










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkJournal of Human Growth and Development
versão impressa ISSN 0104-1282versão On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.2 Santo André maio/ago. 2022
http://dx.doi.org/10.36311/jhgd.v32.10856
ORIGINAL ARTICLE
Perceptions of sex workers about the care received in the health care context
Beatriz Guerta PastoriI; Andrei Biliato ColmanettiII; Claudia de Azevedo AguiarIII
IUniversidade Federal do Triângulo Mineiro (UFTM), Uberaba, MG, Brasil
IIUniversidade Federal do Triângulo Mineiro (UFTM), Uberaba, MG, Brasil
IIIDepartamento de Saúde Coletiva da Universidade Federal do Triângulo Mineiro (UFTM), Uberaba, MG, Brasil
ABSTRACT
OBJECTIVE: sex workers are configured as a historically marginalized group for deviate of the moral and social behavior pattern dictated by conservative dogmas on which Brazil was built. Such exclusion is also expressed in public health policies, where the group is mentioned only in actions and programs aimed at sexually transmitted infections (STIs), which violates basic principles proposed by SUS (Brazilian Unified Health System). This paper aims to analyze the care received in the context of health care from the perspective of sex workers
METHODS: this is a descriptive and exploratory study, with a qualitative approach, that have as referential of analysis the Collective Subject Discourse (CSD), built from a half-structured interview realized with the group in question and a socioeconomic questionnaire. The DSC is a method that assemble opinions and individual expressions in a unique testimony, written in first person singular, that gives voice to this collectivity. The collect was helped by community health agents of Family Health Unit that includes the brothel's territory
RESULTS AND DISCUSSION: were interviewed 22 sex workers, being 19 cis woman and 3 trans woman, most of whom in a situation of social vulnerability - brown or black, little schooling and low rent. The speeches identified the existence of health care that does not meet the specific demands of this population, in addition to the presence of fragmented care and focused on sexual and gynecological health. The trans or cis interviewed, moreover, strong resistance to gender identity and respect for the social name by the team. In addition, there were expressions of fear in revealing the profession during medical appointment, due to the stigma and preconception that fell on them. Even so, these professionals understand that their health needs are met in SUS, which connotes a resigned view of the gaps in the care network, requiring specific health actions, programs and policies for this population
FINAL CONSIDERATIONS: the sex workers are a society's cutout that suffer daily with stigma on their pattern of sexual behavior, living an important condition of social vulnerability. This reflects on fear to seek medical services and to reveal their profession, resulting in gaps on the access and right to health in this population. It is necessary, therefore, creation of health programs and policies specifics and requalification of the health teams for the management of this patients
Keywords: sex workers, delivery of health care, unified health system, collective subject discourse.
Authors summary
Why was this study done?
This study was conceived and carried out based on the authors' concern about the health conditions of sex workers in a little brazilian city. It was intended to understand, from the perspective of these professionals, how the access to the services of the care network occurs and how the health care of these vulnerable women and the target of great social stigma is given.
What did the researchers do and find?
Interviews were conducted with sex workers in their workplaces (prostitution houses in the city), using an instrument containing questions about access to health services and their perceptions of the care received. From the data analysis, through the Collective Subject Discourse, the presence of health care that does not meet the specific demands of sex workers was identified, in addition to the presence of fragmented care focused only on their sexual and gynecological
What do these findings mean?
The results point to the emerging need to implement specific health policies for sex workers, as well as the (re)qualification of health teams and service management for the humanized and comprehensive care of this population.
INTRODUCTION
Sex workers constitute a historically stigmatized and discriminated group, as they deviate from the standard model of socially and morally established behavior. Judged as perverts, drug users, lazy and spreaders of diseases, sex workers are placed on the margins of society and state actions, such as health policies1,2.
For much of the 20th century, health actions aimed at women kept the focus on maternal and child care. In 1984, with the creation of, in Brazil, a public policy called Programa de Atenção Integral à Saúde da Mulher (PAISM), the concept of health care was expanded, but some female population groups, such as sex workers, remained invisible. Two decades later, there was the implementation of the National Policy for Integral Attention to Women's Health (PNAISM), which, despite having expanded its actions to several previously excluded groups, such as women in deprivation of liberty, blacks and lesbians, the specific health needs of sex workers remained hidden3-5.
This absence of public health policies aimed at sex workers reflects negatively on equity in health, without which the other two doctrinal principles of the Unified Health System (SUS) cannot be guaranteed: integrality and universality. This fact, according to Villela and Monteiro6, evidences a laissez-faire posture of the Brazilian State, that is, "under the guise that the right of women to prostitution is respected, there is a lack of assistance to their needs for comfort and safety at work", further contributing to the marginalization of the group.
On the other hand, despite the lack of specific health policies aimed at the integral care of sex workers, they are always remembered and mentioned in actions and programs aimed at controlling infectious diseases, such as the National STD/AIDS Program, thus contributing to the construction of the fragmented view that the sex worker is just a "body from the waist down"7.
Even in gynecological and obstetric health care, obstacles have been observed in accessing services and in care for sex workers. In the study by Szwarcwald8, about 20% of sex workers did not undergo a gynecological examination in the last three years and, of these, half never went to the gynecologist. In addition, approximately 40% of the women interviewed did not seek care the last time they had a sexual health problem.
With regard to care, the study by Villela and Monteiro6 demonstrates that the lack of adaptations of health services to the reality of these women, such as the opening hours of basic health units, associated with the fear of being poorly attended, keeps sex workers away from the health services. This distance, however, can increase the risks of morbidities such as depression, chronic diseases, complications related to induced abortion and others.
Thus, it is questioned how much the demand for health services, the quality of care received and the bond with the team are influenced by the social stigma built on sex workers. Therefore, we seek to analyze how the assistance in health services is, based on the perception of these social actors.
METHODS
This is a descriptive and exploratory study, with a qualitative approach, using the Collective Subject Discourse (CSD) method as a reference for analysis.
Qualitative studies are concerned with understanding the group participating in the research, as well as aspects of their reality that cannot be quantified, infiltrating human perceptions9.
The CSD is a method that rescues and presents the social representations obtained from empirical research. The opinions or individual expressions obtained from the interviews and which have similar meanings are grouped into general semantic categories. In each category "the contents of opinions of similar meaning present in different statements are associated, in order to form with such contents a synthesis statement, written in the first person singular, as if it were a collectivity speaking in the person of an individual"10,11.
Sex workers from the city of Uberaba/MG, Brazil, over 18 years old, participated in the study. The sample size was defined by saturation, as proposed by Minayo9.
For data collection, a semi-structured questionnaire was used, containing socioeconomic-demographic data and open questions about the health care received. The collection took place in 2019 and was carried out in partnership with community health agents of the Family Health Unit responsible for covering the territory where houses of prostitution are located in the city. On an opportune day for the agents and the interviewers, these houses were visited and a first round of interviews was carried out with the sex workers who consented to their participation in the study. In the other interviews, the "snowball method" was used, which consists of indicating friends and/or known people who fit the eligibility criteria of the study. This choice was due to the difficulty in accessing this population.
The interviews were audio-recorded, with the permission of the participants, and transcribed in full for later construction of the CSD.
The study project was approved by the Research Ethics Committee of the proposing institution (Federal University of Triângulo Mineiro), according to CAAE No. 04476218.0.0000.5154, meeting the requirements of the Brazilian Resolution CNS-MS No. 466/2012, including the signing of the Term of Free and Informed Consent.
RESULTS AND DISCUSSION
As shown in table 1, 22 sex workers participated in the survey, all female, 86.4% cis women and 13.6% trans women; most of them declared themselves brown (72.7%), in contrast to 18.2% white; the mean age found was 31.2 years old, ranging from 20 to 59 years (standard deviation 10.0). They were mostly single (90.9%) and had an average of 1.8 children per professional (standard deviation 1.8). As for schooling, 31.8% had incomplete elementary school, 40.9% had incomplete high school (H.S.) and 4.6% had completed H.S. On the other hand, 13.6% had higher education. Prostitution was the exclusive occupation of 50% of the interviewees, while the other half also worked in another profession, such as baker or hairdresser. Regarding the housing condition, 59% said they lived in a rented house and 31.8% in their own house, while 4.6% lived in a loaned house and 4.6% did not have a house. Income was a very variable item, showing contrasts and oscillating between R$ 500 (~US$ 100) and R$ 15,000 (~US$ 3,000) per month. The answer found when asked about religion was quite plural, predominantly Catholicism (27.3%) and those who said they hard no religious belief (36.4%).
The table reveals a vulnerability profile of these women, who are mostly of mixed race/ethnicity, with little education and low income. Such characteristics are in line with data found in other studies on the subject. Lima12, for example, found a profile of sex workers in his research who, for the most part, self-reported as brown or black, young, single, with little or no academic training and low purchasing power.
Hankel et al.,13 reported that ethnic-racial identity is determinant in the way a woman will relate to her work. They highlight that black women are more likely to work for pimps and face physical aggression and sex trafficking in their profession. In addition, they claim that structural racism and sexism are determinant to justify a greater share of African-American women in work such as street prostitution, than in closed places with some health and safety. Clarke et al.,14 also showed a relationship between race and the age of starting work as a sex worker, showing that African-American women have the highest rates of entry into the profession during their youth.
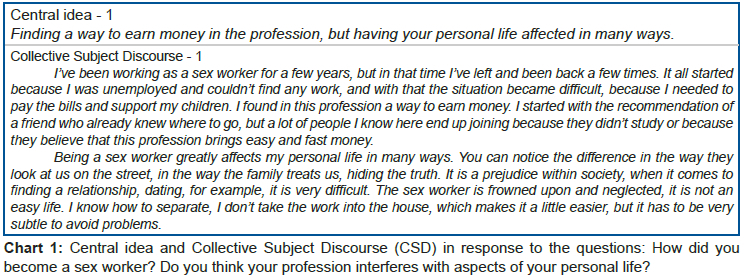
Next, we will present the central ideas and excerpts from the CSD related to the perception of sex workers about the impact of their profession on the attention and care they receive in health:
Table 1 shows a strong relationship between entry into the prostitution business with unemployment and financial difficulties. This association, added to the low level of education, represents the main factors that make the sex market, for these women, a possible path to be followed. Despite being poorly paid and stigmatized, prostitution is more profitable and accessible to poor women with little or no professional training15. In addition, the social barriers that make them vulnerable prevent both the exit of these professionals from the system of selling and exploiting their bodies, as well as their entry into the formal job market16.
Juliano15 reiterates that the strongest social prejudice occurs against those who are in greater financial difficulties, and that it worsens if there are other elements, such as belonging to an ethnic minority, being an immigrant or having black or brown skin.
For Figueiredo and Peixoto17, prostitution is the result of exploitations legitimized by elites and rulers and of taboos involving sexuality expressed outside the standards. Thus, these women are relegated to marginality and impelled to lack of protection and situations of aggravation. Cruz et al.18, in line, show that the sex worker occupies a space of intense social vulnerability, being more susceptible to different types of violence, precarious working conditions, drug use, risk of gynecological diseases and/or STIs, unwanted pregnancy, discrimination and stigma. It is also the deep prejudice deposited on them that makes them avoid health services, making holistic care impossible, as proposed by the organic laws of the Brazilian Unified Health System.
With regard to health care, the vast majority of sex workers interviewed (90.9%) are exclusive users of the Unified Health System. It is evident, according to the CSD in Chart 2, that the search for medical care, when performed, is predominantly in relation to sexual health and exams for STIs, due to both the occupational risk and the lack of integral care in other specialties.
However, the lack of adaptations to the reality and particularities of this group, such as the itinerant nature of the profession and the lack of time, combined with the fear of being poorly attended due to the stigma on their profession, distance sex workers from health services, as reiterated. by other scientific studies.
Villela and Monteiro6, for example, point out that due to the gaps in successive policies aimed at women, which failed to consider the specific needs of sex workers (such as the pre- Unified Health System maternal and child care model, the PAISM and the PNAISM), there is a lack of adaptability of the health system that keeps sex workers away from the service. They also point out how the Brazilian health system restricts sex workers to strictly sexual aspects, ignoring that the precarious condition in which their service is provided is directly related to the emergence of diseases, such as chronic disease and depression, for example. Platt et al.19, through a meta-analysis, reiterate and confirm the same points in the international context.
The DCS excerpt "...I try to consult more with the gynecologist, because in addition to the delay, the other medical specialties don't attend me properly and don't even look at me...", highlights what Brito-Silva et al.20 discussed about the compartmentalized right to be antagonistic to the principle of integrality of the Unified Health System in its different senses. In other words, as the right to health in the country is thought of from a integrality perspective, attending users of the system is a partial way is an evident non-compliance with the services.
On the other hand, most participants said that the Unified Health System, despite the delay and the characteristics of care, is able to supply their needs; feel included in the health system. This result is similar to that found by Paiva21, where the sex workers studied positively evaluated the care provided, despite not having regular follow-up with professionals from the Family Health Strategy of the Unified Health System.
However, as observed in the excerpt "... I believe that my health demands are met by the Unified Health System", it is possible to perceive a resigned speech of sex professionals, that is, despite finding difficulties and obstacles for the medical care of aspects of their health, in addition to sexual and reproductive ones, conclude that the assistance received satisfies what they are looking for. If there is a system that excludes them from this integral care, either because of the delay in scheduling appointments in other medical specialties, or because health professionals in these specialties do not offer dignified care due to prejudice or stigma, how can sex workers qualify care in all its dimensions? It is easy to understand the reasons why they feel satisfied with the part (or the little) they receive. On this, Peres da Silva22 says that "the understanding of the Unified Health System as a policy created to guarantee the right to health is replaced by the idea of concession by the State. In the user's imagination, the Unified Health System is a needy system and is not associated with its ability to exercise the acquired right".
The fear of judgment on the part of health professionals is a decisive factor for sex workeres not to seek medical care or, when they do, not to reveal their profession23. The study by Bungay et al.24 points out that sex workers do not reveal what they do in clinics for fear of judgments, discrimination due to their social position or for fear of the consultation being limited to STIs, reducing the focus on health problems not related to the sexuality. On the other hand, this omission of information during the anamnesis can also lead to incomplete or inefficient care, as it is a data of clinical interest.
Despite this insecurity, it is reported in the CSD of chart 3 that discrimination during care is not always present among cis women; for transgender women, there is a difference in treatment, especially with regard to the use of the social name. The National Health Policy for Lesbians, Gays, Bisexuals, Transvestites and Transsexuals was integrated into the Unified Health System in 2011, with the general objective of promoting health and a holistic view of the LGBT+ population, fostering means to reduce inequalities and institutional prejudice, since sexual orientation and gender identity directly affect the process of social determination and health status, through the prejudice and stigma suffered25.
The policy emerged as a means to consolidate the pillars of equity, integrality and universality of the Unified Health System, but it presents weaknesses in its implementation, such as the resistance that the medical community has to respect this population within the care practice. This difficulty is demonstrated by chart 3 and reinforced by other studies, as in Ferreira et al.26.
In the study by Muller and Knauth27, the authors report that the prejudice suffered by transvestites and transsexuals and the disrespect for their social name are factors that distance them from medical care and often contribute to the worsening of general diseases in this population. In addition, they claim that the language used by health professionals, quite distant from their own dialect, can culminate in the patient's non-adherence to coping with her health problems.
Integrality encompasses the meaning of a professional performance that understands the individual in his biopsychosocial aspect27. It is noticed that, in the current care model, this principle is disrespected and sex workers are reduced to a small dimension of their lives, contributing to the formation of gaps in care and the perpetuation of stigmas.
FINAL CONSIDERATIONS
Sex workers are stigmatized by society for distancing themselves from the historically accepted pattern of sexual behavior. As a result, they constitute themselves as a social minority of expressive vulnerability (brown or black women, without their own housing, without a fixed salary and with low education), a fact that has a direct and negative impact on their health. In addition, factors such as insecurity and fear of judgment, combined with the lack of specialized care, influence and define how these women relate to and access health devices.
One of the main outlets in this context is the fear of seeking medical attention, of revealing the profession or being reduced to its occupational risks, and, therefore, access to health, the bond with the medical team and the guarantee of the right to health make are difficult to achieve. Despite this, the service was evaluated, most of the time, as satisfactory, although focused on sexual health and despite the low frequency of consultations. This highlights the fragility, also in this population, of the recognition of health as a constitutional right, which results in a behavior of conformity in the face of gaps in the health care network.
With regard to transvestite and transsexual women, the presence of a prejudice related mainly to gender and not to the profession was observed, characterizing an example of disrespect for health policies aimed at this public and another prejudice rooted in the prevailing heteronormative culture.
Finally, it is understood that the creation of health programs and actions specifically aimed at this population group is very important to ensure that the principles of equity and integrality are respected. It is also necessary to (re)qualify health teams for contact with sex workers, with active search, reception, training for proper management, which is free from judgments and respecting the uniqueness of each person. Such initiatives have the potential to deconstruct the stigmas and prejudices that permeate the lives of these women and perpetuate their condition of vulnerability also in the health services.
Author Contributions
Beatriz Guerta Pastori: Participated in the elaboration of the research project, performed data collection and typing. Assisted in the analysis and discussion of the results. Wrote and performed final proofreading of the text; Andrei Biliato Colmanetti: Participated in the elaboration of the research project, performed the collection and typing of data. Assisted in the analysis and discussion of the results. Wrote and performed final proofreading of the text; Claudia de Azevedo Aguiar: He guided the research, reviewed the research project and submitted it to the UFTM Research Ethics Committee. Helped with analyses, described and discussed the results. He carried out a final revision of the text as well as its translation into English. He reviewed the article and approved the version that was submitted;
Financial Support
The research was carried out without financial support.
Conflict of interest
The authors do not have any type of conflict of interest.
REFERENCES
1.Leitão EF, Costa LLS, Brêda MZB, Albuquerque MC dos S de, Jorge JS. A prática cotidiana de saúde das profissionais do sexo. Revista Brasileira em Promoção da Saúde 2012; 25: 295-304. https://doi.org/10.5020/18061230.2012.2259 [ Links ]
2.Moraes MLC de, Costa PB, Aquino PDS, Pinheiro AKB. Educação em saúde com prostitutas de Fortaleza: relato de experiência. Rev Eletr Enf 2008; 10. https://doi.org/10.5216/ree.v10.46823 [ Links ]
3.Aquino P de S, Ximenes LB, Pinheiro AKB. Políticas públicas de saúde voltadas à atenção à prostituta: breve resgate histórico. Enfermagem em Foco 2010; 1. https://doi.org/10.21675/2357-707X.2010.v1.n1.4 [ Links ]
4.Centro de Documentação do Ministério da Saúde. Assistência integral à saúde da mulher: bases de ação programática. Brasília: Ministério da Saúde; 1984. [ Links ]
5.Brasil, editor. Política nacional de atenção integral à saúde da mulher: princípios e diretrizes. 1a. ed., 2a. reimp. Brasília, DF: Editora MS; 2011 [ Links ]
6.Villela WV, Monteiro S. Gênero, estigma e saúde: reflexões a partir da prostituição, do aborto e do HIV/aids entre mulheres. Epidemiol Serv Saúde 2015; 24: 531-40. https://doi.org/10.5123/S1679-49742015000300019 [ Links ]
7.Sousa FR de. Educação Popular em Saúde e participação de prostitutas: contribuições para a gestão participativa do SUS. Interface (Botucatu) 2014; 18: 1568-1568. https://doi.org/10.1590/1807-57622013.0406 [ Links ]
8.Szwarcwald C. Taxas de prevalência de HIV e sífilis e conhecimento, atitudes e práticas de risco relacionadas às infecções sexualmente transmissíveis no grupo das mulheres profissionais do sexo: relatório de pesquisa. Brasília: Ministério da Saúde; 2010. [ Links ]
9.Lefèvre F, Lefèvre AMC. O discurso do sujeito coletivo: um novo enfoque em pesquisa qualitativa; desdobramentos 2003. [ Links ]
10.Lefevre F, Lefevre AMC. Discourse of the collective subject: social representations and communication interventions. Texto Contexto - Enferm 2014; 23: 502-7. https://doi.org/10.1590/0104-07072014000000014 [ Links ]
11.Lima FS da S, Merchán-Hamann E, Urdaneta M, Damacena GN, Szwarcwald CL. Fatores associados à violência contra mulheres profissionais do sexo de dez cidades brasileiras. Cad Saúde Pública 2017; 33. https://doi.org/10.1590/0102-311X00157815 [ Links ]
12.Hankel J, Dewey S, Martinez N. Women Exiting Street-Based Sex Work: Correlations between Ethno-Racial Identity, Number of Children, and Violent Experiences. Journal of Evidence-Informed Social Work 2016; 13: 412-24. https://doi.org/10.1080/23761407.2015.1086718 [ Links ]
13.Clarke RJ, Clarke EA, Roe-Sepowitz D, Fey R. Age at Entry into Prostitution: Relationship to Drug Use, Race, Suicide, Education Level, Childhood Abuse, and Family Experiences. Journal of Human Behavior in the Social Environment 2012; 22: 270-89. https://doi.org/10.1080/10911359.2012.655583 [ Links ]
14.Juliano D. El trabajo sexual en la mira: polémicas y estereotipos. Cad Pagu 2005: 79-106. https://doi.org/10.1590/S0104-83332005000200004 [ Links ]
15.Santos OP dos, Ramalho RC, Oliveira CFD, Lima RCD, Arantes AA, Filho IM de M. Perfil sociodemográfico e avaliação do conhecimento das profissionais do sexo acerca das ISTs em um município na região metropolitana de Goiânia. Revista de Iniciação Científica e Extensão 2019; 2: 81-8. [ Links ]
16.Figueiredo R, Peixoto M. Profissionais do sexo e vulnerabilidade. BIS, Bol Inst Saúde (Impr) 2010: 196-201. [ Links ]
17.Cruz NL da, Ferreira CL, Martins E, Souza M. O cuidado com a saúde das mulheres profissionais do sexo: uma revisão narrativa. Disciplinarum Scientia | Saúde 2016; 17: 339-52. [ Links ]
18.Platt L, Grenfell P, Meiksin R, Elmes J, Sherman SG, Sanders T, etal.. Associations between sex work laws and sex workers' health: A systematic review and meta-analysis of quantitative and qualitative studies. PLoS Med 2018; 15: e1002680. https://doi.org/10.1371/journal.pmed.1002680. [ Links ]
19.Brito-Silva K, Bezerra AFB, Tanaka OY. Direito à saúde e integralidade: uma discussão sobre os desafios e caminhos para sua efetivação. Interface (Botucatu) 2012; 16: 249-60. https://doi.org/10.1590/S1414-32832012005000014 [ Links ]
20.Paiva LL de, Araújo JL de, Nascimento EGC do, Alchieri JC. A vivência das profissionais do sexo. Saúde debate 2013; 37: 467-76. [ Links ]
21.Silva RS. O entendimento do direito à saúde: uma abordagem dos usuários do SUS no Distrito Federal. Cad Ibero Am Direito Sanit 2015; 4: 56-74. https://doi.org/10.17566/ciads.v4i3.156. [ Links ]
22.Benoit C, Jansson SM, Smith M, Flagg J. Prostitution Stigma and Its Effect on the Working Conditions, Personal Lives, and Health of Sex Workers. The Journal of Sex Research 2018; 55: 457-71. https://doi.org/10.1080/00224499.2017.1393652 [ Links ]
23.Bungay V, Kolar K, Thindal S, Remple VP, Johnston CL, Ogilvie G. Community-Based HIV and STI Prevention in Women Working in Indoor Sex Markets. Health Promotion Practice 2013; 14: 247-55. https://doi.org/10.1177/1524839912447189 [ Links ]
24.Ministério da Saúde (Brasil). Política Nacional de Saúde Integral de Lésbicas, Gays, Bissexuais, Travestis e Transexuais - LGBT. Brasília: Ministério da Saúde, 2013. [ Links ]
25.Ferreira B de O, Nascimento EF do, Pedrosa JI dos S, Monte LMI do. Vivências de travestis no acesso ao SUS. Physis 2017; 27: 1023-38. https://doi.org/10.1590/S0103-73312017000400009 [ Links ]
26.Muller MI, Knauth DR. Desigualdades no SUS: o caso do atendimento às travestis é 'babado'! Cad EBAPEBR 2008; 6: 01-14. https://doi.org/10.1590/S1679-39512008000200002 [ Links ]
27.Paim JS, Silva LMV da. Universalidade, integralidade, equidade e SUS. BIS - Bol Inst Saúde 2010. [ Links ]
 Correspondence:
Correspondence:
Beatriz Guerta Pastori
biapastori@hotmail.com
Manuscript received: may 2021
Manuscript accepted: december 2021
Version of record online: june 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}