










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.2 Santo André maio/ago. 2022
http://dx.doi.org/10.36311/JHGD.V32.13321
ORIGINAL ARTICLE
Factors associated with the leisure pratice of individuals on hemodialysis
Alexandre Cardoso da CunhaI; Edson Theodoro dos Santos NetoII; Monica CattafestaIII; Luciane Bresciani SalaroliIV
IFederal University of Espírito Santo, Health Science Center, Departament of Occupational Therapy
IIFederal University of Espírito Santo, Health Science Center, Departament of Social Medicine, Graduate Program in Public Health
IIIFederal University of Espírito Santo, Health Science Center, Graduate Program in Public Health
IVFederal University of Espírito Santo, Health Science Center, Departament of Integrated Health Education, Graduate Program in Public Health
ABSTRACT
INTRODUCTION: Leisure practices are complex activities involving several dimensions of human life such as social, cultural, and health. Using them to increase well-being and in situations of chronic diseases help in the adaptation to the disease
OBJECTIVE: This study analyzed factors associated with leisure practice in individuals on hemodialysis
METHODS: Data were collected by interview during hemodialysis sessions in a cross-sectional, census, with 1024 individuals. Socioeconomic factors, lifestyle, clinical and treatment characteristics were associated with leisure practices and their magnitudes were evaluated by binary logistic regression
RESULTS: We found that being 40 years of age or younger increased the odds of engaging in more leisure activities by 5.26 times (95% CI = 3.86-10.15), never having smoked increased the odds of engaging in more leisure activities by 2.12 (95% CI = 1.04-4.30). However, those who had eight years or less of education were 71.1% less likely to practice more leisure (OR = 0.289, 95%CI = 0.17-0.49
CONCLUSION: The factors associated with higher leisure practices of hemodialysis users are younger age, higher education, and absence of smoking, demonstrating the need to implement public policies to reduce health inequalities and increase leisure practices
Keywords: leisure activities, renal dialysis, social determinants of health, noncommunicable diseases, chronic kidney disease.
Authors summary
Why was this study done?
Leisure practices are complex activities involving several dimensions of human life such as social, cultural, and health. Using them to increase well-being and in situations of chronic diseases help in the adaptation to the disease. Individuals with chronic kidney disease who need hemodialysis have their lives impacted by social and cultural factors and leisure activities. This study was carried out to analyze the factors associated with the practice of leisure in individuals on hemodialysis.
What did the researchers do and find?
Authors interviewed 1024 individuals during hemodialysis and socioeconomic factors, lifestyle habits, clinical and treatment characteristics were associated with leisure practices. Its magnitudes were evaluated by binary logistic regression and found that the greatest leisure practices of hemodialysis users are younger age, higher education and absence of smoking.
What do these findings mean?
The main factors associated with leisure practices are socioeconomic factors and that the routines that hemodialysis impose do not prevent the performance of leisure activities. It is necessary to implement public policies to reduce health inequities and increase leisure practices and improve the well-being of this population.
INTRODUCTION
Chronic Kidney Disease (CKD) is a major public health problem and contributes significantly to the global burden of disease1. It is estimated that in 2017 there were 700 million people diagnosed with CKD in the world2. In Brazil in 2019, the estimated prevalence was 218 people per million, while the estimated incidence was 139.691 people. In the same year, 93.2% of the entire population on dialysis treatment were on hemodialysis3. This treatment interferes with users' social and cultural factors in such an important way that it influences their adherence to treatment and their leisure activities4.
Leisure encompasses complex activities with different dimensions of human life such as health, social and cultural factors. This relationship is described as complex, encompassing socio-economical issues5 to the point of decreasing socioeconomic inequalities in health6. They can include a wide range of options, such as physical activities and sports, theater, expressive and creative activities, and various hobbies. In this relationship, they can be used to benefit various dimensions of health6,7. In chronic disease situations, leisure is a way to improve adaptation to illness and increase well-being8.
The association between leisure, social factors and health are well known9, but research on leisure does not usually use an instrument that evaluates all the possibilities of activities and people's engagement. Some surveys only evaluate the prevalence of physical activities10, some specify the amount of time spent on activities to study people's motivation, but not engagement11 and also, those that research leisure based on qualitative methodologies12.
The positive association between leisure activities and quality of life is already known13 but, in the scientific literature, few investigations evaluate whether any characteristic of hemodialysis treatment may be related to the frequency of leisure practices. The researchers found to concentrate on investigating only leisure-time physical activities13,14 of individuals on hemodialysis, assessing the quality of life only by social and artistic activities13 and assessing whether assessing is a tool that can help improve user satisfaction with the hemodialysis service15.
Few studies evaluate leisure practices in all their dimensions, especially for individuals on hemodialysis. This evaluation may encompass subjective aspects of activity preferences, keeping the characteristics of freedom of choice that leisure has in its conception. In this context, we will describe which socioeconomic and lifestyle factors, and which clinical and treatment characteristics are associated with leisure practices in individuals on hemodialysis. Thus, the objective of this work is to analyze the factors associated with the practice of leisure in individuals on hemodialysis.
METHODS
Type of Study and Population
This is an epidemiological, cross-sectional, and census study. The study population consisted of individuals on hemodialysis in the Greater Vitória Metropolitan Region, Espírito Santo, Brazil (GVMR-ES). Participated in the research of all users of hemodialysis services in public and philanthropic entities, hospitals, and in private clinics convened in GVMR-ES of both genders, older than 18 years and in hemodialysis substitutive renal therapy between February and September 2019. Individuals who were under contact precaution, who did not reside in one of the municipalities of GVMR-ES, who were transferred to a hospital inpatient unit, and/or who had limitations in understanding or answering the questions due to some acute or chronic condition were excluded from the research.
Instrument
Data on socioeconomic characteristics, living habits, treatment, and clinical characteristics were collected. The data were categorized as follows:
(1) Socioeconomic characteristics: sex ("female" and "male"); age group ("18 to 39 years", "40 to 59 years" and "60 years or older"); self-reported race/color ("white", "black" and "brown")16; education in years of study ("up to eight years", "more than eight to 11 years" and "more than 11 years"); income in the minimum wage (MW) ("up to one MW", "more than one to two MW", "more than two to less than five MW" and "five or more MW"); marital status ("with partner" and "without a partner").
(2) Lifestyle characteristics: Drinking alcohol ("yes"/"no"); Smoker ("no, never smoked", "no, smoked in the past but quit" and "yes, regularly").
(3) Clinical and treatment characteristics: Self-reported diseases ("two or less" and "three or more"); Medications used ("less than five" and "five or more"); Self-reported intradialytic complications ("none", "one to three" and "three or more"); Time of chronic kidney disease ("less than five years" and "five years or more"); Time of hemodialysis ("less than two years" and "two years or more"); City of treatment and residence ("same city" and "other city"); Type of care ("public", "private" and "mixed"); Shift that performs hemodialysis ("morning", "afternoon" and "evening").
To measure the dependent variable, Leisure Practices, the Leisure Practices Scale17 was used. It is a Likert-type scale that evaluates eight leisure domains: artistic (going to the movies, theater, musical shows, participating in choir groups, etc.), manual (gardening, cooking, crafting, woodworking, etc.), physical sports (going to the gym, playing ball, hiking, etc.), intellectual (participating in courses, reading, listening or composing music, etc.), social (going to church, going out with friends, going to parties, visiting family, etc), tourism (traveling, participating in excursions, virtual (surf the internet, use social networks, play video games), leisure and contemplation (enjoy nature, the sunset, meditate, etc) with 11 points (from zero to ten, where zero means that the user never practices and ten that he always practices). The answers from the eight domains were added to get the result of the leisure practice scale, which can vary from zero to 80 points and dichotomized into "equal to or below the median" / "above the median" which were, respectively, denominated as "less leisure" and "more leisure".
Data Collection
Data collection occurred between February and September 2019, on the premises of the hemodialysis units, during the period of the individual's stay in the health service.
A pilot test was conducted in the format of a test and retest, in a 15-day interval, to assess the reliability and reproducibility of the data collection instrument. Fifty-eight individuals with CKD on the hemodialysis treatment in Colatina, a city with more than 100 thousand inhabitants located outside the GVMR-ES (and not included in the research sample) participated. Kappa and McNemar test statistics were performed. The adjusted Kappa values for the variables of the instrument ranged from 0.89 to 0.99, which expresses an almost perfect agreement, and in the McNemar tests no variable showed a significant tendency to disagree at a p-value <5%.
Data Analysis
The normality of the variables was assessed using the Kolmogorov-Smirnov test. The descriptive analysis was presented as absolute and relative frequencies. Pearson's chi-square test was used to calculate the difference between the proportions of leisure time practice (less leisure and more leisure) and the other variables. To calculate the odds ratio, we used the binomial logistic regression model. We included those with statistical significance up to 5% in the association test and that did not present collinearity. The significance level was set at 5% and the 95% confidence interval (95%CI). Data were analyzed using IBM SPSS Statistic22.
Ethical and Legal Aspects of the Research
The research was approved by the Research Ethics Committee of the Health Sciences Center of the Federal University of Espírito Santo (UFES), under number 3.002.709 and CAAE 68528817.4.0000.5060 and met the criteria of Resolution No. 466/2012 of the National Health Council. The individuals on hemodialysis who agreed to participate in the research signed the Informed Consent Form (ICF) before answering the questionnaire.
RESULTS
We identified 1351 users in the hemodialysis units of GVMR-ES. Of these, 215 were excluded (137 for being in contact precaution and 78 with comprehension limitations or to answer the questionnaire) and there were also 89 losses (67 for being admitted to other hospital units, besides 15 who died and seven who were transferred from the hemodialysis unit before data collection). Of the 1047 eligible individuals, 23 (2.2%) refused to participate. The population of this study was thus constituted of 1024 individuals on hemodialysis.
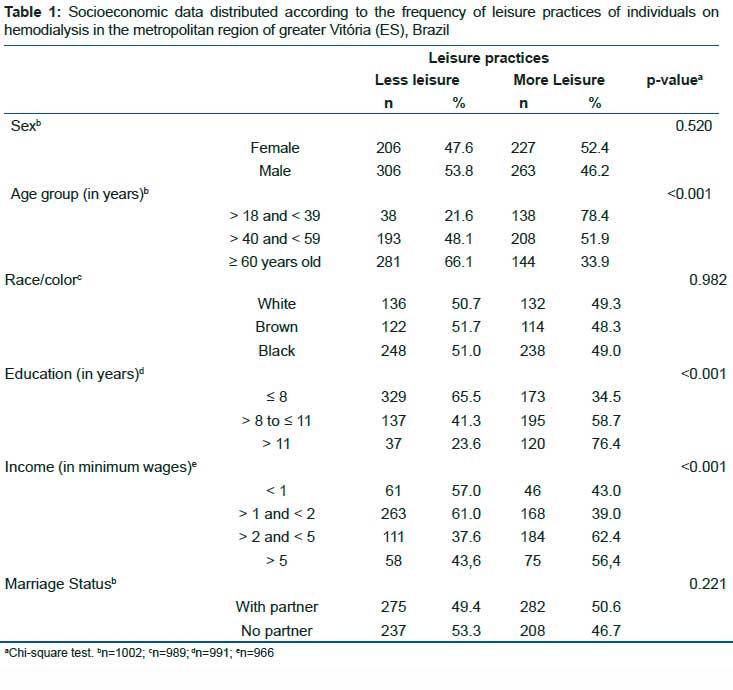
In the bivariate analyses, we observed that leisure practices were associated with some socioeconomic variables. The greatest involvement in leisure activities was associated with being 18 to 40 years old (p<0.001), having 11 or more years of schooling (p<0.001), and receiving more than two to five minimum wages (p<0.001) (table 1).
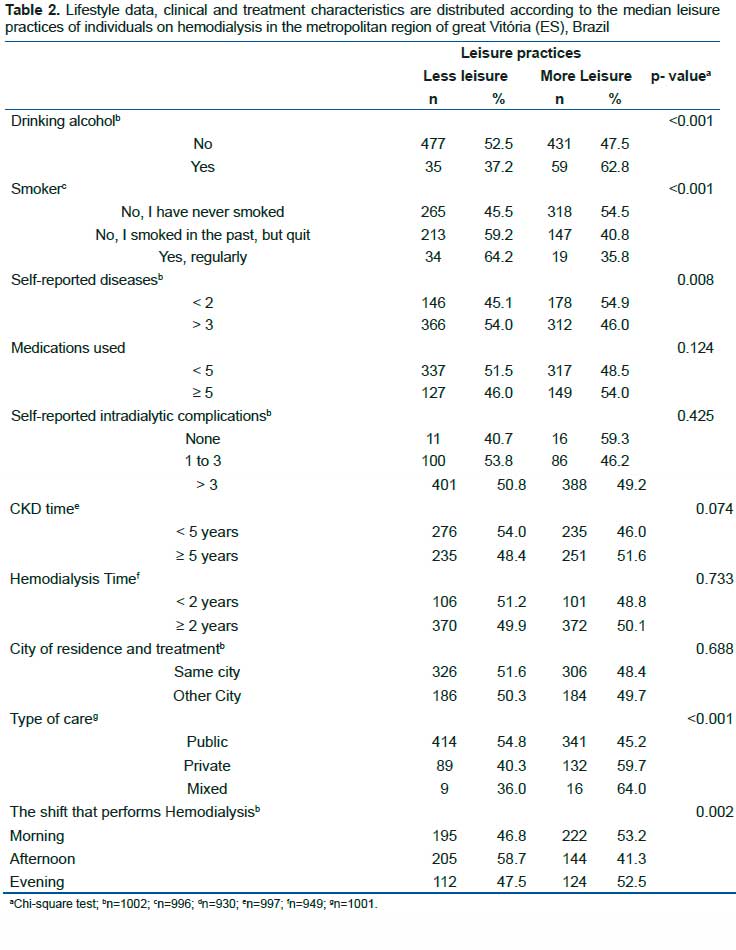
For individuals on hemodialysis an association of higher leisure practices was observed with the consumption of alcoholic beverages (p=0.005) and with never having smoked (p<0.001) (table 2).
Greater leisure practices were observed among individuals on hemodialysis who self-reported fewer diseases (p=0.008), those who used the private treatment system modality (p<0.001), and those who performed hemodialysis in the morning or evening shifts (p=0.002) (table 2).
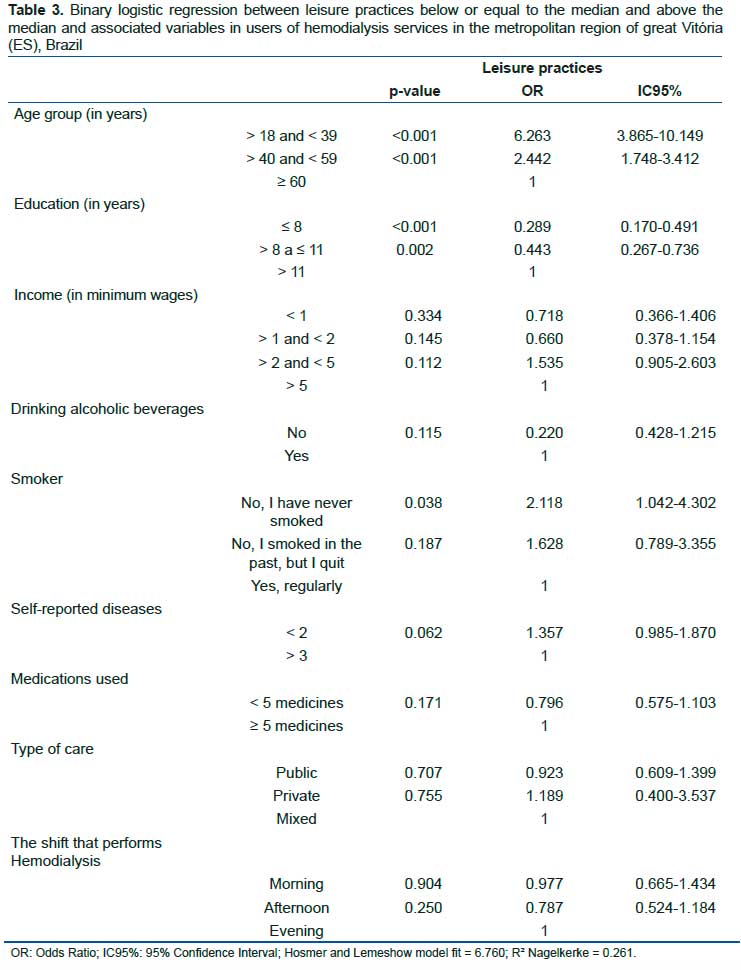
Table 3 presents the regression with the variables that presented a p-value lower than 0.05 in the bivariate analysis. Age group, education, and smoking remained associated with leisure practices.
Binary logistic regression showed that being less than 40 years old increases the odds (95%CI= 3.413-9.252) by 6.26 times and being between 40 and less than 59 years old increases the odds (95%CI= 1.748-3.412) of practicing more leisure activities by 2.44 times when compared to individuals aged 60 years or older. The individuals on hemodialysis who had less than eight years of the study presented 71.1% fewer chances (95%CI= 0.166 - 0.493) and those with more than eight to 11 years of the study presented 55.7% fewer chances (95%CI= 0.267-0.736) of being in the group that practice more leisure when compared to individuals with 8 years or less of study.
For lifestyle variables, users who reported never having smoked were 2.8 times more likely (95% CI= 1.301-6.051) to practice leisure time above the median. No variables among those configuring clinical and treatment characteristics were significant after adjustment.
DISCUSSION
This work was organized to identify and analyze the factors associated with the practice of leisure in individuals on hemodialysis. Thus, elements linked to the daily life of hemodialysis treatment, clinical characteristics, lifestyle, and socioeconomic habits were investigated.
Leisure is described in the literature as capable of helping in health, adaptation to chronic diseases, and well-being. Using an instrument that addresses the 8 dimensions of leisure in research with hemodialysis users is unprecedented and helps to explain the contradiction that the literature points out about the frequency of leisure practices in this population. It should be noted that presenting associations of clinical characteristics and treatment of this population is also unprecedented and contributes to the hemodialysis service teams guiding their users based on the scientific literature.
The results show that the factors associated with more leisure practices of individuals on hemodialysis are age, level of education, and smoking habit, and then, the groups that most practice leisure activities are young adults, with higher levels of education and who did not smoke. However, it is important to point out that this study used an instrument to evaluate leisure practices never used before with the study population, which points to greater caution in comparing results for analysis.
The main finding of this work is that the results of the final adjusted model indicate that clinical and treatment characteristics do not affect the leisure practices of individuals on hemodialysis in their different contexts. Although we did not find research in the literature that specifically investigates this relationship, some articles use the impact of these treatment characteristics on patients' lives to justify lifestyle studies18. Socioeconomic inequalities hinder more the realization of leisure practices than the treatment routine, which gives indications that if the subject can organize himself to enjoy leisure moments, the heavy routine that a hemodialysis treatment imposes may be overcome.
In the present study lower levels of education are related to lower levels of leisure practices. This association is also found in studies that investigated only the elderly19 or only adults20. Low education, besides being a barrier to leisure19 is associated with lower cognitive levels and impairment in social functions of hemodialysis users21, which may cause users to have fewer internal resources to cope/practice more domains of leisure and adjust them to the reality they live after the disease has been diagnosed and treatment has started.
Although some studies indicate that low income is a limiting factor for the access to leisure18, it was not verified any association between the frequency of leisure practices and income. Manual, social and virtual activities are more practiced by people with lower income and less education, and on the other hand, artistic activities are performed by people with higher education, as well as tourism activities are more practiced by people with higher income22. The sum of the answers of all the domains may have masked the relations of each domain with income, which may explain the result found.
The findings corroborate with the scientific literature, that older people have fewer leisure practices. The increase in age is a factor that decreases the chances of performing sports-physical leisure activities23 and increases the sedentary leisure time4. It is also important to consider that the senescence process increases the possibility of sarcopenia, and in individuals on hemodialysis, this is an important functional limiting factor24. The changes that the body presents in the senescence process, added to those provided by CKD and the psychological effect of long periods in a treatment environment, often only reinforce a new place in the world: that of being sick. The process of becoming ill has a lot of pain, suffering, and doubts about the diagnosis25. This framework associated with setting a preference for certain domains of leisure may impact the decrease in leisure practices by older people.
Leisure can be a helping element in changing this picture because it is a fundamental process that collaborates in the construction of meanings of the "art of life"26 and can help the person not only to experience/be in the everyday life, but to overcome the feeling of being sick by the hope in the future and also to renew the meaning of his existence27, providing a better quality of life8.
Never having smoked was positively associated with higher leisure practices in this study. Although the habit of smoking is associated with sedentary leisure28, many other activities open themselves as leisure possibilities. This result can be explained by the fact that hemodialysis service users, due to chronic kidney disease, are exposed to a lot of information and guidance about food and healthy habits and people who do not smoke have more chances to adhere to healthy eating patterns29, which can increase the sense of well-being and willingness to varied leisure activities.
In this sense, it is noted that the leisure practices of individuals on hemodialysis need more attention from health professionals. Hemodialysis generates important changes in people's lives, in their daily lives, in their work/study, and their eating habits. The hemodialysis service teams must have professionals who understand the importance of leisure activities and their potential to facilitate the management of symptoms, improve well-being, and adapt to life with a chronic disease.
As the main limitation of this study we can point out the difficulty of studying behavioral characteristics quantitatively, however, it is important because it is unprecedented research in the literature, being one of the few studies that investigate the leisure of individuals on hemodialysis with an instrument with the 8 domains of leisure practices. Another limitation is, in a cross-sectional study, establishing temporal causality between the associations. We also understand that by using the Leisure Practices Scale considering the totality of the 8 domains, the possibility of discussing the different characteristics of each of the eight leisure domains and their associations with the variables studied was diminished. However, the form of analysis adopted values the variety of leisure practices, considering them as a personal (or collective) choice, free and that generates pleasure.
CONCLUSION
This work sought to study the association of socioeconomic factors, lifestyle habits, clinical characteristics, and hemodialysis treatment to the leisure practices of individuals on hemodialysis. All individuals under treatment for GVMR-ES, in the period from February to September 2019, were interviewed and based on Pearson's Chi-square result, the binomial logistic regression model was assembled to estimate the odds ratio of each factor in leisure practices.
Based on the results, it is possible to infer that the factors associated with higher leisure practices of individuals on hemodialysis are socioeconomic factors. Being less than 40 years old and not yet experiencing the decline in body functionality that senescence produces is one of the factors that contribute to greater leisure practices. Another factor identified by the research is the higher level of education that is associated with lower cognitive levels and impairment in social functions as limiting such practices.
Another factor associated with higher leisure practices was the habit of not smoking. The exposure to the various guidelines and recommendations for healthy habits and care regarding CKD that the individual on hemodialysis receives. This may increase the periods of the feeling of well-being that facilitate leisure practices.
The main finding is that, unlike the initial hypothesis of the research, the clinical characteristics and treatment were not associated with the leisure practices of the individual on hemodialysis. Despite the constant treatment routine, individuals on hemodialysis find ways to participate in leisure activities and live a life that is not centered only on the disease. These findings indicate the importance of having public policies that favor the reduction of social and health inequalities and that are aimed at promoting leisure practices in this population. It also points to the need for hemodialysis service teams to have professionals who can perform interventions to expand such practices and favor an increase in the well-being of people who are on treatment.
Author Contributions
Conceptualization, A.C.C.; methodology, A.C.C., L.B.S. e E.T.S.N.; formal analysis, A.C.C.; writing- original draft preparation, A.C.C.; writing-review and editing, L.B.S., E.T.S.N., and M.C.; supervision, L.B.S. and E.T.S.N.; project administration, L.B.S.; funding acquisition, L.B.S. and E.T.S.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Fundação de Amparo à Pesquisa do Espírito Santo (FAPES), grant number 83164324.
Conflicts of Interest
The authors declare no conflict of interest.
REFERENCES
1.Murray CJL, Aravkin AY, Zheng P, Abbafati C, Abbas KM, Abbasi-Kangevari M, et al. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet 2020; 396: 1223-49. DOI: https://doi.org/10.1016/S0140-6736(20)30752-2 [ Links ]
2.GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020; 395: 709-33. DOI: https://doi.org/10.1016/S0140-6736(20)30045-3 [ Links ]
3.Neves PDM de M, Sesso R de CC, Thomé FS, Lugon JR, Nascimento MM. Brazilian dialysis survey 2019. Braz J Nephrol 2021; 43: 217-27. DOI: https://doi.org/10.1590/2175-8239-JBN-2020-0161 [ Links ]
4.Lee EJ, Chang AK, Chung YC. Socioecological Factors Affecting Fluid Restriction Adherence Among Korean Patients Receiving Hemodialysis: A Qualitative Study. J Transcult Nurs 2021; 32: 239-47. DOI: https://doi.org/10.1177/1043659620919162 [ Links ]
5.Mansfield L. Leisure and health - critical commentary. Annals of Leisure Research 2021; 24: 283-94. DOI: https://doi.org/10.1080/11745398.2020.1767664 [ Links ]
6.Straker L, Holtermann A, Lee I-M, van der Beek AJ, Stamatakis E. Privileging the privileged: the public health focus on leisure time physical activity has contributed to widening socioeconomic inequalities in health. Br J Sports Med 2020: bjsports-2020-103356. DOI: https://doi.org/10.1136/bjsports-2020-103356 [ Links ]
7.Young J, Maxwell H, Peel N. Leisure meets health: important intersections and alternative discourses. Annals of Leisure Research 2021; 24: 275-82. DOI: https://doi.org/10.1080/11745398.2020.1836666 [ Links ]
8.McQuoid J. Finding joy in poor health: The leisure-scapes of chronic illness. Soc Sci Med 2017; 183: 88-96. DOI: https://doi.org/10.1016/j.socscimed.2017.04.044 [ Links ]
9.Lima MG, Malta DC, Monteiro CN, Sousa NF da S, Stopa SR, Medina L de PB, et al. Correction: Leisure-time physical activity and sports in the Brazilian population: A social disparity analysis. PLOS ONE 2020; 15: e0228095. DOI: https://doi.org/10.1371/journal.pone.0228095 [ Links ]
10.Martins RC, Silva ICM da, Hallal PC. Physical activity in the rural population of Pelotas, Brazil: prevalence and associated factors. Revista de Saúde Pública 2018; 52: 9s-9s. DOI: https://doi.org/10.11606/S1518-8787.2018052000265 [ Links ]
11.Chen M, Xue S, Shi Y. Leisure activities and leisure motivations of Chinese residents. PLOS ONE 2018; 13: e0206740. DOI: https://doi.org/10.1371/journal.pone.0206740 [ Links ]
12.Paudel S, Owen AJ, Smith BJ. Socio-ecological influences of leisure-time physical activity among Nepalese adults: a qualitative study. BMC Public Health 2021; 21: 1443. DOI: https://doi.org/10.1186/s12889-021-11484-3 [ Links ]
13.Agadayi E, Dede F, Coskun Yenigün E, Köksal Cevher S, Sencan i, Özkara A. The effects of artistic and social activities during hemodialysis on the life quality, pain perception, anxiety status of the patients and intradialytic complications. FAMILY PRACTICE AND PALLIATIVE CARE. 2019, Aug 30; 4 (2): 46-50. [ Links ]
14.Ghafourifard M, Mehrizade B, Hassankhani H, Heidari M. Hemodialysis patients perceived exercise benefits and barriers: the association with health-related quality of life. BMC Nephrol 2021; 22: 94. DOI: https://doi.org/10.1186/s12882-021-02292-3 [ Links ]
15.Pedreira-Robles G, Vasco-Gómez A, Martínez-Delgado Y, Herrera-Morales C, Baz-Rodríguez MT, Junyent-Iglesias E, et al. Déficit de actividades recreativas en hemodiálisis. Satisfacción y coste económico ante un proyecto lúdico terapéutico. Enfermería Nefrológica 2020; 23: 83-92. DOI: https://doi.org/10.37551/s2254-28842020010 [ Links ]
16.IBGE. Pesquisa nacional por amostra de domicílios: síntese de indicadores 2015 [Internet]. Rio de Janeiro: Coordenação de Trabalho e Rendimento; 2016. 108 p. DOI: https://biblioteca.ibge.gov.br/visualizacao/livros/liv98887.pdf [ Links ]
17.Andrade RD, Schwartz GM, Tavares GH, Pelegrini A, Teixeira CS, Felden ÉPG. Validade de construto e consistência interna da Escala de Práticas no Lazer (EPL) para adultos. Ciênc saúde coletiva 2018; 23: 519-28. DOI: https://doi.org/10.1590/1413-81232018232.11492016 [ Links ]
18.Sarah Teixeira Soutto Mayor, Hélder Ferreira Isayama. O lazer do brasileiro: sexo, estado civil e escolaridade. In: Edmur Antonio Stoppa, Hélder Ferreira Isayama, editors. Lazer no Brasil: representações e concretizações das vivências cotidianas. 1st ed. Campinas: Autores Associados; 2017. p. 19-36. [ Links ]
19.Pitilin E de B, Massaroli A, Luzardo AR, Lentsck MH, Baratieri T, Gasparin VA. Factors associated with leisure activities of elderly residents in rural areas. Rev Bras Enferm 2020; 73 Suppl 3: e20190600. DOI: https://doi.org/10.1590/0034-7167-2019-0600 [ Links ]
20.Kim J, Heo J, Dvorak R, Ryu J, Han A. Benefits of leisure activities for health and life satisfaction among Western migrants. Annals of Leisure Research 2018; 21: 47-57. DOI: https://doi.org/10.1080/11745398.2017.1379421 [ Links ]
21.Pretto C, Winkelmann ER, Hildebrandt LM, Barbosa D, Colet C, Stumm E. Quality of life of chronic kidney patients on hemodialysis and related factors*. Revista Latino-Americana de Enfermagem 2020. DOI: https://doi.org/10.1590/1518-8345.3641.3327 [ Links ]
22.Andrade RD, Schwartz GM, Felden ÉPG. Variáveis Socioeconômicas e o Envolvimento no Lazer. Licere 2018; 21. DOI: https://doi.org/10.35699/1981-3171.2018.1779 [ Links ]
23.Casas RCRL, Bernal RTI, Jorge A de O, Melo EM de, Malta DC. Fatores associados à prática de Atividade Física na população brasileira - Vigitel 2013. Saúde debate 2018; 42: 134-44. DOI: https://doi.org/10.1590/0103-11042018S410 [ Links ]
24.Kittiskulnam P, Chertow GM, Carrero JJ, Delgado C, Kaysen GA, Johansen KL. Sarcopenia and its individual criteria are associated, in part, with mortality among patients on hemodialysis. Kidney Int 2017; 92: 238-47. DOI: https://doi.org/10.1016/j.kint.2017.01.024 [ Links ]
25.Berardinelli LMM, Santos I dos, Santos MLCS dos, Lima TCL, Missio AC, Berardinelli LM. Identificando vulnerabilidade para complicações cardiovasculares em idosos: uma estratégia para o cuidado. Rev Enferm UERJ 2011: 541-6 [ Links ]
26.Bouwer J, Leeuwen M van. Philosophy of Leisure: Foundations of the Good Life. London: Routledge; 2018. DOI: https://doi.org/10.4324/9781315692647 [ Links ]
27.Sá M do C, Nabais AS. Fronteiras entre saúde e doença para pessoas que vivem com Doença Crónica. New Trends in Qualitative Research 2021; 8. DOI: https://doi.org/10.36367/ntqr.8.2021.637-644 [ Links ]
28.Zheng Y, Cai G-Y, Chen X-M, Fu P, Chen J-H, Ding X-Q, et al. Prevalence, awareness, treatment, and control of hypertension in the non-dialysis chronic kidney disease patients. Chin Med J (Engl) 2013; 126: 2276-80. [ Links ]
29.Gomes AP, Bierhals IO, Vieira LS, Soares ALG, Flores TR, Assunção MCF, et al. Padrões alimentares de idosos e seus determinantes: um estudo de base populacional. Ciência and Saúde Coletiva 2020; 25: 1999-2008. DOI: https://doi.org/10.1590/1413-81232020256.20932018 [ Links ]
 Correspondence:
Correspondence:
Alexandre Cardoso da Cunha
accunhato@gmail.com
Manuscript received: may 2021
Manuscript accepted: december 2021
Version of record online: june 2022


{kind=link}
{kind=link}
{kind=link}