










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.2 Santo André maio/ago. 2022
http://dx.doi.org/10.36311/jhgd.v32.13312
ORIGINAL ARTICLE
Deep endometriosis: clinical and epidemiological findings of diagnosed women according to the criteria of the International Deep Endometriosis Analysis (IDEA) group
Cicília Fraga Rocha PontesI, II; Luciana Pardini ChamiéIII, IV; Mauro Monteiro de AguiarV; Eduardo Just da Costa e SilvaVI; Debora Farias Batista LeiteVII; Simone Angélica Leite de Carvalho SilvaVIII; José Luiz FigueiredoIX
IPrograma de Pós-Graduação em cirurgia, Universidade Federal de Pernambuco/Pesquisa e Extensão EBSERH, Recife-PE, Brasil
IIMedere, Medicina Diagnóstica Especializada, Recife (PE) Brasil
IIIDepartamento de diagnóstico por imagem, Fleury Medicina e Saúde, São Paulo (SP), Brasil
IVDepartamento de diagnóstico por imagem, Chamié Imagem da Mulher, São Paulo (SP), Brasil
VDepartamento de ginecologia, Universidade Federal de Pernambuco, Recife, PE 50670-901, Brasil
VIDepartamento de Radiologia, Instituto de Medicina Integral Professor Fernando Figueira, Recife, PE, 50070-550, Brasil - Departamento de Radiologia, do Hospital das Clínicas da Universidade Federal de Pernambuco, Recife, PE 50670-901, Brasil
VIIÁrea Acadêmica de Ginecologia e Obstetrícia do Centro de Ciências Médicas da Universidade Federal de Pernambuco; Hospital das Clínicas da Universidade Federal de Pernambuco, Recife, PE, Brasil
VIIIUniversidade de Pernambuco, UPE, Recife, PE, Brasil
IXDepartamento de Cirurgia, Universidade Federal de Pernambuco, Recife, PE 50670-901, Brasil
ABSTRACT
INTRODUCTION: endometriosis occurs when tissue similar to the endometrium affects the peritoneum, which can infiltrate structures and organs such as the bowel, ureter, bladder or vagina and is usually accompanied by an inflammatory process. It is estimated that the disease affects 6 to 10% of women of reproductive age and more than 50% of infertile women. The clinical and epidemiological data of patients with Deep endometriosis (DE) available in the literature come from studies whose samples were selected by surgery, therefore subject to selection bias. Transvaginal pelvic ultrasound with bowel preparation (TVUBP) has high specificity and sensitivity values
OBJECTIVE: to analyze the clinical and epidemiological profile of patients with DE diagnosed through the TVUBP
METHODS: it is a cross-sectional study of 227 patients with an ultrasound diagnosis of deep endometriosis
RESULTS: infertility affected 43.8% of women. Painful symptoms considered as moderate or severe (visual analogue scale, VAS, >3) had the following prevalence and mean values on the VAS scale, respectively: dysmenorrhea in 84.7% (6.9), dyspareunia in 69.1%, (4.5), menstrual dyschezia in 60.7% (4.3) and menstrual dysuria in 35.7% of patients. A history of multiple surgeries occurred in 10.4% and only 6.8% of patients had undergone physiotherapy for the pelvic floor
CONCLUSION: the DE population had a high prevalence of infertility and pain symptoms, which reflect the social impact on these women's quality of life and family planning. The high frequency of history of multiple surgical approaches and the low incidence of history of pelvic physiotherapy in the population with DE, contrary to the currently established ideal treatment recommendations, indicate the difficulty of access for patients to specialized centers
Keywords: endometriosis, epidemiology, ultrasonography, dysmenorrhea, dyspareunia, pelvic pain, infertility.
Authors summary
Why was this study done?
Generate information to contribute of alerting healthcare professionals who treat patients with deep endometriosis (DE) . The study was carried out to characterize the population with DE, a disease of high prevalence and social and economic impact worldwide. Most of the evidence that characterize the population with DE comes from samples submitted to surgical procedures (laparoscopy or laparotomy).Knowing the characteristics of women with DE can contribute to build strategies for organizing a network focused on public health, optimizing financial resources.
What did the researchers do and find?
We collected data from ultrasound reports in women with DE following the most up-to-date international protocol (IDEA group, 2016) to increase the specificity of the study sample selection. We collected information on the characteristics of patients with DE through a targeted clinical questionnaire. Our findings revealed a 43.8% of infertility prevalence. Painful symptoms considered moderate or severe had the following prevalence and mean values on the VAS scale, respectively: dysmenorrhea in 84.7% (6.9), dyspareunia in 69.1% (4,5), menstrual dyschezia in 60.7 % (4.3) and menstrual dysuria in 35.7% of patients. The study revealed a history of previous surgery to treat endometriosis in 29.5% of the patients. Only 6.8% of women with DE had undergone physiotherapy for the pelvic floor.
What do these findings mean?
The high prevalence of patients with multiple surgical approaches and the low prevalence of a history of pelvic physiotherapy (in contrast to the high prevalence of pain symptoms) indicate failure in the initial therapeutic approach currently recommended, reflecting the need for awareness of professionals in the area and encouragement the organization of reference centers. Some data reveal the social impact of DE and serve as an alert for the negative effect that the disease can have on the reproductive life of DE patients, reinforcing the importance of multidisciplinary care.
INTRODUCTION
Endometriosis is defined by the presence of endometrium-like epithelium and/or stroma outside the uterus, usually associated with an inflammatory process, which can infiltrate organs such as the intestine, vagina, and bladder1. It is a chronic, progressive, and complex disease, affecting about 10% of women of reproductive age and more than 50% of infertile patients2,3.
The classic clinical picture of deep endometriosis (DE) may present symptoms as progressive dysmenorrhea, menstrual Dyschezia, menstrual Dysuria, dyspareunia, chronic pelvic pain, and infertility, among other urinary and gastrointestinal symptom4,5. However, the clinical diagnosis is challenging because, in addition to some women being asymptomatic, DE can also present nonspecific symptoms4,6.
In public health, DE should be considered a problem, as the symptoms lead to loss of work productivity, causing a significant economic burden, and inducing costs comparable to other chronic diseases to treat pain and infertility problems. In addition, DE also impairs patients' quality of life with negative consequences on sexual function and personal relationships6,7.
Despite the diagnosis evolution, which currently can be performed with high accuracy by transvaginal ultrasound8,9, the technique can be optimized when performed after bowel preparation10-12. Knowledge about the clinical and epidemiological characteristics of women living with DE comes from samples taken from women diagnosed during a surgical procedure13-18, being, therefore, susceptible to selection bias.
Thus, this research aims to analyze the epidemiological and clinical characteristics of women living with DE diagnosed with a non-invasive protocol by transvaginal ultrasound.
METHODS
Study design
This was a cross-sectional study, carried out in Recife, Pernambuco, Brazil, between May 2019 and May 2021, approved by the Institutional Review Board of the Hospital das Clínicas of the Federal University of Pernambuco (Letter of approval No. 4,883.90).
Eligibility criteria
Women with suspected endometriosis who underwent transvaginal ultrasound after bowel preparation (TVUBP) for DE research in a public university service and two private clinics in the city of Recife were eligible. They were consecutively invited by convenience before the procedure was performed by a research assistant. Inclusion criteria were patients who underwent transvaginal ultrasound with a complete bowel preparation protocol and responded to the clinical questionnaire. Exclusion criteria were: history or suspicion of pelvic neoplasia and whose ultrasound result was negative, that is, without specific criteria for deep endometriosis. Only women with deep endometriosis diagnosed by transvaginal ultrasound remained in the final sample.
Procedures
Clinical history such as time of symptoms, time to diagnosis, obstetric and surgical history, and past and current medication history. Eligible participants completed a questionnaire on clinical and epidemiological aspects based on the international visual analog pain scale (VAS)19,20, assembled for this research. On a scale from 0 to 10, it addresses pain such as the menstrual period, dysmenorrhea, dyspareunia, Dysuria, and Dyschezia. Concerning pain symptoms, the women were instructed to consider the symptoms prior to using hormone blockade if they were using clinical treatment at the time of the examination.
Each exam was performed and interpreted in real-time by the same radiologist (C.P), who has had experience in gynecological ultrasound for nine years and in endometriosis research for five years (at baseline). Exams were performed with a 5-9 MHz probe (Logic E9 and Voluson E8, GE Healthcare®, Milwaukee, WIS).
Participants used two doses of oral laxative the day before the test (Bisacodyl, at 8:00 and 14:00), a low-residue diet for 24 hours before the test, and a rectal enema one hour before21.
All participants were evaluated according to the protocol of the International Deep Endometriosis Analysis Group, IDEA GROUP22.
Statistical analysis
Data were entered into an Excel 2010 spreadsheet and transferred to SPSS 13.0 software (Statistical Package for the Social Sciences) for statistical analysis. The variables were represented by measures of central tendency and adequate dispersion.
RESULTS
We recruited 398 women. Of these, 171 were excluded because they did not show specific signs of DE on TVUBP or were neoplasia suspected (Figure 1). Our final sample consisted of 227 women diagnosed with DE.

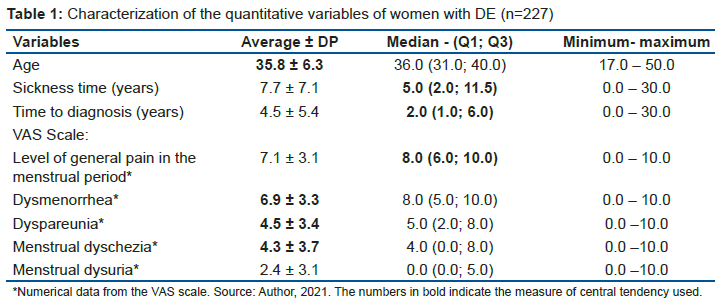
The mean age was 35.8 years, 80% of the patients were over 30 years old at the examination time. The median times of illness and delay to diagnosis were five and two years, respectively.
The average level of General Pain in the menstrual period by the VAS scale was 7.1. Painful symptoms obtained the following mean scores: 6.9 for dysmenorrhea, 4.3 for menstrual Dyschezia, and 4.5for dyspareunia. Menstrual Dysuria did not show a linear distribution. Table 1 summarized quantitative clinical and epidemiological characteristics.
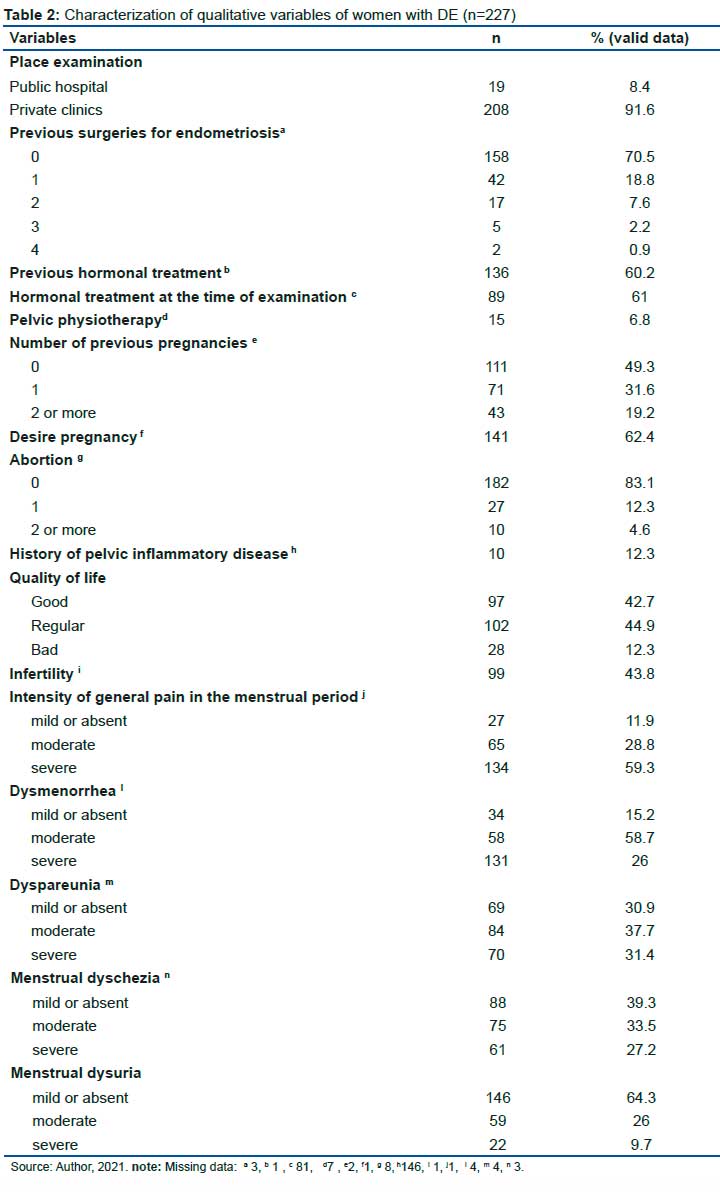
Qualitative characteristics are summarized in table 2.
Regarding treatment history, 29.5% of patients had already received surgical treatment for endometriosis, and 10.7% (24 of 224) had a history of 2 or more surgeries for DE. Oral contraceptive drug treatment or estrogen blockade had already been performed in 60.2% of patients, and 61% were using it at the time of the examination. Regarding the previous physiotherapy to relieve symptoms, only 6.8% of the patients had received it.
Concerning the clinical-obstetric history, 49.3% of the patients had no children, 63.6% had a desire to conceive, 4.6% had a chronology of 2 or more previous miscarriages, and 12.3% reported pelvic inflammatory disease.
As for the quality of life, 44.9% classified it as regular, 42.7% as good, and 12.3% as poor. Regarding classic symptoms, infertility occurred in 43.8% of women, and pain symptoms were subclassified as absent (VAS 0), mild (VAS 1.2), moderate (VAS 3,4,5,6, 7), and severe (VAS 9 and 10).
Painful symptoms considered moderate or severe had the following decreasing prevalence: Dysmenorrhea in 84.7%, Dyspareunia in 69.1%, menstrual Dyschezia in 60.7%, and menstrual Dysuria in 35.7%.
DISCUSSION
Our findings indicate a high prevalence of infertility and pain symptoms (mainly Dysmenorrhea, Dyspareunia, and menstrual Dyschezia), revealing particularities compared to outcomes reported in other countries2,10,15,18,23.
The mean age of patients was 35.8 years, similar to other studies24-26. Although the disease is typically diagnosed in this age group, probably when there are symptoms that cause repercussions or these patients seek diagnostic investigation, many studies have already shown that the onset of DE is early since adolescence27.
Infertility occurred in 43.8% of the patients in our sample, a higher number than that found by Leonardi et al.24 (20.9% in Australia), Bazot et al.28 (22.85% in France), or Morgan-Ortiz et al.26 (26%, in Austria). Our number is expected to be higher when compared to such studies that exclusively studied operated patients and possibly excluded those with infertility referred for assisted reproduction therapy.
The higher prevalence of infertility in this Brazilian region may be due to our sample selection. It was focused on those still looking for diagnostic investigation such as pain, infertility, or altered findings in routine exams.
It is noteworthy that there is a difference in methodology between this manuscript and previous researchers, who evaluated the records of patients in tertiary centers or interviewed women undergoing laparoscopy. The delay time between the onset of symptoms and the moment of diagnosis in this study (2.0 years) was lower than the value found by European researchers (which varied between 4 and 10 years)29-31. Therefore, a naturally longer delay in indicating a laparoscopy is expected than in requesting an ultrasound, due to the invasive nature of the former. Another issue is that most of the sample in this study was collected in private clinics (91.6%), whose access time to the diagnostic investigation exam should be much shorter when compared to patients in the public health system, as already demonstrated by Nnoaham in 201131.
Despite this, the fact that 60.2% of the patients had already used oral contraceptives or estrogen blockade makes us believe that probably many patients in this study already had an asymptomatic disease and the perception of the onset of symptoms may have occurred when the patients discontinued the treatment to try to conceive. The concept is already well established that the previous history of oral contraceptives is associated with more severe cases of endometriosis, possibly masking the symptoms but without preventing the progression of the disease in these patients32,33.
Patients in this study exhibited pain symptoms with a mean score of 6.9 for Dysmenorrhea and 4,3 for menstrual Dyschezia (other researchers found values that ranged between 6.9 and 7.7 for the first and, 6.6 for the last23,32,34). The slightly higher values in studies published in the literature may be justified because these authors consider only patients with surgical indications, potentially more severe than those in this research.
The high prevalence of moderate or severe pain symptoms (>85%) and infertility (43.8%) must be some of the reasons why 57.2% of the patients included in the study considered their quality of life moderate or poor.
On the other hand, some patients with moderate or severe pain levels on the VAS scale but responsive to clinical treatment explain the almost 43% of patients who judged their quality of life to be good. Future studies that investigate the correlation between pain intensity and prolonged use of contraceptives, which could interfere with the perception of quality of life, may be helpful.
Our data reflect the difficulties women face in accessing specialized treatment. It is essential to highlight that 29.5% of patients with DE had 1 to 4 previous surgeries for endometriosis treatment16,23, and, among these, 10.7% (24 of 224) had a history of 2 or more surgeries for DE, but persisted with ultrasound findings compatible with the disease. Since these women are usually seen by generalist gynecologists and have an early indication for surgery, without initial staging using an acceptable imaging method, there is a detriment to the planning of an excellent surgical team and, therefore, an increase in the rate of residual disease. The current concept of good practices seeks a smaller number of approaches, with a single and complete surgery being ideal, as advocated by Chapron6.
The role of pelvic physiotherapy in assessing and treating muscle disorders involving the pelvic floor, with consequent improvement in pain symptoms and the quality of life of women with DE, is already well established6,35. Still, in the treatment of DE, only 6.6% of the participants in this study had already performed pelvic physiotherapy. Our findings warn and reveal how this method has been used little in Pernambuco.
The knowledge dissemination among general gynecologists about new treatments, ideal diagnostic methods, and the creation of endometriosis reference centers are strategies with an expected positive impact on the affected population.
Some of our figures reveal the social impact of DE and alert the negative effect that the disease can cause on the reproductive life of DE women: 80% of the patients studied were over 30 years old, 62.4% had a desire to conceive, 43.8% already fulfilled the infertility criteria and 69.1% complained of deep dyspareunia (moderate and severe). Together, these data reinforce the importance of multidisciplinary care, of a broader look at these patients and their couples, who need to manage many issues arising from the emotional and financial impacts associated with infertility6,7.
However, some limitations of this study must be considered. First, the sample is susceptible to selection bias, as women were recruited from specialized sites to investigate endometriosis. On the other hand, it is noteworthy that our analysis is less susceptible to selection biases presented by most previous researchers whose samples were selected by indication of surgical treatment7,32. Therefore, our sample is more representative of the general population, which has a suggestive clinical history but did not undergo surgery for the diagnosis.
Another factor to consider is that the clinical questionnaires were answered by the participants, who may have had difficulty interpreting the terms used. We reiterate that the research instrument was built with language for lay people; thus, we believe that we have reduced the bias of the interviewer's interference.
On the other hand, the main strength is that the selected sample came from patients diagnosed in reference centers, using a non-invasive method, following international criteria, which made the chance of a false positive low (IDEA, 2016).
CONCLUSION
The analyzed sample of women living with DE had a high prevalence of infertility and pain symptoms (mainly dysmenorrhea, dyspareunia, and menstrual Dyschezia), reflecting the social impact of impairing on quality of life and family planning for these women. The high frequency of history of multiple surgical approaches and the low incidence of history of performing pelvic physiotherapy in the population with DE, contrary to the recommendations of ideal treatment, indicates the difficulty of access of patients to specialized centers. Selecting the sample based on ultrasound diagnostic criteria opens the horizon for a new methodology for analyzing patients with DE, possibly bringing them closer to the general population.
Author Contributions
Cicília: lead author, writing the text; Cicília, Mauro, Simone: idealization and elaboration of the questionnaires; Cicília, Mauro, Luciana, E. Just, Débora Leite and Jóse Luíz: text review.
Acknowledgments
Beatriz Correia for her collaboration in organizing the database; Homero Júnior, Camila Edeuzuita da Silva and Elisângela Regina da Silva for their help in collecting the clinical questionnaires.
Conflicts of Interest
None of the authors have a conflict of interest to declare.
REFERENCES
1.Sampson, J. A. Peritoneal endometriosis due to premenstrual dissemination of endometrial tissue into the peritoneal cavity. Am. J. Obstet. Gynecol.14, 422-469 (1927). [ Links ]
2.Giudice, L. C. & Kao, L. C. Endometriosis. Lancet364, 1789-1799 (2004). [ Links ]
3.Kuznetsov L, Dworzynski K, Davies M, Overton C. Diagnosis and management of endometriosis: Summary of NICE guidance. BMJ (Online). 2017; 358:1-5. [ Links ]
4.Fauconnier A, Chapron C. Endometriosis and pelvic pain: Epidemiological evidence of the relationship and implications. Human Reproduction Update. 2005; 11(6): 595-606. [ Links ]
5.Giudice, L. C., & Ph, D. (2010). Endometriosis. N Engl J Med 2010; 362: 2389-98. [ Links ]
6.CHAPRON, C. et al. Rethinking mechanisms, diagnosis and management of endometriosis. Nature Reviews Endocrinology, v.15, n.11, p.666-682, 2019. [ Links ]
7.MABROUK, M. et al. Painful Love: Superficial Dyspareunia and Three Dimensional Transperineal Ultrasound Evaluation of Pelvic Floor Muscle in Women with Endometriosis. Journal of Sex & Marital Therapy, v.46, n.2, p.187-196, 2020. [ Links ]
8.Bazot M, Thomassin I, Hourani R, Cortez A, Darai E. Diagnostic accuracy of transvaginal sonography for deep pelvic endometriosis. Ultrasound Obstet Gynecol 2004; 24(2): 180-185. [ Links ]
9.DESLANDES, A. et al. (2020). Current Status of Transvaginal Ultrasound Accuracy in the Diagnosis of Deep Infiltrating Endometriosis Before Surgery. Journal of Ultrasound in Medicine, 1-14. [ Links ]
10.ABRAO, M. S. et al. Comparison between clinical examination, transvaginal sonography and magnetic resonance imaging for the diagnosis of deep endometriosis. Hum Reprod, v.22, n.12, p. 3092-3097, 2007 [ Links ]
11.Goncalves, M. O. D. C., Podgaec, S., Dias, J. A., Gonzalez, M., & Abrao, M. S. (2010). Transvaginal ultrasonography with bowel preparation is able to predict the number of lesions and rectosigmoid layers affected in cases of deep endometriosis, defining surgical strategy. Human Reproduction, 25(3), 665-671. [ Links ]
12.Chamié, L. P., Pereira, R. M. A., Zanatta, A., & Serafini, P. C. (2010). Transvaginal US after Bowel Preparation for Deeply Infiltrating Endometriosis: Protocol, Imaging Appearances, and Laparoscopic Correlation. RadioGraphics, 30(5), 1235-1249. [ Links ]
13.Fauconnier A, Chapron C, Dubuisson JB, Vieira M, Dousset B, Bréart G. Relation between pain symptoms and the anatomic location of deep infiltrating endometriosis. Fertility and Sterility. 2002; 78(4): 719-26. [ Links ]
14.CHAPRON, C. et al. (2001). Does deep endometriosis infiltrating the uterosacral ligaments present an asymmetric lateral distribution? British Journal of Obstetrics and Gynaecology, 108(10), 1021-1024. [ Links ]
15.Chapron C, Fauconnier A, Vieira M, Barakat H, Dousset B, Pansini V, et al. Anatomical distribution of deeply infiltrating endometriosis: Surgical implications and proposition for a classification. Human Reproduction. 2003; 18(1): 157-61. [ Links ]
16.Chapron C, Chopin N, Borghese B, Foulot H, Dousset B, Vacher-Lavenu MC, et al. Deeply infiltrating endometriosis: Pathogenetic implications of the anatomical distribution. Human Reproduction. 2006; 21(7): 1839-45. [ Links ]
17.TISSOT, M. et al. Clinical presentation of endometriosis identified at interval laparoscopic tubal sterilization: Prospective series of 465 cases. Journal of Gynecology Obstetrics and Human Reproduction, 46(8), 647-650, 2017. [ Links ]
18.BAZOT, M, I. et al. Diagnostic accuracy of transvaginal sonography for deep pelvic endometriosis. Ultrasound in Obstetrics and Gynecology, v.24, n.2, p.180-185, 2004. [ Links ]
19.Martinez, J. E., Centola Grassi, D., & Marques, L. G. (2011). Análise da aplicabilidade de três instrumentos de avaliação de dor em distintas unidades de atendimento: ambulatório, enfermaria e urgência. In Rev Bras Reumatol (Vol. 51, Issue 4). [ Links ]
20.Haefeli, M., & Elfering, A. (2006). Pain assessment. In European Spine Journal (Vol. 15, Issue SUPPL. 1). [ Links ]
21.Chamié, L. P. (2019). Ultrasound evaluation of deeply infiltrative endometriosis: technique and interpretation. Abdominal Radiology. [ Links ]
22.GUERRIERO, S. et al. Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis, including terms, definitions and measurements: a consensus opinion from the International Deep Endometriosis Analysis (IDEA) group. Ultrasound in Obstetrics & Gynecology, v. 48, n.3, p. 318-332, 2016. [ Links ]
23.Ros, C., Guirior, C., Mension, E., Rius, M., Valdés-Bango, M., Tortajada, M., Matas, I., Martínez-Zamora, M. Á., Gracia, M., & Carmona, F. (2021). Transvaginal ultrasound for the diagnosis of endometriosis in the uterosacral ligaments, torus uterinus and posterior vaginal fornix: a prospective study. Ultrasound in Obstetrics & Gynecology. [ Links ]
24.Leonardi, M., Martins, W. P., Espada, M., Arianayagam, M., &Condous, G. (2020). Proposed technique to visualize and classify uterosacral ligament deep endometriosis with and without infiltration into parametrium or torus uterinus. In Ultrasound in Obstetrics and Gynecology (Vol. 55, Issue 1, pp. 137-139). John Wiley and Sons Ltd. [ Links ]
25.BAZOT, M. et al. Diagnostic accuracy of physical examination, transvaginal sonography, ectal endoscopic sonography, and magnetic resonance imaging to diagnoses deep infiltrating endometriosis. Fertility and Sterility, v. 92, n.1, p.1825-1833, 2009. [ Links ]
26.MORGAN-ORTIZ, F. et al. (2018). Clinical characteristics and location of lesions in patients with deep infiltrating endometriosis using the revised Enzian classification. Journal of the Turkish German Gynecology Association, 20(3), 133-137. [ Links ]
27.Dovey, S., &Sanfilippo, J. (2010). Endometriosis and the adolescent. ClinicalObstetricsandGynecology, 53(2), 420-428. [ Links ]
28. Bazot, M., Lafont, C., Rouzier, R., Roseau, G., Thomassin-Naggara, I., Daraï, E. (2008). Diagnostic accuracy of physical examination, transvaginal sonography, rectal endoscopic sonography, and magnetic resonance imaging to diagnose deep infiltrating endometriosis. [ Links ]
29.HUDELIST, G. et al. Diagnostic delay for endometriosis in Austria and Germany: Causes and possible consequences. Human Reproduction, v.27, n.12, p.3412-3416, 2012. [ Links ]
30.GHAI, V. et al. (2020). Diagnostic delay for superficial and deep endometriosis in the United Kingdom. Journal of Obstetrics and Gynaecology, 40(1), 83-89. [ Links ]
31.NNOAHAM, K. E. et al. (2011). Impact of endometriosis on quality of life and work productivity: A multicenter study across ten countries. Fertility and Sterility, 96(2). [ Links ]
32.CHAPRON C. et al. Oral contraceptives (OC) and endometriosis: the past use of OC for treating severe primary dysmenorrheal appears as a marker associated with endometriosis, especially deep infiltrating endometriosis. HumReprod 2011; 26:2028e35. [ Links ]
33.Vercellini, P., Eskenazi, B., Consonni, D., Somigliana, E., Parazzini, F., Abbiati, A., & Fedele, L. (2010). Oral contraceptives and risk of endometriosis : a systematic review and meta-analysis. 00(0), 159-170. [ Links ]
34.PILLET, M. C. L.et al. (2014). A clinical score can predict associated deep infiltrating endometriosis before surgery for an endometrioma. 0(0), 1-11. [ Links ]
35.YONG, P. J. et al. (2015). Concurrent deep-superficial dyspareunia: Prevalence, associations and outcomes in a multidisciplinary vulvodynia program. The Journal of Sexual Medicine,12 (1), 219-227. [ Links ]
 Correspondence:
Correspondence:
Cicília Fraga Rocha Pontes
ciciliapontesradiologia@gmail.com
Manuscript received: may 2021
Manuscript accepted: december 2021
Version of record online: june 2022


{kind=link}
{kind=link}