their lives and 97.7% had their own toothbrush (table 2).
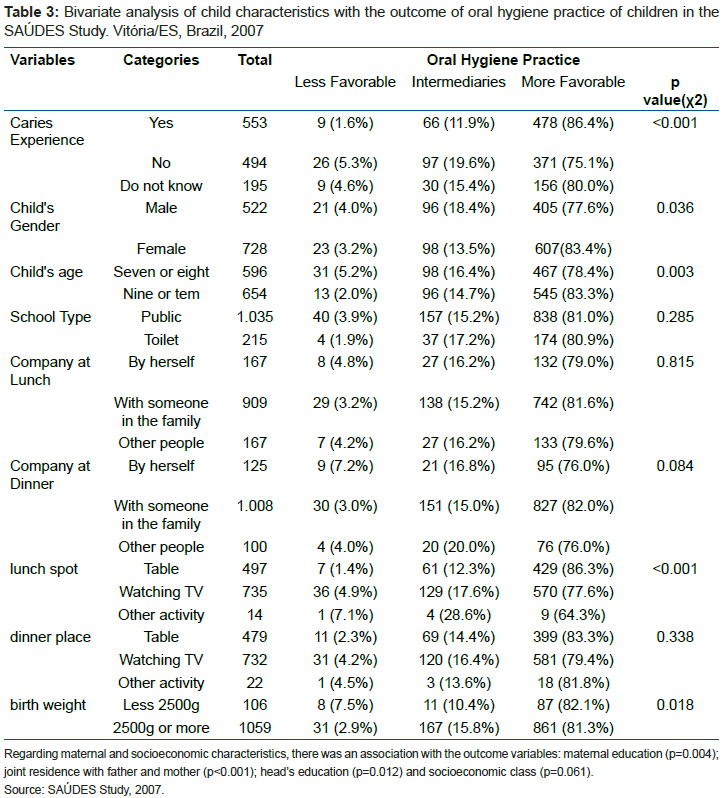
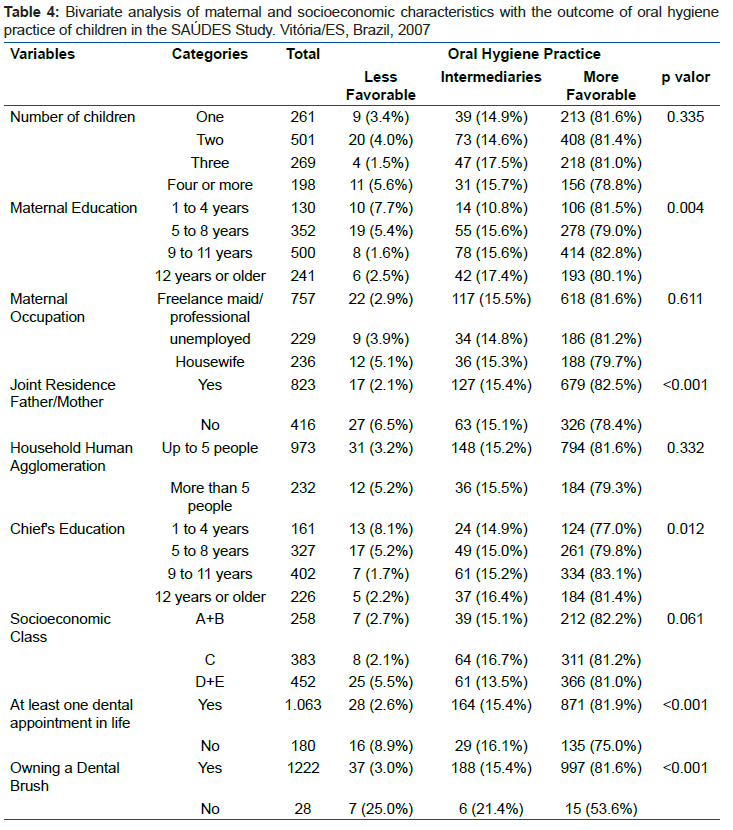
Tables 3 and 4 present the results of the bivariate analyzes related to child, maternal and socioeconomic characteristics and the three possible outcome scenarios. In these analyses, oral hygiene practices were associated, considering a significance level of 10%, with: at least one dental appointment in life (p<0.001), own toothbrush (p<0.001), caries experience (p<0.001). <0.001), sex (p=0.036), age (p=0.003), company at dinner (p=0.084), lunch location (p<0.001) and birth weight (p=0.018).
Taking oral hygiene practices at the least favorable level as a reference, the following were associated with the intermediate level: birth weight (OR=3.69; 95%CI=1.15-11.88), father and mother living together (OR=3.09; 95%CI=1.29-7.43) and at least one dental appointment in life (OR=2.52; 95%CI=1.02-6.27). However, at the most favorable level, two other variables were significantly associated in the final model: caries experience (OR=2.88; 95% CI=1.15-7.20) and owning a toothbrush (OR=4 .72; 95% CI=1.43-15.66), in addition to the variables: joint father and mother residence (OR=2.87; 95% CI=1.26-6.53) and at least one dental appointment in their lifetime (OR=3.01; 95% CI=1.32-6.85), according to table 5.
DISCUSSION
The adoption of positive behaviors by individuals regarding their oral health is influenced by a series of external factors, such as: socioeconomic level, income, education17, housing and housing conditions18, and mainly by their individual characteristics19. Health is, therefore, the result of different modes of social organization20.
The variable possession of own toothbrush was associated, with the outcome at the most favorable level, since children who had a toothbrush had almost five times the chance of having a more favorable oral hygiene practice, in relation to a less favorable practice, than those children who did not have a toothbrush or shared it at home. It should be understood that access to the toothbrush tool is the initial presupposition for the incorporation of oral hygiene habits by the child21, but not the only one.
Considering that in childhood, parents and family are the most important influence on the development and formation of oral health habits by children2,22,23, this study also investigated aspects concerning the family environment in which the child was inserted. Regarding family aspects, the results showed a positive association between the fact that the child lives in the same house with the father and mother and oral hygiene practices at an intermediate and more favorable level, when considering the less favorable situation as a reference. Thus, schoolchildren who lived with their father and mother in the same house were about three times more likely to have an intermediate or more favorable oral hygiene practice than those children who did not have a joint residence with both parents. Based on this scientific evidence, the importance of family structure in children's health behaviors is contacted and that parents together are the main responsible for teaching oral health to minors24,25.
Similarly, other investigations have shown results similar to those found in the present study, by pointing to an association between the habits and lifestyle of families and the frequency of brushing by children. Maes et al.26 showed that in children and adolescents aged 11 to 15 years, those who lived with both parents in the same household were more likely to brush their teeth more than once a day compared to those who lived with only one parent. responsible.
In another study, carried out by Levin et al 5, with children aged 11 to 15 years, the chance of brushing their teeth twice a day was lower among those who lived with only one parent compared to those who lived with both. In a survey conducted in 32 countries around the world, with parents of children aged 3 and 4 years old, it was observed that when parents encourage children to brush at least twice a day, this is essential for the habit to be acquired and perpetuated. by minors26,27.
In addition to the influence that parents have on the frequency of oral hygiene practices of their children, it is also observed that families of divorced/separated parents face situations that can negatively influence the physical health of their members28. The decrease in the economic resources available to meet family needs, low levels of social support and changes in routine resulting from family restructuring can weaken the quality of physical health of minors28, since poor family cohesion is directly related to a greater chance of low frequency of daily brushing by children and adolescents11. Thus, it can be inferred that the adoption of more favorable oral hygiene habits depends on the favorable family environment and that parents have a decisive influence on the oral health of their children.
Regarding the characteristics of those responsible for the minors, maternal schooling was not significantly associated with the practice of oral hygiene at a more favorable level, contrary to some studies6,29,30. However, this finding corroborates the study by Casanova-Rosado et al.4 in which maternal and paternal education levels were not different between the high and low brushing frequency groups. However, in order to represent socioeconomic variables: education of the head and social class, it was inserted as an adjustment variable in the final model.
It should be considered that, despite the knowledge acquired through schooling, it allows greater access to health information, by allowing individuals to make more positive decisions about health care and to perpetuate care in their family environment31. In addition, the teaching of oral hygiene methods is widespread in society, especially in the school environment, which can contribute to reducing the inequalities of information that the different levels of education provide. The Brazilian government's Programa Saúde na Escola (PSE) can be cited as an example. It has been instituted in the municipalities since 2007, with the purpose of promoting the general and oral health of students in public education institutions. Among the actions concerning oral health are: oral health education, supervised brushing and topical application of fluor32. In the specific case of Vitória-ES, where the present study was conducted, health actions in schools have been carried out systematically, even before the launch of this policy.
The association of oral hygiene practices with the use of dental services has also been reported by different scientific studies17,33. In this study, a dental appointment performed at least once in a lifetime was significantly associated with the variable "oral hygiene practices", demonstrating that those who had a dental appointment have approximately three times the chance of having a more favorable oral hygiene practice than those children who have never been to the dentist.
These findings corroborate the research conducted by Casanova-Rosado et al.4, whose results showed a higher probability (37%) of brushing their teeth, at least once a day, in children who had already been to the dentist. Similarly, other studies30,17 have reported a higher frequency of daily brushing in groups that use dental services more frequently. The association of dental consultation with a more favorable oral hygiene practice may occur due to more constant guidance by a trained professional on the importance of hygiene habits in maintaining oral health, encouraging the child to brush and use wire more often. In addition, the consultation seems to stimulate oral hygiene when compared to the less favorable level. The scientific literature reports that children develop a greater ability to incorporate care taught by a qualified professional4.
Low birth weight (<2500g) was also significantly associated with intermediate level of oral hygiene practice. Children with low birth weight have an increased risk of cerebral palsy, seizures, severe mental retardation, respiratory tract infections, among other risks34. In the oral cavity, there may also be alterations related to defects in dental enamel, alteration in the chronology of tooth eruption and predisposition to dental caries lesions in the primary dentition, in addition to dysfunctions in the craniofacial complex that can cause palate deviation35.
In view of the related complications, the results found may be due to the association between psychosocial aspects and the adoption of positive habits related to oral health. The study by Davlogio et al.10 showed that those adolescents who did not feel discriminated against and were accepted by their social group brushed their teeth more frequently. In another study conducted by Koerber et al.12 those children who did not have problems with their physical appearance also adopted more favorable oral hygiene habits.
Among the oral diseases, dental caries is the main disease that affects the oral cavity. In this sense, the removal of biofilm from the dental surface through brushing by schoolchildren contributes significantly to its prevention1. The results of the present study showed an association between the positive caries experience and the most favorable level of oral hygiene practice, contrary to some studies4,36,37 that described a positive association between a higher frequency of brushing and flossing and a lower incidence of caries . However, the studies presented4,36,37 consider the frequency of brushing limited to once or twice a day, without considering the use of dental floss. In this study, the assessment of the levels of oral hygiene practices was more rigorous, because the frequency of brushing, at the most favorable level, for example, considered the child brushing twice or more times a day, linked to the use of the toothbrush. floss sporadically or frequently. This may explain the apparent contradiction between the present study and the scientific literature consulted.
In addition, previous caries experience can have a positive influence by encouraging the adoption of more frequent hygiene habits, since health attitudes and behaviors are significantly affected by life experiences and personal histories2.
The main limitation of the study is the time elapsed from data collection to publication (15 years), however, as it is an association study and not a prevalence study, the findings remain valid. Other limitations are related to the fact that the information obtained from the children and from the guardians' questionnaire are subject to information and memory bias. In addition, the associations found should be analyzed with caution, since the study does not intend to make direct inferences between causes and effects, but rather to assess the complexity of behavioral and social elements involved in children's oral hygiene practice.
Despite being a school-based study, the inference of the results for a population of non-school children is strong. With the inclusion of schoolchildren in the design, almost all children aged 7 to 10 years were obtained, since more than 99%38 of children aged 6 to 14 years are enrolled in the education system.
CONCLUSION
The adoption of oral hygiene habits in children is a complex behavior determined by a variety of factors related to different aspects of life. Among the child characteristics studied, birth weight and caries experience were associated with intermediate and more favorable oral hygiene practice, respectively. The results of this study reinforce that family cohesion is important for the frequency of performing oral hygiene habits, in the same way as the use of health services through dental appointments and the possession of one's own toothbrush without sharing.
The importance of social determinants in the adoption of positive habits to maintain adequate oral health is evident, reinforcing the need for a more comprehensive approach from the perspective of social inequalities. In addition, a greater understanding on the part of health professionals is of fundamental need of how health behaviors evolve, develop and change so that knowledge about oral hygiene methods is transmitted individually according to the social and family context in which each child is inserted. In addition, the considerations explained in this study can be used to support actions and health programs that are more positive and effective in relation to the adoption and perpetuation of oral hygiene habits and maintenance of oral health by children and those involved in their social context.
Author Contributions
Conception, planning, analysis, interpretation of results and writing of the work: MPMZ; Design, planning, interpretation of results and final review of the work: MCBM; Analysis, interpretation of results and writing of the work: KGM; conception, planning, interpretation of results, writing of the work and final review of the work: ETSN. All authors approved the final version submitted.
Funding
This project was funded by the Vitória Science and Technology Support Fund (FACITEC).
Acknowledgments
Municipal Department of Education of Vitória- Espírito Santo, Brazil.
Conflicts of Interest
The authors declare that they have no conflicts of interest regarding the authorship and publication of this article.
REFERENCES
1.Herrera MDS, Medina-Solis C.E, Minaya-Sánchez M, Pontigo-Loyola AP, Villalobos-Rodelo JJ, Islas-Granillo H, Rosa-Santillana RL, Maupomé G. Dental plaque, preventive care, and tooth brushing associated with dental caries in primary teeth in schoolchildren ages 6-9 years of Leon, Nicaragua. Med Sci Monit. 2013; 19: 1019-1026. DOI: 10.12659/MSM.884025 [ Links ]
2.Freeman R. The determinants of dental health attitudes and behaviours. British Dental Journal. 1999; 187(1): 15-18. [ Links ]
3.Filho AP, Buss PM, Esperidião MA. Promoção da saúde e seus fundamentos: Determinantes sociais de saúde, ação intersetorial e políticas públicas saudáveis. 2014. In Paim JS; Almeida-Filho N. Saúde Coletiva: teoria e prática. Rio de Janeiro, ed. Medbook 2014; 305-326. [ Links ]
4.Casanova-Rosado AJ, Medina-Solís CE, Casanova-Rosado JF, Vallejos-Sánchez AA, Minaya-Sánchez M, Mendoza-Rodríguez M, Márquez-Rodríguez S, Maupomé G. Tooth brushing frequency in Mexican schoolchildren and associated socio-demographic, socioeconomic, and dental variables. Med. Sci. Monit. 2014; 20: 938-44. [ Links ]
5.Levin KA, Currie C. Adolescent toothbrushing and the home environment: sociodemographic factors, family relationships and mealtime routines and disorganisation. Community Dent Oral Epidemiol. 2010; 38:10-18. [ Links ]
6.Lapresa LB, Barbero BS, Arizaleta LH. Prevalencia de hábitos bucodentales saludables en la población infanto-juvenil residente en España. An Pediatr. 2012; 76(3): 140-47. [ Links ]
7.Stanev N, Doichinova L, Andreeva-Borisova R. The Role Of Parents Health Literacy For The Development Of Dental Caries In Children. MedInform. 2020; 7(2): 1190-1197. [ Links ]
8.Macgregor IDM, Balding JW. Toothbrushing frequency in relation to family size and bedtimes in English schoolchildren. Community Dent Oral Epidemiol. 1987; 15: 181-3. [ Links ]
9.Faria CP, Cade NV, Nascimento LR, Molina MDCB. Prevalência de excesso de peso em crianças de sete a dez anos de Vitória - ES, Brasil: um estudo de base escolar. Revista Brasileira de Pesquisa em Saúde. 2011; 13(1): 31-37. [ Links ]
10.Davoglio RS, Aerts DRG, Abegg C, Freddo SL, Monteiro L. Fatores associados a hábitos de saúde bucal e utilização de serviços odontológicos entre adolescentes. Cad. Saúde Pública. 2009; 25(3): 655-667. [ Links ]
11.Ferreira LL, Brandão GAM, Garcia G, Batista MF, Costa LST, Ambrosano GMB, Possobon RF. Coesão familiar associada à saúde bucal, fatores socioeconômicos e comportamentos em saúde. Ciência & Saúde Coletiva. 2013; 18(8): 2461-73. [ Links ]
12.Koerber A, Graumlich S, Punwani LC, Berbaum ML, Burns JL, Levy SR, Cowell JM, Flay BR. Covariates of Tooth-brushing Frequency in Low-income African Americans From Grades 5 to 8. Pediatric Dentistry 2006; 28(6). [ Links ]
13.Instituto Brasileiro de Geografia e Estatística (IBGE); 2022. Avaliable from: https://www.ibge.gov.br/estatisticas/sociais/populacao/9103-estimativas-de-populacao.html?edicao=31451&t=resultados > [ Links ].
14.Oliveira Neto AG, Mendes E de O, Thomes CR, Lima S da S, Oliveira R da C, Pinto C de O, Santos JL dos, Bandeira ME, Vieira HF, Carvalho WC, Silva DW dos S, Costa LVD de A, Santana LR, Feitosa ACR. A promotion of oral health in the context of the primary school environment: bibliographic review. Research Society and Development. 2021; 10(12): e78101220191. [ Links ]
15.Instituto Brasileiro de Geografia e Estatística, 2019. Produto Interno Bruto dos Municípios. Avaliable from: <https://www.ibge.gov.br/estatisticas/economicas/contas-nacionais/9088-produto-interno-bruto-dos-municipios.html?=&t=destaques> [ Links ].
16.Ministério da Saúde. Brasil, 2012. Índice de Desempenho do SUS (IDSUS). Avaliable from: <http://legado.vitoria.es.gov.br/regionais/indicadores/idsus1.asp> [ Links ].
17.Medina-Solís CE, Villalobos-Rodelo JJ, Márquez-Corona ML, Vallejos-Sánchez AA, Portillo-Núñez CL, Casanova-Rosado AJ. Desigualdades socioeconómicas en la utilización de servicios de salud bucal: estudio en escolares mexicanos de 6 a 12 años de edad. Cad. Saúde Pública. 2009; 25(12): 2621-31. [ Links ]
18.Braubach M, Fairburn J. Social inequities in environmental risks associated with housing and residential location-a review of evidence. European Journal of Public Health. 2009; 20(1): 36-42. [ Links ]
19.Gabardo MCL, Moysés SJ, Moysés ST, Olandoski M, Olinto M. TA, Pattussi MP. Multilevel analysis of self-perception in oral health and associated factors in Southern Brazilian adults: a cross-sectional study. Cad. Saúde Pública. 2015; 31(1): 49-59. [ Links ]
20.Campos GW, Barros RB, Castro AM. de. Avaliação de política nacional de promoção da saúde. Ciência & Saúde Coletiva. 2004; 9(3): 745-49. [ Links ]
21.Prado JS, Aquino DR, Cortelli JR, Cortelli SC. Condição Dentária e Hábitos de Higiene Bucal em Crianças com Idade Escolar. Rev. Biociênc 2001; 7(1): 63-69. [ Links ]
22.Okada M, Kawamura M, Kaihara Y, Matsuzaki Y, Kuwahara S, Ishidori H, Miura K. Influence of parents' oral health behaviour on oral health status of their school children: an exploratory study employing a causal modelling technique. International Journal of Paediatric Dentistry 2002; 12: 101-108. [ Links ]
23.Castilho ARF, Mialheb FL, Barbosa TS, Puppin-Rontanid MR. Influence of family environment on children's oral health: a systematic review. J Pediatr 2013; 89(2): 116-123. [ Links ]
24.Domingues SM, Carvalho ACD, Narvai PC. Saúde bucal e cuidado odontológico: representações sociais de mães usuárias de um serviço público de saúde. Rev Bras Crescimento Desenvolv Hum 2008; 18(1): 66-78. [ Links ]
25.Freire MCM, Sheiham A, Bino YA. Hábitos de higiene bucal e fatores sociodemográficos em adolescentes. Rev Bras Epidemiol 2007; 10(4): 606-14. [ Links ]
26.Maes L, Vereecken C, Vanobbergen J, Honkala S. Tooth brushing and social characteristics of families in 32 countries. International Dental Journal 2006; 56: 159-167. [ Links ]
27.Adair PM, Pine CM. Burnside G, Nicoll AD, Gillett A. et al. Familial and cultural perceptions and beliefs of oral hygiene and dietary practices among ethnically and socio-economically diverse groups. Community Dent Health. 2004; 21: 102-11. [ Links ]
28.Roseiro CP, Paula KMP de, Mancini CN. Estresse e enfrentamento infantil no contexto do divórcio parental. Arq. bras. psicol. 2020; 72(1): 55-71. [ Links ]
29.Vallejos-Sánchez AA, Medina-Solís CE, Maupomé G, Casanova-Rosado JF, Minaya-Sánchez M, Villalobos-Rodelo JJ, Pontigo-Loyola AP. Sociobehavioral Factors Influencing Toothbrushing Frequency Among Schoolchildren. J Am Dent Assoc. 2008; 139: 743-749. [ Links ]
30.Rajab LD, Petersen PE, Bakaeen G, Hamdan MA. Oral health behaviour of schoolchildren and parents in Jordan. International Journal of Paediatric Dentistry. 2002; 12: 168-76. [ Links ]
31.Paredes SO, Almeida DB, Fernandes JMFA, Forte FDS, Sampaio FC. Behavioral and social factors related to dental caries in 3 to 13 year-old children from João Pessoa, Paraíba, Brazil. Rev. odonto ciênc 2009; 24(3): 231-35. [ Links ]
32.Ministério da Saúde. Indicadores e Padrões de Avaliação - PSE Ciclo 2021/2022. Brasília: Departamento de Atenção Básica, Secretaria de Atenção à Saúde, Ministério da Saúde, Brasília, 2021. [ Links ]
33.Solis G, Pesaressi E, Mormontoy W. Tendencia y factores asociados a la frecuencia de cepillado dental en menores de doce años, Perú 2013-2018. Rev Peru Med Exp Salud Publica. 2019; 36(4): 562-72. [ Links ]
34.Diniz MF, Coldebella RC, Zuanon ACC, Cordeiro RCL. Alterações orais em crianças prematuras e de baixo peso ao nascer: a importância da relação entre pediatras e odontopediatras. Rev Paul Pediatr. 2011; 29(3): 449-55. [ Links ]
35.Sousa MF, Lobato LS, Pereira Neta MAL, Sousa LF, Farias TC, Pinheiro MWS, Caldas TT da S, Gomes HLP, Aquiles I da SL, Castro LFN, Cruz ES da, Dias A da S e S. Oral alterations in preterm and low birth weight children: the importance of multidisciplinary work. Research Society and Development. 2022; 11(3): e24311326528. [ Links ]
36.Guido JA, Mier EAM, Soto A, Eggertsson H, Sanders BJ, Jone JE, Weddell JA, Cruz IV, Concha JLA. Caries prevalence and its association with brushing habits, water availability, and the intake of sugared beverages. International Journal of Paediatric Dentistry. 2011; 21: 432-440. [ Links ]
37.Hernández-Martínez CT, Medina-Solís CE, Robles-Bermeo NL, Mendonza-Rodríguez MM, Veras-Hernández M, Rosa-Santillana R, Escoffié-Ramírez M Márquez-Rodríguez. Uso de auxiliares para la higiene bucal y su distribución por edad y sexo em escolares de seis a 12 años de edad. Revista de Investigacíón Clínica. 2014; 66(2): 157-163. [ Links ]
38.Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Nacional por Amostra de Domicílios Contínua (PNAD-C - Suplemento educação): microdados 2020. Avaliable from: <https://www.ibge.gov.br/estatisticas/downloadsestatisticas.html?caminho=Trabalho_e_Rendimento/Pesquisa_Nacional_por_Amostra_de_Domicilios_continua/Anual/Microdados/Trimestre> [ Links ]
 Correspondence:
Correspondence:
Edson Theodoro dos Santos-Neto
edsontheodoroneto@gmail.com
Manuscript received: may 2021
Manuscript accepted: december 2021
Version of record online: june 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}