










Serviços Personalizados
artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.2 Santo André maio/ago. 2022
http://dx.doi.org/10.36311/jhgd.v32.13228
ORIGINAL ARTICLE
Measuring harm-free care in childbirth: a pilot application of the Maternity Safety Thermometer in Brazil
Bruna Dias AlonsoI; Denise Yoshie NiyII; Cláudia de Azevedo AguiarIII; Eder Lucio da FonsecaIV; Jane SandallV; Carmen Simone Grilo DinizVI
IRM, BSc, MSc, PhD. Department of Health, Life Cycles, and Society; School of Public Health, University of São Paulo, Brazil. Midwifery course; School of Arts, Sciences and Humanities, University of São Paulo, Brazil. Nursing and Medicine courses; FAM, Brazil
IIMSc, PhD. Department of Health, Life Cycles, and Society; School of Public Health, University of São Paulo, Brazil
IIIBSc, MSc, PhD. Department of Public Health, Federal University of Triângulo Mineiro, Brazil
IVMSc, PhD. John P. Hussman Institute for Human Genomics, Miller School of Medicine, University of Miami, USA
VBSc, MSc, PhD. Department of Women and Children's Health, Faculty of Life Sciences and Medicine, King's College London, UK
VIMD, MSc, PhD. Department of Health, Life Cycles, and Society; Public Health School of University of São Paulo, Brasil
ABSTRACT
INTRODUCTION: interventions during labour and childbirth are frequently unnecessary and can be harmful to most women and babies in Brazil. In addition, there is a high prevalence of abuse and disrespect situations
OBJECTIVE: to describe the prevalence of maternal and neonatal harm and harm-free care in a Brazilian maternity setting
METHODS: pilot application of the Portuguese version of Maternal Safety Thermometer (MST) by a cross-sectional study in a public setting. Data collection was made at two timepoints
RESULTS: 140 women were included. Over 84% of women had a postpartum sutured wound, resulting from a caesarean section, an episiotomy, or a perineal trauma. Puerperal infection, especially on a caesarean wound, was the most frequent physical harm. Women's perception of safety, including being left alone in labour, and feeling their safety concerns were not taken seriously, decreased from 80.6% to 43.3% in the second timepoint. Using the MST helped to improve the quality of medical records since critical information about a patient's health status was not properly recorded, or even absent
CONCLUSION: MST is a concise tool which includes indicators related to harm-free care measured in a short time range. However, this study suggests that the MST can underestimate harm if it is used alone to assess harm-free care in maternities with excessive levels of intervention, and poor reporting of harms (i.e., blood loss), as in most Brazilian settings
Keywords: Childbirth, Hospitals, Maternity, Patient Safety, Outcome Assessment, Health Care.
RESUMO
INTRODUÇÃO: No Brasil, as intervenções durante o parto e o nascimento são prejudiciais e, em sua maioria, desnecessárias. Além disso, é alta a prevalência de abusos e desrespeito à mulher e ao bebê neste período
OBJETIVO: Descrever a prevalência dos danos maternos e neonatais, e do cuidado livre de danos em uma maternidade brasileira
MÉTODO: Estudo transversal, com aplicação piloto, em português, do Termômetro de Segurança da Maternidade (TSM) em uma instituição pública. A coleta de dados foi realizada em dois momentos
RESULTADOS: 140 mulheres foram incluídas. Mais de 84% delas deixaram a maternidade com algum tipo de ferida suturada, resultante de cesariana, episiotomia ou outro trauma perineal. Infecção puerperal, principalmente na incisão da cesariana, foi o dano físico mais frequente. A percepção de segurança das mulheres - incluindo ficar sozinha no trabalho de parto e sentir que suas preocupações com relação à segurança não foram consideradas - diminuiu de 80,6% para 43,3% no segundo momento. O uso do TSM ajudou a melhorar a qualidade dos registros em prontuário, dado que, informações importantes sobre a condição das pacientes não eram registradas adequadamente ou estiveram ausentes
CONCLUSÃO: O TSM é uma ferramenta concisa que possibilita descrever o cuidado livre de danos rapidamente. No entanto, este estudo sugere que, se usado isoladamente, o TSM pode subestimar danos em serviços com níveis excessivos de intervenção e com registros inadequados de danos (exemplo, perda sanguínea), como é o caso da maioria das maternidades brasileiras
Palavras-chave: Parto, Maternidades, Segurança do Paciente, Avaliação de Resultados em Cuidados de Saúde.
Authors summary
Why was this study done?
This study is based on the concern about the high prevalence of non-justified childbirth interventions in Brazil, as well as abuse and disrespectful situations. Identifying the harm-free care experienced by women, using the Maternity Safety Thermometer (MST), can be an important resource to understand the childbirth model of care.
What did the researchers do and find?
It was conducted a pilot application of the Portuguese version of MST by a cross-sectional study in a public maternity hospital at two timepoints. We noticed that a significant number of women suffered some kind of harm during labour.
What do these findings mean?
MST is a concise tool which includes indicators related to harm-free care in a short time range. However, this study suggests that the MST can underestimate harm in Brazilian settings if it is used alone.
INTRODUCTION
In Brazil, 98% of women give birth with skilled professionals in a healthcare facility1. However, rates of harmful and mostly unnecessary interventions are high2, besides the high prevalence of abuse and disrespectful situations during childbirth3,4. Moreover, Brazil failed to achieve the UN's Millennium Development Goal 5, as the maternal mortality rate remains unacceptably high (more than 60 per 100,000 live births in 2017)5. Most women do not have access to evidence-based care, which can be confirmed by the high rates of caesarean section, which reached 56.3% in 20191.
The excess of caesarean section in Brazil has been concerning since the 1980s. Public policies and government programs have addressed maternal and women's health, but the challenge of reducing unnecessary interventions prevails. A national survey on childbirth care showed that many low-risk women suffer interventions, such as labour stimulation with oxytocin (38.2%) and amniotomy (40.7%). Of those who have a vaginal birth, 37.3% suffer Kristeller maneuver, 56.1% have an episiotomy and 91.7% give birth in lithotomy position2. The overmedicalization of childbirth results in a context where it is exceptional to experience a vaginal delivery without interventions since: only 5.6% of all low-risk women are discharged without a wound caused by assistance2. Therefore, the concept of a harm-free care6 is highly counter-hegemonic7, depicting a situation that Miller et al.8 have named as "too much too soon", referring to the "unnecessary use of non-evidence-based interventions, as well as the use of interventions that can be life-saving when used appropriately, but harmful when applied routinely or overused".
Several factors can explain the Brazilian context, including the underfunding of the public health sector, as well as the existence and expansion of a private sector, which is not duly supervised nor regulated9. Thus, if the public sector faces problems such as lack of human resources9, the private sector adopts a model of care based on caesarean section for almost every woman2. As far as equity is one of the principles of the Brazilian Unified Health System (SUS), which includes the public and private sectors, there is an understanding that "the health system must go beyond universal, unregulated access to technology, and move towards safe, effective and transparent care"10.
The Brazilian Ministry of Health launched the National Patient Safety Program in 2013, which is supervised by the National Health Surveillance Agency (ANVISA). According to the ANVISA, safety is "the reduction, to an acceptable minimum, of the risk of unnecessary harm associated with health care"11. The The ANVISA recognizes that the health system frequently fails to offer safe maternity care, due to inadequate facility infrastructure or errors in the work process, among other factors, and states that "inadequate care is not able to reduce harms it has caused, in addition to potentiating them, often resulting in preventable death of women and children or permanent injuries and sequelae"12. These concepts are aligned to the WHO's vision of safety, which adds the need to avoid preventable injuries and reduce medical errors13.
The Maternity Safety Thermometer (MST) was created and tested by the English National Health Service (NHS), between 2013 and 2014, as a tool to quickly assess the prevalence of maternal and neonatal health harms14. It was inspired by the Safety Thermometer (ST), created in 2011 by NHS, which estimates the prevalence of health harm at a one-time point and, like a thermometer, indicates combined outcomes in a short time range6. The ST, as well as the MST, allows identifying the most frequent harm in a hospital and the number of patients who were benefited from harm-free care6.
There are few scientific publications concerning the MST in any language, especially in low- and middle-income settings. Melo15 proposed a cross-cultural translation and adaptation of the MST into Brazilian Portuguese language and used it in three hospitals in Northeastern Brazil, and Salgado et al.16 have made use of this tool version with secondary analysis of data from a previous national survey (Birth in Brazil survey). This study aims to describe the prevalence of maternal and neonatal harm, and harm-free care in a Brazilian maternity setting according to the pilot application of MST.
METHODS
Study Design
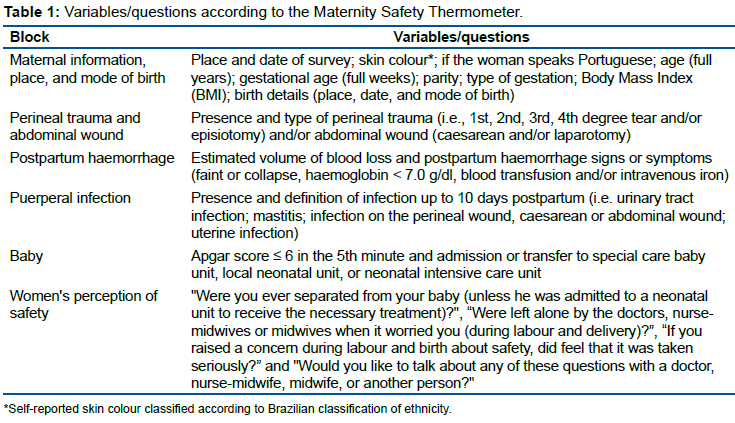
This is a cross-sectional study, with data collected through the cross-cultural adaptation of the MST to the Brazilian Portuguese language15. MST covers information regarding 1) Place and mode of birth, 2) Perineal trauma and abdominal wound, 3) Postpartum haemorrhage, 4) Puerperal infection, 5) Apgar score and term newborn transfer, 6) Women's perception of safety. Thus, it constitutes three types of indicators: physical harm-free care, harm-free care reported by women according to their perception of safety, and combined harm-free care14.
This study is part of the HAMABE Research project17 which aimed to develop and evaluate the sustainability of a participatory implementation of the Mother-Baby Friendly Birthing Facilities Initiative18 (later called International Childbirth Initiative) in two Brazilian SUS settings in São Paulo State/Brazil. HAMABE project was based on Change Laboratory methodology19 which includes a cycle of sessions to make empirical observations of workplace activity systems. Working group meetings - composed of representatives of the maternity hospital's users, researchers, clinicians, and managers - took place periodically in 2017-2018, when setting observation findings and quantitative indicators were discussed, as well as women's demands, and contradictions and tensions in the activity system. Data from MST was used as one of the resources, like "mirrors" data. This research was carried out in a maternity service located in the city of São Paulo/Brazil, which is part of SUS and is currently managed by a private institution. It provides care to low-risk women, who are assisted mostly by nurse-midwives. There is an alongside birth centre, surgical theatre, postpartum rooming-in care, and neonatal intensive care unit. It was a training ground for some undergraduates and postgraduates in the health area until 2017, but the training program was discontinued, for patient safety reasons. In 2016, it registered 5,359 live births, of which 69% were vaginal deliveries1.
Study Population and Eligibility Criteria
All women with newborns (regardless of weight and gestational age at birth) or stillbirths (weight ≥500 grams and/or gestational age ≥22 weeks) were included. Women under 18 years old who did not have a parent or guardian present, as well as women who did not understand Portuguese and did not have a translator, were excluded.
Data Collection
Data collection was made at two timepoints, one in May 2017 (time 1) and another in June 2018 (time 2). In each period, during five consecutive days, all the eligible women who consented to take part in the research were interviewed at least 12 hours after birth (convenience sampling).
Data were also extracted from medical records and Body Mass Index (BMI) information was collected from prenatal cards when available because such information was not recorded in hospital records.
Between 10 and 15 days postpartum, the participants were interviewed via telephone (4 attempts on different days and at different times) as a way of tracking infection cases. If the woman said that she had a puerperal infection (i.e., urinary tract infection; mastitis; infection on the perineal, caesarean or abdominal wound; uterine infection), the research staff also asked if she had pain, redness, purulent discharge, fever, and/or if she took antibiotic prescribed by a physician16. Women with these signs and symptoms were urged to seek medical assistance. A telephone approach was considered, as adherence to postpartum consultation is low20 and women could follow different care pathways from those established by SUS as postpartum reference.
The research staff responsible for collecting the data was composed of undergraduate students in Midwifery and Nutrition, as well as postgraduate students in Public Health. All of them received prior training specific to MST.
The MST variables were grouped into six blocks according to table 1. The MST source of information was the medical records, except the block "Women's perception of safety", which is about women's perspective of care during an interview before maternity discharge, and the questions on puerperal infection cases in postpartum telephone interviews.
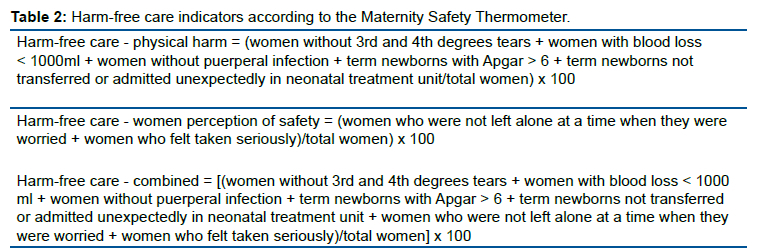
The most serious harms were: 3rd and 4th degrees tears, postpartum haemorrhage ≥1,000 ml, puerperal infection, Apgar ≤6 in the 5th minute in term newborns, unexpected transfer of term newborns for neonatal treatment units, women left alone at a time when they were concerned, and women felt not taken seriously. Finally, the following indicators were established: physical harm-free care, harm-free care reported by women according to their perception of safety, and combined harm-free care (table 2).
Data Analysis
The data was typed into Microsoft Excel® with double-entry to avoid typing errors. Absolute and relative frequencies of each variable, prevalence of harms, and harm-free care indicators were calculated. All analyses were conducted using the software SPSS® 22 (SPSS Inc, Chicago, USA).
Ethical and Legal Aspects of the Research
This study has been approved by the Research Ethics Committee of FSP/USP (CAAE 56958716.0.1001.5421).
RESULTS
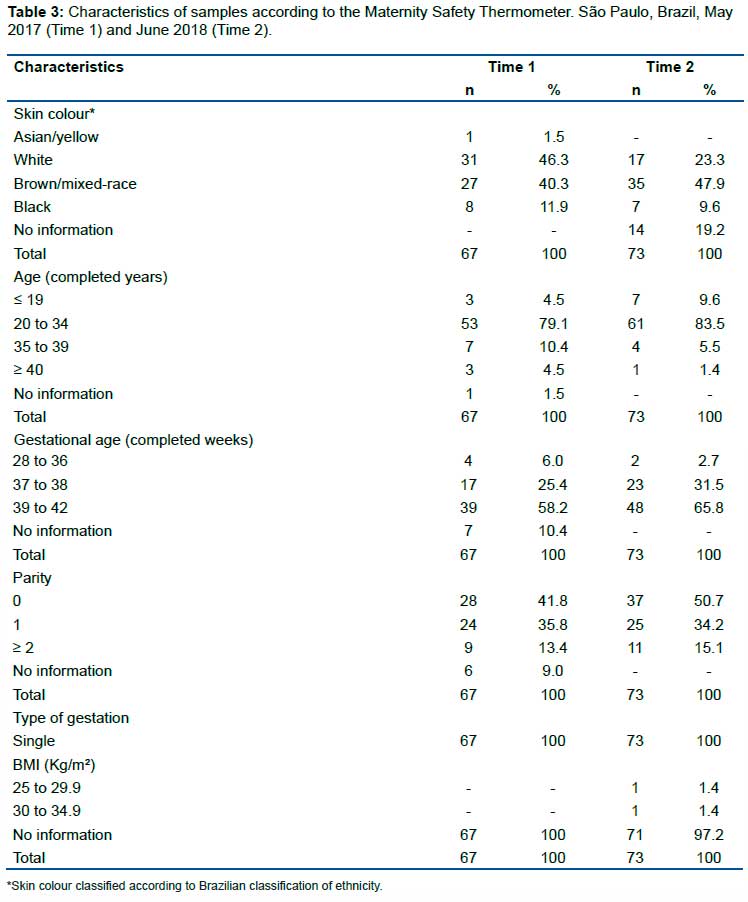
In May 2017, 77 women were eligible for this study. However, ten women were excluded (seven of them were under 18 years old and were not emancipated or did not have the presence of a legal guardian, one did not understand Portuguese as well as did not have a translator, and two did not consent to participate in the study), totalling 67 women in time 1. In June 2018, 76 women were eligible for this study. Two of them did not consent to participate in the research and one did not understand Portuguese and did not have a translator. Therefore, time 2 was composed of 73 women. Details of samples on time 1 and 2 are presented in table 3.
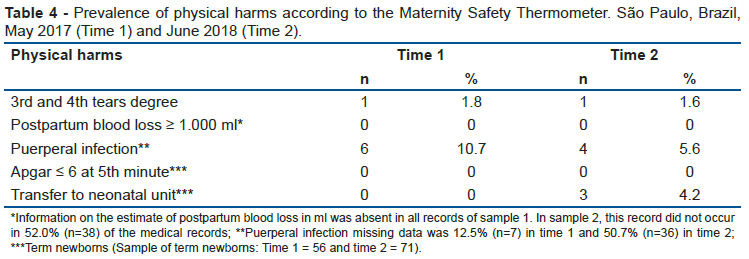
There was no data of postpartum blood loss estimated in millilitres (ml) in medical records in time 1 (table 4). Some professionals registered the postpartum blood loss as "physiological/normal/adequate" or "increased". However, this kind of estimate was not accounted for because it was noted that there was no standardization among nurse-midwives and physicians from that maternity. In time 2, the absence of recorded data on postpartum blood loss estimated in ml on medical records decreased to 52.0% (n=38) (bleeding ≤ 499 ml = 41.1% (n=30) and bleeding between 500 to 999 ml = 6.9% (n=5)) (table 4). It should be clarified that, due to the lack of estimates of blood loss in medical records in time 1, this data could not be accounted for in the indicator, impacting the physical harm-free care indicator.
Regarding signs and symptoms after vaginal birth or caesarean, in time 1, 43.3% (n=29) of medical records did not record this information. This did not happen in time 2 when all medical records showed that no women had any faint or collapse, haemoglobin measured less than 7.0 g/dl, received a blood transfusion or intravenous iron.
Over 84,0% of women had a perineal trauma or abdominal wound (time 1: 84.6% (n=55) and time 2: 84.9% (n=62)). Caesarean section ratio corresponded to 23.6% (n=13) in time 1 and 29.0% (n=18) in time 2. Regarding perineal trauma, 3rd and 4th tears degree was as expected less frequent (table 4) than others spontaneous tears (1st and 2nd tears degree in time 1: 1.8% (n=1) and 61.8% (n=35) and time 2: 1.6% (n=1) and 54.8% (n=34).The proportion of episiotomies was 12.7% (n=7) in time 1 and 14.5% (n=9) in time 2. Analyzing only women who had a vaginal birth (time 1: 80.6% (n = 42) and time 2: 75.3% (n = 55)), the proportion of intact perineum was low (time 1: 28.6% (n=12) and time 2: 20.0% (n=11)).
Puerperal infection corresponded to 10.7% in time 1 (6 cases of infection on caesarean wound) and 5.6% in time 2 (2 cases of infection on caesarean wound and 2 cases of infection on perineal wound). It was not possible to contact 12.5% (n=7) of the women in time 1 and 50.7% (n=36) in time 2 (table 4). The most common reason for that was the fact that women did not answer the telephone calls from the research staff. Also, there were cases in which women said a non-existent telephone number.
All pregnancies were from a single fetus and there was no fetus or neonate death, thus the sample was 67 e 73 babies in time 1 and 2, respectively. No term newborn (i.e., more than 37 weeks) in both samples received an Apgar score equal or less than 6 at 5th minute of birth. No term newborn was transferred to neonatal intensive care unit in time 1. However, this rate was 4.2% (n=3) in time 2 (table 4). According to the medical records, it was not possible to differentiate any admission to neonatal intensive care unit as expected or unexpected. It should be noted that the data about newborn admission/transfer was absent in 16.1% (n=9) of the medical records in time 1 and 1.4% (n=1) in time 2 (table 4).
Regarding the harm-free care reported by women according to their perception of safety, it was 80.6% in time 1 and 43.8% in time 2. The prevalence of the most severe harms according to this indicator is described in table 5. Besides that, excluding the case in which the newborn was admitted in a neonatal intensive care unit, 34.3% (n=23) of the women reported having been separated from their babies at any time during hospitalization in time 1 and 24.7% (n=18) in time 2. Women who would like to talk about a pending issue with the caregivers corresponded to 3.0% (n=2) in time 1 and 11.0% (n=8) in time 2.
DISCUSSION
This study demonstrated potentialities and restraints for the use of the MST in a Brazilian maternity service, besides the MST's cross-cultural adaptation. Having been applied in two moments - before and after an intervention that aimed to improve care (HAMABE project), this tool allowed a quick visualization of the improvements obtained in some indicators, such as the separation of mother and baby situations, and the rate of puerperal infection cases.
Harm collected by MST is severe postpartum haemorrhage, one of the main causes of maternal death worldwide21, including in Brazil5. However, the postpartum blood loss measurement is still challenging even though a systematic review describes a range of available methods to estimate blood loss22. Despite the improvement observed in this study between times 1 and 2, postpartum blood loss was under-reported. In May 2017, no medical records had the information in ml about blood loss estimated. When there was some record, it was inaccurate information, such as "increased bleeding". In June 2018, 52.0% of medical records lacked the information, a considerable improvement compared to time 1. On one hand, the 48.0% records of blood loss in ml could be attributed to the meetings promoted by the HAMABE project, although the method used by staff to estimate blood loss is unknown. On the other hand, it is still concerning that almost half the records did not have information about such a crucial condition. This result reinforces the need for further improvement in the quality and safety of maternity care16.
Caesarean sections and episiotomies are not explicitly included in the physical harm-free care and combined harm-free care indicators by the NHS MST14. However, in a context such as Brazil, with high rates of caesarean sections and episiotomies, it would be relevant to consider these data. In this study, the rates of surgical wounds resulting from caesarean sections and episiotomies combined were high (time 1: 36.4% and time 2: 43.5%). Another study that used MST as a tool to describe outcomes from a secondary analysis of Birth in Brazil survey found that caesarean sections and episiotomies were among the most frequent physical interventions (52.6% and 87.7%, respectively) in the Brazilian Southeast region16, which includes the states of São Paulo, Rio de Janeiro, Minas Gerais, and Espírito Santo (42.0% of the country's population).
In this case, if we consider that the studied maternity provides care to low-risk women, the caesarean rates were high (time 1: 23.6% and time 2: 29.0%) and the sample showed a great proportion of nulliparas (time 1: 41.8% and time 2: 50.7%), all single pregnancies, and mostly term (>37 weeks) pregnancies (time 1: 83.6% and time 2: 97.3%). Although it is known that caesarean section rates higher than 10-15% are not associated with better maternal and neonatal outcomes23, it was not possible to classify caesarean according to Robson's groups based on the information collected by the MST.
Episiotomy rates found in this study (time 1: 12.7% and time 2: 14.5%) were above the maximum of 10% recommended by the WHO24, although much lower than previous national studies2. Routine or liberal use of episiotomy is not recommended in spontaneous vaginal birth25. However, it has been discussed the subjectivity of judgment and definitions for the indications of episiotomy. Studies have shown positive results with non-episiotomy protocols26. Others described adverse outcomes associated with episiotomies, such as more perineal pain, postpartum infection27, sexual dysfunction, and incontinences28.
Brazilian social movements have pointed out that the high rates of episiotomies and other painful and harmful interventions have been used to promote caesarean sections as a "less undignified" way to delivery, which is reinforced by the public-private divide in the health system as well as the social inequalities that mark Brazilian society, especially those related to gender issues29. In this context, it is crucial to affirm that unnecessary medical interventions - including caesarean sections - are harmful.
MST showed that puerperal infection, especially infection on caesarean wounds, was the most frequent physical harm in both times. Estimating this kind of harm is important since sepsis is among the main causes of maternal death worldwide, including Brazil21. In addition, a national survey identified that post-infection hysterectomies and bleeding were the cause of 18% of maternal near-miss in Brazil30.
Postpartum infection cases may be underestimated in this study. In the NHS, MST is finalized up to 10 days after delivery, when the woman returns to the community clinic or is visited by a midwife as part of routine care. The current policy of Brazil provides care to postpartum women and newborns in primary health care or home visit. However, there are barriers, such as: scheduling an appointment only for the newborn, low adherence to postpartum consultation20 and women often go to postpartum care in a service different from the one pre-booked. For these reasons, we made telephone calls between 10 and 15 days after delivery for all women. However, as described in other study16, this approach was challenging given that in many cases nobody answered after several attempts, or the telephone number registered did not exist.
Other study has pointed out the association between obesity and advanced maternal age, and postpartum infections31. However, puerperal infection strongly relates to the quality of care, especially maternity care. Caesarean section has been described as an important cause of infection cases. Results from a Brazilian cohort study showed that caesarean section had an almost three times higher risk of postpartum infection, as an early complication32. Another study carried out in Sweden found as factors associated with postpartum infections: caesarean sections (OR 10.7%, 95% CI 9.80-11.9), 3rd and 4th degrees tears (OR 10.7%, 95% CI 9.80-11.9), and episiotomies (OR 10.2, 95% CI 8.94-11.5)27.
Also considered as physical harm by MST, the transfer of term infants to neonatal intensive care unit in this study was high (4.2% in time 2) considering that most of the women cared for by the maternity were low-risk. These transfers were quite unexpected, as was the high proportion of missing information in time 1 (16.1% of the medical records).
The increased need for intermediate or intensive care for the newborn is only one of the outcomes described by systematic reviews about the effects of caesarean section33 and induced labour34. In Brazil, neonatal morbidity and mortality have as main causes prematurity, intrapartum asphyxia, and low birth weight, factors that can also be associated with mode of delivery35. Factors related to pregnancy, quality of care, and social determinants have also been associated with neonatal morbidity and mortality, such as the reduced number of prenatal consultations, maternal socioeconomic status, and access to health services35.
Despite mother-baby separation not being considered as serious harm by MST, the benefits of continuous mother-baby contact have been reaffirmed for decades by studies and recently by WHO25. The "golden hour" encompasses a set of evidence-based practices (i.e., skin-to-skin contact, delayed umbilical cord clamping, and breastfeeding) that contribute to the physiological stabilization of mother and newborn. However, in Brazil, healthy full-term newborns are frequently separated from their mothers to undergo procedures, such as the use of inhaled oxygen, upper airways and gastric aspiration, and use of incubator36. In this study, reports of mother-baby separation decreased (34.3% in time 1 and 24.7% in time 2). MST applied on a national survey database by Salgado et al.16 found that 69.5% of women referred to separation from their babies between 2011 and 2012.
One of the innovations presented by the MST is considering the women's perception of safety as part of harm-free care indicator. Qualitative evidence demonstrates that many women are speaking up about their concerns and safety alerts, however, the maternity staff needs to listen and respond to them37. This assessment is extremely relevant in any setting, especially in maternities where the model of care is distant or in transition to an optimal and safe care pathway.
Reports of being left alone during labour when there was some type of concern scored significantly (time 1: 14.9% and time 2: 21.9%), possibly as a response to an increase in women's information about their entitlement in childbirth in this service, promoted by the HAMABE project38. In Brazil, a hegemonic model of care relies on medical interventions rather than one-to-one care (one professional per woman)2, which can contribute to these findings. Moreover, Brazilian women often report feeling lonely and abandoned immediately after childbirth, when health professionals exit the room39, sometimes even leaving women with legs up and open. There are frequent reports of lack of empathy in caregiving, classified as a disrespectful and abusive situation in childbirth. Venturi et al.40 concluded that 25% of Brazilian women suffer obstetric violence, in other words, they are subjected to degrading and inhumane situations during pregnancy, birth, and/or postpartum. Additionally, in time 2, 17.8% of women felt they were not taken seriously. This is confirmed by qualitative data, which showed that women felt health professionals devalued their choices and desires38.
Lastly, in this study, it was not possible to estimate the combined harm-free care indicator, given the poor quality of the blood loss record in ml. Medical records in Brazil often underreport or incorrectly report interventions, which makes it difficult to retrospectively assess health outcomes and care practices41. Salgado et al.16, nevertheless, found that only 2% of women in the Brazilian Southeast region did not experience any type of harm during hospitalization. Another study carried out in three hospitals in Northeastern Brazil found that 18,6% of all women received harm-free care15. It is unknown what would be the ideal rate, however, Salgado et al.16 pointed out that the Brazilian assistance is more frequently a provider of harm rather than harm-free care.
CONCLUSION
We conclude that MST is a concise tool and could measure harm-free indicators related to the care offered to women and newborns in a short time range. In a Brazilian context, MST is innovative as it approaches the safety of maternal and childcare from the woman's perspective. In this study, MST also helped to improve the quality of medical records, as it made clear that relevant information about a patient's health status was not properly registered.
However, this study suggests that reliance just on MST may make some problems invisible if it is used alone to assess this indicator in Brazil, because of the invisibility of service-related harm, due to poor medical records. Despite the cross-cultural adaptation to Brazilian Portuguese language15, MST still reflects the NHS setting and does not express issues related to the safety of women and neonates in maternities with excessive levels of interventions (i.e., induced labour, oxytocin augmentation, episiotomy, caesarean section), such as most Brazilian services2. Nevertheless, MST can be further improved to make visible the role of unnecessary interventions to better respond to the patient safety challenges in Brazil.
Author Contributions
Bruna Dias Alonso elaborated the research project, carried out the data collection, performed data analysis, and discussion of the results. Wrote and carried out the final review of the text; Denise Yoshie Niy participated the data collection and data analysis. Wrote and carried out the final review of the text; Cláudia de Azevedo Aguiar co-advised the execution of the study. Wrote and carried out the final review of the text; Eder Lucio da Fonseca participated of statistical analysis. Wrote and carried out the final review of the text; Jane Sandall co-advised the execution of the study. Wrote and carried out the final review of the text; Carmen Simone Grilo Diniz co-advised the execution of the study. Wrote and carried out the final review of the text.
Funding
FAPESP funded the HAMABE research project (Process number 2015/50498-0), and CAPES funded the Bruna Dias Alonso PhD (Finance Code 001).
Acknowledgments
The authors would like to thank all the women who gave interviews for this study. The authors also thank FSP/USP LabTel for provision structure for data collection via telephone calls.
Conflicts of Interest
The authors do not have conflicts of interest.
REFERENCES
1.Brasil, Ministério da Saúde. DATASUS/SINASC-Sistema de Informações sobre Nascidos Vivos. http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinasc/cnv/nvuf.def Accessed October 21, 2019. [ Links ]
2.Leal MC, Pereira APE, Domingues RMSM, Theme Filha MM, Dias MAB, Nakamura-Pereira M, Bastos MH, Gama SGN. Obstetric interventions during labor and childbirth in Brazilian low-risk women. Cad Saude Publica 2014; 30. DOI:10.1590/0102-311X00151513 [ Links ]
3.WHO. The prevention and elimination of disrespect and abuse during facility-based childbirth. Geneva: WHO, 2014. [ Links ]
4.Hotimsky SN, de Aguiar JM, Venturi GA. Violência institucional no parto em maternidades brasileiras. In: Venturi G, Godinho T (Org.). Mulheres brasileiras e gênero nos espaços público e privado: uma década de mudanças na opinião pública. São Paulo: Perseu Abramo; Sesc, 2013. [ Links ]
5.Pacagnella RC, Nakamura-Pereira M, Gomes-Sponholz F, Aguiar RALP, Guerra GVQL, Diniz CSG, Campos BBNS, Amaral EM, Moraes Filho OB. Maternal mortality in Brazil: Proposals and strategies for its reduction. Rev. Bras. Ginecol. e Obstet. 2018; 40: 501-6. DOI: 10.1055/s-0038-1672181 [ Links ]
6.Power M, Stewart K, Brotherton A. What is the NHS safety thermometer? Clin Risk. 2012;18:163-9. DOI: 10.1258/cr.2012.012038 [ Links ]
7.Davis-Floyd RE, Sargent CF. Childbirth and authoritative knowledge. London: University of California Press, 1997. [ Links ]
8.Miller S et al. Beyond too little, too late and too much, too soon: a pathway towards evidence-based, respectful maternity care worldwide. The Lancet, 2016; vol. 388, 2176-2192. DOI: 10.1016/S0140-6736(16)31472-6 [ Links ]
9.Viacava F, De Oliveira RAD, Carvalho C de C, Laguardia J, Bellido JG. SUS: Supply, access to and use of health services over the last 30 years. Cienc e Saude Coletiva 2018; 23: 1751-62. DOI: 10.1590/1413-81232018236.06022018 [ Links ]
10.Diniz SG, d'Oliveira AFP L, Lansky S. Equity and women's health services for contraception, abortion and childbirth in Brazil. Reproductive Health Matters, 2012, 20(4): 84-101. DOI: 10.1016/S0968-8080(12)40657-7 [ Links ]
11.Anvisa. Resolução RDC nº 36, de 25 de julho de 2013. Institui ações para a segurança do paciente em serviços de saúde e dá outras providências. Brasília, DF: Anvisa, 2013. [ Links ]
12.Anvisa. Serviços de atenção materna e neonatal: segurança e qualidade. Brasília, DF: Anvisa, 2014. [ Links ]
13.WHO. Standards for improving quality of maternal and newborn care in health facilities. Geneva: WHO, 2016. [ Links ]
14.NHS. Maternity Safety Thermometer. 2015. https://www.safetythermometer.nhs.uk/index.php?option=com_content&view=article&xml:id=93&Itemxml:id=633. Accessed October 21, 2019. [ Links ]
15. Melo, CR de. Crosscultural adaptation of the Maternity Safety Thermometer to the Brazilian Portuguese language. 2015. 291p. Thesis (Ph.D.). Post-Graduate Program in Nursing, Federal University of Santa Catarina, Florianópolis, 2015. [ Links ]
16.Salgado HO, Queiroz MR, dos Santos HG, Andreucci CB, Diniz CSG. Using the Maternity Safety Thermometer to estimate harm-free care in Southeast Brazil: A hospital-based cohort. Birth Published Online First: 3 October 2019. DOI: 10.1111/birt.12454 [ Links ]
17. Diniz CSG, Bussadori JCC, Lemes LB, Moisés ECD, Prado CAC, McCourt C. A change laboratory for maternity care in Brazil: Pilot implementation of Mother Baby Friendly Birthing Initiative, Medical Teacher, 2020. DOI: 10.1080/0142159X.2020.1791319 [ Links ]
18.International Federation of Gynecol. Mother-baby friendly birthing facilities. Int J Gynecol Obstet 2015;128:95-9. DOI: 10.1016/j.ijgo.2014.10.013 [ Links ]
19. Engeström Y, Sannino A, Virkkunen J. On the methodological demands of formative interventions. Mind, Cult. Act. 2014; 21: 118-28. DOI: 10.1080/10749039.2014.891868. [ Links ]
20.Serruya SJ, Cecatti JG, Lago T di G. The Brazilian Ministry of Health's Program for Humanization of Prenatal and Childbirth Care: preliminary results. Cad. Saúde Pública, 2004; 5: 1281-1289. DOI: 10.1590/S0102-311X2004000500022 [ Links ]
21. GBD 2015 Maternal Mortality Collaborators. Global, regional, and national levels of maternal mortality, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016; 388: 1775-812. DOI: 10.1016/S0140-6736(16)31470-2 [ Links ]
22.Diaz V, Abalos E, Carroli G. Methods for blood loss estimation after vaginal birth. Cochrane Database Syst. Rev. 2018; 2018. DOI: 10.1002/14651858.CD010980.pub2 [ Links ]
23. Betran AP, Torloni MR, Zhang J, Ye J, Mikolajczyk R, Deneux-Tharaux C, Oladapo OT, Souza JP, Özge T, Vogel JP, Gülmezoglu AM. What is the optimal rate of caesarean section at population level? A systematic review of ecologic studies. Reprod. Health 2015; 12. DOI: 10.1186/s12978-015-0043-6 [ Links ]
24. WHO. Care in normal birth: a practical guide. Geneva: WHO, 1996. [ Links ]
25. WHO. WHO recommendations: intrapartum care for a positive childbirth experience. Geneva: WHO, 2018. [ Links ]
26. Amorim M M, Coutinho I C, Melo I, Katz L. Selective episiotomy vs. implementation of a non-episiotomy protocol: a randomized clinical trial. Reprocutive Health, 14 (55), 2017. DOI: 10.1186/s12978-017-0315-4 [ Links ]
27. Axelsson D, Brynhildsen J, Blomberg M. Postpartum infection in relation to maternal characteristics, obstetric interventions and complications. J Perinat Med 2018; 46: 271-8. DOI: 10.1515/jpm-2016-0389 [ Links ]
28.Chang SR, Chen KH, Lin HH, Chao YMY, Lai YH. Comparison of the effects of episiotomy and no episiotomy on pain, urinary incontinence, and sexual function 3 months postpartum: A prospective follow-up study. Int J Nurs Stud 2011; 48: 409-18. DOI: 10.1016/j.ijnurstu.2010.07.017 [ Links ]
29. Diniz CSG, Rattner D, d'Oliveira AFPL, Aguiar JM, Niy DY. Disrespect and abuse in childbirth in Brazil: social activism, public policies and providers' training. Reprod. Health Matters 2018; 26: 19-35. DOI: 10.1080/09688080.2018.1502019 [ Links ]
30.Dias MAB, Domingues RMSM, Schilithz AOC, Nakamura-Pereira M, Diniz CSG, Brum IR, Martins AL, Theme Filha MM, Gama SGN, Leal M do C. Incidence of maternal near miss in hospital childbirth and postpartum: data from the Birth in Brazil study. Cad Saude Publica 2014; 30: S169-81. DOI: 10.1590/0102-311x00154213 [ Links ]
31.Gundersen TD, Krebs L, Loekkegaard ECL, Rasmussen SC, Glavind J, Clausen TD. Postpartum urinary tract infection by mode of delivery: A Danish nationwide cohort study. BMJ Open 2018; 8. DOI: 10.1136/bmjopen-2017-018479 [ Links ]
32.Mascarello KC, Matijasevich A, Santos IDS dos, Silveira MF. Early and late puerperal complications associated with the mode of delivery in a cohort in Brazil. Rev Bras Epidemiol 2018; 21. DOI: 10.1590/1980-549720180010 [ Links ]
33.Sandall J, Tribe RM, Avery L, Mola G, Visser GHA, Homer CSE, Gibbons D, Kelly NM, Kennedy HP, Kidanto H, Taylor P, Temmerman M. Short-term and long-term effects of caesarean section on the health of women and children. Lancet 2018; 392: 1349-57. DOI: 10.1016/S0140-6736(18)31930-5 [ Links ]
34.Saccone G, Della Corte L, Maruotti GM, Quist-Nelson J, Raffone A, De Vivo V, Esposito G, Zullo F , Berghella V. Induction of labor at full-term in pregnant women with uncomplicated singleton pregnancy: A systematic review and meta-analysis of randomized trials. Acta Obstet. Gynecol. Scand. 2019. DOI: 10.1111/aogs.13561 [ Links ]
35.Lansky S, Friche A de AL, da Silva AAM, Campos D, Bittencourt DAS, Carvalho ML, Frias PG, Cavalcante RS, Cunha AJLA. Birth in Brazil survey: Neonatal mortality profle, and maternal and child care. Cad Saude Publica 2014; 30. DOI: 10.1590/0102-311X00133213 [ Links ]
36.Moreira MEL, Gama SGN da, Pereira APE, Silva AAM, Lansky S, Pinheiro RS, Gonçalves AC, Leal MC. Clinical practices in the hospital care of healthy newborn infant in Brazil. Cad Saude Publica 2014; 30: S128-39. DOI: 10.1590/0102-311x00145213 [ Links ]
37.Rance S, Mccourt C, Rayment J, Mackintosh N, Carter W, Watson K, Sandall J. Women's safety alerts in maternity care: is speaking up enough? BMJ Qual Saf 2013; 22: 348-355. DOI: 10.1136/bmjqs-2012-001295 [ Links ]
38.Niy DY, Oliveira VC de, Oliveira LR de, Alonso BD, Diniz CSG. Overcoming the culture of physical immobilization of birthing women in Brazilian healthcare system- Findings of an intervention study in São Paulo, Brazil. Interface - Comun Saúde, Educ 2019; 23. DOI: 10.1590/interface.180074 [ Links ]
39.Salgado HDO, Niy DY, Diniz CSG. Groggy and with Tied Hands: The First Contact with the Newborn According to Women that Had an Unwanted C-Section. J Hum Growth Dev 2013; 23: 190. DOI: 10.7322/jhgd.61298 [ Links ]
40.Venturi G, Godinho T. Mulheres Brasileiras e Genero nos Espacos Publico e Privado - Uma decada de mudancas da opiniao publica. São Paulo: Editora Fundacao Perseu Abramo/Servico Social do Comercio; 2013. [ Links ]
41.Santos NET, Leal MC, Oliveira AE, Zandonade E, Gama SGN. Concordância entre informações do Cartão da Gestante e da memória materna sobre assistência pré-natal. Cad. Saúde Pública. 2012. Feb; 28 (2): 256-266. DOI: 10.1590/S0102-311X2013000500019 [ Links ]
 Correspondence:
Correspondence:
Bruna Dias Alonso
bruna.dias.alonso@gmail.com
Manuscript received: may 2021
Manuscript accepted: december 2021
Version of record online: june 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}