










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkEstudos de Psicologia (Natal)
versión impresa ISSN 1413-294Xversión On-line ISSN 1678-4669
Estud. psicol. (Natal) vol.26 no.1 Natal ene./mar. 2021
http://dx.doi.org/10.22491/1678-4669.20210004
10.22491/1678-4669.20210004
PSYCHOBIOLOGY AND COGNITIVE PSYCHOLOGY
Social isolation in Brazil: analysis of adherence, influence of personality, well-being and psychological distress
Isolamento social no Brasil: análise da adesão, influência da personalidade, bem-estar e angústia psicológica
Aislamiento social en Brasil: análisis de adherencia, influencia de la personalidad, bienestar y angustia psicológica
Daniela Sacramento ZaniniI; Evandro Morais PeixotoII; Josemberg Moura de AndradeIII; Mônica Moreira CamposI; Jose Luis Pais RibeiroIV
IPontifícia Universidade Católica de Goiás
IIUniversidade São Francisco
IIIUniversidade de Brasília
IVUniversidade do Porto. Instituto Universitário Lisboa
ABSTRACT
At the end of 2019, the world was shaken by a public health problem, COVID-19. To combat it, the WHO recommended social isolation which, despite the benefits in reducing contagion, can have psychological consequences. This article aimed to evaluate the sociodemographic and personal characteristics that can influence social isolation. A total of 1,914 individuals, aged between 14 and 86, 77.7% of whom were women, from 25 Federative Units in Brazil, participated in the study. It was observed that people with elementary or secondary education only, with incomes below the minimum wage, of black ethnicity and who seek information about the pandemic on social networks, are those who have observed significantly less social isolation. People who did not adhere to isolation had higher levels of positive affect and stress mindset and lower levels of conscientiousness. The findings suggest the importance of recognizing relevant social and psychological characteristics for engaging in restrictive measures.
Keywords: coronavirus; social isolation; personality; wellbeing; psychological distress.
RESUMO
No fim de 2019 o mundo foi surpreendido por um problema de saúde pública, a COVID-19. Como medidas para seu enfrentamento a OMS recomendou o isolamento social que, apesar dos benefícios para diminuição do contágio pode trazer consequências psicológicas. Este artigo buscou avaliar as características sociodemográficas e pessoais que podem influenciar no isolamento social. Participaram do estudo 1.914 indivíduos, com idades entre 14 e 86 anos, 77,7% mulheres, de 25 Unidades Federativas do Brasil. Observou-se que pessoas com ensino fundamental ou médio, com renda inferior a um salário mínimo, de etnia negra e que buscam informações sobre a pandemia em rede sociais são as que realizaram significativamente menos isolamento social. Pessoas que não aderiram ao isolamento apresentavam maiores níveis de afetos positivos e mentalidade sobre o estresse e menores níveis de conscienciosidade. Os achados sugerem a importância de reconhecer características sociais e psicológicas relevantes para o engajamento em medidas restritivas.
Palavras-chave: coronavírus; isolamento social; personalidade; bem-estar; angústia psicológica.
RESUMEN
A finales de 2019, el mundo se sorprendió con un problema de salud pública, COVID-19. Como medidas para combatirlo, la OMS recomendó el aislamiento social, que, a pesar de los beneficios para reducir el contagio, puede tener consecuencias psicológicas. Este artículo buscó evaluar las características sociodemográficas y personales que pueden influir en el aislamiento social. 1.914 personas, con edades comprendidas entre 14 y 86 años, 77,7% mujeres, de 25 unidades federativas en Brasil participaron en el estudio. Se observó que las personas con educación primaria o secundaria, con ingresos inferiores al salario mínimo, de etnia negra y que buscan información sobre la pandemia en las redes sociales son aquellas que han logrado un aislamiento social significativamente menor. Las personas que no adhirieron al aislamiento tenían niveles más altos de afectos positivos y mentalidad sobre el estrés y niveles más bajos de concienciosidad. Los resultados sugieren la importancia de reconocer características sociales y psicológicas relevantes para participar en medidas restrictivas.
Palabras clave: coronavirus; aislamiento social; personalidad; bienestar; angustia psicológica.
At the end of 2019, the world was shaken by a health issue that would soon spread and turn into a pandemic (World Health Organization [WHO], 2020). Although some researchers had suggested that a health problem of this magnitude could occur (Wolfe, 2011), the general public was not privy to this information.
It was with this feeling of incredulity that the world observed the progression of the new Coronavirus (SAR-CoV-2) and the concomitant illness, COVID-19. Appearing for the first time in the Chinese city of Wuhan, in December 2019, the new Coronavirus had made its way to Europe by January 2020, ostensibly in the Italian region of Lombardy. The virus then spread across the planet leading the WHO, in March 2020, to proclaim a state of pandemic (WHO, 2020). COVID-19 and its consequences rapidly sparked concern, distress and fear among the global population (Ahorsy et al., 2020).
Generally speaking, the health authorities have indicated that, of those people infected with Coronavirus, 80% may evolve asymptomatically, 15% may require hospitalization and 5% may experience severe respiratory difficulty evolving into respiratory insufficiency and the need for mechanical ventilation. Moreover, COVID-19 has a mortality rate that is considered relatively low (around 2% of cases) (Ministério da Saúde , 2021). However, due to its rapid spread and capacity to infect (Werneck & Carvalho, 2020), this 'low' mortality rate and low level of complication may represent a significant number of people who have the potential to bring the health services to a state of collapse. In such cases, it could even trigger an increase in mortality due to problems in getting adequate medical help.
A study published in the Lancet in March 2021 revealed a rate of demand for beds in intensive care units (ICU) in Italy, as a consequence of COVID-19, equating to between 9% and 11% of those infected (Remuzzi & Remuzzi, 2020). This means that for every 100 people infected with Coronavirus, between nine and 11 have required intensive care, the occupation of a bed in ICU, the need for a respirator and specialized medical care. Considering that, in the equivalent period of the previous year (March 2020), the forecast rate of infection was 30,000 people, this meant there would be a demand for around 4,000 ICU beds, exceeding the availability in the country's health system (Remuzzi & Remuzzi, 2020). The outcome was viewed with great consternation by the world's population through the reporting in the media of a health system in collapse, professionals working grueling hours and significant social turmoil.
As measures to cope with the pandemic and its grave consequences, the WHO recommended systematic social isolation in order to reduce the possibility of contagion, give control to the health services and to encourage the advancement of studies into the virus and effective forms to combat it (vaccines, drugs, etc.) (Werneck & Carvalho, 2020). Social isolation seeks to restrict the movement of individuals to avoid the spread of the virus or contagion (Centers for Disease Control and Prevention [CDC], 2020a). It is a coping measure used to control epidemics and pandemics (Brooks et al., 2020), particularly when no other means to combat and treat the disease are available.
Nevertheless, despite the benefits of social isolation to diminish contagion (Werneck & Carvalho, 2020) a number of stressors, especially psychological stressors, may be linked to it. These include increased anxiety, depression and stress (Maia & Dias, 2020), confusion, anger, and even posttraumatic stress (Brooks et al., 2020). The main stress factors reported are the length of time in social isolation, fear of the disease, insufficient information, reduced incomes, frustration, and stigma (Brooks et al., 2020). Add to this the stress of living in uncharted territory where the solution and/or forms of coping are yet to be discovered.
In Brazil, social isolation was proposed as a measure to contain the advance of COVID-19 through the Quarantine Law (Lei nº. 13.979/2020). However, autonomy was given to the state governments to take decisions about the best strategies to address the pandemic, depending on the health situation in each city and/or federal state (Moreira, 2020). Moreover, the lack of explicit guidance from the federal government and the issuance of confusing measures and guidance from the governors, at the various levels, and the health authorities, created a lack of consensus in terms of health actions at the national level. Thus, the government of the Federal District of Brasilia was the first to declare social isolation on March 10, 2020, followed by other state governors, for example the governor of Goiás, on March 16. Despite this, although some states took a little longer to proclaim social isolation as an official measure, with the consequent closure of schools and non-essential businesses, the overall message was to practice social isolation, to avoid circulation in the streets, overcrowding, and large gatherings. In this regard, it may be said that, since March 2021, Brazil has been experiencing a situation of social isolation with significant potential to impact the population's mental health.
The present article seeks to evaluate the sociodemographic and personal characteristics that may have an impact on the observance of social isolation and their effects on the levels of psychological distress in the Brazilian population.
Method
Participants
A total of 1,914 individuals took part in this study (22.3% male and 77.7% female), aged between 14 and 86 (mean = 34.88, SD = 13.61), from 24 federal states and the Federal District. In terms of the geographical region of the country, 56 (2.9%) came from the North, 571 (29.8%) from the Northeast, 537 (28.1%) from the Midwest, 587 (30.7%) from the Southeast and 163 (8.5%) from the South. As for the level of education, 0.4% of respondents stated they had completed elementary education, 0.8% incomplete high school, 5.1% completed high school, 26.6% incomplete college education, 17.8% completed college education, 9% incomplete postgraduate education and 40.2% completed postgraduation. The inclusion criteria were as follows: agreeing to participate in the study by means of a free and informed consent form and the completion of the responses to the instrument.
Instruments
Sociodemographic and Social Isolation Questionnaire. For this study, a questionnaire was developed aimed at evaluating sociodemographic data such as age, sex, marital status, level of family income, etc. Questions were also developed related to adherence to social isolation, motivation to adhere to social isolation, existence of people defined as in the risk group and children in the family group observing social isolation, level of activity during social isolation, etc.
Kessler Psychological Distress Scale (K10). A translation and adaptation of the k10 scale was carried out for the evaluation of psychological distress in the Brazilian population, consisting of a single-factor structure with a Cronbach's alpha reliability coefficient equal to 0.90.
This instrument consists of 10 self-report items evaluating the level of emotional distress related to having experienced stress in the previous 30 days. The items are answered based on a 5-point Likert scale (1 = not at all, to 5 = all the time). Higher scores signify a higher level of psychological distress and psychic suffering (Andrews & Slade, 2001).
Life Satisfaction Scale (LSS). Devised by Diener, Emmons, Larsen, and Griffin (1985), the LSS evaluates cognitive aspects of subjective wellbeing, considered the gold standard for the evaluation of the construct (Diener, 2000). This scale consists of five self-report items that evaluate the respondent's level of satisfaction with life by means of a 7-point Likert-type response scale. The Brazilian version was adapted and validated by Zanon et al. (2014) and their adaptation studies demonstrate good evidence of accuracy and validity, and preliminary standards (Hutz, Zanon, & Bardagi, 2014).
Positive and Negative Affect Scale (PANAS). Originally developed by Watson, Clark, and Tellegen (1988), PANAS evaluates the emotional components of subjective wellbeing through positive affect (PA) and negative affect (NA). The scale is composed of 20 words that express emotions, of which 10 relate to positive affect and 10 to negative affect, answered by way of a 5-point Likert scale (1 = not even a little, and 5 = very much). In Brazil, the scale was adapted by Zanon and Hutz, in 2014, presenting studies that demonstrate good reliability, evidence of factorial validity and preliminary standards (Zanon & Hutz, 2014).
Personality Mini-Markers. The markers for the evaluation of personality in the FFM model were originally developed by Hutz et al. (1998). It is an instrument comprising 64 adjectives divided into five subscales that complete the statement "I am a person...". The response scale is a 5-point Likert scale with the following extremes: 1 = I completely disagree, and 5 = I completely agree. Subsequently, Hauck Filho, Machado, Teixeira, and Bandeira (2012) developed a short version with 25 adjectives whose response procedures mirror those of the original scale. The authors reported satisfactory validity evidence and reliability coefficients via Cronbach's alpha between 0.61 (for openness) and 0.83 (for extroversion).
Stress Mindset Measure (SMM). Developed by Crum, Salovey, and Achor (2013), the SMM evaluates the beliefs that an individual maintains in respect of the consequences that stress can exert on his performance and growth. The scale consists of 8 items of which four are positive (e.g., the effects of stress are positive and may be useful) and four negative (e.g., living with stress exhausts my health and energy), answered by way of a Likert-type scale in which the responses range from 0 = I strongly disagree to 4 = I strongly agree. An adaptation study and an evaluation of evidence of validity of the SMM for the Brazilian context demonstrated the adequacy of the single-factor structure as well as good indicators of reliability, with Cronbach's alpha equal to 0.868 and McDonald's omega 0.869 (Peixoto, Rocha, Franco, & Bueno, 2019). For the composition of the final stress mindset score, the negative items should be inverted, and all the items summed. The higher the scores, the higher the positive mindset levels.
Procedures
Participants were recruited through announcements in the press and social media (Whatsapp, Facebook, Instagram,etc.). The invitation for voluntary participation had to be certified by means of the Free and Informed Consent Form in which anonymity was guaranteed, as was the ability to withdraw at any stage of the study without obligation. In addition, the researchers' contact details were supplied should further information about the study be required or if any complications arose as a result of participating in the study. The participants had to answer the instruments virtually (online) using the Google Forms platform. All responses were registered between April 4 and April 17, 2020, in other words around one month after the onset of the pandemic in Brazil.
Data Analysis
The data were analyzed in line with the objectives of the study. Descriptive and inferential statistics were used with the aid of the SPSS 26.0 statistical software package. A characterization of the sociodemographic profile was carried out using contingency tables according to adherence to social isolation. The categorical variables were displayed using absolute frequency (n) and relative frequency (%) while the continuous variables were displayed using the mean and standard deviation. The normality of the data was ascertained using the Kolmogorov-Smirnov test. A comparison of the categorical exploratory variables with adherence to social isolation was conducted using Pearson's chi-square and post-hoc chi-square tests with Bonferroni correction when significant differences were found in contingencies above 2x2, as advocated by MacDonald and Gardner (2000). The comparison of the continuous exploratory variables with adherence to social isolation was performed through the application of the Mann-Whitney test. The effect size was established using Cohen's d test. In order to isolate the effect of social isolation on wellbeing, meaning of life, psychological distress and personality, a Covariance Analysis was performed using as covariables those which demonstrated significance/effect on isolation in a previous analysis (sex, marital status, profession, level of education, family income, working from home, how busy they were while in isolation, number of people at home in the risk group and how many times a week they would go out). A confidence interval of 95% (p < 0.05) was adopted for all the analyses.
Results
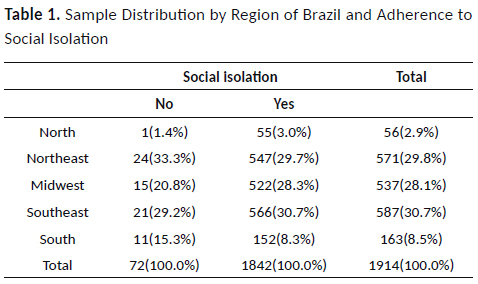
The highest participation by the respondents was observed in the Northeast, Midwest and Southeast regions, in decreasing order. As a whole, these three regions of Brazil accounted for almost 90% of all responses. Moreover, the majority of the sample (1,842 participants) observed social isolation during the data collection period (as opposed to 72 who did not), with adherence to social isolation being lowest in the Northeast and the South. The data relating to the social isolation variable, taking into consideration the participant's geographical region, can be viewed in Table 1.
It is important to stress that, among the people who observed social isolation, 29.2% report having done so to comply with health recommendations, 42.4% to avoid infecting others and 28.4% to avoid catching the disease themselves. Moreover, of the total number of participants, only 11 (0.6%) reported having received a diagnosis of Covid-19 at the time of the data collection. All of these observed social isolation. Table 2, below, shows the characterization of the sociodemographic profile of the sample according to whether or not isolation was observed.
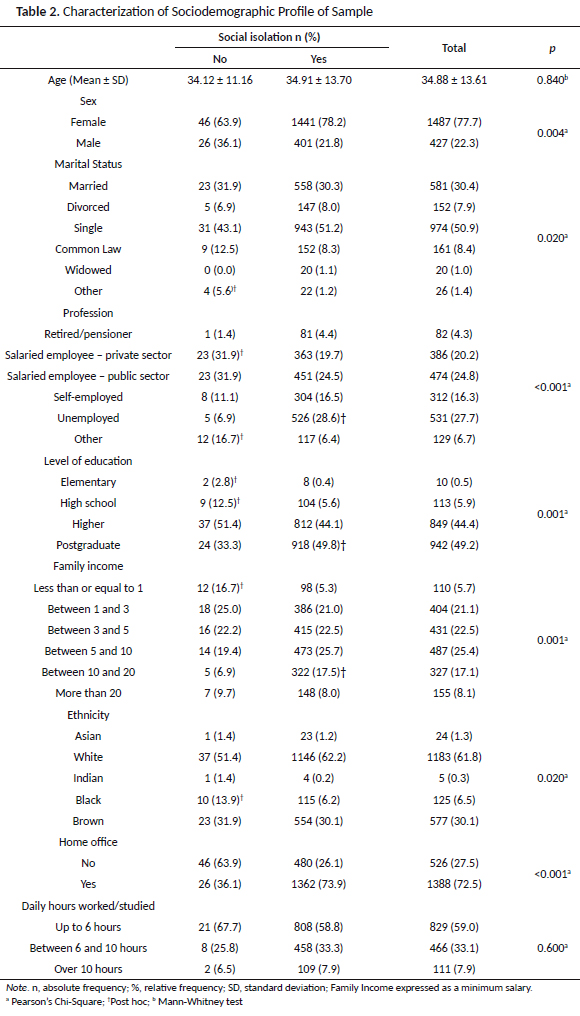
As can be seen from Table 2, no significant differences were observed in terms of age (p = 0.84) or study/working hours (p = 0.60) with the observance or nonobservance of social isolation. All the other variables presented with significant differences, with women, the unemployed, those with a postgraduate degree, with incomes between 10 and 20 minimum salaries and those studying or working from home, observing significantly greater social isolation. However, individuals who are classified in other forms of relationship (marital status), with elementary or high school education, with incomes below one minimum salary and ethnic blacks, are those who observe social isolation to a significantly lower degree.
Also noted was the influence of the perception of living conditions, confidence in the health service, ways to obtain COVID-19 information and diagnosis on adherence or nonadherence to social isolation. People who stated they remained busy during isolation and who get their information from groups or social networks and who go out four to six times a week, are those who observe significantly less social isolation. However, people who have higher numbers of individuals in the risk group living in their homes, who get their information about the pandemic from the television and do not go out at all or just one to three times a week, are those who present with significantly higher adherence to social isolation (see Table 3).
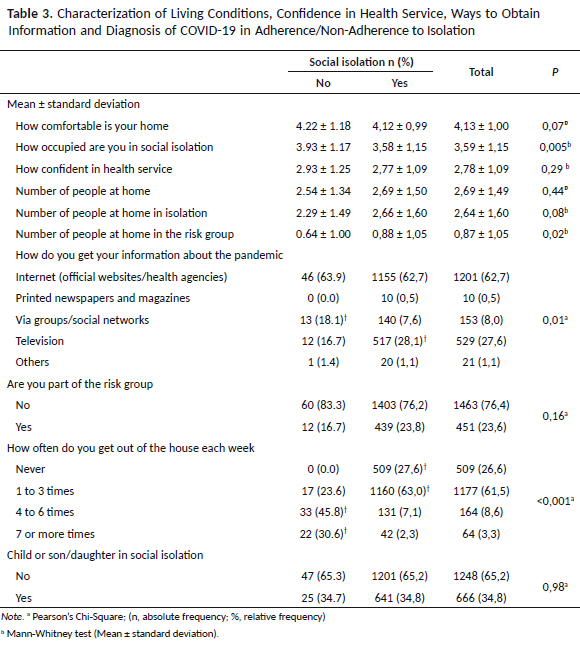
Although there were no significant differences, attention is drawn to the fact that the evaluation of home comforts, as well as the number of people at home or observing social isolation in the same house, number of children at home, belonging to a risk group or confidence in the health service, had no impact on whether or not social isolation was observed.
Table 4 exhibits the data related to the difference in the mean value of people who observe and do not observe social isolation, according to personality, wellbeing, meaning of life, stress mindset, and psychological distress by means of the Mann-Whitney technique (expressed through pa) and ANCOVA (expressed through pb) in which the effect of the sociodemographic covariables and sample characteristics that exerted an effect on the observance or nonobservance of social isolation was controlled. Accordingly, when considering just the difference in who does or does not observe social isolation, it can be seen that those individuals who do not follow social isolation show higher positive affect indices.
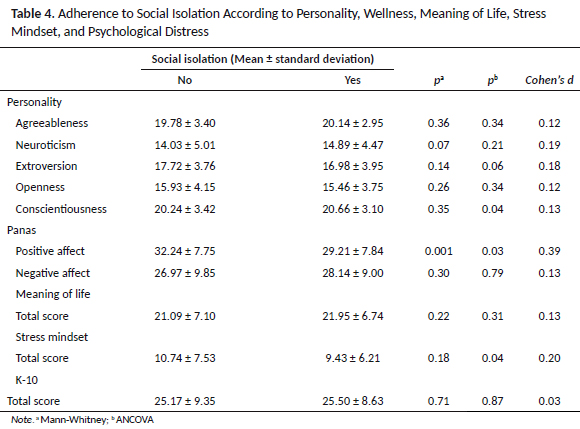
However, when controlling the effect of the covariables (described in Tables 2 and 3) that exhibit significant differences and considering only the effect of personality, wellbeing, meaning of life, stress mindset, and psychological distress on the behavior of those who do or do not observe social isolation, it can be seen that people who observe greater social isolation have higher indices of conscientiousness. On the other hand, people who do not observe social isolation have higher positive affect and stress mindset indices (i.e., they tend to see a stressful situation in a more positive way). In all the analyses, the effect size was between small and average, which indicates that the sample size had a minimal effect (see Table 4).
Discussion
The challenges imposed by the pandemic caused by the Coronavirus have led to health authorities recommending measures to combat the virus. Although measures like quarantine, physical isolation, and good hygiene have had an effect on reducing contagion (Prem et al., 2020), studies have suggested that sociodemographic characteristics (Garg et al., 2020) and psychological characteristics (Carvalho, Pianowski, & Gonçalves, 2020) may contribute to the level of people's commitment to these actions. Given these observations, the primary aim of the present study was to evaluate those sociodemographic and psychological characteristics that might influence observance of social isolation, as well as the effects of this measure on the levels of psychological distress in the Brazilian population.
As far as the sociodemographic aspects are concerned, the observed results corroborate the hypotheses of the influence of these aspects on maintaining social isolation, given the existence of a less socially privileged group of participants, in other words, those with a poorer educational background, monthly income less than one minimum salary and of black ethnicity, who are less observant of this pandemic containment measure. These results reveal the social gulf that exists in the Brazilian population, also observed in other cultures such as in North America. As indicated by the CDC (CDC, 2020b), people from ethnic minorities are more likely to live in more heavily populated areas with a larger number of people living under one roof and, therefore, they find it more difficult to practice measures of social isolation. In this regard, studies have also indicated that the exclusionary capitalist model is highlighted by the present pandemic, which is exposing the vulnerability of specific social groups beyond the realms of global interconnectedness (Nunes, 2020).
In the case of Brazil, these characteristics are even more alarming. The people with the lowest levels of education and lowest salaries are the ones performing the essential services (cleaners, cab or public transport drivers, etc.) or informal work (Instituto Brasileiro de Geografia e Estatística [IBGE], 2016, 2021) who, as they rely on their own devices to support their families, have to expose themselves to situations of social contact.
On the subject of ethnic minorities, the CDC (2020b) warns of the effects of institutional racism which, over the years, has led to these groups being denied access to health-related services, contributing to the establishment of chronic illnesses associated with higher mortality when the individual is infected with Covid-19. In this regard, the findings reported in this study are consistent with the reality of life in Brazil.
Another very important aspect is the way people go about obtaining information on the pandemic, where those who look for information in groups or on social networks are less adherent to the observance of social isolation. Problems of this kind are being discussed in the present scientific context (Lima, Lopes, & Brito, 2020) such as the challenge of providing quick, reliable information to the public in order to reduce contagion and control the pandemic. These efforts are being conducted by different social agents such as scientific journals that have started to allow open access to studies that address aspects of Covid-19. However, a percentage of the general public has acquired information through channels such as Facebook, Twitter, WhatsApp, YouTube and Instagram. The biggest problem in this case is to dissociate false information from that which is reliable. These people are often exposed to fake news such as promises of cures or drugs or actions that will render the individual less susceptible to infection from the virus, causing them to be less concerned about physical exposure.
From a psychological point of view, it was found that people who do not observe social isolation have higher indices of positive affect and stress mindset. This means that those who have a more positive view of a stressful situation (stress mindset) and/or report more situations of pleasure of the positive affect kind, with a hedonistic attitude (Reppold, Zanini, Campos, Faria, & Tocchetto, 2019), are less observant of social isolation. This finding is in line with the discussions related to the big five factor model of personality which indicates that lower indices of conscientiousness are related to reduced social commitment (Carvalho et al., 2020). In fact, this piece of information is connected with the previous finding related to the item in the questionnaire about isolation in which individuals who observed social isolation, for the most part, indicated they did so to protect others and not for egotistical motives or simple obedience with the rules. In this way, the importance of the individual characteristic of connectivity and social commitment may be discussed as a strong factor for adherence to social isolation as opposed to the liberalistic and egotistical view that would likely lead to indifference towards others (Nunes, 2020).
In short, the present article presented data that provide evidence of the high rate of adherence to social isolation at the beginning of the pandemic in Brazil (equivalent to the first month), especially among people with higher levels of education, higher incomes and who receive their information on the pandemic by television. On the other hand, people who do not observe social isolation have lower incomes, lower levels of education, get their information from social media and present with higher positive affect and stress mindset indices, as well as lower indices of conscientiousness. As a whole, these data demonstrate the influence of characteristics of personality (more specifically, conscientiousness), form of perception of the stressful event, level of personal gratification (positive affect) and social aspects, on adherence to restrictive social interaction measures and infection control. Future studies should evaluate the effect of the time spent living with the pandemic and social isolation on levels of adherence and people's health.
References
Ahorsu, D. K., Lin, C.-Y. Imani, D., Saffari, M., Griffiths, M. D., & Pakpour, A. H. (2020). The Fear of COVID-19 Scale: Development and initial validation. International Journal of Mental Health and Addiction, 1-9. doi: 10.1007/s11469-020-00270-8 [ Links ]
Andrews, G., & Slade, T. (2001). Interpreting scores on the Kessler Psychological Distress Scale (k10). Australian and New Zealand Journal of Public Health, 25(6), 494-497. doi: 10.1111/j.1467-842X.2001.tb00310.x [ Links ]
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet, 395(10227), 912-920. doi: 10.1016/S0140-6736(20)30460-8 [ Links ]
Carvalho, L. F., Pianowski, G., & Gonçalves A. P. (2020). Personality differences and the COVID-19: Are extroversion and conscientiousness personality traits associated with engagement in containment measures? Trends Psychiatry Psychotherapy, 42(2), 179-184. doi: 10.1590/2237-6089-2020-0029 [ Links ]
Centers for Disease Control and Prevention. (2020a, April 31). COVID-19 in Racial and Ethnic Minority Groups. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/racial-ethnic-minorities.html [ Links ]
Centers for Disease Control and Prevention. (2020b, April 10). Social distancing, quarantine, and isolation: Keep your distance to slow the spread. Retrieved from http://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/social-distancing.html [ Links ]
Crum, A. J., Salovey, P., & Achor, S. (2013). Rethinking stress: The role of mindsets in determining the stress response. Journal of Personality and Social Psychology, 104(4), 716-33. doi:10.1037/a0031201 [ Links ]
Diener, E. (2000). Subjective well-being: The science of happiness and a proposal for a national index. American Psychologist, 55(1), 34-43. doi: 10.1037/0003-066X.55.1.34 [ Links ]
Diener, E., Emmons, R., Larsen, R., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49(1), 91-95. doi: 10.1207/s15327752jpa4901_13 [ Links ]
Field, A. (2020). Descobrindo a estatística usando o SPSS (5th. ed.). Porto Alegre: Penso. [ Links ]
Garg, S., Kim, L., Whitaker, M., O'Halloran, A, Cummings, C., Holstein, R., ... Fry, A. (2020). Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019 - COVID-NET, 14 States, March 1-30, 2020. Morbidity and Mortality Weekly Report – MWR, 69(15), 458-464. doi: 10.15585/mmwr.mm6915e3 [ Links ]
Hauck Filho, N., Machado, W. L., Teixeira, M. A. P., & Bandeira, D. R. (2012). Evidências de validade de marcadores reduzidos para a avaliação da personalidade no modelo dos cinco grandes fatores. Psicologia: Teoria e Pesquisa, 28(4), 417-423. doi: 10.1590/S0102-37722012000400007 [ Links ]
Hutz, C. S., Nunes, C. H., Silveira, A. D., Serra, J., Anton, M., & Wieczorek, L. S. (1998). O desenvolvimento de marcadores para a avaliação da personalidade no modelo dos cinco grandes fatores. Psicologia: Reflexão e Crítica, 11(2), 395-411. doi: 10.1590/S0102-79721998000200015 [ Links ]
Hutz, C. S., Zanon, C., & Bardagi, M. (2014). Satisfação de Vida. In C. S. Hutz (Ed.), Avaliação em Psicologia Positiva (pp. 43-48). Porto Alegre: Artmed. [ Links ]
Instituto Brasileiro de Geografia e Estatística. (2016). Mobilidade sócio-ocupacional 2014. Retrieved from https://biblioteca.ibge.gov.br/index.php/biblioteca-catalogo?view=detalhes&id=298815 [ Links ]
Instituto Brasileiro de Geografia e Estatística. (2021). Trabalho e rendimento: economia informal urbana. Retrieved from https://ces.ibge.gov.br/apresentacao/portarias/200-comite-de-estatisticas-sociais/base-de-dados/1150-economia-informal-urbana.html [ Links ]
Lei n. 13.979, de 6 de fevereiro de 2020.(2020, 6 de fevereiro). Dispõe sobre as medidas para enfrentamento da emergência de saúde pública de importância internacional decorrente do coronavírus responsável pelo surto de 2019. Diário Oficial da União, seção 1. Retrieved from http://www.in.gov.br/en/web/dou/-/lei-n-13.979-de-6-de-fevereiro-de-2020-242078735 [ Links ]
Lima, D. L., Lopes, M. A. A A. M., & Brito, A. M. (2020). Social media: friend or foe in the COVID-19 pandemic?. Clinics, 75, e1953. doi: 10.6061/clinics/2020/e1953 [ Links ]
MacDonald, P. L., & Gardner, R. C. (2000). Type I error rate comparisons of post hoc procedures for I j Chi-Square tables. Educational and Psychological Measurement, 60(5), 735-754. doi: 10.1177%2F00131640021970871 [ Links ]
Maia, B. R., & Dias, P. C. (2020). Ansiedade, depressão e estresse em estudantes universitários: o impacto da COVID-19. Estudos de Psicologia (Campinas), 37, e200067. doi: 10.1590/1982-0275202037e200067 [ Links ]
Ministério da Saúde (2021, September 14). Brasil: #pátria vacinada. Retrieved from https://coronavirus.saude.gov.br/sobre-a-doenca#o-que-e-covid [ Links ]
Moreira, R. S. (2020). COVID-19: unidades de terapia intensiva, ventiladores mecânicos e perfis latentes de mortalidade associados à letalidade no Brasil. Cadernos de Saúde Pública, 36(5). doi: 10.1590/0102-311X00080020 [ Links ]
Nunes, J. (2020). A pandemia de COVID-19: securitização, crise neoliberal e a vulnerabilização global. Cadernos de Saúde Pública, 36(4), e00063120. doi: 10.1590/0102-311X00063120 [ Links ]
Peixoto, E. M., Rocha, G. M. A., Franco, J. O., & Bueno, J. M. H. (2019). Avaliação da mentalidade sobre o estresse em amostra do Norte e Nordeste brasileiro. Estudos de Psicologia, 24(3), 328-339. doi: 10.22491/1678-4669.20190033 [ Links ]
Prem, K., Liu, Y., Russell, T. W., Kucharski, A. J., Eggo, R. M., Davies, N., ... Hellewell, J. (2020). The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. The Lancet Public Health, 5(5), e261-e270. doi: 10.1016/S2468-2667(20)30073-6 [ Links ]
Remuzzi, A., & Remuzzi, G. (2020). COVID-19 and Italy: What next? Lancet, 395, 1225-1228. doi: 10.1016/ S0140-6736(20)30627-9 [ Links ]
Reppold, C. T., Zanini, D. S., Campos, D. C., Faria, M. R. G. V., & Tocchetto, B. S. (2019). Felicidade como produto: um olhar crítico sobre a ciência da Psicologia Positiva. Avaliação Psicológica, 18(4), 333-342. doi: 10.15689/ap.2019.1804.18777.01 [ Links ]
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063-1070. doi: 10.1037/0022-3514.54.6.1063 [ Links ]
Werneck, G. L., & Carvalho, M. S. (2020). A pandemia de COVID-19 no Brasil: crônica de uma crise sanitária anunciada. Cadernos de Saúde Pública, 36(5). doi: 10.1590/0102-311X0006882 [ Links ]
Wolfe N. (2011). The viral storm: the dawn of a new pandemic age. New York: Times Books. [ Links ]
World Health Organization. (2020). Coronavirus disease 2019 (COVID-19) Situation Report – 78. Retrieved from https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200407-sitrep-78-covid-19.pdf [ Links ]
Zanon, C., Bardagi, M. P., Layous, K., & Hutz, C. S. (2014). Validation of the Satisfaction with Life Scale to Brazilians: Evidences of Measurement Noninvariance Across Brazil and US. Social Indicators Research, 119, 443-453. doi:10.1007/s11205-013-0478-5 [ Links ]
Zanon, C., & Hutz, C. S. (2014). Escala de Afetos Positivos e Negativos (PANAS). In C. S. Hutz (Ed.), Avaliação em Psicologia Positiva (pp. 63-67). Porto Alegre: Artmed. [ Links ]
 Endereço:
Endereço:
Rua 9 n769 ap 702 Setor Oeste
Goiania-Goiás
CEP 74.110-199
Telefone: (62) 99984-1664
Email: dazanini@yahoo.com
Received in 31.may.20
Revised in 28.jan.21
Accepted in 18.mar.21
Daniela Sacramento Zanini, Doutora em Psicologia Clínica e da Saúde pela Universidad de Barcelona (UB)/Espanha, Pós doutora pela Universidad de Barcelona (UB)/Espanha e pela Universidade do Porto (UP)/Portugal, é Professora da Pontifícia Universidade Católica de Goiás (PUC Goiás).
Evandro Morais Peixoto, Doutor em Psicologia como Profissão e Ciência pela Pontifícia Universidade Católica de Campinas (PUC – Campinas), com estágio doutoral desenvolvido na Université du Québec à Trois -Rivières UQTR/Canadá, Estágio pós doutoral em Psicologia pela Universidade São Francisco (USF), é Docente do Programa de Pós-Graduação Stricto Sensu em Psicologia da Universidade São Francisco (USF). Email: peixotoem@gmail.com
Josemberg Moura de Andrade, Doutor em Psicologia Social, do Trabalho e das Organizações pela Universidade de Brasília (UnB), é Professor Associado II do Departamento de Psicologia Social e do Trabalho (PST) do Instituto de Psicologia da Universidade de Brasília (UnB). Email: josemberg.andrade@gmail.com
Mônica Moreira Campos, Graduanda no curso de Psicologia na Pontifícia Universidade Católica de Goiás (PUC – GO). Email: monicammc9908@gmail.com
Jose Luis Pais Ribeiro, Doutor em Psicologia pela Universidade do Porto/Portugal, é Professor Associado da Faculdade de Psicologia e de Ciências da Educação da Universidade do Porto/Portugal e Investigador no William James Center for Research do Instituto Universitário Lisboa (ISPA). Email: jlpr@fpce.up.pt

