










Services on Demand
article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkJournal of Human Growth and Development
Print version ISSN 0104-1282On-line version ISSN 2175-3598
J. Hum. Growth Dev. vol.32 no.2 Santo André May/Aug. 2022
http://dx.doi.org/10.36311/jhgd.v32.13322
ORIGINAL ARTICLE
Understanding the impact of newborn touch upon mothers of hospitalized preterm neonates
Christopher BarnesI; Elvidina N. Adamson-MacedoII
IPhD, School of Psychology, College of Health, Psychology and Social Care, University of Derby, Derby, U.K
IIPhD, University of Wolverhampton, Retired Prof. Emeritus formerly with School of Health [CHSCI], Wolverhampton, U.K
ABSTRACT
INTRODUCTION: Many interventions have been designed to support the development of the preterm baby and minimise the complications of prematurity. However, there is limited evidence of the possible psychological benefits of touch to the mother when she is the one performing the support programme during the hospitalisation of her newborn
OBJECTIVE: This study explored whether the type of touch provided to preterm neonates had an impact on maternal self-efficacy, self-esteem and maternal-to-infant attachment, as-well-as newborn weight gain
METHODS: Using a randomised cluster trial, forty babies and their mothers were allocated to one of two groups receiving either a touch-based intervention (TAC-TIC; Touching And Caressing; Tender In Caring) or spontaneous touch
RESULTS: Mothers who provided the touch-based intervention demonstrated greater increases in self-efficacy, self-esteem and attachment, and babies gained more weight than those using spontaneous touch
CONCLUSION: The results indicate that systematic touch interventions may be used to facilitate the mother-baby relationship as well as to promote newborn weight gain
Keywords: Touch; Preterm; Newborn; Self-efficacy; Self-esteem; Attachment.
RESUMO
INTRODUÇÃO: muitas intervenções têm sido desenhadas para apoiar o desenvolvimento do bebê prematuro e minimizar as complicações da prematuridade. No entanto, são limitadas as evidências dos possíveis benefícios psicológicos do toque para a mãe quando é ela quem realiza o programa de apoio durante a hospitalização de seu recém-nascido
OBJETIVO: este estudo explorou se o tipo de toque fornecido aos recém-nascidos prematuros teve impacto na autoeficácia materna, autoestima e apego materno-infantil, bem como no ganho de peso do recém-nascido
MÉTODO: usando um estudo randomizado de cluster, quarenta bebês e suas mães foram alocados em um dos dois grupos que receberam uma intervenção baseada em toque (TAC-TIC; Tocando e acariciando; Tender In Caring) ou toque espontâneo
RESULTADOS: as mães que forneceram a intervenção baseada no toque demonstraram maiores aumentos na autoeficácia, autoestima e apego, e os bebês ganharam mais peso do que aqueles que usaram o toque espontâneo
CONCLUSÃO: os resultados indicam que intervenções sistemáticas de toque podem ser utilizadas para facilitar a relação mãe-bebê, bem como para promover o ganho de peso do recém-nascido
Palavras-chave: toque, pré-termo, recém-nascido, autoeficácia, autoestima, apego
Authors summary
Why was this study done?
There is limited evidence about the psychological outcomes for mothers when they are the ones who deliver touch-based interventions to their babies. This is particularly the case for mothers of premature and hospitalised newborns.
What did the researchers do and find?
We allocated women to one of two groups who either used a touch-based intervention (TAC-TIC) or spontaneous touch (Control). Women implemented touch for 3 minutes (once per day) over 10 consecutive days. It was found that mothers who took part in the TAC-TIC intervention demonstrated greater gains in their self-efficacy, attachment and self-esteem than the spontaneous touch group across time.
What do these findings mean?
The findings indicate that when women apply a touch-based intervention (such as TAC-TIC) it is likely to have positive psychological outcomes for them as well as the baby.
INTRODUCTION
The birth of a premature baby has been described as a stressful event for parents and there is an abundance of literature available that ranges from parents' own accounts1,2, from clinical observations3, and from scientific research4,5. There have been many therapeutic interventions created to date which aim to support the growth, both physical and mental, of the preterm newborn6,7 and minimise the complications of prematurity8. The kinds of intervention that have been used to date with preterms have predominantly been tactile in nature and have reported that some form of touch may play a vital role in facilitating the development of a preterm9,10.
Since the 1970s several types of touch interventions/support programmes have been developed, and these have included; skin-to-skin contact such as kangaroo care11, gentle systematic touch such as TAC-TIC (Touching And Caressing-Tender In Caring12, and moderate pressure touch such as massage13. A review of interventions in place in 82 neonatal units in the United States of America14 suggests that static touch or skin-to-skin contact is used the most (containment [86%] and kangaroo care [98%]) with active touch used less than half of the time (massage [38%]). The benefits of receiving early supplemental touch to babies are well documented in the literature and generally relate to growth and development15-17 and include, increased oxygen levels18,6, enhanced behavioural organisation19, reduced hospital stay, reduced loss of weight during first week and weight gain12,14,20-23.
However, the majority of these interventions have almost exclusively reported effects upon the baby and not investigated the effects on the parents when they are the ones providing the touch. In the limited number of studies that have been conducted, the benefits are in relation to breastfeeding outcomes24, mothers emotional suffering and self-esteem25, maternal mood state26, mother-infant interaction27, and attachment28. However, these studies have almost exclusively recruited mothers when they are at home, 3-4 months following birth and/or with fullterm newborns. Yet there is a much more limited amount of work conducted that has investigated the possible psychological benefits to mothers of hospitalised preterms when they are the ones performing the intervention/support programme. Therefore, there is a real need to develop and evaluate touch intervention programmes that aim to support parents and their preterm newborns during this time. Also, intervention/support programmes that target the psychosocial support of parents29 may have a positive effect upon the child's environment, and fits within the theoretical framework of Neonatal Health Psychology30.
The factors that could contribute most to the mother's psychological wellness at this time may include; maternal self-efficacy, self-esteem and the quality of attachment31. Maternal self-efficacy has its roots within Social Cognitive Theory32 and is a type of self-reflective thought that affects how a parent thinks, feels and acts32,33, and is a major determinant of human motivation34. Maternal self-efficacy is defined as being, "specific to a women's perceived performance in the maternal role, and the beliefs she has in her ability to respond contingently to the signals of her infant"35. Mothers who have a higher self-efficacy are likely to display more sensitive behaviour towards their baby36, will choose to take part in more challenging parenting activities and are more likely to persevere when confronting obstacles or adverse situations37. Indeed, Lappin38 and Clausen, Aguilar, and Ludwig39 have shown that mothers who use touch as an intervention/support programme with their 3-4-month-olds demonstrate increased self-efficacy. Indeed self-efficacy has also been shown to predict child weight outcomes40.
Maternal self-esteem on the other hand refers to the value a woman attaches to her reflected appraisal of herself as a mother36,41. Mothers with a higher self-esteem are more likely to maximise developmental outcomes in their infants and higher self-esteem also results in successful parenting behaviours42. Mothers who have a high self-esteem will develop more positive parenting styles43 and benefit from lower levels of parenting stress44, anxiety and depression45. The emerging mother-infant relationship, particularly the mother's ability to interact and care for her preterm infant, is viewed as central to the mother's development of self-worth46,47. In fact, Cody48 found higher self-esteem in mothers who had used touch as an intervention/support programme with their infants.
Maternal attachment is the unique, affectionate relationship that develops between a woman and her baby and which persists over time49. Research suggests that mothers who have increased levels of attachment to their child are much more likely to have children who go on to form secure lifelong relationships50, that these attachments remain stable across several generations51, and that their children will more likely adapt to varying social situations with greater ease52. In a study by Feldman, et al.53 they have shown that Kangaroo Care provided to premature infants resulted in increased maternal attachment behavior in the postpartum period from 6 months to 10 years of age.
The primary aim of this study was to explore whether the type of touch provided to hospitalized preterm neonates would impact maternal self-efficacy, self-esteem, and maternal-to-infant attachment.
METHODS
Study design
This study used a pre-test/Post-test repeated measures design. Independent variables included Touch-type (TAC-TIC [Experimental] or Spontaneous [Control] touch) and Timepoint (Pre-test/Post-test). Dependent variables included Maternal Self-efficacy, Self-esteem, and Attachment Scores).
Participants
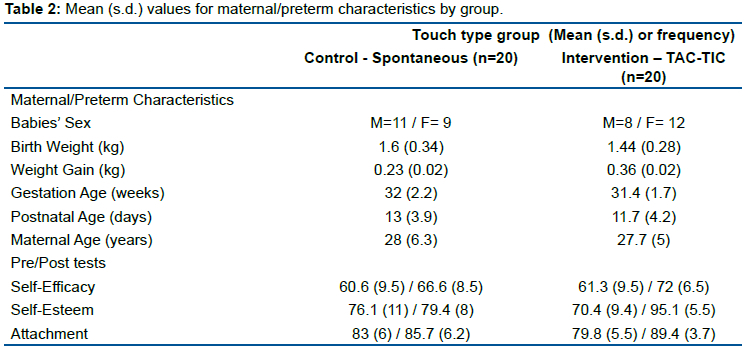
A sample of 40 mothers (age from 18-42) and their healthy preterm babies (i.e. those whose condition is relatively stable and who are not receiving oxygen therapy or mechanical ventilation) were recruited by convenience and allocated to one of two touch-type groups (A structured touch intervention/support programme - TAC-TIC [Touching And Caressing-Tender In Caring] or a group of mothers who provided a spontaneous touch intervention) using a cluster randomised trial. Mothers and their babies were recruited if the infant was born preterm (<2.5kg in birth weight and <37 weeks gestational age), was within their first 28 days of postnatal life, had no diagnosed genetic anomalies, congenital malformations, and were not receiving oxygen therapy. Sample size was estimated based on a large effect size, with 80% power and at a 0.05 level of significance. There was no attrition from the study and each of the forty mothers who consented to take part was retained for the entire duration. The average time spent in the hospital was 37 (s.d. =3.74) for the control group and 32.7 (s.d.= 2.2) for the TAC-TIC group.
Touch Intervention
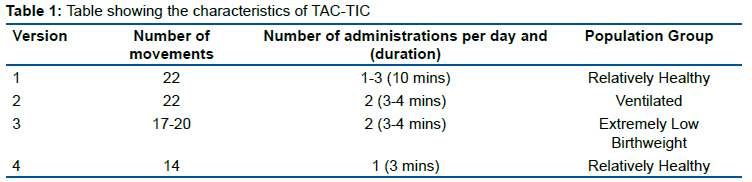
In the intervention/support programme group mothers were taught and followed a specific protocol of systematic touch known as TAC-TIC (TAC-TIC - Touching And Caressing; Tender In Caring12). As can be seen in Table 1 this version of TAC-TIC was developed (Version-4) for use with relatively healthy preterms; it consists of 14 individual stroking movements that are repeated continuously 3 times during a 3-minute session and without undressing the baby. This version of TAC-TIC was designed to be carried out by the mother in comparison to other previous versions that were designed for babies on ventilation and carried out by a researcher. Mothers were taught how to use TAC-TIC and practised this on a doll first before touching their own baby. The information provided to mothers was only procedural and involved describing and demonstrating the way in which the baby should be touched. Once mothers understood what they needed to do they proceeded with the first session of the 10-day study period (1 session of 3 minutes per day) under supervision by the investigator who is a trained psychologist.
Spontaneous touch - support group)
Rather than making comparisons between babies who received TAC-TIC and those who received standard care and nothing more, it was believed that spontaneous touch would act as a truer comparison group. In the spontaneous touch group the mothers were asked to use spontaneous touch to interact with their baby and that this was to be done however they normally touched their baby. No further instruction was given on how they might go about this. However, mothers were asked; (1) not to handle (e.g. pick up or turn over), (2) perform any activities such as feeding or changing, or (3) stimulate any of the other senses of the baby (e.g. talking to the baby), which was requested of mothers in the intervention/support programme group too. Mothers in the Spontaneous touch group also carried this out for three minutes, once per day over 10 days. Both groups checked in with the investigator on a daily basis to ensure the session was conducted.
Note: the randomised cluster trial design implies that there was a period of 'wash-out' between groups thus mothers did not meet with each other.
Measures
Mothers in both groups were given the same pre/post-test questionnaires that measured three different psychological constructs (maternal self-efficacy, self-esteem and attachment) and also a short factual section (measuring factors such as babies' birthweight, gestation age, maternal age etc). Weight gain was recorded by nursing staff and noted by the lead author. The psychometric measures comprised the following.
The Perceived Maternal Parenting Self-Efficacy questionnaire (PMP S-E54) consists of 20 items and four subscales (Caretaking procedures [4], evoking changes in their baby's behaviour [7], reading their baby's behaviour or signalling [6], and situational issues [3]). All items are on a four-point Likert scale and range from 'strongly agree' to 'strongly disagree'. Thus, mothers can have a potential self-efficacy score of between 20-80. The scale has been fully validated with a UK population which includes an internal reliability of 0.91, and a test-retest reliability value of 0.96.
The Maternal Self-Esteem Inventory (MSRI55) short form has 26 items measured on 5 individual subscales (Caretaking ability [6], General ability and preparedness for mothering role [8], Acceptance of baby [3], expected relationship with the baby [5], and Feelings concerning pregnancy, labour and delivery [4]). In this study the MSRI had a total pre-intervention item alpha of 0.84.
The Parent-to-infant attachment questionnaire (PIA56) is a 19 item scale with 3 subscales (Quality of attachment [9], Absence of hostility [5], and Pleasure in interaction [5]). In this study the questionnaire had a total pre-intervention item alpha of 0.69.
Procedures
Following University and hospital ethics approval of the project, and once mothers provided informed consent, the study lasted over a 10-day period. At the beginning (day-1) and end (day-10) of the study mothers were asked to fill-in the same questionnaires. During the study period mothers were asked to touch their baby in line with the process documented above for either the spontaneous touch or TAC-TIC intervention/support programme group and this was supplemental to the standard care mothers/babies received. Also, the baby's weight was monitored at the onset and closure of the study period. There was a period of 'washout' lasting 3 weeks between recruitment of TAC-TIC intervention/support programme and Spontaneous touch group mothers to avoid potential confounds.
RESULTS
A total of forty-seven mothers and their babies, who met the inclusion/exclusion criteria, were approached and in all 40 took part. The sample characteristics can be seen in table 1. Data screening indicated that the sample were normally distributed and there were no significant differences between any of the baseline measures and the intervention group that the mother/baby belonged to.
Relationships between Self-efficacy, Attachment, Self-esteem and demographic characteristics
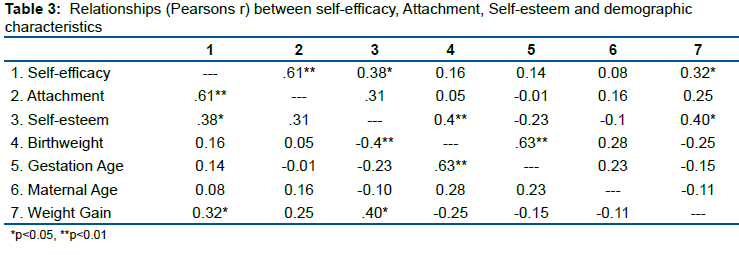
Pearson's correlations between Self-efficacy, Attachment, Self-esteem and demographic characteristics can be seen in table 2. A higher parenting self-efficacy was significantly related to a greater maternal-to-infant attachment (p<0.01), and greater maternal self-esteem (p<0.05). Higher maternal self-esteem was significantly related to weight gain in the babies (p<0.05) as was self-efficacy (p<0.05).
Effects of touch type and pre-test/post-test measurement on maternal self-efficacy, attachment and self-esteem, and newborn weight gain
A two way repeated measures ANOVA was carried out on three separate dependent maternal variables; self-efficacy, attachment and self-esteem. There was a significant main effect of intervention (touch type) for self-esteem (F(1,38)=4.49, p<0.05, η2=0.04) where mothers in the TAC-TIC intervention scored higher than those in the spontaneous touch group. But no significant main effects were found for self-efficacy (F(1,38)=1.68, p>0.05, η2=0.04) or attachment (F(1,38)=0.024, p>0.05, η2=0.001). There was a significant main effect of time (pre/post-test) for self-efficacy (F(1,38)=40.88, p<0.001, η2=0.19), Attachment (F(1,38)=47.52, p<0.001, η2=0.23), and Self-esteem (F(1,38)=94.38, p<0.001, η2=0.31) where scores at post-test were significantly higher than pre-test. In addition, there were significant interaction effects between intervention (touch type) and time (pre/post-test) for attachment (F(1,38)=15.16, p<0.001, η2=0.07) and self-esteem (F(1,38)=55.19, p<0.001, η2=0.18), but not for self-efficacy (F(1,38)= 3.24, p>0.05, η2=0.02). In general, the interactions seem to indicate that mothers who took part in the TAC-TIC intervention increased more in their self-efficacy, attachment and self-esteem than the spontaneous touch group from pre- to post-test - although there was a non-significant interaction with self-efficacy this was approaching significance (p=0.08, power = 0.42). In addition, although baseline measurements were not significantly different the TAC-TIC intervention mothers did have lower on average scores for Attachment and Self-esteem. However, there was a significant main effect of intervention on the amount of weight the baby gained (F(1,38)=18.18, p<0.001, η2=0.12). The mean weight gain over the study period was higher for the TAC-TIC intervention support programme.
DISCUSSION
The primary aim of this study was to explore whether the type of touch provided (systematic or spontaneous) to hospitalised preterm neonates would, (i) have an impact upon maternal self-efficacy, self-esteem and maternal-to-infant attachment, and (ii) demonstrate changes in growth of the baby as indicated by weight gain. In this study both systematic and spontaneous touch produced increases in all maternal psychological variables over time. Although it is unclear why spontaneous touch demonstrates these effects it may be because the group of mothers in this study were also required to check-in daily with the investigator and different effects may have been observed if their only contact time was solely during the completion of the pre/post-test measures.
Despite this, it is clear that maternal variables showed significantly greater increases for mothers who provide systematic touch rather than spontaneous touch and this supports the use and importance of touch as a support programme within neonatal units, particularly during the neonatal period in hospital Though self-efficacy was only approaching significance for the interaction, the results show that this finding was underpowered and that baseline measures - although not significantly different - were lower for the intervention group. These results can be taken as evidence and support for the use of touch as a support programme within the context of the neonatal unit although some caution is needed when interpreting the results and their respective effect sizes. Based upon our findings, previous research and theory, it is likely that these mothers have stronger beliefs in their ability to deal with the full range of parenting tasks at this time32,33, will attempt more difficult parenting tasks, and show greater perseverance when confronting negative situations such as changes in infant health status37. Although further testing is necessary it is plausible that increases in maternal self-efficacy, self-esteem and attachment will equip mothers with all of the necessary skills and self-belief they need in order to provide sensitive behaviour towards their baby36 and allow them to better adjust stimulation to their baby's social signals. It appears that the use of touch by mothers is a clinically important intervention to consider when offering psychological support.
Weight gain was also significantly different between the groups and babies who received the touch intervention gained more weight over the study period than controls. This finding is in line with previous research in the area12,14,20-23. Significant correlations were also found between the mothers' psychological variables, and between self-esteem and weight gain. The correlation between self-esteem and weight gain is interesting but the nature of this relationship remains unclear since it is not possible to conclude which factor results in the effect on the other. Related studies with mothers of 1 year olds indicate that maternal parenting self-efficacy predicts child weight outcomes40 but limited to date has found such a relationship with maternal self-esteem. Whilst it is not possible to establish the direction of causality the results from this study simply indicate a difference between type of touch and weight gain, and type of touch and self-esteem.
A strength of this study was the use of a robust study design. Nevertheless it was not possible to ensure that mothers only applied the touch intervention whilst the investigator was present. This is an issue that is very difficult to control. However, mothers were asked to check-in with the investigator and were loosely monitored throughout the day. It would be valuable to investigate the duration of time needed to produce significant benefits; including the duration of time touch is performed within each session and the number of days the therapeutic intervention lasts for, since mothers only used the touch intervention for 3 minutes in this study. Currently, there is considerable variation in how tactile interventions are delivered ranging from days through to weeks. This may of course vary in accordance with the individual needs of each and every baby and the required threshold necessary to see any health and developmental benefit and a larger clinical trial is recommended.
CONCLUSION
This study has shown that touch interventions play an important role not only for baby's but also for their mothers. Measurement of self-efficacy, self-esteem and attachment should be considered in order to help health professional's guide and support parents of preterms. Touch interventions such as the one in this study are complimentary to existing ones which are already in use (e.g. kangaroo care) and recommended for use in maternity services57. The benefits of such interventions includes those to the baby but also extends to the parents thus facilitating/promoting early parenting. This is important because the touch intervention used in this study is easy for mothers to perform, does not involve removing the baby from their incubator or cot, does not involve handling or undressing the baby, and empowers the parents to take a more active role in their own baby's growth and development. However, further longitudinal study is required in order to understand the future impact upon the newborn and parent.
Acknowledgement
We wish to thank the parents who agreed to take part in this research whilst parenting their newborn in the neonatal unit.
REFERENCES
1.Leung C. Born too soon. in E.N. Adamson-Macedo (Ed.), Expanding Frontiers of Neonatology. Special Issue of Neuroendocrinology Letters, 2004 25(1). [ Links ]
2.Manns SV. Life after the NNU: the long term effects on mothers' lives, managing a child at home with broncho-pulmonary dysplasia and on home oxygen. Neuro Endocrinology Letters. 2004 Dec 1; 25: 127-32. [ Links ]
3.Knepfer, G. and Johns, C. (1989) Nursing for Life. Pan Books, Australia. [ Links ]
4.Pederson DR, Bento S, Chance GW, Evans B, Fox AM. Maternal emotional responses to preterm birth. American Journal of Orthopsychiatry. 1987 Jan; 57(1): 15-21. [ Links ]
5.Padden T, Glenn S. Maternal experiences of preterm birth and neonatal intensive care. Journal of reproductive and infant psychology. 1997 May 1; 15(2): 121-39. [ Links ]
6.Adamson-Macedo EN, de Roiste A, Wilson A, Hayes JA, Eaton B, de Carvalho F. systematic gentle/light stroking and maternal random touching of ventilated preterms: A preliminary study. International Journal of Prenatal and Perinatal Psychology and Medicine. 1997; 9(1): 17-31. [ Links ]
7.Field T. Massage therapy research review. Complementary therapies in clinical practice. 2014 Nov 1; 20(4): 224-9. [ Links ]
8.Field T, Hernandez-Reif M, Diego M, Schanberg S, Kuhn C. Cortisol decreases and serotonin and dopamine increase following massage therapy. International Journal of neuroscience. 2005 Jan 1; 115(10): 1397-413. [ Links ]
9.McIlduff A. Parental touch of the neonate: Encourage or condemn?. Australian College of Midwives Incorporated Journal. 1998 Mar 1; 11(1): 18-22. [ Links ]
10.White-Traut R, Wink T, Minehart T, Holditch-Davis D. Frequency of premature infant engagement and disengagement behaviors during two maternally administered interventions. Newborn and Infant Nursing Reviews. 2012 Sep 1; 12(3): 124-31. [ Links ]
11.Barabach L, Sedlock J, Salmon K. Making kangaroo care the norm: Implementation of a new model of care. Journal of Obstetric, Gynecologic & Neonatal Nursing. 2012 Jun 1; 41: S53-4. [ Links ]
12.Adamson-Macedo EN. Effects of tactile stimulation on low and very low birthweight infants during the first week of life. Current psychological research & reviews. 1985 Dec; 4(4): 305-8. [ Links ]
13.Field T. Interventions in early infancy. Infant Mental Health Journal. 1992 Dec; 13(4): 329-36. [ Links ]
14.Field T, Diego M, Hernandez-Reif M. Preterm infant massage therapy research: a review. Infant behavior and development. 2010 Apr 1; 33(2): 115-24. [ Links ]
15.Oehler JM. Research utilization: The NICU environment. Neonatal network: NN. 1996 Apr; 15(3): 85-6. [ Links ]
16.Harrison L, Olivet L, Cunningham K, Bodin MB, Hicks C. Effects of gentle human touch on preterm infants: pilot study results. Neonatal Network: NN. 1996 Mar 1; 15(2): 35-42. [ Links ]
17.Harrison L, Sherrod RA, Dunn L, Olivet L. Effects of hospital-based instruction on interactions between parents and preterm infants. Neonatal network: NN. 1991 Apr; 9(7): 27-33. [ Links ]
18.De Roiste EA. Aspects of tactile stimulation with infants in intensive and special care baby units. University of Glasgow (United Kingdom); 1991. [ Links ]
19.Ohgi S, Fukuda M, Moriuchi H, Kusumoto T, Akiyama T, Nugent JK, Brazelton TB, Arisawa K, Takahashi T, Saitoh H. Comparison of kangaroo care and standard care: behavioral organization, development, and temperament in healthy, low-birth-weight infants through 1 year. Journal of Perinatology. 2002 Jul; 22(5): 374-9. [ Links ]
20.Roiste AD, Bushnell IW. Tactile stimulation and pre-term infant performance on an instrumental conditioning task. Journal of Reproductive and Infant Psychology. 1993 Jul 1; 11(3): 155-63. [ Links ]
21.Róiste ÁD, Bushnell IW. The immediate gastric effects of a tactile stimulation programme on premature infants. Journal of reproductive and infant psychology. 1995 Jan 1; 13(1): 57-62. [ Links ]
22.de Róiste A, Bushnell IW. Tactile stimulation: Short-and long-term benefits for pre-term infants. British Journal of Developmental Psychology. 1996 Mar; 14(1): 41-53. [ Links ]
23.Ruiz-Peláez JG, Charpak N, Cuervo LG. Kangaroo Mother Care, an example to follow from developing countries. Bmj. 2004 Nov 11; 329(7475): 1179-81. [ Links ]
24.Moore ER, Bergman N, Anderson GC, Medley N. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane database of systematic Reviews. 2016 (11). [ Links ]
25.Anderzén-Carlsson A, Lamy ZC, Eriksson M. Parental experiences of providing skin-to-skin care to their newborn infant-Part 1: A qualitative systematic review. International journal of qualitative studies on health and well-being. 2014 Jan 1; 9(1): 24906. [ Links ]
26.Fujita M, Endoh Y, Saimon N, Yamaguchi S. Effect of massaging babies on mothers: pilot study on the changes in mood states and salivary cortisol level. Complementary Therapies in Clinical Practice. 2006 Aug 1; 12(3): 181-5. [ Links ]
27.Onozawa K, Glover V, Adams D, Modi N, Kumar RC. Infant massage improves mother-infant interaction for mothers with postnatal depression. Journal of affective disorders. 2001 Mar 1; 63(1-3): 201-7. [ Links ]
28.Gürol A, Polat S. The effects of baby massage on attachment between mother and their infants. Asian nursing research. 2012 Mar 1; 6(1): 35-41. [ Links ]
29.Benzies KM, Magill-Evans JE, Hayden KA, Ballantyne M. Key components of early intervention programs for preterm infants and their parents: a systematic review and meta-analysis. BMC pregnancy and childbirth. 2013 Jan; 13(1): 1-5. [ Links ]
30.Adamson-Macedo EN. Neonatal Psychology: Theories and Practice. Journal of Human Growth and Development 2016; 26: 129-32. DOI: https://doi.org/10.7322/jhgd.119236 [ Links ]
31.Prilleltensky I. Cultural assumptions, social justice and mental health: Challenging the status quo. Cultural cognition and psychopathology. 2001: 251-66. [ Links ]
32.Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychological review. 1977 Mar; 84(2): 191. [ Links ]
33.Bandura A. Self-efficacy: The exercise of control). New York. 1997. [ Links ]
34.Koul R. An analysis of the reliability and validity of personal internet teaching efficacy beliefs scale. The Electronic Journal for Research in Science & Mathematics Education. 1999 Jan 1. [ Links ]
35.Teti DM, Gelfand DM. Behavioral competence among mothers of infants in the first year: The mediational role of maternal self-efficacy. Child development. 1991 Oct; 62(5): 918-29. [ Links ]
36.Leerkes EM, Crockenberg SC. The development of maternal self-efficacy and its impact on maternal behavior. Infancy. 2002 May 1; 3(2): 227-47. [ Links ]
37.Pajares, F. Overview of social cognitive theory and of self-efficacy. Retrieved 03/06/2013, from http://www.uky.edu/~eushe2/Pajares/eff.html. [ Links ]
38.Lappin G. Infant massage: A strategy to promote self-efficacy in parents of blind infants. British Journal of Visual Impairment. 2006 Sep; 24(3): 145-9. [ Links ]
39.Clausen JM, Aguilar RM, Ludwig ME. Fostering healthy attachment between substance dependent parents and their infant children. Journal of Infant, Child, and Adolescent Psychotherapy. 2012 Oct 1; 11(4): 376-86. [ Links ]
40.Anzman-Frasca S, Stifter CA, Paul IM, Birch LL. Infant temperament and maternal parenting self-efficacy predict child weight outcomes. Infant Behavior and Development. 2013 Dec 1; 36(4) :494-7. [ Links ]
41.McGrath MM, Meyer EC. Maternal self-esteem: from theory to clinical practice in a special care nursery. Children's Health Care. 1992 Sep 1; 21(4): 199-205. [ Links ]
42.Mercer RT. Parents at risk. Springer Publishing Co; 1990. [ Links ]
43.Farrow C, Blissett J. Maternal cognitions, psychopathologic symptoms, and infant temperament as predictors of early infant feeding problems: a longitudinal study. International Journal of Eating Disorders. 2006 Mar; 39(2): 128-34. [ Links ]
44.Chang Y, Fine MA, Ispa J, Thornburg KR, Sharp E, Wolfenstein M. Understanding parenting stress among young, low-income, African-American, first-time mothers. Early Education and Development. 2004 Jul 1; 15(3): 265-82. [ Links ]
45.Graham SM, Clark MS. Self-esteem and organization of valenced information about others: The" Jekyll and Hyde"-ing of relationship partners. Journal of Personality and Social Psychology. 2006 Apr; 90(4): 652. [ Links ]
46.Als H. A synactive model of neonatal behavioral organization: framework for the assessment of neurobehavioral development in the premature infant and for support of infants and parents in the neonatal intensive care environment. Physical & Occupational Therapy in Pediatrics. 1986 Jan 1; 6(3-4): 3-53. [ Links ]
47.Spielman V, Taubman-Ben-Ari O. Parental self-efficacy and stress-related growth in the transition to parenthood: A comparison between parents of pre-and full-term babies. Health & Social Work. 2009 Aug 1; 34(3): 201-12. [ Links ]
48.Cody AL. The effects of infant massage on the attitudes and perceptions of mothers who massage their hospitalized premature infants. The Wright Institute; 1995. [ Links ]
49.Müller ME. A questionnaire to measure mother-to-infant attachment. Journal of Nursing measurement. 1994 Jan 1; 2(2): 129-41. [ Links ]
50.Raval V, Goldberg S, Atkinson L, Benoit D, Myhal N, Poulton L, Zwiers M. Maternal attachment, maternal responsiveness and infant attachment. Infant Behavior and Development. 2001 Mar 1; 24(3): 281-304. [ Links ]
51.Roskam I, Meunier JC, Stievenart M. Parent attachment, childrearing behavior, and child attachment: Mediated effects predicting preschoolers' externalizing behavior. Journal of Applied Developmental Psychology. 2011 Jul 1; 32(4): 170-9. [ Links ]
52.Egeland B, Hiester M. The long-term consequences of infant day-care and mother-infant attachment. Child development. 1995 Apr; 66(2): 474-85. [ Links ]
53.Feldman R, Weller A, Sirota L, Eidelman AI. Testing a family intervention hypothesis: the contribution of mother-infant skin-to-skin contact (kangaroo care) to family interaction, proximity, and touch. Journal of Family Psychology. 2003 Mar; 17(1): 94. [ Links ]
54.Barnes CR, Adamson-Macedo EN. Perceived maternal parenting self-efficacy (PMP SE) tool: Development and validation with mothers of hospitalized preterm neonates. Journal of advanced nursing. 2007 Dec; 60(5): 550-60. [ Links ]
55.Shea E. Tronick E (Belester M. Yongman eds). The Maternal Self-Report Inventory, a research and Clinical Instrument for Assessing Maternal Self-Esteem. Theory and research in behavioral pediatrics. New York: Plenun Press. 1988; 4: 109-40. [ Links ]
56.Condon JT, Corkindale CJ. The assessment of parent-to-infant attachment: development of a self-report questionnaire instrument. Journal of Reproductive and Infant Psychology. 1998 Feb 1; 16(1): 57-76. [ Links ]
57.Jefferies AL, Canadian Paediatric Society, Fetus and Newborn Committee. Kangaroo care for the preterm infant and family. Paediatrics & child health. 2012 Mar 1; 17(3): 141-3. [ Links ]
 Correspondence:
Correspondence:
Christopher Barnes
c.barnes1@derby.ac.uk
Manuscript received: may 2021
Manuscript accepted: december 2021
Version of record online: june 2022


{kind=link}
{kind=link}
{kind=link}