










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkEstudos de Psicologia (Natal)
versão impressa ISSN 1413-294Xversão On-line ISSN 1678-4669
Estud. psicol. (Natal) vol.25 no.3 Natal jul./set. 2020
https://doi.org/10.22491/1678-4669.202000025
DOI: 10.22491/1678-4669.202000025
PSYCHOBIOLOGY AND COGNITIVE PSYCHOLOGY
An exploratory study using the network approach for quality of life and blood markers in a Brazilian population
Um estudo exploratório utilizando a aplicação da abordagem de rede à qualidade de vida e marcadores sanguíneos em uma população brasileira
Un estudio exploratorio utilizando la aplicación del enfoque de red a la calidad de vida y los marcadores sanguíneos en una población brasileña
Carolina Gontijo RibeiroI,II; Amalia Raquel Pérez-NebraIII,IV
IClínica Renalcare
IIEspaço Terapêutico Carla Abreu
IIIUniversidade de Brasília
IVUniversidad Internacional de Valencia
ABSTRACT
Although it is generally considered that quality of life (QoL) is related to blood markers, there are different approaches to the relation between these variables. We proposed here a dynamic interaction test. The aim was to ascertain which blood indicators relate to QoL through a network perspective in a common population. Answered a questionnaire and conducted blood exams 108 Brazilians. Of these, 84 were female, with a mean age of 43.85 years old (SD = 16.20). Data analysis indicated that CRP, T4 (FT4), Thyroid-stimulating hormone, and Cortisol bridges with QoL dimensions. The data suggest that QoL is related to blood markers, but some trends were less than the literature has indicated. This present study is exploratory. The relations are complex, and our findings suggest that the dynamic network structure expands the range of QoL and blood markers research, making it possible to investigate a new range of questions and analyses.
Keywords: quality of life; hormones; CRP; physiological process.
RESUMO
Embora se considere geralmente que a qualidade de vida (QV) está relacionada a marcadores sanguíneos, existem diferentes abordagens para a relação entre essas variáveis. Propomos aqui um teste de interação dinâmica. O objetivo foi verificar quais indicadores de sangue se relacionam com a QV através de uma perspectiva de rede em uma população comum. Respondeu a um questionário e realizou exames de sangue 108 brasileiros. Desses, 84 eram do sexo feminino, com média de idade de 43,85 anos (DP = 16,20). A análise dos dados indicou que a PCR, T4 (FT4), hormônio estimulante da tireoide e cortisol fazem pontes com dimensões de QV. Os dados sugerem que a QV está relacionada a determinados marcadores sanguíneos, mas algumas tendências foram inferiores às indicadas pela literatura. O presente trabalho é exploratório. As relações são complexas e nossos achados sugerem que a estrutura dinâmica da rede expande a gama de pesquisas sobre QV e marcadores sanguíneos, possibilitando a investigação de um novo espectro de perguntas e análises.
Palavras-chave: qualidade de vida; hormonas; CRP; processo fisiológico.
RESUMEN
Aunque generalmente se considera que la calidad de vida (QoL) esté relacionada con los marcadores sanguíneos, existen diferentes enfoques para la relación entre estas variables. Propusimos aquí una prueba de interacción dinámica. El objetivo era determinar qué indicadores sanguíneos se relacionan con la calidad de vida a través de una perspectiva de red en una población común. Respondieron a un cuestionario y realizaron exámenes de sangre a 108 brasileños. De estos, 84 eran mujeres, con una edad media de 43,85 años (DE = 16,20). El análisis de datos indicó que CRP, T4 (FT4), hormona estimulante de la tiroides y cortisol hacen puentes con dimensiones de calidad de vida. Los datos sugieren que la calidad de vida está relacionada con ciertos marcadores sanguíneos, pero algunas tendencias fueron menores de lo que la literatura ha indicado. El presente trabajo es exploratorio. Las relaciones son complejas, y nuestros hallazgos sugieren que la estructura dinámica de la red amplía el rango de QoL y las investigaciones de marcadores sanguíneos, lo que permite investigar un nuevo rango de preguntas y análisis.
Palabras clave: calidad de vida; hormonas CRP; proceso fisiológico.
The social changes and technological advances in medicine have increased life expectancy, and chronic conditions dominate. In this circumstance, quality of life (QoL) gains centrality in the health domain. QoL is a multidimensional and perceived concept, which varies from person to person (Pomeroy, Tennant, Mills, & Young, 2020). It implies that physiological, sociological, and psychological factors may contribute to a good or bad perception of QoL. Each of these factors has different ways of being measured and related to QoL.
Nevertheless, what they have in common is that they are mutually influenced. In the medical practice, health may be measured through traditional measurements, based on laboratory tests and clinical assessment (blood markers). However, they consider the illness more than the individual herself (Fleck, 2008). These measurements end up defining only health status and fail to address people's life contexts (Patrick, 2008; Pomeroy et al., 2020). According to Traverso-Yépez (2001), many professionals limit their efforts to finding a diagnosis for a physical problem that resolves the patient's symptoms and neglects to investigate psychological and social issues. Biomedical assessment is a starting point for a good QoL, but both are not synonymous (Chatterji & Bickenbach, 2008; Hevey, 2018). Accordingly, understanding a person's health does not involve the physiological aspects alone, and this person's perception of her situation. Thus, should be analyzed both: QoL and blood markers, and how they are related.
Defining QoL is problematic, as this involves both the global form – general satisfaction with life – and its division into components (physical, psychological, social relationships, and environment) (Pomeroy et al., 2020). Its conceptualization, and consequently operationalization, suffer critics. One of the most definitions used is from the World Health Organization (WHO). WHO defines QoL as "an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns" (The WHOQOL Group, 1995, p. 1404). This concept interrelates the environment with physical and psychosocial aspects, and independence and beliefs, providing a subjective assessment (Fleck, 2008). Furthermore, QoL is associated with the subjective assessment of a person's health and that person's subjective satisfaction with their health, personal relationships, ability to carry out routine tasks, and living conditions in general – as well as positive states, such as: feeling cheerful and happy (Chatterji & Bichenback, 2008).
Studies using the WHOQOL-BREF questionnaire describe QoL related to specific groups or blood tests. About groups: of older adults (Pereira et al., 2006; Roediger et al., 2019; Santos, Hugo, Leal, & Hilgert, 2013), multiple sclerosis (Pomeroy et al., 2020); physical activity (Maruf, Akinpelu, & Salako, 2013; Ponte & Fedosse, 2016), and specific professions (Vieira, Cerqueira, & Freitas, 2013), among others. Studies using the WHOQOL-BREF and tests have included: cholesterol (Chew, Sidik, & Ghazali, 2015; Fontela, Winkelmann, Pretto, & Berleze, 2015), blood pressure (Melchiors et al., 2010; Tavares, Martins, Diniz, Dias, & Santos, 2011), and body mass index (Castro, Matsuo, & Nunes, 2010). There are few studies relating the WHOQOL-BREF with the blood indicators that are broadly used. Hence, we will consider in the present study: Cortisol, Ferritin, tT4 and thyroid-stimulating hormone (TSH) (Hettiarachchi, Fonseka, Gunasekara, Jayasinghe, & Maduranga, 2014), Cortisol (Knuth et al., 2016), TSH and tT4 (Vigário et al., 2014), and Red Blood cells and Platelets based on the exploratory nature of the study. The later exams are usually asked for physicians, but there is no hypothesis associated with them. The literature tends to report studies undertaken in the Europe-United States axis; samples with high income, high educational levels, and specific groups. Accordingly, there is a gap in the literature to conduct studies with the general population, including different markers, and we will offer initial results to it.
The QoL and blood markers relationship has been studied in different ways. Usually, aspects of the system in a sequential process (Hevey, 2018): one variable predicts the other in a line. The point is that sometimes blood markers predict psychological states (Pulopulos & Kozusznik, 2018; Tariq, Wert, Cheriyath, & Joshi, 2018), or vice-versa (Martin & Dobbin, 1988). Sometimes they are correlated (Fried et al., 2019; Pandrc et al., 2017) or show moderators (Afonso, Pérez-Nebra, Modesto, & Zambonato, accepted; Fried et al., 2019; Martin & Dobbin, 1988; Zambonato & Pérez-Nebra, accepted). Hence, they have a mutual influence and can be conceptualized as a reciprocal interaction system: in a dynamic network process (Cramer et al., 2016; Hevey, 2018). Although the network perspective is a new branch in psychology, the basic idea of a network is not new (Cramer et al., 2016; Fonseca-Pedrero, 2018).
The network analysis offers a potential gain to study the biopsychosocial model. The biopsychosocial model suggests mutually and dynamic interaction between psychological, biological, interpersonal, and contextual variables as a complex system (Hevey, 2018). The network structure allows analyzing the model's core structural and relational features (Hevey, 2018). The recent proposition to study health psychology using the network approach comes from Hevey (2018). As the proposition is new, we will describe a network and how it can be applied here.
The network is an answer to the biomedical model (Cramer et al., 2016). When describing a psychopathological or a psychoneuroimmunology process, it is difficult to identify a common cause as a condition of many symptoms. The idea is that the symptoms co-occur because they mutually influence each other (Cramer et al., 2016). A network is complex because there are many connections between symptoms, and any of them can trigger the network to starts an improvement (or deterioration) of the system. It is also possible to infer the structure by examining the importance of the variables according to their centrality (Cramer et al., 2016; Fonseca-Pedrero, 2018).
The present work had as its general aim to describe the relationship between QoL and blood markers. Its specific objectives were: representing the dynamics of the QoL dimensions, representing the markers' dynamic, and the conjoint relation in a population with low income and low educational level. We first hypothesized that the general dimension of the WHOQOL-BREF will be the central items in the instrument structure (H1). The blood markers were selected by their know relation with QoL, their mechanism (inflammatory or protective), or their everyday use in the medical area. In the blood markers structure, we hypothesize that the hormones will be the most central (H2). Finally, there are well-known related variables to QoL in the whole structure, like Cortisol, Ferritin, thyroid hormones (Hettiarachchi et al., 2014; Vigário et al., 2014). Thus we hypothesized that those markers will be related to QoL (H3). It is also possible to hypothesize that c-reactive protein and Neutrophils to Lymphocyte ratio has a negative relation to QoL as both are inflammation markers (H4) (Faugere et al., 2018; Fried et al., 2019; Levy & Bavishi, 2018; Roediger et al., 2019). Vitamin D is related to increase the absorption of nutrients, so its relation will be positive with QoL (H5). Other default exams will be included as they are commonly asked by physicians and explore the relation.
Method
Participants
The participants were 108 users of a community service project provided by the university laboratory, the Community Treatment Center (CAC), in a region with stable daily global solar radiation (MJ/m2 varying between 16 and 18 during the year). Users usually come to this university laboratory because services are almost free (2 euros per exam pack). Thus, if they have work application demands, periodic exams, or any other issue, they use the service. Their mean age was 43.85 years old (SD=16.20), of whom 84 were female. Regarding educational level, 70.4% of the sample had graduated from high school education, and 15.7% had a basic level of education (13.9% missing values); 50.9% had no permanent jobs; 40.7% had permanent jobs (8.3% of missing),;13.9% working a mean of 40 hours per week (range between 6 and 60; 57.4% of missing). Informed consent was obtained from all individual participants included in the study, and the authors received only the patient's registration number.
The sample was selected for convenience. When the patient arrived in the laboratory, we offer to participate in a study. We include exams that are not in the original petition (e.g., Vitamin D). We could receive up to 6 patients per day because it is the number of available comfortable chairs to wait for the cortisol exam collection. After the first cycle of collection, we could not collect any more data from disturbing the laboratory routine.
Criterions for selection were: be a Brazilian speaker, have a legal age, if not, it was necessary to have a signature of the responsible (only one case), be fasting for 8 hours, not have consumed alcoholic beverage in the last 24 hours, and available to rest from the collection of Cortisol. The first stage of exclusion criteria was to declare having any health issue (infection, HIV positive, cancer, pregnancy, diabetes) or any other known injury that could interfere with the exams. The second stage of exclusion criteria was based on the exam results (e.g., high TSH levels), which we explain in the statistical procedure above.
Instruments
QoL was measured using the WHOQOL-BREF, developed by the World Health Organization (WHO) (Fleck et al., 2000; Kossakowski et al., 2016). The instrument showed merely acceptable fitting index (x2/df = 1.67; CFI = .72; RMSEA = .10). It has 26 questions; two generals, relating to the quality of life (omega = .62), and 24 referents to the instrument's domains (physical, psychological, social relationships, and environment, omegas of .79, .82, .68, and .76, respectively). According to the original instrument, the questions were answered on a scale from 1 to 5, with anchoring between intensity, frequency, and satisfaction. Higher scores indicate better quality of life (Fleck, 2000; Fleck et al., 2000).
Demographic data were evaluated: the reason for the exam, age, gender, education, work, history of the disease, exposure to the sun, and physical activity.
Paper and Pen Procedure
The patients who went to the CAC during morning time (6:00 am to 8:30 am) were invited to participate in the study. Before starting, the study's aim was explained to them, and they were requested to sign the terms of free and informed consent. However, many were reluctant or were worried about answering, as most could not read (were illiterate), while others were unable to understand the question or specific vocabulary, causing them to require help in order to answer the questionnaire and – frequently – making it necessary to read the questionnaire to the participants in its entirety. The questionnaires were answered using paper and pen. The average time to answer was 40 minutes (SD = 20). The research was approved by the Research Ethics Committee in Brazil, Centro Universitário de Brasília (05/05/2016/ 51340715.2.000.0023).
Blood Collection Procedure
The fluid samples (blood) were taken following a 30 minute rest and an 8 hours fast using three tubes with 4ml, two of them were gel separator vacuum tubes and the other, EDTA. The method used in the equipment were: enzymatic with hexokinase to conduct Glycemia test; immunoturbidimetry to CRP and Ferritin test; electrochemiluminescence, to hormones, and fluorescent flow cytometry, to complete blood test. Glycemia kit was GLIC3; Cortisol was CORT II; CRP was CRPLX, and Ferritin was FEER2. The equipment used was INTEGRA 400 plus. In the hormones tests, tT3 used FT3 III; TSH used TSH; tT4 used FT4 III, and Vitamin D used VitD II. The equipment used for these tests was Cobas e 411. The reagent used for the complete blood test was CELLPACK, SULSOLYSER, STROMATOLYSER -4DL, and the equipment name is XS-1000. We took the reference values used in the (CAC) and, in general, the population was healthy (6 exceptions: 3 for high glycemia, 2 with problems of the thyroid, 1 high Ferritin – no difference was found in these cases in QoL).
The reference values for each biochemical marker were: Glycemia (70 a 99 mg/dl), Cortisol (4.3 a 22.4 g/dL), CRP (< 0.30 mg/dL), tT3 (80 a 180ng/dl), TSH (0.55 a 4.78 mcUI/mL), tT4 (0.7–1.8 ng/dl), Vitamin D (> 30.0 ng/ml), Ferritin (22.0 a 322.0 ng/mL for men and 10.0 a 291.0 ng/mL for women), Red blood cells (4.6 a 6.2 milion/ml for men and 4.2 a 5.4 milion/ml for women), Hemoglobin (12.0 a 18.0 g/dL), Hematocrits (42%-52% for men and 36%-48% for women), Leukocytes (3.800 a 9.800/mm3), Neutrophils (1.800 a 7.700/mm3), Lymphocyte (1.000 a 4.800/mm3), Platelets (140.000 a 4000.000/mm3).
Data Analysis
The data were tabulated and analyzed using the SPSS program and R packages (Bringmann et al., 2019; Epskamp, Cramer, Waldorp, Schmittmann, & Borsboom, 2018; Fonseca-Pedrero, 2018) (qgraph, glasso, polycor, and psych). Initially, we conducted a confirmatory factor analysis (CFA) for the WHOQOL-BREF instrument and omegas reliability tests (between 0.7 and 0.8) to confirm if it was possible to use the instrument as it was initially proposed. We tested the normality assumption, although it is not required for network analysis. We have two participants with non-normal TSH (75.0 and 6.3 mU/mL), and in glycemia, we have six participants slightly above 125 mg/dL. Any of them declare a diabetes issue in the questionnaire, which made it impossible to exclude them from data collection previously. For TSH, we decided to exclude the cases because the normality was disturbed, and in the glycemia case, the normality was not impaired, and it does not disturb the analysis.
The network estimation was conducted in three ways to test the three hypotheses. First, for the WHOQOL-BREF instrument structure (Epskamp, 2013; Epskamp et al., 2018). The network analyses were based on all connections, and we estimate the centrality of the items of the WHOQOL-BREF. Second, we conducted the same test with the blood markers to see the structure between blood and QoL variables. The third analysis includes both symptoms and how they are connected. We test controlling sex and age differences.
Results
Figure 1 shows the inferred network of the dynamics between the 26 WHOQOL-BREF items. The network's global structure reflects that the dimensions of the WHOQOL-BREF instrument are connected, but the clusters are partially clear. Item 12, from Psychological dimension ("How satisfied are you with yourself"), followed by item 26 from General dimension ("How satisfied are you with your health") were the most significant strength (S). They were expected to influence more items (EI) (S = 2.98; EI = 2.86; and S = 1.56, EI = 1.63, respectively).
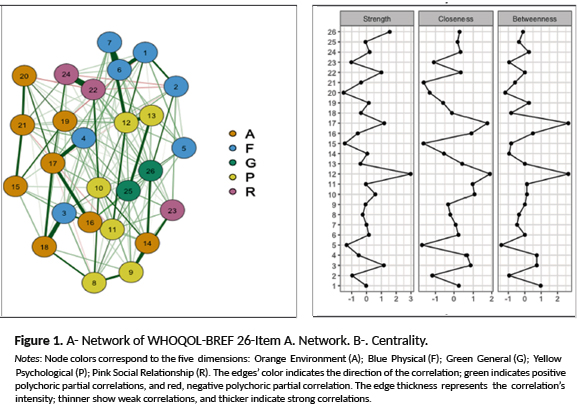
The strength and expected influence average of each dimension were calculated, and the General dimension was the most influence, followed by Psychological, Physical, Social Relationship and Environment (S averages = .74; .47; -.21; .06; -.37; EI averages .94; .59; -.23; -.32; -.35). This result supports Hypothesis 1, where the General dimension was the most central.
Figure 2 presents the relationship between blood markers. In general, it is possible to see clusters of red blood cells, white blood cells, and thyroid hormones. It shows that hematocrits and hemoglobin were the most central and expected influent variables (respectively S = 1.96; 1.83; EI = 1.87; 2.01). These results contradict Hypothesis 2 of this work, which proposes that hormones would be the center. It is also important to notice that sex is a central variable related to several blood markers.
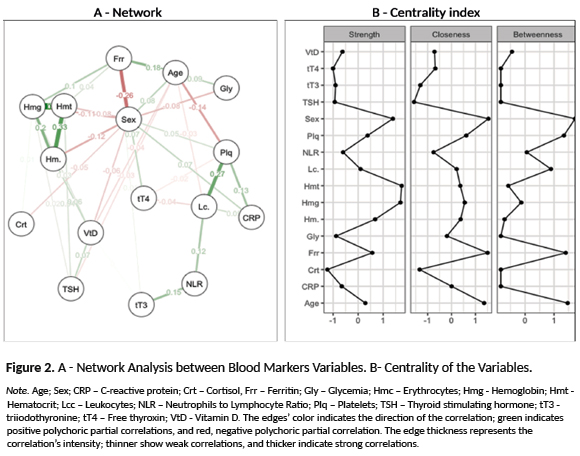
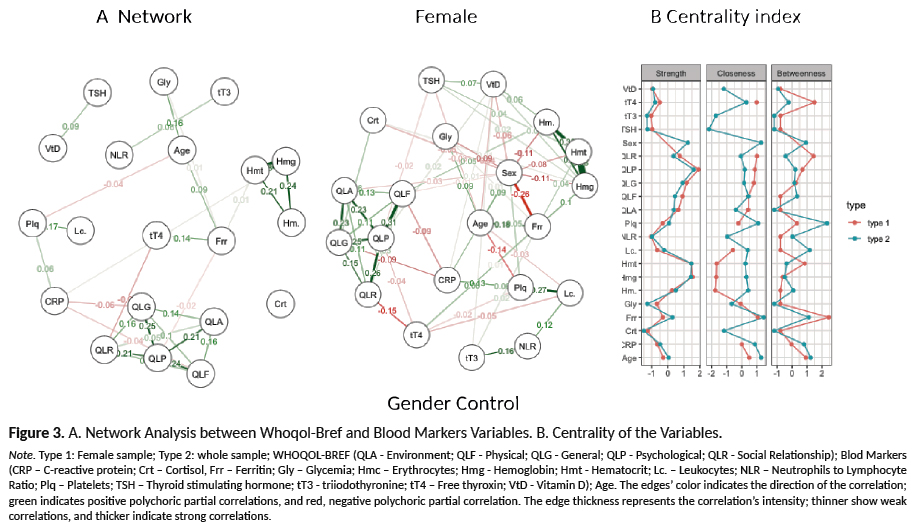
Figure 3 indicates that, in general, the variables have a weak relation. We split the sample between males and females as the blood markers could show differences by gender. Although hematocrits and hemoglobin's centrality was evident, their relations with WHOQOL-BREF dimensions were weak or inexistent. In this case, C-reactive protein (CRP), Free thyroxin (tT4), Thyroid-stimulating hormone (TSH), and Cortisol (Crt) were the blood markers that rebound negatively in the WHOQOL-BREF dimensions, particularly CRP. These results partially support H3, where cortisol and thyroid-stimulating hormone would be the main bridges, but not Ferritin. H4 was also partially supported, were of the inflammatory markers only CPR remained. Although, H5 shows no support, as Vitamin D does not appear related to QoL. Age and sex do not show differences in WHOQOL-BREF to mediate any process.
Network analysis can also show mediation effects (Hevey, 2018). In this case, CRP, tT4, Crt, and TSH also work as a mediator between QoL and the other blood markers, as in the case of Vitamin D.
Discussion
The present study aimed to describe the relationship between QoL and blood markers through a network perspective. We first hypothesized that the general dimension of the WHOQOL-BREF would be the central items in the instrument structure (H1). Results show that in the QoL instrument, the General dimension serves its original purpose; however, it could improve its psychometric parameters.
Regard the blood markers; we hypothesize that the hormones will be the most central (H2). The red cell's series are central and affect the other blood markers refuting H2. We hypothesized that Cortisol, Ferritin, thyroid hormone markers would be related to QoL (H3) c-reactive protein, and Neutrophils to Lymphocyte ratio has a negative relation to QoL (H4), Vitamin D would have a positive relationship with QoL (H5). Results show a relation with PCR, tT4, TSH, and Crt as partially expected, supporting H3, supporting partially H4, and refuting H5.
Cortisol presented a weak positive relationship with QoL-general. Cortisol increases resistance to the stressor event in an acute way (Fleck, 2000). This result strongly suggested the importance of possible contextual moderators between Cortisol and QoL (Júnior & Abramov, 2011). Another possible explanation is based on the type of analysis used. As in network analysis, the correlation used is partial; thus, it could show some relation in the bivariate analysis. We tested this alternative hypothesis, but the results were non-significant. In our sample, Cortisol shows a weak non-significative positive relation with all QoL variables.
CRP is a protein that monitors the processes of infection and inflammation, facilitating the diagnosis of inflammatory diseases (Guimarães, De Brito, Góes, Reis, & Reges, 2014). Accordingly, it can indicate the existence of some inflammations or infections. An increase in CRP indicates some inflammation in the organism, impairing the individual's health – and explaining CRP's negative relationship with the Physical and Psychological dimensions and with the perception of QoL-general.
It may be inferred that inflammation worsens the subject's QoL perception. It uses to increases pain and reduces energy (Levy & Bavishi, 2018). It hinders sleep and the ability to work and carry out everyday tasks (Fried et al, 2019). It also worsens the individual's mental health (Faugere et al, 2018). In other words, it leads to worse health conditions and, accordingly, worse perception of QoL as we found here. However, as in Roediger et al. (2019), there are exceptions where they did not found a relationship between QoL and CRP.
The increase in tT4 was related to reductions in the Psychological and Social Relationships dimensions. Studies have corroborated a worsening in Psychological perception (Knuth et al., 2016) with tT4, in which the cognitive (memory and concentration) and affective (self-esteem and positive feelings) conditions reduce, and there is a poor perception of social relationships, in which the personal relationships, support, and sexual activity worsen. tT4 is also vital for brain functioning, such as reasoning and the ability to concentrate, and the body's growth and development (Knuth et al., 2016). Considering this and the result obtained in the present research, it indicates that high levels of tT4 hinder the Psychological dimension.
We did not have any specific hypothesis related to red blood cells. However, it presented a positive relationship with the Physical dimension, as the greater the production of red blood cells, the better was the perception of QoL-physical. There is a positive relation between red blood cells and oxygenation in the body (Uzunian & Birner, 2008). With higher levels of oxygen in the blood, the physical condition improves, and - consequently - she is more inclined, and has the energy, to undertake everyday activities and work. Hereafter, it is surprising that red blood cells are not related to other dimensions.
Some limitations may be indicated. We have difficulties with the questionnaires applied. We need to adapt the psychological instruments to low-educational levels. Although we have sex differences in the study, unfortunately, we do not control the menstrual cycle, and we could not equilibrate the number of men as they do not go to do blood exams in the research period. Another point was that the participants invited to participate in the study were undertaking tests, which took significant time, suggesting that they may have some rates outside the reference values. However, the parameters presented were generally normal.
Although these limitations, as far as the authors can tell, this is the first time this type of study has been undertaken. Furthermore, it is necessary to consider the profile of this study's participants. It could be understood as an innovation. It was undertaken with a general population, with a low educational level, and which was underprivileged. The literature typically neglects such groups. As an agenda, a future study on the role of inflammatory markers in other contexts could be undertaken (e.g., presenteeism at work – going to work when sick or compulsive work at home). Also, to seek some longitudinal study, it could be interesting to study Cortisol in hair.
Conclusion
This study met the initial aims to describe an exploratory relationship between QoL and blood markers and indicate that these aspects interact – showing a comprehensive view of the theme, considering that the subject's health condition/illness involves the combination of biological, psychological, and social variables. Although the results, in general, support the literature, where CPR and Thyroid hormones have a negative relation to QoL, and Cortisol, positive, the relations are weaker than what is usually presented. Moreover, Vitamin D, Ferritin, and Neutrophils and Lymphocytes ratio were not related to QoL in this sample.
The relevance of the present work relates to the contribution of results involving a different profile of participants from that found in the literature.
References
Afonso, R., Pérez-Nebra, A. R., Modesto, J. G., & Zambonato, A. (Accepted). Negative life events, coping and biological markers: an analysis based on the Transactional Model of Stress. Brasília, DF. [ Links ]
Bringmann, L. F., Elmer, T., Epskamp, S., Krause, W., Schoch, D., Wichers, M., ... Snippe, E. (2019). What do centrality measures measure in psychological networks? Journal of Abnormal Psychology, 128(8), 892-903.doi: 10.1037/abn0000446 [ Links ]
Castro, M. R. P., Matsuo, T., & Nunes, S. O. V. (2010). Características clínicas e qualidade de vida de fumantes em um centro de referência de abordagem e tratamento do tabagismo. Jornal Brasileiro de Pneumologia, 36(1), 67-74. doi: 10.1590/S1806-37132010000100012 [ Links ]
Chatterji, S., & Bickenbach, J. (2008). Considerações sobre qualidade de vida. In M. P. A. Fleck (Eds.), A avaliação de qualidade de vida: guia para profissionais da saúde (pp. 40-47). Porto Alegre: Artmed. [ Links ]
Chew, B., Sidik, S. M., & Ghazali, S. S. (2015). Negative effects of diabetes–related distress on health-related quality of life: An evaluation among the adult patients with type 2 diabetes mellitus in three primary healthcare clinics in Malaysia. Health and Quality of Life Outcomes, 13(1), 187.doi:10.1186/s12955-015-0384-4 [ Links ]
Cramer, A. O. J., Van Borkulo, C. D., Giltay, E. J., Van Der Maas, H. L. J., Kendler, K. S., Scheffer, M., & Borsboom, D. (2016). Major depression as a complex dynamic system. PLoS One, 11(12). doi: 10.1371/journal.pone.0167490 [ Links ]
Epskamp, S. (2013). New Features in qgraph. In R Package documentation (pp. 1-12). Retrieved from http://www2.uaem.mx/r-mirror/web/packages/qgraph/qgraph.pdf [ Links ]
Epskamp, S., Cramer, A., Waldorp, L., Schmittmann, V., & Borsboom, D. (2012). qgraph: Network visualizations of relationships in Psychometric Data. Journal of Statistical Software, 48(4), 1-18. doi: 10.18637/jss.v048.i04 [ Links ]
Faugere, M., Micoulaud-Franchi, J. A., Faget-Agius, C., Lançon, C., Cermolacce, M., & Richieri, R. (2018). Quality of life is associated with chronic inflammation in depression: A cross-sectional study. Journal of Affective Disorders, 227, 494-497. doi: 10.1016/j.jad.2017.11.061 [ Links ]
Fleck, M. P. A. (2000). O instrumento de avaliação de qualidade de vida da Organização Mundial da Saúde (WHOQOL-100): características e perspectivas. Revista Ciência e Saúde, 5(1), 33-38. doi: 0.1590/S1413-81232000000100004 [ Links ]
Fleck, M. P. A. (2008). Problemas conceituais em qualidade de vida. In M. P. A Fleck (Ed.), A avaliação de qualidade de vida: guia para profissionais da saúde (pp. 19-28). Porto Alegre: Artmed. [ Links ]
Fleck, M. P. A., Louzada, S., Xavier, M., Chachamovich, E., Vieira, G., Santos, L., & Pinzon, V. (2000). Aplicação da versão em português do instrumento abreviado de avaliação da qualidade de vida "WHOQOL-bref". Revista de Saúde Pública, 34(2), 178-183. doi: 10.1590/S0034-89102000000200012 [ Links ]
Fonseca-Pedrero, E. (2018). Análisis de redes en psicología. Papeles del Psicólogo, 39(1),1-12. doi: 10.23923/pap.psicol2018.2852 [ Links ]
Fontela, P. C., Winkelmann, E. R., Pretto, L. M., & Berleze, E. M. (2015). Sleep respiratory disorders and clinical profile in patients with type 2 diabetes mellitus. International Archives of Otorhinolaryngology, 19(1), 67-73. doi: 10.1055/s-0034-1395998 [ Links ]
Fried, E. I., von Stockert, S., Haslbeck, J. M. B., Lamers, F., Schoevers, R. A., & Penninx, B. W. J. H. (2019). Using network analysis to examine links between individual depressive symptoms, inflammatory markers, and covariates. Psychological Medicine, 1-9. doi: 10.1017/s0033291719002770 [ Links ]
Guimarães, A. O., De Brito, A. M. G., Góes, C. S., Reis, A. A., & Reges, A. L. S. (2014). Proteína C reativa e velocidade de hemossedimentação na avaliação laboratorial de processos inflamatórios. Scire Salutis, 4(1), 6-16. doi: 10.6008/SPC2236-9600.2014.001.0001 [ Links ]
Hettiarachchi, M., Fonseka, C. L., Gunasekara, P., Jayasinghe, P., & Maduranga, D. (2014). How does the quality of life and the underlying biochemical indicators correlate with the performance in academic examinations in a group of medical students of Sri Lanka? Medical Education Online, 19. doi: 10.3402/meo.v19.22772 [ Links ]
Hevey, D. (2018). Network analysis: A brief overview and tutorial. Health Psychology and Behavioral Medicine, 6(1), 301-328. doi: 10.1080/21642850.2018.1521283 [ Links ]
Júnior, C. A. M. & Abramov, D. M. (2011). Fisiologia essencial. Rio de Janeiro: Guanabara Koogan. [ Links ]
Knuth, B., Cocco, R., Radtke, V., Medeiros, J., Oses, J., Wiener, C., & Jansen, K. (2016). Stress, depression, quality of life and salivary cortisol levels in community health agents. Acta Neuropsychiatrica, 28(3), 165-172. doi: 10.1017/neu.2015.58 [ Links ]
Kossakowski, J. J., Epskamp, S., Kieffer, J. M., Van Borkulo, C. D., Rhemtulla, M, & Borsboom, D. (2016). The application of a network approach to Health-Related Quality of Life (HRQoL): Introducing a new method for assessing HRQoL in healthy adults and cancer patients. Quality of Life Research, 25(4), 781-792. doi: 10.1007/s11136-015-1127-z [ Links ]
Levy, B. R., & Bavishi, A. (2018). Survival advantage mechanism: Inflammation as a Mediator of positive self-perceptions of aging on longevity. Journals of Gerontology - Series B, 73(3), 409-412. doi: 10.1093/geronb/gbw035 [ Links ]
Martin, R. A., & Dobbin, J. P. (1988). Sense of Humor, Hassles, and Immunoglobulin A: Evidence for a Stress-Moderating Effect of Humor. The International Journal of Psychiatry in Medicine, 18(2), 93 105. doi: 10.2190/724B-3V06-QC5N-6587 [ Links ]
Maruf, F. A., Akinpelu, A. O., & Salako, B. L. (2013). Self-Reported quality of life before and after aerobic exercise training in individuals with Hypertension: A randomized controlled trial. Psychology: Health & Well-being, 5(2), 209-224. doi: 10.1111/aphw.12005 [ Links ]
Melchiors, A. C., Correr, C. J., Pontarolo, R., Santos, F. O. S., & Souza, R. A. P. (2010). Qualidade de vida em pacientes hipertensos e validade concorrente do Minichal Brasil. Arquivos Brasileiros de Cardiologia, 94(3), 357-364. doi: 10.1590/S0066-782X2010000300013 [ Links ]
Pandrc, M. S., Ristić, A., Kostovski, V., Stanković, M., Antić, V., Milin-Lazović, J., & Ciric, J. (2017). The effect of early substitution of subclinical hypothyroidism on biochemical blood parameters and the quality of life. Medical Biochemistry, 36(2):127-36. doi: 10.1515/jomb-2017-0007 [ Links ]
Patrick, D., (2008). A qualidade de vida pode ser medida? Como? In M. P. A. Fleck (Ed.), A avaliação de qualidade de vida: Guia para profissionais da saúde (pp. 29-39). Porto Alegre: Artmed. [ Links ]
Pereira, R. J., Cotta, R. M. M., Franceschini, S. C. C., Ribeiro, R. C. L, Sampaio, R. F., Priore, S. E., & Cecon, P. R. (2006). Contribuição dos domínios físico, social, psicológico e ambiental para a qualidade de vida global de idosos. Revista de Psiquiatria do Rio Grande do Sul, 28(1), 27-38. doi: 10.1590/S0101-81082006000100005 [ Links ]
Pomeroy, I. M., Tennant, A., Mills, R. J., & Young, C. A. (2020). The WHOQOL-BREF: A modern psychometric evaluation of its internal construct validity in people with multiple sclerosis. Quality of Life Research, 29(7): 1961-1972. doi: 10.1007/s11136-020-02463-z [ Links ]
Ponte, A. S., & Fedosse, E. (2016). Lesão Encefálica Adquirida: impacto na atividade laboral de sujeitos em idade produtiva e de seus familiares. Ciência e Saúde Coletiva, 21(10), 3171-3182. doi: 10.1590/1413-812320152110.19162016 [ Links ]
Pulopulos, M. M., & Kozusznik, M. W. (2018). The moderating role of meaning in life in the relationship between perceived stress and diurnal Cortisol. The International Journal on the Biology Stress, 21(3), 203-210. doi: 10.1080/10253890.2018.1429397 [ Links ]
Roediger, M. A., Marucci, M. F. N., Duim E. L., Santos, J. L. F., Duarte, Y. A. O., & Oliveira, C. (2019). Inflammation and quality of life in later life: findings from the health, well-being and aging study (SABE). Health and Quality of Life Outcomes, 17(26). doi: 10.1186/s12955-019-1092-2 [ Links ]
Santos, C. M., Hugo, F. N., Leal, A. F., & Hilgert, J. B. (2013). Comparison of two assessment instruments of quality of life in older adults. Revista Brasileira de Epidemiologia, 16(2), 328-337. doi: 10.1590/S1415-790X2013000200009 [ Links ]
Tariq, A., Wert, Y., Cheriyath, P., & Joshi, R. (2018). Effects of long-term combination LT4 and LT3 therapy for improving hypothyroidism and overall quality of life. Southern Medical Jounal, 111(6): 363-369. doi: 10.14423/SMJ.0000000000000823 [ Links ]
Tavares, D. M. S., Martins, N. P. F., Diniz, M. A., Dias, F. A., & Santos, N. M. F. (2011). Qualidade de vida de idosos com hipertensão arterial. Revista Enfermagem, 1(3), 438-444. doi: 10.5216/ree.v13i2.10876 [ Links ]
The WHOQOL Group (1995). The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Social Science and Medicine, 4(10), 1403-1409. doi: 10.1016/0277-9536(95)00112-k [ Links ]
Traverso-Yépez, M. (2001). A interface Psicologia Social e Saúde: perspectivas e desafios. Psicologia em Estudo, 6(2), 49-56. doi: 10.1590/S1413-73722001000200007 [ Links ]
Uzunian, A., & Birner, E. (2008). Circulação Biologia. In A. Uzunian & E. Birner (Eds.), Biologia (pp. 632-653). São Paulo: Harbra. [ Links ]
Vieira, G. C., Cerqueira, P. H. A., & Freitas, L. C., (2013). Qualidade de vida dos profissionais do setor madeireiro de Vitória da Conquista-BA. Floresta e Ambiente, 20(2), 231-237. doi: 10.4322/floram.2013.002 [ Links ]
Vigário, P. D. S., Chachamovitz, D. S. D. O., Teixeira, P. D. F. D. S., Rocque, M. D. L., Santos, M. L. D., & Vaisman, M., (2014). Exercise is associated with better quality of life in patients on TSH-suppressive therapy with levothyroxine for differentiated thyroid carcinoma. Arquivos Brasileiros de Endocrinologia & Metabologia, 58(3), 274-281. doi: 10.1590/0004-2730000002968 [ Links ]
Zambonato, A., & Pérez-Nebra, A. R. (accepted). Negative Events and Biochemical Markers: Test for the Moderating Effect of Humor. Trends in Psychology. [ Links ]
Received in 29.jun.20
Revised in 07.dec.20
Accepted in 31.dec.20
Carolina Gontijo Ribeiro, Graduada em Psicologia pelo Centro Universitário de Brasília (Uniceub), Analista de RH na clínica Renalcare e Psicóloga clínica no Espaço Terapêutico Carla Abreu. Endereço para correspondência: Shin QI 07 conjunto 17 casa 07 – Lago Norte, Brasília DF. Telefone: (61) 99158-8059. Email: caroolgr@gmail.com
Amalia Raquel Pérez-Nebra, Doutora em Psicologia Social, do Trabalho e das Organizações pela Universidade de Brasília (UnB), Pós-doutora no Institut d'Investigació em Psicologia del RRHH, del Desenvolupament Organitzacional i de la Qualitat de Vida Laboral (IDOCAL), Universitat de València (UV), é Professor Visitante na Universidade de Brasília e Universidad Internacional de Valencia. Email: amaliaraquel.perez@campusviu.es


{kind=link}