










Serviços Personalizados
artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.2 Santo André maio/ago. 2022
http://dx.doi.org/10.36311/jhgd.v32.13145
ORIGINAL ARTICLE
Determinants of age at first birth among women in Ethiopia using cox proportional hazards model
Yihenew Mitiku AlemuI; Molalign Gualu GobenaII
IDepartment of Statistics, College of Natural & Computational Science, Assosa University, Assosa, Ethiopia
IIDepartment of Statistics, College of Natural & Computational Science, Assosa University, Assosa, Ethiopia
ABSTRACT
BACKGROUNG: the age at first birth corresponds to the age of the mother giving birth to the first child. The delivery of the primary child is an important event that leaves a social mark on a woman's life. It is a woman's clear transition to parenthood with the roles and responsibilities involved. Premature birth can negatively affect women's socio-economic well-being in subsequent years. The study aims at accessing the determinants of age at first birth among Ethiopian women
METHODS: the data for this study was extracted from the published reports of Ethiopian Demographic and Health Survey. The study used15, 683women aged 15-49 years from nine regions and two city administrations. Cox Proportional hazards model was used for identifying factors associated with age at first birth
RESULTS: the median time of age at first birth for Ethiopian women was22 years with 95% CI; (21.82, 22.18).Cox Proportional Hazards Model shows that region, place of residence, education, wealth index, religion, work status, age at first marriage, age at first sex, and use of contraceptives have significant effects on the age at first birth at 5% level of significance. From region category, Amhararegion (p-value=0.398), BenishangulGumuz(p-value=0.112) Region, and Gambella region(p-value=0.062) were not significant at 5% level of significance
CONCLUSIONS: the age at first birth was positively correlated with the age at first sexual intercourse. A woman who has sexual intercourse much earlier gives birth earlier than a woman who is late for first intercourse
Keywords: birth, age, proportional hazards model.
RESUMO
INTRODUÇÃO: a idade do primeiro parto corresponde à idade da mãe que dá à luz ao primeiro filho. O parto do filho primário é um evento importante que deixa uma marca social na vida da mulher. É a transição clara de uma mulher para a paternidade com os papéis e responsabilidades envolvidos. O nascimento prematuro pode afetar negativamente o bem-estar socioeconômico das mulheres nos anos subsequentes. O estudo visa acessar os determinantes da idade ao primeiro parto entre as mulheres etíopes
MÉTODO: os dados para este estudo foram extraídos dos relatórios publicados do Ethiopian Demographic and Health Survey. O estudo utilizou15.683 mulheres de 15 a 49 anos de nove regiões e duas prefeituras. O modelo de riscos proporcionais de Cox foi utilizado para identificar os fatores associados à idade ao primeiro parto
RESULTADOS: o tempo mediano de idade ao primeiro parto para mulheres etíopes foi de 22 anos com IC 95%; (21,82; 22,18).O Modelo de Riscos Proporcionais de Cox mostra que região, local de residência, educação, índice de riqueza, religião, situação profissional, idade do primeiro casamento, idade da primeira relação sexual e uso de anticoncepcionais têm efeitos significativos sobre a primeira idade nascimento ao nível de 5% de significância. Da categoria de região, Amhararegion (p-value=0,398), BenishangulGumuz (p-value=0,112) Region, e Gambella region (p-value=0,062) não foram significativos ao nível de significância de 5%
CONCLUSÃO: a idade do primeiro parto correlacionou-se positivamente com a idade da primeira relação sexual. Uma mulher que tem relações sexuais muito mais cedo, dá à luz mais cedo do que uma mulher que está atrasada para a primeira relação
Palavras-chave: Parto, idade, Modelo de riscos proporcionais.
Authors summary
Why was this study done?
Age at first birth was one of the health problems of the mother and her child. This study was conducted to identify social and demographic factors that affect age at first birth among women in Ethiopia.
What did the researchers do and find?
The data for this study was extracted from the published reports of Ethiopian Demographic and Health Survey. The study uses a total of 15,683 women. Using Cox proportional hazard model we found that Region, educational background, age at first marriage, religion, residence, work status, wealth index, age of sexual intercourse, and contraceptive use were significantly affect age at first birth.
What do these findings mean?
The result of the study indicated that as age at first marriage increases there was a decrease in time to first birth. Women in rural areas were less likely to give birth for the first time than women in urban areas. The risk of first birth increases with age at first sexual intercourse. Women using birth control had a lower risk of having their first child than women not using birth control.
INTRODUCTION
First childbirth is the age at which a mother gives birth for the first time. According to the report, a woman's reproductive age has a strong influence on the demographic behavior of women and the general population1.The delivery of the primary child is an important event that leaves a social markon a woman's life. It is a woman's clear transition to parenthood with the roles and responsibilities involved.
Premature birth can negatively affect women's socio-economic well-being in subsequent years2. Indeed, when women begin to give birth, they have to give up certain roles to take on others that can require a lot of time and resources3. The negative consequences of this can be in the areas of career development, education, marital stability, wealth and, most importantly health. It also affects the types and opportunities of care for women and their children, social changes, reproductive tendencies and economic conditions. Teenage pregnancies due to premature delivery of the earliest child are also associated with maternal mortality3.Studying the dynamics of birth timing and intervals is important for many reasons, including understanding the overall family size and maternal mortality4. Modeling birth data is one of the best advantages of socio-economic research. Some predictors were used to determine birth patterns such as first birth interval after marriage5. Several hypothetical approaches have been developed to clarifythevariations in fertility. The most common indicator of fertility rate is the total fertility rate. Thisis defined as the average number of children a woman will have if she reaches reproductive age3.
Factors that affect the time at which the first child is born are varied and to varying degrees. There are economic, national and international factors as well as personal, family, and social factors. Personal factors were attitudes like contraceptive use and education. Family factors include socioeconomic characteristics such as parental education, place of residence, place of birth, religion, societal and employment status. Social factors include norms, practices, peer pressure, and reception of cohabitation6.
According to a study on the factors that determine the time to delivery of the first children after marriage7,the occupational status of woman is of great importance in the period after the first child birth. They said that women who go to work after marriage were more likely to have their first child longer after marriage than those who remain comfortable after their first marriage. However, these results are in inconsistent with the results of the study conducted by8 that analyzed the factors that determine marriage at the time of first child birth after marriage, which indicates that the first child after marriage is not affected regardless of whether a woman works or not after marriage.Therefore this study aims at assessing the determinants of age at first birth among Ethiopian women using Cox Proportional Hazards Model.
METHODS
Source of Data
The data for this study was extracted from the published reports of Ethiopian Demographic and Health Survey9. The 2016 Ethiopia Demographic and Health Survey (EDHS) is designed to provide data to monitor the population and health situation in Ethiopia. EDHS 2016 is the fourth Demographic and Health Survey conducted in Ethiopia since 2000. The objective of the survey is to provide reliable estimates of fertility, marriage, sexual activity, reproductive preferences, family planning methods, breastfeeding practices, nutrition, childhood and motherhood, mortality, maternal and child health, HIV/AIDS and other sexually transmitted infections (STIs), women's empowerment, female genital mutilation/mutation, and domestic violence without Program managers and decision makers can use to evaluate and improve existing programs.
Sampling Design
The sampling framework used for EDHS 2016 was the Ethiopian Population and Housing Census (PHC), conducted in 2007 by the Central Statistics Authority (CSA) in Ethiopia. The Census base is a comprehensive list of 84,915 census tracts (EAs) created for the 2007 PHC. Administratively, Ethiopia is divided into nine geographic regions and two administrative cities. The 2016 EDHS form is designed to provide estimates of key indicators for the country as a whole, for separate urban and rural areas, and for each of the nine regions and two administrative cities.
The 2016 EDHS sample was stratified and selected in two stages. Each region was stratified into urban and rural areas, yielding 21 sampling strata. Samples of EAs were selected independently in each stratum in two stages. Implicit stratification and proportional allocation were achieved at each of the lower administrative levels by sorting the sampling frame within each sampling stratum before sample selection, according to administrative units in different levels, and by using a probability proportional to size selection at the first stage of sampling.
In the first phase,a total of 645sites (202 urban areas and 443 rural areas) were selected with a probability proportional to the size of the site (based on the 2007 PHC) and with the selection of the siteselected independently in each stratum sampling. Household census activities were conducted in selected regions from September to December 2015. The list of households obtained was therefore used as a sampling frame to select households at the second level. All women aged 15-49 who were permanent residents of selected households or guests staying in the household the night before the survey were eligible to be interviewed.In the interviewed households, 16,583 eligible women were identified for individual interviews; interviews were completed with 15,683 women, yielding a response rate of 95 percent9.
Variables in the Study
The Response Variable
The response variable is the age at first birth, which is measured in years. For analysis, those women gave birth event coded 1 (success) and those who did not give birth 0 (censored).
Explanatory Variables
Several predictors were considered in this study to investigate the determinant factors of age at first birth. These were education, region, religion, work status, wealth index, place of residence, age at first marriage, age at first sex, and use of contraceptive.
Methods of Data Analysis
The Survival Model
Survival analysis is a set of statistical data analysis procedures where the outcome variable of interest is the time until an event occurs. By time we mean the year, month, week or day from the start of tracking an individual until an event occurs; alternatively, time can refer to an individual's age when an event occurs. By case we mean mortality, morbidity, relapse into remission, recovery (e.g. return to work), or any other specified experience of interest that may occur with an individual. The problem of analyzing data over time arises in several application areas such as medicine, biology, public health, epidemiology, engineering, economics, sociology, demographics, etc. The terms lifetime analysis, duration analysis, event history analysis, failure-time analysis, reliability analysis, and transition analysis refer essentially to the same group of techniques, although the emphases in certain modeling aspects could differ across disciplines10.
The use of survival analysis, as distinct from the use of other statistical methods, is more important when some subjects lose follow-up time or when the observation period ends, and some patients may not know the event of interest during the study period. In the second case, we cannot have complete information about these people. These incomplete observations are believed to have been censored. Most existential analysis considers a major analytical problem to be censorship. Basically, censorship occurs when we have information about the survival time of an individual, but we do not know the exact survival time. Such an event can occur due to either; one did not experience the event until the end of the study, one was lost to follow-up for the duration of the study, and one withdrew from the study for unknown/known reasons. There are three types of censorship.
Right censoring: Survival time is said to be right censored when it is recorded from its beginning to a defined time before its end time. This type of censoring is a commonly recognized during survival analysis and considered in this study.
Left censoring: Survival time is said to be left censored if an individual develops an event of interest prior to the beginning of the study.
Interval censorship: Duration is said to be interval censorship when it is known only that the event of interest occurred during a period of time, but the exact time of its occurrence is not known.
Cox PH Regression Model
Proposed a semi-parametric model for the hazard function that allows the addition of covariates, while keeping the baseline hazards unspecified and can take only positive values. With this parameterization, the Cox hazard function is11

Where , ho (t) is the baseline hazard function which is obtained when all X′s are set to zero; Xi is a vector of covariates and β is a vector of parameters.
In this model, no distributional assumption is made for the survival time; the only assumption is that the hazard ratio does not change over time (i.e., proportional hazard model). Even though the baseline hazard is not specified, we can still get a good estimate for the regression coefficients, β, hazard ratio, and adjusted hazard curves.
The hazard ratio of two individuals with different covariates X and X*is given by:

This hazard ratio is time-independent, that is why this is called the proportional hazards model. The parameter of the Cox proportional hazard model refers to the hazard ratio of one group in comparison to the other groups for categorical covariates and the change in hazard ratio with a unit change of the covariate for the continuous variables when other covariates are fixed.
The change in hazard ratio for the continuous covariate is given by:

which represent the change in the hazard when there is a unit change in the covarite while other covariates keep constant.
For categorical explanatory variable X with levels, the model contains (a-1) dummy variables defined as Di = 1, if x =i, and 0 otherwise for i= 1,2,…,a -1. Let β_1,β_2,…,β_(a-1) denote the coefficient of the levels of dummy variables. The ratio of the hazard of two subjects, one with X at level j and the other with k (j,k = 1,2,…, a-1), provided that the values of all other explanatory variables for this subject are the same, the hazard ratio between these two categories is given by:

The quantity exp(βj - βk)100% signifies the ratio of the hazard function for the subject at level j and k of covariates, given that the effect of other covariate keeps fixed.
RESULTS
Descriptive results
The result (table 1) showed from the total of 15,683 respondents, 7193 (45.9%) women had given birth and the remaining 8,490 (54.1%) had not given birth. Of the total, 1682 (10.7%) respondents were from the Tigray region, 1128 (7.2%) were from theAfar region, 1719 (11%) were from the Amhara region, 1892 (12.1%) werefrom the Oromia region, 1391 (8.9%)were from the Somali region, 1126 (7.2%)were from theBenishangulgumuz region, 1849 (11.8%)were from the southern region, 1035 (6.6%) werefrom theGambella region, 906 (5.8%) were from the Harari region, 1824 (11.6%) were from the city government of Addis Ababa and 1131 (7.2%) from the city government of Dire Dewa. The majority of respondents 7033 (44.80%) had no education while 5213 (33.2%) had primary education, 2238 (33.2%) had secondary education, and 1199 (7. 6%) had a higher education.
In terms of the wealth index, about 5940 (37.9%) were classified as poor, about 2002 (12.85%) were in the medium range and the remaining 7741 (49.4%) were rich. More than half (63.8%) of women were unemployed. Of the total study participants, 6413 (40.9%) were Orthodox, 91 (0.6%)were Catholic, 2814 (17.9%)were Protestant, 6209 (39.9%) were Muslim, 84 (0.5%)were traditional and 72 (0.5%) were other religion. The majority of respondents 10335 (65.9%) were rural residents and 5348 (34.1%) were urban residents. Approximately 12,371 (78.9%) women were not using contraception and 3,312 (21.1%) were using contraception. The median time of age at first birth for Ethiopian women was 22 years with 95% CI; (21.82, 22.18) (table 1).
Results of Cox proportional Hazards Model
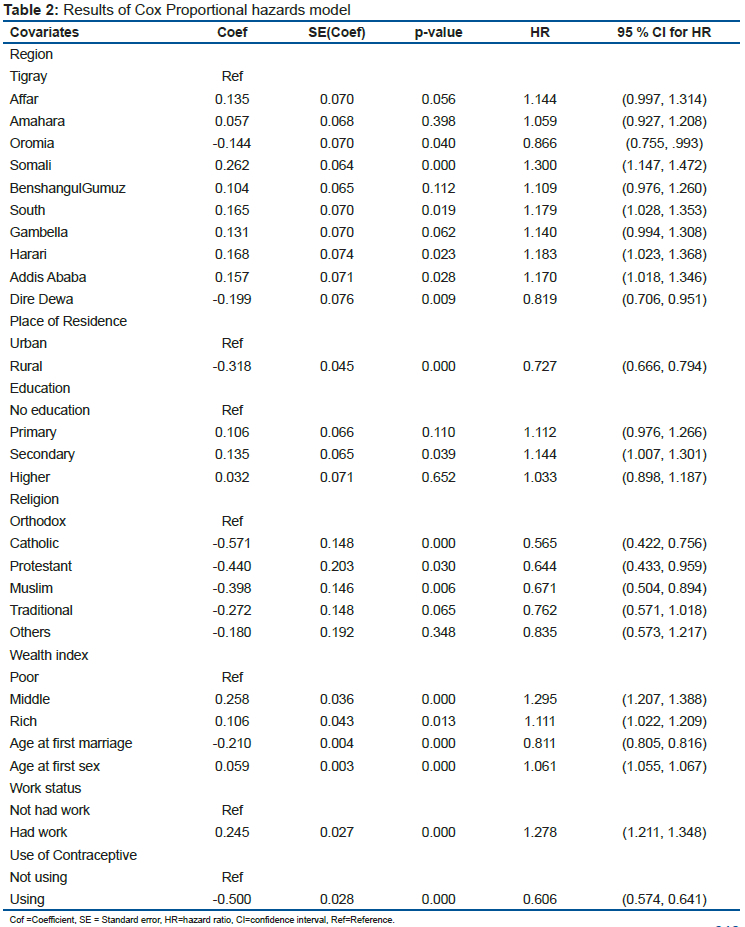
Cox proportional hazard model (table 2) showedthat regions, residence, education, wealth index, religion, work status, age at first marriage, age at first intercourse and contraceptive use had a significant effect on age at firstchildbearing at the 5% level of significance. In the regional classification, the Amhara region (p-value = 0.398), the BenishangulGumuz region (p-value = 0.112) and the Gambella region (p-value = 0.062) were not significant. Primary (p-value = 0.110) and secondary (p-value = 0.652) education levels were also not significant at the 5% level of significance.
The hazard ratios for the Oromia region, the Somali region, the Southern region, the Harari region, Addis Ababa and Dire Dewa were 0.866, 1.30, 1.179, 1.183, 1.170 and 0.819 with p-values of 0.040, 0.000, 0.019, 0.023, 0.028 and 0.09 respectively. This showed that women in the Oromia region were 86.6% less likely to have their first child than women in the Tigray region. Women in the Somali region are 1.30 times more likely to give birth than women in the Tigray region. Women in theSouthern region are 1.179 times more likely to give birth than women in the Tigray region. The chance of giving delivery to a first child for women in the Harari region is at least 18.3% higher. Women in Addis Ababa were 17% more likely to have their first child than women in the Tigray region. The risk of age at first birth for women in Dire Dewa was 81.9% lower than for women in the Tigray region.
Cox's proportional hazard model showed that place of residence significantly affects the age at first birth in women (p-value = 0.000 and HR = 0.727). This shows that women in rural areas were 72.7% less likely to give birth for the first time than women in urban areas. Women with secondary education are 14.4% more likely to have their first child than women with no education.
The risk ratios for Catholic, Protestant, and Muslim religious groups were 0.565, 0.644, and 0.671 with p-values of 0.000, 0.030, and 0.006, respectively. This showed that Catholic women had a 56.5% lower risk of having their first child than Orthodox women. Similarly, the time delay before first childbearing among Protestant and Muslim women was 0.565 times and 0.644 times lower, respectively, comparedwith Orthodox women. Regarding the wealth index, women in the middle quintile are 1.295 times more likely to have their first child than women in the poor quintile. The risk of giving birth for the first time in rich women is 1.111 times higher than poor.
The hazard ratio for age at first marriage was 0.811 with P-value=0.000. This indicates that there was an 81.1 decrease in time to first birth with a one year increase in age. The risk of first birth increases with age at first sex. This means that there was a 10.61% increase in the time to first birth relative to a one year increase in age. The hazard ratio for women who had work is 1.278. This suggests that the risk of having a first child in women in labor is 1.278 times higher than in women who are not in labor. Women using birth control had a 60.6% lower risk of having their first child than women not using birth control.
DISCUSSION
The study aimed to approach the factors determining the age of first childbearing of Ethiopian women. Region, educational background, age at first marriage, religion, residence, occupation, wealth index, age of sexual intercourse, and contraceptive use were significant factors. The median age at first birth for Ethiopian women was 22.
The findings of this study showed that region had a significant effect on age at first birth at 5% level of significance. Women from Oromia region were less likely to have birth compared with women in Tigray region. Women from South region were more likely to have birth than those Tigray region women. Time to first birth in Somali region women was higher than Tigray region women. The chance of first birth was higher in Harari region women. The study by12showed that the probability of having a first child immediately after the first marriage was significantly higher in the Oromia and SNNP regions than in the Amhara region.
The results of this study suggest that place of residence is an important predictor of the timing of first childbearing among Ethiopian women. Rural women have a 72.7% lower risk of having their first child than urban women. A study by13showed that whether women are in urban or rural areas, the time to give birth after marriage is not affected. The results of this study also showed that uneducated women were at lower risk of having their first child than women withsecondary education.In a similar research by8, women's education level had a strong positive effect on the timing of their first childbirth, and that women with primary or secondary education were at higher risk of having their first child after marriage than their illiterate colleagues. This contradicts withthe report14that womanabove primary education are less likely to get married earlier than uneducated women.
The study found that religion to be a risk factor of age at first birth in Ethiopia. The risk of age at first birth was low for Catholic religion, Protestant, and Muslim religion thanthose Orthodox religion. This is in contrast to studies14that found Muslim women were 1.14 times more likely to have their first child at an early age, while Catholic and other religious women were less likely to have their first child early. Similar results were obtained in Bangladesh15;Muslim women tend to give birth earlier than women of other religions. We have shown that the wealth index has a significant effect on the timing of aging at birth. Women in the middle quintile were 1.295 times more likely to have their first child than the poor. Rich women were 1.111 times more likely to have their first child than poor women. A study on the determinants of childbirth interval found that the income class of married women had a great influence on the timing of having their first child after marriage16; High-income class of women tend to spend more time having their first children after marriage than do the poorest women.
In this study, age at first childbearingwas negatively related to age at first marriage. This shows that there was an 81.1% decrease in time to first birth to every year increase in age. This is similar with a retrospective study ofage at marriage and time of first childdelivery12,17,indicating that the first marriage has significant impact on the risk of having child after the first marriage. Women who got married at a younger age in their first marriage were less likely to have their first child than women who married slightly older. The age at first birth was positively correlated to age at first sexualintercourse.Women who start sexual intercourse much earlier have their first child before the woman who is late for the first sexual intercourse.A Ugandan study examined the association between the ages of first sexual intercourse, the time of marriage and the time of first child birth and recognized important connection between age of first sexual intercourse and time of first birth18.
The study found that the risk of having a first child was 1.278 times higher among working women than in women without a job. This is consistent with a study by7 that found that women's employment status is of great importance during the time of first childbearing after marriage, stating that women go to work after marriage are more likely to have a longer time to give birth to the first child after marriage compared to other partners.However, these results are in contrast to the conclusions of the study conducted by8 which analyzed the determinants of marriage from first childbearing after marriage, which showed that although women have working or not after marriage, her chances of having her first child after marriage are not affected. Women using birth control had a 60.6% lower risk of having their first child delayed than women not using contraception. A Nigerian study by19 showed that the correct use of reliable contraception can delay childbearing. We expect women who use contraception to have their first child later than women who do not use contraception.
Limitations of the Study
The data for this study was extracted from the published reports of Ethiopian Demographic and Health Survey, which is the large data set and covers a large geographical area. Age at first birth was calculated based on the women recall for most participants this may result in recall and reporting biases.
Contributions to public health
If child birth occurs before adolescence is fully developed, the risk of morbidity and mortality in women can be much higher.Pregnancy is the leading cause of death among young women aged 15-19 years. Children born at early age are also at increased risk of poor health.The younger a woman is when she gives birth for the first time, the longer her total childbearing years and the more likely she is to give birth, increasing the risk to the life and health of the mother and child.
This study was important to provide an input for health care planners and program managers in designing site specific and scientifically sound interventions to address the gap in the utilization of family planning and increasing age at first birth due to this there would be noticeable effect in bringing down the level of infant mortality and thereby improving the health of women.
CONCLUSION
The purpose of this study was to investigate the determinantsof age at the first child birth among reproductive age of Ethiopian women. The Study showed that the median age at first child birth was 22 years. As a result of the Cox proportional hazards model, the major determinants of age of first child birth were region, place of residence, education, religion, wealth index, work status, age at first marriage, age at sexual intercourse, and contraceptive method. Age at first birth was positively correlated with age at first sexual intercourse.
List of Abbreviations
CI= Confidence Interval
CSA= Central Statistics Agency
DHS= Demographic and Health Survey
EA= Enumeration area
EDHS= Ethiopian Demographic and Health Survey
HIV/AIDS= Human Immune deficiency Virus/AcquiredImmune deficiency Syndrome
PHC=Population and Housing Census
STDs= Sexual Transmitted Diseases
Declarations
Ethics approval and consent to participate: Ethics approval and consent to participate were not applicable since thedata for this study was extracted from the published reports of Ethiopian Demographic and Health Survey.
Availability of Data and Materials
Data sets were obtainedfrom the CSA website accessed via http://www.statsethiopia.gov.et/.
Conflict of Interest
The authors declare that they have no conflicts interests.
Funding
There are no any funding sources.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Author's Contributions
YM contributed to the study concept and design,performed the analysis on the data set, as well as wrote thefirst draft of the paper. MG contributed to the analysisand interpretation of the data, in addition to drafting andcritical revision of the manuscript. All authors read and approved thefinal manuscript.
Acknowledgment
The authors of this article would like to thank the Central Statistical Agency of Ethiopia forallowing using the data.
REFERENCES
1.National Population Commission (Nigeria) and ICF International. Nigeria Demographic and Health Survey 2013. National Population Commission, Abuja, Nigeria; 2014. [ Links ]
2.OECD. Mean Age of Mothers as First Child Birth. 2012. [ Links ]
3.Manda S, Meyer R. Age at first marriage in Malawi: a Bayesian multilevel analysis using a discrete time to event model. Roy Stat Soc: Series A2005; 168: 439-455. [ Links ]
4.Gyimah SO. The dynamics of timing and spacing of births in Ghana. 57TJ Comp Fam Stud57T 2005; 36: 41-60. [ Links ]
5.Lloyd CB. Growing up global: the changing transitions to adulthood in developing countries. Washington, DC: the National Academies Press; 2005. [ Links ]
6.AminulHaque M, Sayem AM. Socioeconomic determinants of age at first birth in rural areas of Bangladesh. Asia Pac J Public Health. 2009; 21:104-11. [ Links ]
7.Daury, S.C. Bayesian Analysis of Cox Proportional Hazards Model for Time to First Birth after Marriage of Women in Bangladesh. Dhaka: Population council, 2012. [ Links ]
8.Azad, M.R., Mohitul, A.M. & Mohammad, M.A. Analysis of the determinants of marriage to first birth interval in Bangladesh. International Journal of Management and Sustainability, 2013, 2(12), 208-219. [ Links ]
9.Central Statistical Agency, Ethiopian Demographic and Health Survey, Addis Ababa, Ethiopia, 2016. [ Links ]
10.Aalen, O., Borgan, O., &Gjessing, H. Survival and event history analysis: a process point of view. Springer Science & Business Media, 2008. [ Links ]
11. Cox, D. R. Regression Models and Life Tables (with discussion), Journal of the Royal Statistical Society, Series B, 1972, 34(2). [ Links ]
12. Eshetu G. and Dula E. Age at First Marriage and First Birth Interval in Ethiopia: Analysis of the Roles of Social and Demographic Factor. African Population Studies, (2014). Vol. 28, Nº 3. [ Links ]
13.Anuwoje, I., & Albert, L. Survival analysis of time to first birth after marriage. Research on Humanities and Social Sciences, 2013. 3 (12), 117-126. [ Links ]
14.Chandrasekhar S. Factors Affecting age at marriage and age at first birth in India. J. Quantitative Econ. 2010, 8(2): 81-97. [ Links ]
15.Kumar GA, Danabalan M. Determinants of Delayed First Birth. Indian J Community Med. 2006; 31: 4-5. [ Links ]
16.Nath, D.C., Land, K.C. &Goswami, G. Effects of the status of women on the first-birth interval in Indian urban society. Journal of Biosocial Science, (1999), 31(1), 55-69. Avaliable from: http://www.ncbi.nlm.nih.gov/pubmed/10081237 [ Links ]
17.Singh, S. N., &Narendra, R. Survival analysis of duration of waiting time to conception. Electronic Journal of Applied Statistical Analysis, 2011, 4(2), 144-154. Doi: 10.1285/i20705948v4n2p144. [ Links ]
18.Miller, B. C., & Heaton, T. B. Age at First Sexual Intercourse and the Timing of Marriage and Childbirth. Journal of Marriage and Family, 2014, 53(3), 719-732. [ Links ]
19.Adebowale SA, Fagbamigbe FA, Bamgboye EA. Contraceptive use: implication for completed fertility, parity progression and maternal nutritional status in Nigeria. Afr J Reprod Health; 2011, 15: 60-7. [ Links ]
 Correspondence:
Correspondence:
Yihenew Mitiku Alemu
yihenew.mt@gmail.com
Manuscript received: may 2021
Manuscript accepted: december 2021
Version of record online: june 2022


{kind=link}
{kind=link}