










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.2 Santo André maio/ago. 2022
http://dx.doi.org/10.36311/jhgd.v32.12955
ORIGINAL ARTICLE
Evaluation of actions to address acquired syphilis between 2016 and 2019, in a southeast brazilian state capital city
Mara Rejane Barroso BarcelosI; Eliane de Fátima Almeida LimaII; Marcello Dala Bernardina DallaIII; Thais Barroso VargasIV; Julia Amorim Meireles BarrosoV; Mariana Porto de SouzaVI; Cindy Amaral BarbosaVII; Cândida Caniçali PrimoVIII
IDepartamento de Ginecologia e Obstetrícia - Universidade Federal do Espírito Santo - Av. Mal. Campos, 1468 - Maruípe, Vitória - ES, Brazil, 29047-105
IIDepartamento de Enfermagem, Universidade Federal do Espírito Santo - Av. Mal. Campos, 1468 - Maruípe, Vitória - ES, Brazil, 29047-105
IIIHospital Universitário Cassiano Antônio de Moraes/ Universidade Federal do Espírito Santo (HUCAM-UFES) - Av Mal. Mascarenhas de Moraes, 1355, Santos Dumont, Vitória - ES, Brazil, 29041-295
IVEscola Superior de Ciências da Santa Casa de Misericórdia de Vitória - Av. Nossa Sra. da Penha, 2190 - Bela Vista, Vitória - ES, Brazil, 29027-502
VUniversidade Vila Velha - Endereço/CEP - Av. Comissário José Dantas de Melo, 21 - Boa Vista II, Vila Velha - ES, Brazil, 29102-920
VIEscola Superior de Ciências da Santa Casa de Misericórdia de Vitória - Av. Nossa Sra. da Penha, 2190 - Bela Vista, Vitória - ES, Brazil, 29027-502
VIIFaculdade Multivix - Rua José Alves, 301, Goiabeiras, Vitória, ES Brazil
VIIIDepartamento de Enfermagem, Universidade Federal do Espírito Santo - Av. Mal. Campos, 1468 - Maruípe, Vitória - ES, Brazil, 29047-105
ABSTRACT
INTRODUCTION: sexually Transmitted Infections (STIs) represent a global public health problem, and are responsible for direct effects on reproductive and child health, causing consequences such as infertility and complications during pregnancy and delivery, fetal death, as well as a variety of health problems in affected children
OBJECTIVE: to evaluate outcome indicators related to acquired syphilis in the period 2016-2019 in a southeast Brazilian state capital
METHODS: this is a descriptive management evaluation study with a quantitative approach, which evaluated the outcome indicators "provision of adequate syphilis treatment in the general population" and "monitoring of acquired syphilis". Data were collected on the Notifiable Health Conditions Information System (SINAN), for the period from January 1st 2016 to December 31st 2019. Information regarding treatment and monitoring of cases of acquired syphilis was obtained by searching electronic medical records between August 1st 2020 and March 31st 2021
RESULTS: the municipality of Vitória had 2,647 cases of acquired syphilis, using the criterion of year of diagnosis. The notified cases related to 1,641 men (61.99%) and 1,006 women (38.01%). The predominant age group was 20 to 29 years, while race / skin color was predominantly brown. The most frequent level of education was complete high school. The non-treponemal test was performed in 84.93% of the cases and the treponemal test in 47.22%. Regarding the "provision of adequate syphilis treatment" indicator, we found a total of 90.08% for adequate treatment of cases in Vitória's public health service network for the four-year period: 87.25% in 2016; 85.27% in 2017; 91.79% in 2018; and 94.23% in 2019. Regarding the "monitoring of syphilis cases in the general population" indicator, we found a total of 35.72% for adequate monitoring of cases in Vitória's public health service network for the four-year period: 33.33% in 2016; 36.83% in 2017; 34.53% in 2018; and 38.20% in 2019
CONCLUSION: the outcome indicators evaluated in Vitória, in the 2016-2019 four-year period, were: adequate treatment 90.08% and adequate monitoring 35.72%
Keywords: syphilis, epidemiological monitoring, health evaluation.
Authors summary
Why was this study done?
Given that data on investigation of acquired syphilis is not available on Notifiable Health Conditions Information System (SINAN) and in view of the need to analyze the epidemiological profile and the results of two components of the plan for fighting the disease in Vitória (ES), analyzing notified cases and evaluating the indicators for acquired syphilis treatment and monitoring is considered to be of utmost importance.
What did the researchers do and find?
The authors examined the data identified and reviewed electronic medical records in order to examine investigation data on 2647 notified cases. They found an increase in the frequency of the disease in the period 2017-2019. In relation to the indicator "provision of adequate syphilis treatment", the authors found that it was 90.08% among the cases notified in the municipal health system (SEMUS), while the indicator for adequate "monitoring of syphilis cases in the general population" was only 35.72%.
What do these findings mean?
Although the city of Vitória has shown gradual improvements in the percentage of adequate treatment of acquired syphilis, the percentage of adequate monitoring is still far from the desired level, posing a challenge to the health service and its management. These results point to the need to reevaluate strategies, in the sense of improving them, with emphasis on monitoring the disease.
INTRODUCTION
Syphilis is a global public health problem and its epidemiology varies around the world1. The World Health Organization (WHO) has estimated a total of 6.3 million incident cases of syphilis worldwide, based on prevalence data from 2009 to 2016, with 0.5% global prevalence of syphilis in men and women, ranging regionally 0.1% to 1.6%2.
Acquired syphilis is a health condition for which notification has been compulsory in Brazil since 2010, as per Ordinance No. 24723. The acquired syphilis detection rate showed a threefold increase in the period from 2014 to 2018, rising from 25.1 to 79.8 cases/100,000 inhabitants4. Notwithstanding, it is considered to be an underreported health condition5. Underreporting negatively impacts the response to sexually transmitted infections (STIs) in Brazil, both in terms of total cases as well as in terms of behavioral aspects and vulnerability6.
Between 2010 and June 2021, Brazil reported a total of 917,473 cases of acquired syphilis on the Notifiable Health Conditions Information System (SINAN), with 51.7% in the Southeast, 22.4% in the South, 13.4% in the Northeast, 6.9% in the Midwest, and 5.6% in the North2.
In the state of Espírito Santo (ES), in the period from 2010 to 2018, acquired syphilis had increasing detection rates. In 2019 (117.1 cases/100,000 inhab.), and 2020 (78.8 cases/100,000 inhab.), it was one of 11 Brazilian states with detection rates higher than the national average, ranking second and third in the country, respectively, in those years2,7.
In the period from 2010 to 2018, the municipality of Vitória (ES) was among the 16 state capitals with syphilis detection rates in pregnant women higher than the national rate8. In 2019 (222.3 cases/100,000 inhab.) and 2020 (141.9 cases/100,000 inhab.), it was the state capital with the highest syphilis detection rate2,7.
In 2016, when syphilis was declared a serious public health issue by the Ministry of Health8, the municipality of Vitória enhanced its Syphilis Response Plan to achieve better surveillance and health care. The plan has eight components, two of which relate directly to acquired syphilis: providing adequate treatment for syphilis in the general population and monitoring acquired syphilis cases. In addition to the strategies set out in the plan, various levels of municipal health service management and health care have been working together, highlighting integration between surveillance care, focusing on addressing the disease9.
Outcome evaluation consists of assessing the effect of care on the health status of the population, based on its satisfaction with the care received. The results can be a reflection of care actions, but it is not possible to point out errors without evaluating the stages that preceded care10. In view of the interrelationship between the care provider and the care receiver in this process, this study will consider the process as being the Syphilis Response Plan itself and the actions performed to fulfill each of its components, based on the relationship between health service providers and health service users.
Indicators are considered to be variables aimed at providing the best possible image of an object, so that the choice of the indicators is a critical task for the evaluator11,12.
This study was based on the premises covered by Novaes13, whereby: the objective is improvement; the position of the evaluator is variable, sometimes internal, sometimes external; the prioritized focus is characterization/quantification; the methodology is quantitative; the context is natural; the use of information generates instruments for management; and the judgment formulated in relation to temporality generates norms in an integrated and continuous context13.
Given that data on investigation of acquired syphilis is not available on the Notifiable Health Conditions Information System (SINAN)6 and considering the need to evaluate the epidemiological profile of the disease in the municipality, evaluating acquired syphilis treatment and monitoring indicators is of the utmost importance for contributing to the evaluation of the components of the Response Plan in force in the municipality.
As such, the objective of this study is to evaluate the outcome indicators of components 3 and 4 of the Syphilis Response Plan9, namely "provision of adequate syphilis treatment in the general population" and "monitoring of acquired syphilis cases", among the cases notified by the municipal health services between 2016 and 2019 in Vitória, capital of the state of Espírito Santo, Brazil.
METHODS
This is a descriptive management evaluation study using a quantitative approach.
The study scenario is the municipality of Vitória, capital of the state of Espírito Santo. It has a territorial area of 97.123 km2 and an estimated population of 365,855 inhabitants. The municipality is located partly on an island and partly on the mainland and is divided into six health regions, namely: Maruípe, Continental, Forte São João, Centro, São Pedro and Santo Antônio14.
The criteria for inclusion in the study were: being a notified case of acquired syphilis in the period from January 1st 2016 to December 31st 2019 and having a registered address within the municipality of Vitória (ES).
The exclusion criteria were: being a duplicated record on the SINAN database and having a registered address outside the municipality of Vitória (ES).
Before case notification data were input to the SINAN system, the notification forms were checked by the Vitória Municipal Epidemiological Surveillance Service, in accordance with Ministry of Health case definition criteria in force between 2016 and 201915-17. An acquired syphilis case was considered to be an asymptomatic individual who had a reactive non-treponemal test result with any reactive treponemal test titer; or a symptomatic individual with at least one reactive test result (treponemal or non-treponemal)15,16.
Currently, with regard to acquired syphilis cases, only identification data and demographic data can be included on the SINAN system6. In order to undertake this study, we had to go back to the original notification forms in order to verify information about case investigation, such as clinical data missing from the original notification and in situations where the original notification was not located. This involved retrieving information from medical records and also, when necessary, from the Sistema Informatizado Rede Bem Estar [Computerized Welfare Network System] (SGIRBE).
The study analyzed cases of acquired syphilis notified in the municipality of Vitória between 2016 and 2019. This involved retrieving information data from the SINAN system, retrieving investigation data from the acquired syphilis notification forms, followed by checking the corresponding electronic medical records. We also retrieved data on case monitoring from electronic medical records held on the SGIRBE system.
Data was retrieved from the Notifiable Health Conditions Information System (SINAN) relating to the period from January 1st 2016 to December 31st 2019. Information on case treatment and monitoring was retrieved from electronic medical records between August 1st 2020 and March 31st 2021.
Data was retrieved from original notification forms and from SGIRBE system records between August 22nd 2020 and July 21st 2021. These variables were input to an Excel spreadsheet and added to the information retrieved from the SINAN system.
The identification variables studied were: Federative Unit (Espírito Santo; other states); municipality of notification (Vitória; Vila Velha; other municipalities); services providing notification (SEMUS; private laboratories; hospitals and clinics in Vitória; health centers in other municipalities).
The demographic variables studied were: age categorized in 10 year intervals (10 a 19 years; 20-29 years; 30-39 years; 40-49 years, 50 or over); self-reported skin color (according to the categories used by the Brazilian Institute of Geography and Statistics (IBGE) - stratified into white, brown, black, indigenous and yellow); schooling (illiterate, incomplete elementary education, complete elementary education, complete high school education and complete higher education); and health region of residence.
The clinical and laboratory variables studied were: non-treponemal test (reactive, non-reactive, not performed); Venereal Disease Research Laboratory - VDRL titer (less than or equal to 1/8; greater than 1/8); treponemal test (reactive, non-reactive, not performed); clinical classification (primary, secondary, tertiary; latent; unknown); treatment (Benzathine Penicillin G 2.4 million UI; Benzathine Penicillin G 4.8 million I; Benzathine Penicillin G 7.2 million UI; other regimen; not performed; unknown); adequate treatment (yes; no; unknown); post-treatment monitoring with 1 VDRL (yes; no; unknown); adequate monitoring (yes; no; unknown).
The acquired syphilis detection rate was calculated by dividing the number of annual cases by the population estimated for the municipality by SEMUS/Health Information Center, according to the IBGE/Federal Audit Court estimate for the year, multiplied by 100,000 inhabitants.
The indicators for components 3 and 4 of the Plan were calculated based only on cases of acquired syphilis notified by the health services linked to the SEMUS, since the other services are not under the control of the municipality, nor is there access or connection by computerized systems between them and the SEMUS.
The third component, "provision of adequate syphilis treatment in the general population"9, was analyzed based on the "percentage of adequate syphilis treatment" indicator, among the cases cared for by the health services of the Vitória Municipal Health Department (SEMUS).
Treatment considered adequate for acquired syphilis - in terms of dosage and time - was complete use of Benzathine Penicillin according to the clinical stage of the disease, or alternative drugs, as established in the Treatment Guidelines Clinical Protocol. Prescription of Doxycycline 100mg, according to the clinical stage of the disease, was considered to be a "different regimen". The indicator for adequate treatment was the sum of percentage treatment with 7.2 million IU, 2.4 million IU of Benzathine Penicillin and treatment with Doxycycline 100mg every 12 hours, for 15 or 30 days, according to the clinical stage of the disease18.
The fourth component, "monitoring of acquired syphilis cases in the general population"9, was analyzed based on the "percentage of adequate monitoring" indicator.
Adequate monitoring was considered to be performance of the non-treponemal test every 3 months until the 12th month of follow-up of a patient with acquired syphilis, with examination at 3, 6, 9 and 12 months after treatment. Stopping monitoring after the cure criterion had been met was also considered to be adequate. The reference non-treponemal test used in this study was the VDRL test. The cure criterion during monitoring was analyzed, by verifying a twofold titer decrease in six months for recent syphilis or a twofold titer decrease in one year for late syphilis18.
Statistical analysis was performed using the PSPP statistical package, version 1.3.1, from July 22nd to August 31st 2021. Categorical variables were expressed in the descriptive analysis according to by their absolute and relative frequencies.
This research was submitted to the Research Ethics Committee of the Centro de Ciências da Saúde, Universidade Federal do Espírito Santo, and approved as per Opinion No. 3.787.294, dated December 20th 2019, Certificate of Submission for Ethical Appraisal No. 25982319.6.0000.5060.
RESULTS
We identified 2,781 notified cases of people resident in Vitória, being 785 in 2016, 505 in 2017, 604 in 2018, and 888 in 2019. A total of 134 duplicate cases were excluded -53 in 2016, 16 in 2017, 16 in 2018 and 49 in 2019 -, so that 2,647 cases remained in the study (732 in 2016, 489 in 2017, 588 in 2018 and 838 in 2019). Among these, the number of notified cases was found to be on the increase from 2017 to 2019. The percentage of males was predominant throughout the four-year period (data not shown).
The acquired syphilis detection rate was 203.58/100,000 inhabitants in 2016; 134.66/100,000 in 2017; 164.12/100,000 in 2018; and 231.43/100,000 inhabitants in 2019 (data not shown).
Between 2016 and 2019, 2,644 cases (99.88%) were notified in Espírito Santo. Only three cases (0.12%) occurred in other states: one (0.04%) in Minas Gerais, one (0.04%) in Rio de Janeiro and one (0.04%) in Santa Catarina (data not shown).
With regard to the municipalities, cases were notified as follows: Vitória 2,281 (92.38%); Vila Velha, 344 (13%); Fundão and Serra, 6 each (0.23%); Cariacica and Viana, 2 each (0.23%); other municipalities in the state of Espírito Santo (Guaçuí, Linhares and São Domingos do Norte), 1 case each (0,04%); municipalities in other states (Ribeirão das Neves, Rio de Janeiro and Brusque), 1 case each (0.04%) (data not shown).
Regarding the sources of notification, SEMUS (Vitória Municipal Health Department services) notified 1,966 cases (74.27%), followed by private laboratories, 469 (17.72%); hospitals in Vitória, 166 (6.27%); health centers, emergency services, reference centers and prison health services in other municipalities, 29 (1.10%); hospitals and clinics in other municipalities, 9 (0.34%); and private clinics in Vitória, 8 (0.30%) (data not shown).
Over the four-year period, the health regions with the highest percentage of notified cases were Maruípe (660; 24.93%), followed by the Continental (603; 22.78%), Forte São João (449; 16.96%), Centro (346; 13.07%), São Pedro (315; 11.90%) and Santo Antônio (274; 10.35%) health regions (table 1).
With regard to sex, 1,641 male (61.99%) and 1,006 female (38.01%) cases were notified. The male sex was predominant in all 4 years, with percentages above 60% (table 1).
The 20 to 29 year age group was predominant in all years, totaling 905 cases, (34.57%); followed by those aged 30-39, 655 cases (24.74%); 50 years or older, 460 (17.38%); 40-49 years, 311 (11.75%); 13-19 years, 303 (11.45%); and under 13 years old, 3 (0.11%) (table 1).
The most frequent race/skin color was brown, with 849 cases (31.89%); followed by white, 473 (17.87%); black, 270 (10.20%); yellow, 7 (0.26%); and indigenous, 4 (0.15%). We identified 1,049 cases (39.63%) whose race/skin color was unknown (table 1).
The most frequent level of schooling was complete high school education, with 636 cases (24.03%); followed by incomplete elementary education, 458 (17.30%); complete elementary education, 430 (16.24%); and complete higher education, 205 (7.54%). Level of schooling was unknown for 904 cases (34.15%) (table 1).
The non-treponemal test performed was the VDRL. With regard to testing, of the total number included in the study, 2,332 cases (88.10%) underwent non-treponemal testing (VDRL). Among these, 2,248 (84.93%) tested positive (table 2). Among the cases having the VDRL test, a total of 1,732 (88.10%) came from the municipal health network (SEMUS), of which 1,672 cases (85.05%) were reactive and 1,118 (63.93%) had titers greater than 1/8 (data not shown).
The treponemal tests used were the Rapid Test (RT) or the Treponemal Antibody Test (SIF). A total of 1,250 cases (47.22%) underwent treponemal testing. Among these, 1,173 (44.31%) were reactive (table 2). Among the cases that underwent treponemal testing, a total of 1,124 cases (57.17%) came from the SEMUS health network, and of these, 1,063 (54.07%) were reactive.
With regard to clinical classification of the disease, latent cases were the most frequent (1,027 cases; 38.80%); followed by primary (350; 13.22%); secondary (273; 10.31%); and tertiary (131; 4.95%). We detected 866 (32.72%) cases with unknown clinical classification (table 2).
Regarding treatment, 1,476 cases (55.65%) were treated with Benzathine Penicillin 7.2 million IU; 404 (15.26%) with Benzathine Penicillin 2.4 million IU; 97 (3.66%) with Benzathine Penicillin 4.8 million IU; 64 (2.42%) with a different regimen. There were 82 cases (3.10%) for whom no treatment was performed and 527 (19.91%) for whom treatment was unknown (data not shown).
Regarding monitoring, 1,295 cases (48.92%) had at least 1 post-treatment VDRL (data not shown).
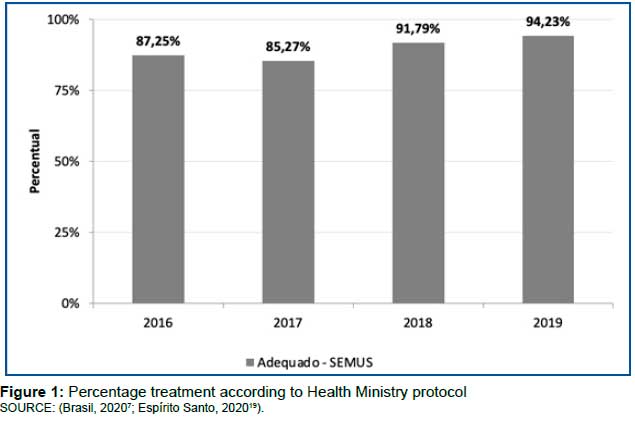
As for the indicator for component 3, "provision of adequate syphilis treatment", we found that the percentage of adequate treatment among cases in the SEMUS network was 90.08% in the total four-year period: 87.25% in 2016; 85.27% in 2017; 91.79 in 2018; and 94.23% in 2019 (figure 1).
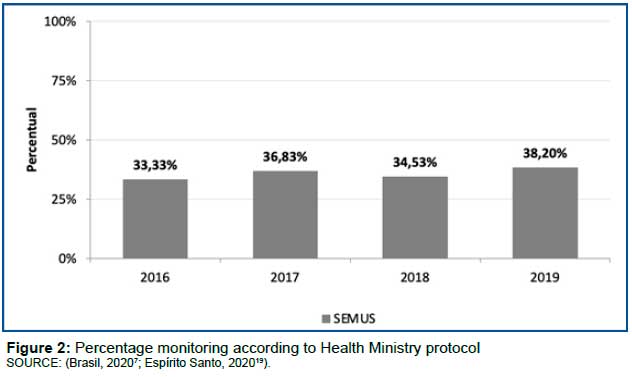
Regarding the indicator for component 4, "monitoring of syphilis cases in the general population", we found that the percentage of adequate monitoring, among the cases in the SEMUS network, was 35.72% in the total four-year period: 33.33% in 2016; 36.83% in 2017; 34.53% in 2018; and 38.20% in 2019 (figure 2).
DISCUSSION
When analyzing the four-year period from 2016 to 2019, there was a decrease in the municipality of Vitória in the number of acquired syphilis cases and also in its detection rate in the period 2016-2017. In 2017, there was a drop in the number of acquired syphilis notifications throughout the state of Espírito Santo, coinciding with the period when there was a global shortage of Benzathine Penicillin between 2013 and 201720. The same indicators showed an increase in the three-year period from 2017 to 2019. Part of this increase can probably be attributed to the increase in rapid testing in Vitória - especially in the SEMUS network services - similarly to what has been happening in other municipalities21.
The increased detection rate means that the syphilis epidemic is on the rise in the municipality. Several studies have emphasized the resurgence of syphilis in specific populations, including men who have sex with men (MSM), in various parts of the world22,23. Notified cases can be considered to be either prevalent or incident, since it is not always possible to identify the clinical stage of the disease6.
In Brazil, the acquired syphilis detection rate increased until 2018, when it reached 76.4 cases per 100,000 inhabitants. In 2019, there was a reduction in the rate, with 74.2 cases per 100,000 inhabitants, and in 2020 it fell to 54.5 cases per 100,000 inhabitants. This reduction has been attributed to data transfer problems between the Brazilian National Health System (SUS) management levels, delays in notification and input to the SINAN databases, as well as local mobilization of health workers caused by the COVID-19 pandemic2.
The predominant age group in all the years studied was the 20-29 age group, followed by the 30-39 age group, in line with what was seen in Brazil in the same period. However, the 50 years and over age bracket was the third most frequent in Vitória, and the fifth most frequent in Brazil, which deserves the attention of health service management to ensure that there are prevention actions and early detection for this target audience as well. In other words, it is a generation that began its sex life without safe sex practices, as well as having aspects of greater vulnerability, such as greater difficulty in erection among men and less vaginal lubrication among women7,24,25.
Whereas in Vitória the relative frequency of acquired syphilis cases was 61.99% in males and 38.01% in females over the four-year period, in Brazil during the 2010-2019 time series 41.1% were male cases and 58.9% were female cases7.
The pattern of race/skin color distribution in Vitória resembled that of Brazil as a whole. People of brown and black skin color added together over the four-year period accounted for 42.19% in Vitória, while in Brazil in 2019 they accounted for 48.3%. The most frequent level of education was complete high school, followed by incomplete elementary and complete elementary education. This schooling profile among acquired syphilis cases was also identified in Brazil as a whole in 2019. In Vitória, unknown education level accounted for 34.15% of cases in the four-year period, while in Brazil in 2019 it accounted for 36.2%7. A study conducted in the cities of Augusto Corrêa, Barcarena and Bragança, in the state of Pará, found association between acquired syphilis and low schooling levels26.
When higher percentages of acquired syphilis are found among Black people and those with low education levels, this points to the concept of vulnerability, which seeks to understand how social, cultural and individual aspects interact to lead to conditions in which certain dangers or threats may materialize27,28.
In this study, 88.10% of cases had a non-treponemal test, this being the test chosen to monitor treatment. Treponemal tests were performed in 47.22% of cases because they are easy to perform, provide results within 30 minutes, do not require laboratory infrastructure, can be performed by any trained person, but once the result is positive it tends to remain positive for life. Therefore, they are not useful for monitoring treatment, nor do they distinguish between current and previous infection21.
With regard to the clinical classification of the disease, the latent stage was most frequent, followed by the primary, secondary and tertiary stages. It is important to distinguish between recent (up to one year of case progression) and late latent syphilis, since in incident cases, the primary, secondary and recent latent forms are considered stages of greater transmissibility6.
The "provision of adequate treatment" indicator increased over the four-year period, reaching 94.23% in 2019, reflecting improvements in component 3 of the Syphilis Response Plan in Vitória.
Although 48.92% of the cases had at least one VDRL test after treatment, a single test is not considered adequate according to Ministry of Health criteria18.
With regard to the "monitoring of syphilis cases in the general population" indicator, adequate monitoring was found to be 35.72% for the total four-year period, improving only from 2016 to 2017 and from 2018 to 2019. Moreover, this is a challenge for municipal health services and municipal health management, since monitoring the response to treatment is mandatory and must be performed throughout the health care network18.
It is our understanding that part of this percentage of inadequate monitoring, or indeed no monitoring at all, is due to the low perception of these health service users regarding their vulnerability. A qualitative study conducted with eight women aged 21 to 44 years old who had a prior history of sexually transmitted infections detected that they had low perception of their vulnerability, suggesting that prevention actions should be planned that are not limited to transferring information, but rather include exchange of knowledge, beliefs and values, and respect their experience of life and their sexuality29.
Regarding data on investigation of acquired syphilis not being available on the SINAN system, authors have been emphatic about the need for alignment between the revisions of case definition, the notification form, epidemiological investigation and SINAN -the system intended to receive and hold these data -, in order for there to be better quality of information about surveillance actions. Once the epidemiological investigation data on acquired syphilis has been systematically collected, it needs to be input to and processed by the system6.
The inexistence of investigation data on the SINAN system was considered to be a complicating factor, resulting in the need to review printed notification forms, notification forms linked to the electronic medical records held on cases registered in the SEMUS network, and electronic medical records themselves, when we were unable to locate the notification. Some of these steps would have been spared if the investigation data were available on the SINAN system.
There is a notable incompleteness of data on race/skin color, education and clinical classification. This study provides an informed justification for health service management for completion of these fields to be mandatory when inputting notifications on Vitória's computerized health system19.
Some stages of this work were affected by the COVID-19 pandemic, without significant repercussions on the final result. Only data for the year 2019 may have suffered some repercussion due to the pandemic, but it is not clear if there was really any influence30.
A limitation of this study was analysis of secondary data, which is subject to completion errors and/or incomplete information. Moreover, as the monitoring indicator for acquired syphilis was based on searching electronic medical records, there may have been completion errors.
It is also noteworthy that this is an unprecedented study, since the entire data on the investigation of acquired syphilis had not been analyzed systematically prior to this study. Knowledge of these indicators allows a reevaluation of strategies, in the sense of improvement, with emphasis on monitoring the disease.
CONCLUSION
The municipality of Vitória had an adequate treatment percentage (90.08%) throughout the 2016-2019 four-year period, with an increase each year. With regard to the adequate monitoring percentage, notwithstanding its improvement in 2019 (38.20%), it is still far from desirable. In order to achieve gradual improvement of these indicators, we suggest greater adherence to the Ministry of Health protocols.
REFERENCES
1.Çakmak SK, Tamer E, karadag AS, Waugh M. Syphilis: A great imitator. Clinics in dermatology. 2019; 37(3): 182-191. DOI: 10.1016/j.clindermatol.2019.01.007 [ Links ]
2.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis (DCCI). Boletim Epidemiológico da Sífilis, 2021 out; 01 (Número Especial). [ Links ]
3.Portaria Nº. 2.472, de 31 de Agosto de 2010. Nº. 168 - DOU de 01/09/10 - p. 50 - seção 1. 2010. [ Links ]
4.Pan American Health Organization (PAHO). New generations free of HIV, syphilis, hepatitis B, and chagas disease: EMTCT plus in the Americas, 2018 [Internet]. Washington, D.C.: Pan American Health Organization; 2019. 42p. Available from: https://www.paho.org/en/documents/new-generations-free-hiv-syphilis-hepatitis-b-an-d-chagas-disease-americas-emtct-plus-2018 [ Links ]
5.Lafeta KRG, Martelli Júnior H, Silveira MF, Paranaíba LMR. Sífilis materna e congênita, subnotificação e difícil controle. Rev Bras Epidemiol [Internet]. 2016; 19(10): 63-74. DOI: https://doi.org/10.1590/1980-5497201600010006 [ Links ]
6.Domingues CSB, Lannoy LH, Saraceni V, Cunha ARC, Pereira GFM. Protocolo Brasileiro para Infecções Sexualmente Transmissíveis 2020: vigilância epidemiológica. Epidemiologia e Serviços de Saúde [online], 2021. DOI: https://doi.org/10.1590/S1679-4974202100002.esp1 [ Links ]
7.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis (DCCI). Boletim Epidemiológico da Sífilis. 2020. Brasília: Ministério da Saúde, 2020. [ Links ]
8.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância, Prevenção e Controle das Infecções Sexualmente Transmissíveis, do HIV/AIDS e das Hepatites Virais (DIAHV). Boletim Epidemiológico da Sífilis, 2018; 49(45). [ Links ]
9.Vitória (ES). Prefeitura Municipal. Secretaria Municipal de Saúde. Plano de enfrentamento "Vitória contra sífilis". Vitória; 2016. [ Links ]
10.Donabedian A. The definition of quality: a conceptual exploration. In: Donabedian A. Explorations in quality assessment and monitoring. Ann Arbor, Michigan: Health Administration Press; 1980. p. 1-31. [ Links ]
11.Tanaka OY, Tamaki EM. O papel da avaliação para a tomada de decisão na gestão de serviços de saúde. Ciênc. saúde coletiva. 2012 Apr;17(4): 821-828. DOI: http://dx.doi.org/10.1590/S1413-81232012000400002 [ Links ]
12.Tanaka OY. Avaliação da atenção básica em saúde: uma nova proposta. Saude soc. 2011; 20(4): 927-934. DOI: http://dx.doi.org/10.1590/S0104-12902011000400010 [ Links ]
13.Novaes HMD. Avaliação de programas, serviços e tecnologias em saúde. Rev. Saúde Pública. 2000; 34 (5): 547-59. [ Links ]
14.Vitória (ES). Prefeitura Municipal. Secretaria Municipal de Saúde. Plano Municipal de Saúde. Período 2018-2021. Vitória; 2018. [ Links ]
15.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Coordenação Geral de Desenvolvimento da Epidemiologia em Serviços. Guia de Vigilância em Saúde. Brasília: Ministério da Saúde; 2016. [ Links ]
16.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância, Prevenção e Controle das Infecções Sexualmente Transmissíveis, do HIV/AIDS e das Hepatites Virais (DIAHV). Nota informativa. (2- SEI/2017); 2017. [ Links ]
17.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. Protocolo clínico e diretrizes terapêuticas para atenção integral ás pessoas com infecções sexualmente transmissíveis (IST). Brasília: Ministério da Saúde; 2019. [ Links ]
18.Freitas FLS, Benzaken AS, Passos MRL, Coelho ICB, Miranda AE. Protocolo Brasileiro para Infecções Sexualmente Transmissíveis 2020: sífilis adquirida. Epidemiologia e Serviços de Saúde [online], 2021. [ Links ]
19.Espírito Santo (Estado). Secretaria Municipal de Saúde de Vitória. Bancos de dados do Sistema Único de Saúde: base municipal anos 2010 a 2019 do Sistema de Informação de Mortalidade (SIM), Sistema de Informação de Nascidos Vivos (SINASC) e Sistema de Informação de Agravos de Notificação (SINAN). Vitória: SEMUS, 2020. [ Links ]
20.Araujo RS, Souza ASS, Braga JU. A quem afetou o desabastecimento de penicilina para sífilis no Rio de Janeiro, 2013-2017? Rev Saude Publica. 2020; 54: 109. [ Links ]
21.Gaspar PC, Bigolin A, Alonso Neto JB, Pereira EDS, Bazzo ML. Protocolo Brasileiro para Infecções Sexualmente Transmissíveis 2020: testes diagnósticos para sífilis. Epidemiologia e Serviços de Saúde [online], 2021. [ Links ]
22.Pierbon M, Cocchio S, Russo C, Bonamin MA, Baldo V. Sexually-transmitted infections: What is the true prevalence? A cross-sectional online survey of men who have sex with men in the Veneto Region of Italy. J. Prev Med Hyg. 2019; 60(3). [ Links ]
23.Lee NY, Chen YC, Liu HY, et al. Increased repeat syphilis among HIV-infected patients: A nationwide population-based cohort study in Taiwan. Medicine. 2020; 99(28): e21132. [ Links ]
24.Aguiar RB, leal MCC, marques APO. Knowledge and attitudes about sexuality in the elderly with HIV. Ciênc Saúde Coletiva [Internet]. 2020; 25(6): 2051-62. [ Links ]
25.Araujo MAL, Uesono J, Machado NMS, Pinto VM, Amaral E. Protocolo Brasileiro para Infecções Sexualmente Transmissíveis 2020: abordagem às pessoas com vida sexual ativa. Epidemiologia e Serviços de Saúde [online]. 2021; 30(spe1): e2020628. [ Links ]
26.Souza RL, Madeira LDPS, Pereira MVS, Silva RM, Sales JBL, Azevedo VN, Feitosa RNM, Monteiro JC, Ishak MOG, Ishak R, Ribeiro ALR, Oliveira-Filho AB, Machado LFA. Prevalência de sífilis em mulheres profissionais do sexo em três municípios do interior do estado do Pará, Amazônia brasileira. Doenças infecciosas de BMC. 2020; 20(1): 129, 2020. [ Links ]
27.Oviedo RAM, Czeresnia, D. O conceito de vulnerabilidade e seu caráter biossocial. Interface - Comunicação, Saúde, Educação [online]. 2015; 19(53): 237-250. [ Links ]
28.Ozelame JEEP, Frota OP, Ferreira Júnior MA, Teston EF. Vulnerabilidade à sífilis gestacional e congênita: uma análise de 11 anos. Rev enferm UERJ, Rio de Janeiro. 2020; 28(1): e50487. [ Links ]
29.Moura SLO, Silva MAM, Moreira ACA, Freitas CASL, Pinheiro AKB. Percepção de mulheres quanto à sua vulnerabilidade às Infecções Sexualmente Transmissiveis. Escola Anna Nery [online]. 2021; 25(1): e20190325. [ Links ]
30.Maciel ELN, Jabor PM, Macedo LR, Almada GL, Zanotti RL, Cerutti Junior C, Gomes CC, Alencar FEC, Reuter T, Andrade VLG, Cardoso AO, Medeiros Junior NF, Bastos WM, Bertolani MN, Silva LT, Zandonade E. Living conditions, seroprevalence and symptoms of COVID-19 in slums in the Metropolitan Region of Vitória (Espírito Santo). Revista Brasileira de Epidemiologia [online]. 2021; 24: e210048. [ Links ]
 Correspondence:
Correspondence:
Mara Rejane Barroso Barcelos
mararsb@gmail.com
Manuscript received: may 2021
Manuscript accepted: december 2021
Version of record online: june 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}