










Serviços Personalizados
artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkEstudos de Psicologia (Natal)
versão impressa ISSN 1413-294Xversão On-line ISSN 1678-4669
Estud. psicol. (Natal) vol.22 no.3 Natal set. 2017
http://dx.doi.org/10.22491/1678-4669.20170027
PSYCHOBIOLOGY AND COGNITIVE PSYCHOLOGY
Neuropsychological assessment of patients with fibromyalgia
Avaliação neuropsicológica de pacientes com fibromialgia
Evaluación neuropsicológica de los pacientes con fibromialgia
Rubens GoulartI; Cinthia PessoaII; Império Lombardi JuniorIII
IPrefeitura Municipal de Santos
IIPrefeitura Municipal de Santos
IIIUniversidade Federal de São Paulo
ABSTRACT
The aim of the present study was to investigate associations among symptoms of depression, anxiety, pain perception and cognitive impairment in patients with a diagnosis of fibromyalgia. We evaluated 32 women volunteers with a diagnosis of fibromyalgia based on the criteria of the ACR. The control group was matched to the patient group for age, schooling and income. The volunteers were submitted to a neuropsychological battery focused on Memory, Attention, Executive Functions, Perceived Pain, Anxiety and Depression. Anxiety was more relevant than depression in the group of women with fibromyalgia, the perception of pain was very high and cognitive impairment was more evident in executive functions, especially planning and inhibitory control. Memory and attention were more impaired in the fibromyalgia group, especially on tasks that require executive functions. Patients with fibromyalgia seem to be less efficient in tasks related to executive functions.
Keywords: neuropsychology; fibromyalgia; executive function.
RESUMO
O escopo desse artigo é a investigação das associações entre sintomas de depressão, ansiedade, percepção da dor e déficits cognitivos em pacientes com diagnostico de fibromialgia. Avaliamos 32 mulheres com diagnósticos de fibromialgia segundo a ACR. O grupo controle foi equiparado em termos de idade, escolaridade e renda. Todas as voluntárias foram submetidas a uma bateria neuropsicológica focada em Memoria, Atenção, Funções Executivas, Dor Percebia, Ansiedade e Depressão. Ansiedade foi mais relevante que depressão para o grupo de mulheres com fibromialgia, ao mesmo tempo os níveis de dor foram mais altos e os prejuízos cognitivos mais evidentes foram relacionados às funções executivas, principalmente controle inibitório e planejamento. Memória e atenção estavam mais prejudicadas no grupo fibromialgia, principalmente naquelas tarefas que requisitam mais das funções executivas. Pacientes com fibromialgia parecem menos eficazes em tarefas relacionadas às funções executivas.
Palavras-chave: neuropsicologia; fibromialgia; função executiva.
RESUMEN
Investigar las asociaciones entre los síntomas de depresión, ansiedad, percepción del dolor y deterioro cognitivo en pacientes con diagnóstico de fibromialgia. Se evaluó a 32 mujeres voluntarias con un diagnóstico de fibromialgia según la ACR. El grupo de control fue emparejado con el grupo de pacientes por edad, escolaridad e ingresos. Los voluntarios fueron sometidos a una batería neuropsicológica enfocada en Memoria, Atención, Funciones Ejecutivas, Dolor Percibido, Ansiedad y Depresión. La ansiedad fue más relevante que la depresión en el grupo de mujeres con fibromialgia, la percepción del dolor fue muy alta y el deterioro cognitivo fue más evidente en las funciones ejecutivas, especialmente en la planificación y el control inhibitorio. La memoria y la atención estaban más afectadas en el grupo fibromialgia, especialmente en las tareas que requieren funciones ejecutivas. Las pacientes con fibromialgia parecen ser menos eficientes en tareas relacionadas con las funciones ejecutivas.
Palabras clave: neuropsicología; fibromialgia; función ejecutiva.
Following osteoarthritis, fibromyalgia is the second most frequent rheumatic disease in Brazil. According to different studies, the prevalence of this condition ranges from 2.5% (Senna et al., 2004) to 4.4% (Assumpção et al., 2009) in the national population, affecting the female sex more than the male sex. More than 40% of individuals with fibromyalgia are between 35 and 44 years of age. A number of studies have demonstrated some degree of cognitive impairment in such individuals, especially those who have comorbidities, such as anxiety and depression (Cherry, Weiss, Barakat, Rutledge, & Jones, 2009; Rodríguez-Andreu et al., 2009). Some authors (Kavitz & Kataz, 2015; Walitt et al, 2016) classify the collection of cognitive disorders, like executive dysfunctions and poorly task performance, as "fibro fog" a condition that reflect the sensory and behavioral impairment in this population. However, the specificities of this impairment have been under-explored in the literature (Ambrose, Gracely, & Glass, 2012).
The literature (Vierck, 2006), raises the hypothesis that the pains in fibromyalgia originate in the central nervous system, two classical studies found changes in the brain volume of patients, but in different regions: on Kuchinad et al (2007) about changes in the frontal medial cortex and left hippocampal, other from Schmidt-Wilcke et al. (2007), in the temporal and left thalamic region, however to the present the exact morphological deviations pertaining to FM is still under debate (Lin, Lee, & Weng, 2016). Outside the field of cerebral morphology on Kuchinad et al (2007), also found a relationship between the abnormal functioning of the dopaminergic system and the response to pain in fibromyalgia changes. Luerding et al. (2008) also described these alterations as related to ill cognitive functioning, who postulate that the alterations in the cerebral morphology and the functioning of the dopaminergic system justify the changes in the Executive Functions in patients with fibromyalgia. Consequently, to be situated how important is to study fibromyalgia related to mood changes, especially depression.
According to Lezak (2004), neuropsychology is the branch of psychology that investigates the association between behavior and neurophysiological processes, especially those related to the poor functioning of the neurological substrate and its behavioral expression. However, an analysis of the literature reveals a lack of studies that evaluate the neuropsychological aspects of fibromyalgia with complete testing that encompasses short-term memory, long-term memory, verbal memory, visual memory, attention and problem solving. Correa, Miró, Martínez, Sánchez and Lupiáñez (2011) report the same difficulty.
The aim of the present study was to investigate associations among symptoms of depression, anxiety, pain perception and cognitive impairment in patients with a diagnosis of fibromyalgia.
Methods
Participants
The sample size was calculated in a pilot study, which determined a total of 36 subjects in each group for a 5% significance level. The volunteers were women aged 18 years or older with a diagnosis of fibromyalgia based on the criteria of the American College of Rheumatology (Wolfe et al., 2010) recruited from the rheumatology clinic of the Santos Metropolitan University (Brazil). A control group of the same size was then formed by individuals from the general population through a public call in the press. The control group was matched to the patient group for age, schooling and income, so that the peers had exactly the same quantity of years of study and age, and an income in the same range of minimum wages.
Individuals with not controlled chronic diseases, such as diabetes and hypertension, other psychiatric, neurological or debilitating diseases, those with conditions that posed limitations regarding the performance of activities of daily living, those in need of surgery, those with conditions (other than fibromyalgia) that caused chronic pain, those with amputated limbs, pregnant women and individuals who did not have Portuguese as their primary language were excluded from the study. Moreover, only individuals with a sufficient score on the Mini Mental State Examination participated in the study. A score below the cutoff point is suggestive of severe cognitive impairment, which could impede the individual from undergoing the complete testing process (Bertolucci, Brucki, Campacci, & Juliano, 1994).
This study received approval from the Human Research Ethics Committee of the Federal University of São Paulo (Brazil) under process number 115.892 of 2012. All participants received clarifications regarding the objectives and methods of the study and signed a statement of informed consent.
Measures
All volunteers initially responded to a short patient history questionnaire based on the Brazilian Consensus on Fibromyalgia for the collection of socio-demographic data and symptoms (Heymann et al., 2010). A visual analog scale ranging from 0 (absence of pain) to 10 points (worst pain imaginable) was also administered to measure the level of pain (British Pain Society, 2008) at the time of evaluation and on days when the most severe pains, here called flare-ups.
Non-verbal semantic memory was evaluated using the Rey Complex Figure Test (Jamus & Mäder, 2005; Oliveira & Rigoni, 2010). Between phases two and three of the Rey Figure Test, the Digit Span Sub-test (forward and backward) of the Wechsler Adult Intelligence Scale (WAIS-III) (Weschler, 1997) was administered. This test is widely used as a safe measure of executive functions and attention that evaluates the retention of verbal information (working memory) (Figueiredo & Nascimento, 2007). The Victoria Stroop Test (Strauss, Sherman, & Spreen, 2006) was then administered, which is widely used for the evaluation of selective attention in neuropsychological research and clinical practice.
The first phase of the Rey Auditory Verbal Learning Test (RAVLT) was administered next, which consisted of a primary list of words, followed by an interference list (Diniz, Cruz, Torres, & Consenza, 2000; Magalhães & Hamda, 2010). After 20 minutes, the second phase was administered for the evaluation of delayed recall, in which the volunteer was asked to recall the words on the primary list. Next, a list of 36 words was presented and the volunteer was asked to circle the 15 words found on the primary list, for which the volunteer was awarded points for recalling the correct words and lost points for circling words not found on the primary list. This presentation of the last part of the test, written rather than oral as recommended by the Brazilian (Magalhães & Hamda, 2010) adaptation, followed the model presented by Lesak (2004), because this technique allows the examiner to separate between patients who are excessively careful and use a high confidence threshold in their responses those who make many errors because they do not really recognize the words.
After the second phase of the RAVLT, the third phase of the Rey Figure Test was administered, in which the volunteer was asked to reproduce the previously copied figure. If the time elapsed was less than 20 minutes, the examiner and patient awaited the remaining minutes to complete the allotted time.
The Trail Making Test (TMT) was then administered, which was originally was part of the Army Individual Test Battery developed by psychologists of the United States Army in 1944. This test is currently in the public domain and therefore its use does not require authorization (Strauss et al., 2006). Next, the Brazilian version of the Hospital Anxiety and Depression Scale (HADS) (Botega, Bi, Zomignan, Garcia, & Pereira, 1995) was administered. The authors of the original version of the scale (Zigmond & Snaith, 1983) sought to exclude common elements of between depression/anxiety and somatic diseases to avoid the overlap of physical symptoms, as occurs on more common scales for the evaluation of anxiety and depression.
The Modified Card Sorting Test (MCST) (Nelson, 1976) was administered last due to the level of frustration it induces, which could influence the responses on the previous tests if administered first. The MCST is a simplified version of the Wisconsin Card Sorting Test developed by Grant and Berg in 1948 for the evaluation of executive functions (Heaton, 1981) and the ability to shift cognitive strategies. After its standardization (Heaton, 1981), the card sorting test began to be used in neuropsychology. In the present study, the version by Nelson (1976) was used, which removed ambiguous stimuli.
Procedure
The volunteers who agreed to participate in the study were submitted to the tests in the order presented above in a one-hour session. The sequence was designed to diminish the interference of verbal and non-verbal tests on each other. A blinded rater with training in neuropsychology and more than five years of experience in clinical practice evaluated the copies of Rey Complex Figure Test, and corrected all the tests.
Statistical Analyses
Continuous data were expressed as mean, standard deviation and 95% confidence interval. The Independent Samples Student's t-test was used for the comparison of the groups regarding each of the variables of interest. The level of significance was set to 5% (p < 0.05). Pearson's linear correlation coefficients were calculated to determine the strength of associations among the variables, with r > 0.40 considered the minimum value for a moderate correlation (Dancey & Reidy, 2006).
Results
Comparisons Between Groups
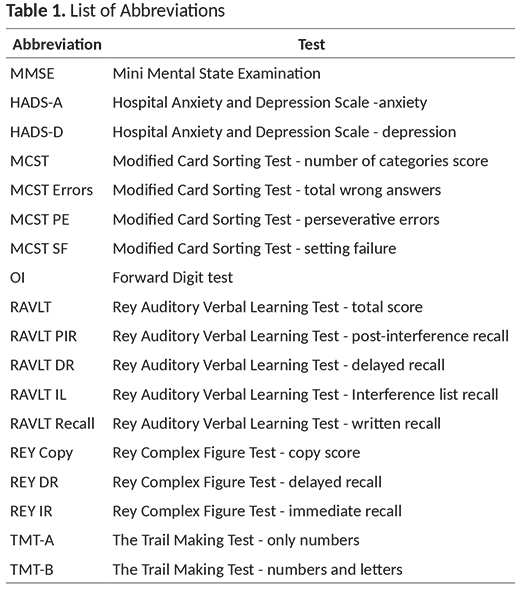
Table 1 displays a list of abbreviation of each test, and Tables 2 and 3 display the results of the tests in the two groups. Statistically significant differences (p < 0.05) between groups were found regarding current pain level, level of pain during a flare-up, HADS anxiety, HADS depression, Rey copy, Rey immediate recall (IR), Rey delayed recall (DR), RAVLT interference list (IL), RAVLT Recall, RAVLT Total, TMT-A and TMT-B.
Demographic Characteristics
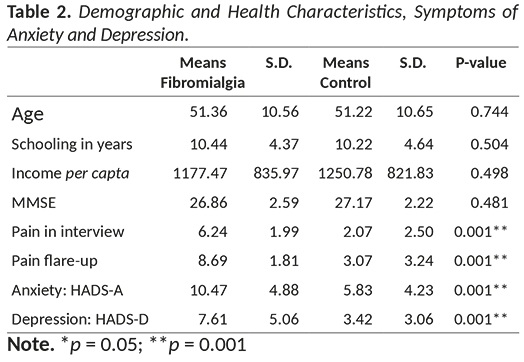
No significant differences between groups were found regarding age, schooling or income (Table 2).
Health Characteristics and Symptoms of Anxiety and Depression
Based on the answers to the patient history questionnaire, the mean time elapsed from diagnosis in the patient group until the interview was 40 months, but the mean time elapsed since the onset of pain was 91 months. As expected, the patient group reported significantly greater pain at the time of the interview and during a flare-up (p < 0.001), with more than a 4-point difference on the 10-point pain scale in comparison to the control group (Table 2).
The analysis of the HADS revealed that the fibromyalgia group exhibited a greater number of traits of both anxiety and depression comparison to the control group (Table 2). Moreover, the mean score of the fibromyalgia group on the anxiety subscale was higher than the expected cutoff point for the Brazilian population, which is 9 points (Botega, Pondé, & Silveira, 1998).
Neuropsychological Assessment
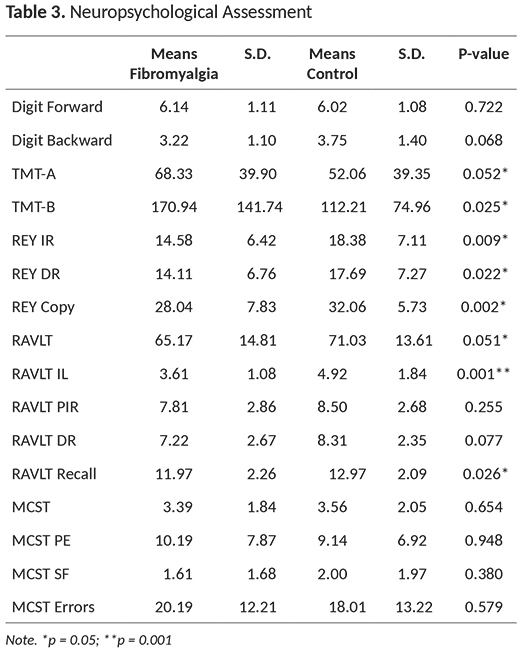
No significant differences in attention were found between groups, as demonstrated by the forward digit sub-test, the score of which was above six on the right side and is within the range expected for the general population (Baddeley, Anderson, & Eysenck, 2011; Miller, 1956/1994). Likewise, no significant differences between groups were found on the Stroop Test, as both groups had mean scores below that expected for the general population, which is from three to six digits (Figueiredo & Nascimento, 2007). This finding was likely due to the low level of schooling in both groups.
The results of the TMT demonstrate a tendency toward a slower performance among the patients with fibromyalgia on the tasks of sustained and alternating attention (Table 3). The mean of this group surpassed the 120-second time limit established as the cutoff point by the Brazilian Academy of Neurology (Nitrini et al., 2005) for part B. The p-value in the inter-group comparison for the second part was 0.025.
The fibromyalgia group demonstrated a general tendency toward a poor performance with regard to memory (Table 3), especially recall of the Rey figure, with scores higher than three points for IR and DR (p = 0.009 and 0.22, respectively). The differences were less accentuated regarding verbal memory evaluated using the RAVLT, with the fibromyalgia group demonstrating a significantly poorer performance only regarding the Interference List and Recognition List (p = 0.026).
The results of the tests that directly evaluate executive functions demonstrated a tendency toward a poorer performance on tasks that required greater cognitive integration, such as copying the Rey figure. However, no statistically significant difference between groups was found regarding the performance on the MCST.
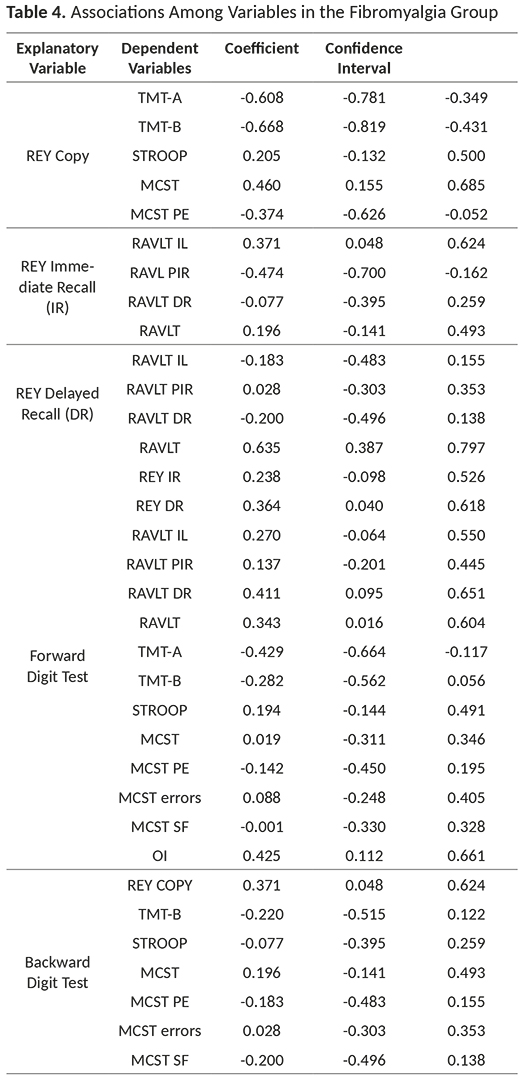
Associations among Variables
In the fibromyalgia group (Table 4), a moderate positive correlation was found between Rey DR and the RAVLT Total. A moderate positive correlation was found between Rey copy and MSCT, whereas a moderate negative correlation was found between Rey copy and TMT-B. A weak positive correlation was found between forward digit test and the following variables: Rey DR, RAVLT recall and RAVLT Total. A weak positive correlation was found between forward digit test and TMT A. Weak correlations were also found between backward digit test and Rey copy as well as between Rey IR and RAVLT IL.
Discussion
General Health Characteristics and Symptoms of Anxiety and Depression
The results of the Mini Mental State Examination (Table 2) used as an eligibility criterion revealed no statistically significant differences between groups, despite a slight tendency toward a poorer performance in the fibromyalgia group. In the opinion of the authors of the present study, this tendency was not clinically relevant. In a study conducted in Spain, however, comparing patients with fibromyalgia, neuropathic pain and diffuse pain, Rodríguez-Andreu et al. (2009) considered a difference of only 0.4 points among the three groups as being relevant. The mean scores in the fibromyalgia groups in both the study cited and the present investigation were the same.
Besides the inferential analysis, 72% and 36% of the fibromyalgia group scored above the cutoff points for anxiety and depression, respectively, whereas these figures were 25% and 8% in the control group. Previous studies report similar percentages. Barros et al. (2012) report anxiety and depression rates of 88% and 50%, respectively, in a sample from the city of Aracaju (northeastern Brazil). However, the authors used a cutoff point for depression lower than the value recommended for the Brazilian population in the validation study, which may explain the divergence regarding the rate of this characteristic. In a study conducted in Madrid, Spain, Vallejo, Rivera, Esteve-Vives and Rodríguez-Muñoz (2012) report mean scores of 12.68 and 10.12, resulting in rates of 79.7% and 34.9% of patients with answers indicative of anxiety and depression in a sample of 301 individuals.
The evaluation of attention span using the forward digit test and selective attention measured using the Stroop test revealed no significant difference between groups. While the Stroop test is considered adequate for measuring selective attention, cognitive flexibility and inhibitory control (Strauss et al., 2006), it is a very rapid and extremely specific measure, which may explain the lack of significant difference between groups. These characteristics of the sample seem to lend support to the hypothesis put forth by Grace, Nielson, Hopkins and Berg (1999) that only more difficult tasks and those that require greater executive control are affected in individuals with fibromyalgia.
The analysis of sustained and alternating attention measured using the TMT-B demonstrated a significantly slower performance in the fibromyalgia group, with a mean difference of more than 55 seconds. The capacity for executive planning exerts an influence on the results of this portion of the TMT. Moreover, the results of other tests revealed some degree of impairment in executive planning, which will be discussed later in this paper. The TMT-A evaluates attention and visual searching, whereas the TMT-B allows an evaluation of alternating attention and cognitive flexibility (Strauss et al., 2006). The fibromyalgia group was qualitatively slower on the task in Part A, which requires inhibitory control and planning, but much slower on Part B, responding negatively to the greater cognitive demand. This demand requires alternating attention, which is mediated by the central executive.
The TMT and Stroop test are used to investigate attention and executive functions. There is a close relationship between executive functions and attention, especially when one considers the currently most accepted concept of working memory (Baddeley et al., 2011), which places the central executive as the controller of attention. The work capacity of the central executive is limited by the attention span (Baddeley, 2000), which was below the normal range in the present sample. The findings reveal an overload of the executive-attention system in the fibromyalgia group whenever a more complex task is required.
The results of the evaluation of verbal memory measured by the RAVLT (interference list and recognition list) follow the same tendency. Both lists have "distracters" that require the renewal of the attention span and the latter list contains new words that should be discarded by the individual taking the test. Thus, the task requires greater effort on the part of the executive-attention system to discriminate the stimuli on the list, which requires greater cognitive skill. The findings lend support to the hypothesis put forth by Leavitt and Katz (2006) in a study entitled "Distraction As a Key Determinant of Impaired Memory in Patients With Fibromyalgia", which states that, when a distraction stimulus is added to a semantic evocation task, individuals with fibromyalgia have a substantially poorer performance than expected.
With RAVLT recall, 36 words are presented, among which only 15 are correct. Yet again, the respondent must face new stimuli that alter the habitual response pattern, inhibiting the impulse to circle words that did not compose the original list while correctly circling the recognized words. Such dual tasks require executive control. As previously stated in the methods this technique from Lesak (2004) allows the examiner to separate between excessively careful patients those more memory affected. The results of the RAVLT demonstrate similar learning curves in both groups, although both curves are below that expected for the mean age of the sample. Despite the similarity in the pattern, the fibromyalgia group retained a smaller number of words. The findings indicate that these patients benefit from repetition and learn when it is possible to concentrate on the stimuli in the same way as the control group or general population (represented by the normative table), but have a lower capacity to retain information. We conclude that the presentation of the list in written form was more sensitive than the standard form recommended by the Brazilian literature.
The results of the Rey Complex Figure test were stronger. The p-values were lower than 0.05 demonstrated a poorer performance in the fibromyalgia group. These findings are coherent, as pictorial memory is directly influenced by the capacity for planning, which is a component of executive functions (Baddeley, 2000) that seems to be impaired in the fibromyalgia group. The difference between groups diminished between the IR and DR phases of the test, as reported in studies that use both these parts of the Rey Figure Test (Lezak, 2004). The third phase is easier than the second, which seems to have favored the fibromyalgia group in the present study. Thus, under reasonable conditions with relatively low executive demands, patients with fibromyalgia learn, but have a poorer performance when dealing with competing stimuli, which is more directly associated with impaired executive functions than memory. Kim et al. (2012) report similar results in a study conducted in Korea, with significant differences between the fibromyalgia and control groups only on the Rey Figure Test and not the RAVLT.
No significant differences between groups were found on the MCST and both groups performed poorer than expected. In a sample also with 36 individuals in each group, Verdejo-Garcia, López-Torrecillas, Calandre, Delgado-Rodríguez and Bechara (2009) found that women with fibromyalgia had a poorer performance than the control group. However, we could find no other studies addressing this issue to counterbalance the analysis. According to Mesulam (2000), the MCST primarily evaluates problem-solving capacity, mental flexibility and the ability to shift strategies in the face of changing reinforcement. A number of authors report a poorer performance on the test among individuals with problems in the dorsolateral region of the prefrontal cortex, which is commonly associated with reasoning capacity and sensitive to one's level of schooling (Heaton, Chelune, Talley, Kay, & Curtiss, 2005; Van den Broek, Bradshaw, & Szabadi, 1993). In the validation study for the Frontal Assessment Battery, Beato et al. (2012) found an association between schooling and performance among 275 individuals, but no associations were found with age or gender. In Nelson's original study (1976), which proposes the version of the MCST used in the present investigation, the author found that age and schooling exerted an influence on the percentage of perseverative errors (PE) in relation to the total number of errors. Using the data displayed in Table 3, this figure was 50% in both groups. Recent studies confirm these influences (Caffarra, Vezzadini, Dieci, Zonato, & Venneri, 2004; Lineweaver, Bond, Thomas, & Salmon, 1999). As both groups in the present study had poorer performances than expected, one may suppose that the low level of schooling influenced this result, indicating that neither group exhibited an adequate ability to shift their behavior pattern in the face of the stimuli.
Considering the cognitive skills evaluated by the different tests, the findings demonstrate that planning and inhibitory control were affected in individuals with fibromyalgia when facing activities that required multiple tasks, which were limited by working memory, whereas no significant differences in comparison to the control group were found regarding problem solving and mental flexibility. The two groups were adequately matched for age, gender and schooling. The fibromyalgia group reported higher levels of pain than the control group, as expected. Moreover, anxiety was more prevalent in the fibromyalgia group than depression, although traits of both comorbidities were found.
Patients with fibromyalgia seem not to be able to manage several stimuli at the same time or those that compete with previously established stimuli, as evidenced by the results of the TMT-B and RAVLT. This may be due to the fact that such patients have a slower performance, as demonstrated on the TMT-A, or have difficulty maintaining inhibitory control, as demonstrated by the results of Rey copy, RAVLT recall and number of perseverative errors on the MCST, which was the same as that of the control group, but higher than expected. Working memory was also poorer than expected, as demonstrated by the digit span test. Thus, executive functions are impaired in patients with fibromyalgia and influence all other functions, which is a pattern known as "fibro fog" (Ambrose et al., 2012).
The lack of a linear correlation between anxiety/depression and neuropsychological functions or between pain and traits of anxiety/depression is not surprising. In a systematic review of the literature, Glass (2008) states the association between depression and cognitive dysfunction in patients with fibromyalgia seems to result more form the selection of the sample, as studies involving well-screened samples with regard to depressive symptoms do not report such an association. In a meta-analysis, Gelonch, Garolera, Rosselló and Pifarré (2013) concluded that most studies analyzed also found no association between anxiety/depression and cognitive dysfunction in patients with fibromyalgia, as such dysfunction persists after controlling the psychological variables. Based on the study by Grace et al. (1999), Genloch et al. (2013) also report that anxiety exerts a negative influence on attention tasks that require a longer time to solve. However, as the battery of tests used in the present study was chosen to allow a rapid evaluation, such effects were not evident.
The reviews of the literature cited above (Glass, 2008; Genloch et al., 2013) report the existence of a consensus in the field of fibromyalgia that pain is negatively related to cognitive performance, especially with regard to memory, attention and processing speed. Therefore, while the correlations between pain and neuropsychological function were not strong in the present study, the findings are coherent with data reported in the literature, as the results of the TMT-A, TMT-B, RAVLT and Rey Complex Figure Test revealed that the fibromyalgia group was slower and exhibited difficulties with regard to memory.
The moderate correlations found regarding memory were not noteworthy, as delayed pictorial recall (measured by Rey DR) and verbal recall (measured by the RAVLT) are components of the same function, namely, memory itself (Baddeley, 2000). The patients with fibromyalgia apparently benefitted from having a minimally preserved attention span on tasks that required memory. One may speculate that these correlations appeared in the fibromyalgia group and not the control group because individuals with fibromyalgia are less dependent on working memory and have more resources with regard to memory itself. However, this issue requires further research.
Regarding executive functions, direct correlations were found among tasks related to planning and execution (REY copy), the formation of categories on the MCST and inhibitory control (measured by the TMT-B) in both groups, which is in agreement with data described in the literature. Anxiety appeared to be more relevant than symptoms of depression in the group of women with fibromyalgia, as the perception of pain was very high and cognitive impairment was more evident in executive functions, especially planning and inhibitory control. However, a number of factors that could not be controlled due to restrictions regarding time and resources may have exerted an influence on the results, such as phases of dyslipidemia, the menstrual cycle and sleep quality. Nonetheless, the present investigation employed a complete battery of tests for the evaluation of neuropsychological characteristics, encompassing all functions commonly associated with fibromyalgia. Further studies should be conducted to examine the causal relationships between fibromyalgia and both cognitive and emotional symptoms, as the description of the cognitive characteristics of this condition is insufficient for an adequate understanding of the complexity of the symptoms.
In conclusion, anxiety was more relevant than symptoms of depression in the group of women with fibromyalgia, as the perception of pain was very high and cognitive impairment was more evident in executive functions, especially planning and inhibitory control. Memory and attention were more impaired in the fibromyalgia group, especially on tasks that require executive functions. Moreover, patients with fibromyalgia seem be more affected in relation to their executive functions, which impairs their performance at memory tests.
References
Ambrose, K. R., Gracely, R. H., & Glass, J. M. (2012). Fibromyalgia dyscognition: concepts and issues. Reumatismo, 64(4), 206-215. doi: 10.4081/reumatismo.2012.206 [ Links ]
Assumpção, A., Cavalcante, A. B., Capela, C. E., Sauer, J. F., Chalot, S. D., Pereira, C. A., & Marques, A. P. (2009). Prevalence of fibromyalgia in a low socioeconomic status population. BMC Musculoskeletal Disorders, 10(64). doi: 10.1186/1471-2474-10-64 [ Links ]
Baddeley, A. (2000). The episodic buffer: a new component of working memory? Trends in Cognitive Sciences, 4(11), 417-423. doi: 10.1016/S1364-6613(00)01538-2 [ Links ]
Baddeley, A., Anderson, M. C., & Eysenck, M. W. (2011). Memória. Porto Alegre: Artmed. [ Links ]
Barros, M. F. A., Silva, L. M. M., Nascimento, J. A., Oliveira, E. A., Cardia, M. C. G., Lucena, N. M. G., ... Carvalho, A. G. C. (2012). A percepção da qualidade de vida de pacientes fibromiálgicas submetidas à intervenção fisioterapêutica. Revista Brasileira de Ciências da Saúde, 16(2), 3-10. doi: 10.4034/RBCS.2012.16.s2.01 [ Links ]
Beato, R., Amaral-Carvalho, V., Guimarães, H. C., Tumas, V., Souza, C. P., Oliveira, G. N., & Caramelli, P. (2012). Frontal assessment battery in a Brazilian sample of healthy controls: normative data. Arquivos de Neuro-Psiquiatria, 70(4), 278-280. doi: 10.1590/S0004-282X2012005000009 [ Links ]
Bertolucci, P. H. F., Brucki, S. M. D., Campacci, S. R., & Juliano, Y. (1994). O mini-exame do estado mental em uma população geral. Impacto da escolaridade. Arquivos de Neuro-Psiquiatria, 52(1), 1-7. doi: 10.1590/S0004-282X1994000100001 [ Links ]
Botega, N. J., Bi, M. R., Zomignan, M. A., Garcia, C., & Pereira, W. A. B. (1995). Transtornos de humor em enfermaria de clínica médica e validação de escala de medida de ansiedade e depressão (HAD) de ansiedade e depressão. Revista de Saúde Pública, 29(5), 355-363. doi: 10.1590/S0034-89101995000500004 [ Links ]
Botega, N. J., Pondé, M., & Silveira, D. C. (1998). Validação da Escala Hospitalar de Ansiedade e Depressão (HAD) em pacientes epilépticos ambulatoriais. Jornal Brasileiro de Psiquiatria, 47(6), 285-289. [ Links ]
British Pain Society. (2008). Pain scales in multiple languages. Retrieved from http://www.britishpainsociety.org/pub_pain_scales.htm [ Links ]
Caffarra, P., Vezzadini, G., Dieci, F., Zonato, F., & Venneri, A. (2004). Modified Card Sorting Test.: normative data. Journal of Clinical and Experimental Neuropsychology, 26(2), 246-250. doi: 10.1076/jcen.26.2.246.28087 [ Links ]
Cherry, B. J., Weiss, J., Barakat, B. K., Rutledge, D. N., & Jones, C. J. (2009). Physical performance as a predictor of attention and processing speed in fibromyalgia. Archives Physical Medicine Rehabilitation, 90(12), 2066-2073. doi: 10.1016/j.apmr.2009.07.011 [ Links ]
Correa, A., Miró, H., Martínez, P., Sánchez, A. I., & Lupiáñez, J. (2011). Temporal preparation and inhibitory deficit in fibromyalgia syndrome. Brainand Cognition, 75(3), 211-216. doi: 10.1016/j.bandc.2010.11.005 [ Links ]
Dancey, C. P., & Reidy, J. (2006). Estatística sem matemática para psicologia: usando SPSS para Windows. Porto Alegre: Artes Médicas. [ Links ]
Diniz, L. F. M., Cruz, M. F., Torres, V. M., & Consenza, R. M. (2000). O teste de aprendizagem auditivo-verbal de Rey: normas para uma população brasileira. Revista Brasileira de Neurologia, 36(3), 79-83. [ Links ]
Figueiredo, V. L. M., & Nascimento, E. (2007). Desempenho nas duas tarefas do subteste Dígitos do WISC-III e do WAIS-III. Psicologia Teoria e Pesquisa, 23(3), 313-318. doi: 10.1590/S0102-37722007000300010 [ Links ]
Gelonch, O., Garolera, M., Rosselló, L., & Pifarré, J. (2013). Cognitive dysfunction in fibromyalgia. Revista de Neurología, 56(11), 573-588. Retrieved from https://www.neurologia.com/articulo/2013016/eng [ Links ]
Glass, J. M. (2008). Fibromyalgia and cognition. Journal of Clinical Psychiatry, 69(2), 20-24. Retrieved from http://www.psychiatrist.com/jcp/article/Pages/2008/v69s02/v69s0204.aspx [ Links ]
Grace, G. M., Nielson, W. R., Hopkins, M., & Berg, M. A. (1999). Concentration and memory deficits in patients with fibromyalgia syndrome. Journal of Clinical Experimental Neuropsychology, 21(4), 477-487. doi: 10.1076/jcen.21.4.477.876 [ Links ]
Heaton, R. K. (1981). Winconsin Card Sorting Test (WCST). Odessa: Psychological Assessment Resources. [ Links ]
Heaton, R. K., Chelune, G. J., Talley, J. L., Kay, G. G., & Curtiss, G. (2005). Teste Wisconsin de Classificação de Cartas: manual revisado e ampliado; adaptação e padronização brasileira. São Paulo: Casa do Psicólogo. [ Links ]
Heymann, R. E., Paiva, E. S., Helfenstein, M. J., Pollak, D. F., Martinez, J. E., Provenza, J. R., ... Fonseca, M. C. M. (2010). Consenso brasileiro do tratamento da fibromyalgia. RBR, 50(1), 56-66. doi: 10.1590/S0482-50042010000100006 [ Links ]
Jamus, D. R., & Mäder, M. J.(2005). A Figura Complexa de Rey e seu papel na avaliação neuropsychologic. Journal of Epilepsy and Clinical Neurophysiology, 11(4), 193-198. doi: 10.1590/S0482-50042010000100006. [ Links ]
Kavitz, H. M, & Katz, R. S. (2015) Fibrofog and fibromyalgia: a narrative review and implications for clinical practice. Rheumatology International, 35(7), 1115-1125. doi: 10.1007/s00296-014-3208-7 [ Links ]
Kim, S. H., Kim, S. H., Kim, S. K., Nam, E. J., Han, S. W., & Lee, S. J. (2012). Spatial versus verbal memory impairments in patients with fibromyalgia. Rheumatology International, 32(5):1135-1142. doi: 10.1007/s00296-010-1762-1 [ Links ]
Kuchinad, A., Schweinhardt, P., Seminowicz, D. A., Wood, P. B., Chizh, B. A., & Bushnell, M. C. (2007). Accelerated brain gray matter loss in fibromyalgia patients: premature aging of the brain? Journal of Neuroscience, 27(15), 4004-4007. doi: 10.1523/JNEUROSCI.0098-07.2007 [ Links ]
Leavitt, F., & Katz, R. S. (2006). Distraction as a key determinant of impaired memory in patients with fibromyalgia. Journal of Rheumatology, 33, 127-132. Retrieved from http://www.jrheum.org/content/33/1/127 [ Links ]
Lezak, M. D. (2004). Neuropsychological Assessment. New York: Oxford. [ Links ]
Lin C., Lee, S. H., & Weng, H. H. (2016). Gray matter atrophy within the default mode network of fibromyalgia: a meta-analysis of voxel-based morphometry studies. BioMed Research International, 2016, Article ID 7296125, 9 pages, 2016. doi:10.1155/2016/7296125
Lineweaver, T. T., Bond, M. W., Thomas, R. G., & Salmon, D. P. (1999). A normative study of Nelson's (1976) modified version of the Wisconsin Card Sorting Test in healthy older adults. The Clinical Neuropsychologist, 13(3), 328-347. doi: 10.1076/clin.13.3.328.1745 [ Links ]
Luerding, R., Weigand, T., Bogdahn, U., & Schmidt-Wilcke, T. (2008). Working memory performance is correlated with local brain morphology in the medial frontal and anterior cingulate cortex in fibromyalgia patients: Structural correlates of pain cognition interaction. Brain, 131(12), 3222-3231. doi: 10.1093/brain/awn229 [ Links ]
Magalhães, S. S., & Hamda, A. C. (2010). The Rey Auditory Verbal Learning Test: normative data for the Brazilian population and analysis of the influence of demographic variables. Psychology & Neuroscience, 3(1), 85-91. doi: 10.3922/j.psns.2010.1.011 [ Links ]
Mesulam, M. (2000). Principles of behavioral and cognitive neurology. New York: Oxford. [ Links ]
Miller, G. A. (1994). The magical number seven, plus or minus two: some limits on our capacity for processing information. Psychological Review, 101(2), 343-352. doi: 10.1037/0033-295X.101.2.343 (Original work published in 1956) [ Links ]
Nelson, H. E. (1976). A modified card sorting test sensitive to frontal lobe defects. Cortex, 12(4), 313-324. doi: 10.1016/S0010-9452(76)80035-4 [ Links ]
Nitrini, R., Caramelli, P., Bottino, C. M. C., Damasceno, B. P., Brucki, S. M. D., & Anghinah, R. (2005). Diagnóstico de Doença de Alzheimer no Brasil: avaliação cognitiva e funcional. Recomendações do Departamento Científico de Neurologia e do Envelhecimento da Academia Brasileira de Neurologia. Arquivos de Neuropsiquiatria, 63(3), 720-727. doi: 10.1590/S0004-282X2005000400034 [ Links ]
Oliveira, M., & Rigoni, M. (2010). Figuras Complexas de Rey: teste de cópia e de reprodução de figuras geométricas complexas. São Paulo: Casa do Psicólogo. [ Links ]
Rodríguez-Andreu, J., Ibáñez-Bosch, R., Portero-Vázquez, A., Masramon, X., Rejas, J., & Gálvez, R. (2009). Cognitive impairment in patients with fibromyalgia syndrome as assessed by the Mini-Mental State Examination. BMC Musculoskeletal Disorders, 10, 162-167. doi: 10.1186/1471-2474-10-162 [ Links ]
Schmidt-Wilcke, T., Luerding, R., Weigand, T., Jurgens, T., Schuierer, G., Leinisch, E., & Bogdahn, U. (2007). Striatal grey matter increase in patients suffering from fibromyalgia–a voxel-based morphometry study. Pain, 132(1), 109-116. doi: 10.1016/j.pain.2007.05.010 [ Links ]
Senna, E. R., De Barros, A. L., Silva, E. O., Costa, I. F., Pereira, L. V., Ciconelli, R. M., & Ferraz, M. B. (2004). Prevalence of reumathic diseases in Brazil: a study using the COPCOARD approach. The Journal of Reumathology, 31(3), 594-597. Retrieved from http://www.jrheum.org/content/31/3/594 [ Links ]
Strauss, E., Sherman, E. M. S., & Spreen, O. (2006). A compendium of neuropsychological tests. New York: Oxford. [ Links ]
Vallejo, M. A., Rivera, J., Esteve-Vives, J., & Rodríguez-Muñoz, M. F. (2012). Uso del cuestionario Hospital Anxiety and Depression Scale (HADS) para evaluar la ansiedad y la depresión en pacientes con fibromyalgia. Revista de Psiquiatría y Salud Mental, 5(2), 107-114. doi: 10.1016/j.rpsm.2012.01.003 [ Links ]
Van den Broek, M. D., Bradshaw, C. M., & Szabadi E. (1993). Utility of the Modified Wisconsin Card Sorting Test in neuropsychological assessment. British Journal Clinical Psychology, 32(3), 333-343. doi: 10.1111/j.2044-8260.1993.tb01064.x [ Links ]
Verdejo-García, A., López-Torrecillas, F., Calandre, E. P., Delgado-Rodríguez, A., & Bechara, A. (2009). Executive function and decision-making in women with fibromyalgia. Archives of Clinical Neuropsychology, 24(1), 113-122. doi: 10.1093/arclin/acp014 [ Links ]
Vierck, C. J. (2006). Mechanisms underlying development of spatially distributed chronic pain (fibromyalgia). Pain, 124(3), 242-263. doi: 10.1016/j.pain.2006.06.001 [ Links ]
Walitt, B., Čeko, M., Khatiwada, M., Gracely, J. L., Rayhan, R., VanMeter, J. W., & Gracely, R. H. (2016). Characterizing "fibrofog": Subjective appraisal, objective performance, and task-related brain activity during a working memory task. NeuroImage : Clinical, 11, 173-180. doi: 10.1016/j.nicl.2016.01.021 [ Links ]
Weschler, D. (1997). Wais-III: Escala Wechler de inteligência para adultos. São Paulo: Casa do Psicólogo, 2004. [ Links ]
Wolfe, F., Clauw, D. J., Fitzcharles, M. A., Goldenberg, D. L., Katz, R. S., Mease, P., ... Yunus, M. B. (2010). The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care & Research, 62(5), 600-610. doi: 10.1002/acr.20140 [ Links ]
Zigmond, A. S., & Snaith, R. P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67(6), 361-370. doi: 10.1111/j.1600-0447.1983.tb09716.x [ Links ]
 Correspondence address:
Correspondence address:
Rubens Goulart
Rua Comandante Bulcão Vianna, 855
Santos-SP, Brasil. CEP. 11090-000
E-mail: rubensgou@gmail.com
Recebido em 07.Mai.17
Revisado em 29.Ago.17
Aceito em 06.Out.17
Rubens Goulart, Master Degree, Health Sciences, Universidade Federal de São Paulo (UNIFESP-BS), Brazil, Clinical Director at the Physical and Intellectual Rehabilitation Specialized Center (CER-II), Municipal Health Department, Santos, São Paulo, Brazil. E-mail: rubensgou@gmail.com
Cinthia Pessoa, Master Degree, Health Sciences, Universidade Federal de São Paulo (UNIFESP-BS), Brazil, Psychologist at the Physical and Intellectual Rehabilitation Specialized Center, Municipal Health Department (CER-II), Santos, São Paulo, Brazil. E-mail: cinthia.pessoa@gmail.com
Império Lombardi Junior, Doctor in Rehabilitation, Universidade Federal de São Paulo (UNIFESP), Brazil, Associate Professor at Universidade Federal de São Paulo (UNIFESP), Brazil. E-mail: imperiolombardi@gmail.com

