










Services on Demand
article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkEstudos de Psicologia (Natal)
Print version ISSN 1413-294XOn-line version ISSN 1678-4669
Estud. psicol. (Natal) vol.26 no.2 Natal apr./June 2021
http://dx.doi.org/10.22491/1678-4669.20210012
10.22491/1678-4669.20210012
PSYCHOBIOLOGY AND COGNITIVE PSYCHOLOGY
Psychological well-being and covid-19: Psychological impacts of quarantine on the brazilian population
Bem-estar psicológico e covid-19: impactos psicológicos da quarentena na população brasileira
Bienestar psicológico y covid-19: impactos psicológicos de la cuarentena en la población brasileña
Mariana MalvezziI; Flávia Feitosa SantanaI; Cléber da Costa FigueiredoI,II
IEscola Superior de Propaganda e Marketing/SP
IIFundação Getúlio Vargas
ABSTRACT
The Covid-19 pandemic had several impacts, both social and psychological ones. Based on Ryff's (1995) Psychological Well-Being (PWB) concept, this work considers health as a whole – not as the absence of disease, but as physical, mental, and social well-being, together with the ability to face challenges in six dimensions: self-acceptance; positive relationships with others; autonomy; environmental mastery; purpose in life; and personal growth. Our main objective was to assess PWB among the quarantined Brazilian population. A second aim was to verify differences in PWB in relation to the following demographics: gender, education, income, and age. A quantitative survey was conducted using Ryff's scale (1995) with a stratified sample proportional to the number of deaths in each region of Brazil as reported by the government on May 3, 2020. The data were collected between May 4 and 10, 2020. The lowest PWB score was found in the low-education, low-income group, whereas the highest PWB score was in found the elderly group.
Keywords: mental health; health promotion; human development; applied psychology.
RESUMO
A Covid-19 trouxe transformações e impactos sociais, entre eles, efeitos psicológicos. Considerando o conceito de Bem-estar Psicológico (BEP) de Ryff (1995), este trabalho apoiou-se em uma visão abrangente da saúde – não a ausência de enfermidade, mas o bem-estar físico, mental, social e capacidade de enfrentar desafios a partir de seis dimensões: autoaceitação; relações positivas com os demais; autonomia; domínio do ambiente; propósito de vida; crescimento pessoal. O objetivo geral é verificar o BEP da população brasileira em quarentena; o secundário, averiguar diferenças no BEP nos estratos: sexo, escolaridade, renda e idade. Fez-se uma pesquisa quantitativa com a escala de Ryff (1995) a partir de amostragem estratificada proporcional à quantidade de óbitos divulgada pelo Governo em 3 de maio de 2020. A coleta de dados ocorreu de 4 a 10 de maio do mesmo ano. Verificou-se menor BEP para baixa escolaridade e renda e maior BEP para idosos.
Palavras-chave: saúde mental; promoção à saúde; desenvolvimento humano; psicologia aplicada.
RESUMEN
La llegada del Covid-19 trajo cambios e impacto social, incluyendo sus efectos psicológicos. Considerando el concepto de RYFF de Bienestar Psicológico (BEP) (1995), este trabajo está respaldado por una visión integral de la salud incluyendo bienestar físico, mental, social y la capacidad de enfrentar desafíos en seis dimensiones: autoaceptación; relaciones positivas; autonomía; dominio del medioambiente; propósito de vida; crecimiento personal. El objetivo general fue verificar el BEP en la población brasileña durante la cuarentena. El objetivo secundario fue averiguar el promedio del BEP de los siguientes estratos sociales: sexo, educación, renta y edad. Una investigación cuantitativa fue hecha, utilizando la escala RYFF, fundamentada en una visualización estratificada proporcional al número de muertes reportadas por el gobierno en el 3 de mayo de 2020. La recolección de datos ocurrió entre el 4 y 10 de mayo. Se registró un BEP más bajo para la escolaridad y menor renta y un BEP más alto entre los ancianos.
Palabras claves: salud mental; promoción de la salud; desarrollo humano; psicología aplicada.
The Covid-19 pandemic, which started in December 2019, caused relevant transformation and social impact in the world, adding to already existing concerns about Psychological Well-Being (PWB). Such concerns include: potential psychological effects (Brooks et al., 2020; Mihashi et al., 2009) for populations with stress symptoms (DiGiovanni, Conley, Chiu, & Zaborski, 2004); emotional burnout (Marjanovic, Greenglass, & Coffey, 2007); fear (Caleo, et al., 2018; DiGiovanni et al., 2004; Pan, Chang, & Yu, 2005; Pellecchia, Crestani, Decroo, Van den Bergh, & Al-Kourdi, 2015); paresthesia (DiGiovanni et al., 2004; Pan et al., 2005); confusion (Braunack-Mayer, Tooher, Collins, Street, & Marshall, 2013; DiGiovanni et al., 2004; Lee, Chan, Chau, Kwok, & Kleinman, 2005; Pan et al., 2005); depression (Hawryluc et al., 2004); and anger (Caleo et al., 2018; DiGiovanni et al., 2004; Pan et al., 2005).
Quarantine, the isolation and restriction of movement for people who may have been exposed to a certain virus – the coronavirus in this case – and may contaminate others (Brooks et al., 2020), is a measure to prevent contagion adopted in most countries, including Brazil. During the quarantine period the Brazilian population was submitted to not only isolation, but to a daily overload of news about the spread of the disease and the number of deaths, not to mention the loss of family members and acquaintances.
The current need for a quarantine on a global basis was unprecedented, but there is a series of studies showing quarantine as a challenging experience, one that can dramatically affect PWB and even lead to suicide in extreme cases (Barbisch, Koenig, & Shih, 2015). These studies compare quarantined and unquarantined populations in the same location and give evidence of different impacts depending on demographics and social class.
Taylor et al. (2008) relate negative effects of the quarantine experience, especially among young people aged 16 to 24, people with lower educational levels, and women, mostly those with only one child. Some studies do not indicate an association of factors, such as marital status, age, education, parenthood, and living with other adults, to an aggravated psychological state (Hawryluck et al., 2004). Some works aimed to study the vulnerability of healthcare workers and people with a psychiatric history (Brooks et al., 2020). The stress factors are manifold: duration of the quarantine, fear of infection, fear of lacking sufficient resources, frustration, lack of information, financial difficulty (Brooks et al., 2020).
The fact is that the quarantine experience may become a worldwide challenge not only in economic, but in public health terms, with a potential effect on psychological health. Investigating its impacts on different populations may bring important information for healthcare, public administration, society at large, and professionals who need to be prepared to deal with quarantine consequences.
Brazil – the seventh country in the world with the highest inequality index (Programa das Nações Unidas para o Desenvolvimento [PNUD], 2019) – faced several economic crises in the last decade and is suffering from political instability and rivalry. The country's Human Development Index (HDI) has stagnated in recent years (PNUD, 2019). Well-being has worsened with consequences from the pandemic and isolation: loss of family members, friends and acquaintances; economic losses and unemployment; changes in working conditions; changes in social and family life, such as homeschooling, elderly care and cohabiting.
To understand these problems we chose the humanist, positive outlook of the PWB model (Ryff, 1995) with its six determinants: self-acceptance, positive relations with others, autonomy, environmental mastery, purpose in life, and personal growth.
The aim of this paper is to investigate the Brazilian population's PWB in the face of the pandemic and quarantine and to fulfill the following objectives: a) to investigate differences in PWB in distinct segments of the Brazilian population; b) to compare female and male PWB; c) to verify whether education is a determinant of PWB; d) to verify whether income is a determinant of PWB; e) to compare well-being of individuals in different age ranges: young (18 – 29); adult (30 – 64): and elderly (65 and over); f) to investigate whether the number of people living in the same household influences PWB; aspiring to contribute with the discussion required to face the pandemic.
The relevance of the present investigation is justified by possible consequences of the quarantine and the spread of Covid-19 among the Brazilian population's PWB. It is also justified by the country's current situation and social inequality, which has different impacts on different social classes. We also aim to contribute to research on quarantine experiences by generating data and information about populations in greater need of assistance.
Psychological well-being and its dimensions
Concepts and reflections on PWB demand a comprehensive understanding of health beyond the biophysical sphere. According to the World Health Organization (WHO), health is a state of "complete physical, mental and social well-being and not merely the absence of disease or infirmity." (WHO, 2020). Health transcends physical well-being and the absence of disease to include broad relationships between individuals and environments in a multiplicity of aspects (family and social life, living conditions, transportation). Seen as a broad subject, health is the product of an articulation between social structures and its functioning, as it derives from an organization of the environment, which raises problems but also offers resources. Health is an intervention on the environment, a social construction evidenced by the different activities involved in its production (Calveti, Muller, & Nunes, 2007; Maggi, 2006).
Health may be dealt with in several ways, which are generally organized in three distinct levels of intervention: primary, secondary, and tertiary prevention (Andrade, Morais, & Andrade, 2012; Martin, 1986). The first two levels are the target of public health; the third one is assigned to curative medicine.
Primary prevention refers to activities aimed to prevent disease – procedures and actions in the social environment intended to control the determinants of diseases and suffering. Such actions are of a sanitary and educational nature (Andrade et al., 2012; Martin, 1986). WHO defines them as "actions aimed at avoiding the manifestation of a certain disease, reducing the risk of new cases" (WHO, 2020).
Secondary prevention aims to deter a pathological process as soon as possible. Preventive activities aim to quickly detect physical and psychological deficiencies not avoided in primary prevention to apply an early-stage treatment (Andrade et al., 2012; Martin, 1986). WHO defines secondary prevention as "actions aimed at diminishing the prevalence of a disease among a population, reducing its progression and duration" (WHO, 2020).
Tertiary prevention seeks to prevent relapses and to reduce complications or sequelae through adequate treatment (Andrade et al., 2012; Martin, 1986). Tertiary prevention involves "actions aimed at reducing the prevalence of chronic disabilities in a population, minimizing functional disabilities as a consequence of disease" (WHO, 2020). Although the three types of prevention are distinct, they do not constitute alternative or antagonistic actions, but aspects of the same process encompassing individual, collective, social, environmental, psychological, and medical issues. This can currently be seen in the search for coordinated actions to combat Covid-19 in the primary, secondary, and tertiary prevention spheres. Social isolation as well as measures to reinforce hygiene and individual protection is part of primary prevention. Secondary prevention reinforces aspects such as early detection of symptoms, care and treatment of the disease. In tertiary prevention curative measures are applied to those with moderate or severe symptoms.
The importance of conceiving health in its historical-social dimension is evident, as well the interdependence of actions aimed at improving it. Our research seeks to inform necessary actions in the Covid-19 pandemic scenario through an assessment of PWB and its importance for health as one of its comprising elements.
This reflection leads to understanding health promotion as every action aimed at improving life quality and society organization, which are conditioning factors for the relationship between individuals and the environment, determinants of pleasure or suffering. Promoting health is thus an activity that should take into consideration a population, its environment, and its history. Those who promote health are the ones entitled to it, for health is gained through the struggle to conquest it (Calveti et al., 2007). Therefore, health requires the population and its government's awareness of the risks present in the social environment, and participation of all in managing individual and collective health (Coelho, 2002; Martin, 1986).
In relation to the concept of health, the psychological meaning of PWB is a vast, multidisciplinary theme encompassing four areas: physical, functional, emotional, and social, involving clinical, social and organizational psychology, as well as developmental and health psychology.
As a recent concept, PWB is understood as a positive dimension of health, despite being already present in the Illuminist ideals. Its theoretical cornerstone are studies from the 1950s and 1960s. From these sets of investigations, the concept of well-being connected to a set of resources (welfare) began to be seen in a global sense, involving subjective aspects. In the following decades the concept and its applications were further developed. In the 1970s the concept acquired a biopsychosocial bias; the 1980s brought a view of PWB as something distinct from subjective well-being (SWB) (Galinha & Ribeiro, 2005; Woyciekoski, Stenert, & Hutz, 2012). Since then, the concepts of PWB and SWB have been largely developed, but there is still no consensus.
The definition of PWB, which is the subject of this research, was introduced by Diener in 1984, being further developed after that. As a theoretical research area, PWB appeared as a criticism of the SWB perspective, which neglected the positive functioning of individuals and did not include in its formulation the ability to face challenges posed by life (Siqueira & Padovam, 2008).
PWB may be understood in three aspects: satisfaction with life, high level of positive affection, and low level of negative affection, considering a series of elements that include levels of emotional responses and judgement of satisfaction with one's life (Machado & Bandeira, 2012). It is based on the eudaemonic perspective, according to which reaching one's life potential should prevail in relation to self-realization, purpose in life, and overcoming challenges (Fave, Brda, Freire, & et al., 2011; Ryff & Keyes, 1995; Santana & Godim, 2016).
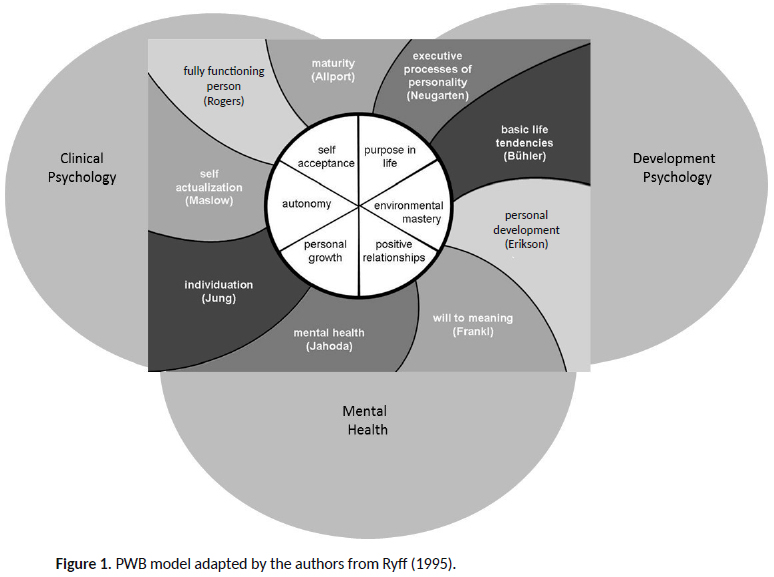
In the 1980s Ryff presented a PWB model based on positive psychology, erected upon several humanistic theories of psychology. Ryff (1995) developed her PWB model drawing from studies in developmental psychology, clinical psychology and mental health to propose its factors, which include: self-acceptance, positive relations with others, autonomy, environmental mastery, purpose in life, and personal growth (Figure 1).
The dimensions comprising PWB may be described as: (a) Self-acceptance: "positive attitude toward self, acknowledges and accepts multiple aspects of self, including good and bad qualities; feels positive about past life" (p. 101); (b) Positive relations with others: "warm, satisfying, trusting relationships with others; is concerned about the welfare of others; is capable of strong empathy, affection, and intimacy" (p. 101); (c) Autonomy: "is able to resist social pressures to think and act in certain ways; regulates behavior from within; evaluates self by personal standards" (p. 101); (d) Purpose in life: "has goals in life and a sense of directedness". The individual "feels there is a connection between the current present and past life; holds beliefs that give life purpose; has aims and objectives for living" (p. 101); (e) Environmental mastery: "has a sense of mastery and competence in managing the environment; controls complex array of external activities; makes effective use of surrounding opportunities" (p. 101); (f) Personal growth: "has feeling of continued development; sees self as growing and expanding; has sense of realizing his or her potential; sees improvement in self and behavior over time" (p. 101).
Studies carried out to validate the PWB model indicated variations that should be considered in future applications. Comparative studies on age differences showed that environmental mastery and autonomy tend to increase with age, whereas purpose in life and personal growth decrease with maturity. Studies on the differences between males and females demonstrated that women evaluate themselves as better in positive relationships with others and personal growth. In terms of cultural differences, model validation studies show differences between Western and Eastern countries (Ryff, 1995). There are several studies referring PWB; their results and validity can be applied to diverse contexts, such as: 1) age (Pereira, Lopes, Gonçalves, & Vasconcelos-Raposo, 2017; Queroz & Neri, 2005; Vijai, 2004); 2) religion (Barnes & Meyer, 2012; Kathleen & Elliott, 2009; Ryff, Singer, & Palmersheim, 2004); 3) gender (Cleary, Zaborski, & Ayanian, 2004; Kertzner, Meyer, Frost, & Stirratt, 2009; Li, Kao & Wu, 2015); 4) nationality (Gloria, Castellanos, & Orozco, 2005; Moradi & Risco, 2006); and 5) social class (Marmot & Furher, 2004; Miner-Rubino,Winter, & Stewart, 2004).
Based on the aforementioned, our investigation intends to verify the following assumptions: 1) women's perceived PWB is lower than men's; this condition may be aggravated with the number of persons living in the same household; 2) young and elderly people, as well as groups at higher risk for Covid-19 complications, show lower perceived PWB than adults at no risk for complications; 3) lower levels of income and education produce lower perceived PWB.
Method
Data collection was carried out between May 4 and 10, 2020. Facebook Ads Manager was used with a set of rules regarding race, education, income, and Brazilian state of residence in order to reach a respondent profile that was closer to the actual demographic structure of the Brazilian population. Using this tool to reach the diversified Brazilian population may be justified by the difficulty to access people offline and by the emergency character of the survey to reach the target audience – around 45 days after the start of the quarantine and with a rising number of deaths in the country –. Via stratified random sampling, Ads Manager was efficient in providing a representative sample of respondents about the psychological effects on well-being. The number of respondents from each Brazilian macroregion is proportional to the number of deaths officially reported by the Federal Government on May 3 (the Sunday before the survey started). Facebook Ads Manager allowed to capture the media effect of death, pain and fear provoked by the pandemic, which had already killed 85 people (1 percent) in the Mid-West; 963 people (14 percent) in the North; 1,918 in the Northeast; 210 people (3 percent) in the South and 3,849 (55 percent) in the Southeast, in a total of 7,025 deaths.
At first, we sought to illustrate the weight of deaths by Brazilian macroregion and, in each Brazilian macroregion, the impact of informing the quantity of deaths by state. According to classical sampling theory (Cochran, 1977), proportionate stratified random sampling is proportional to the population size of the entire population of strata and seeks to describe the population in small groups (Bolfarine & Bussab, 2005).
By the end of the survey, 1,732 answers were obtained. To ensure proportionality in each stratum, a simple random sampling was conducted in the dataset for each state by Brazilian geographic macroregion. For the North and Northeast, we used all the collected data due to the difficulty in getting responses from those regions. The final sample comprised 400 valid responses (3% from MW; 14% from N, 24% from NE, 5% from S, and 54% from SE).
PWB was measured using the six factors' model developed by Ryff et al. (2010) and Ryff e Keyes (1995) with the dimensions: autonomy, environmental mastery, personal growth, positive relations with others, purpose in life, and self-acceptance. The 18-item scale was used despite its lower internal consistency even in English (Seifert, 2021), because data collection via internet, as well the sample size and diversity of Brazilian population required a simpler scale with fewer items. Although there is a validated PWB scale in Portuguese (Machado, Bandeira, & Pawlowscki, 2013), this scale was applied to university students only, and does not warrant goodness-of-fit for the sample in the current investigation.
Based on the assumption that validity is superior than internal reliability of the scale (Costa, 2011), we decided to use content validity. Therefore, the items were translated to Portuguese and the content validation was undertaken by three specialists after a pretest. The items order and the seven-point Likert scale were kept according to the original tool. To formulate each dimension, reverse order items were transcribed to direct order. Each dimension was obtained through the arithmetic mean of its items.
Due to a lack of normality in the measures obtained, we used nonparametric tests to identify PWB nuances between: gender (female = 69%; male = 31%); age (young, 18 to 29 = 18 %; adult, 30 to 64 = 73%; elderly, over 65 = 9%); educational level (graduate = 64%; lower educational level = 36%); income (EÂ (up to R$ 2,090.00) = 21%; D (R$ 2,090.00 to R$ 3,135.00) = 12%; C (R$ 3,135.00 to R$ 10,450.00) = 39%; B (R$ 10,450.00 to R$ 20,900) = 19; A (above R$ 20,900.00) = 10%); and the number of persons living with the respondent in the same household. The variables race (self-reported: White = 56%; Multiracial = 31%; Black = 7.5%; Asian = 3.25%; Indigenous = 0.25%; and no self-classification = 2%) and religion (Catholic = 40%; Not religious = 27%; Protestant = 13%; Spiritism = 10%; African Diasporic Religion = 3%; Other = 7%) were used as baseline and helped characterize the sample and define the representativeness of these population features in the sample.
In order to compare PWB differences for variables with more than two categories we used the Kruskal-Wallis test (Conover, 1999), in which the null hypothesis postulates that there is no psychological effect related to the different categories of a variable. For dimensions where this null hypothesis was rejected, multiple comparisons were run through the Wilcoxon-Mann-Whitney test (Conover, 1999).
Results
Data analysis was carried out using R language in the integrated development environment RStudio Cloud. Statistically significant differences between some of the variables under consideration were revealed. These results may be better understood in the analysis of each variable, as follows.
Age
The preliminary descriptive analysis did not show differences in the dimension perceived personal growth between the three age ranges. Environmental mastery and self-acceptance seemed to be best perceived by the elderly (Figure 2). The Kruskal-Wallis test yielded no evidence of differences between the medians of the personal growth (p = 0.50) and purpose in life (p = 0.17) dimensions for the three age groups.
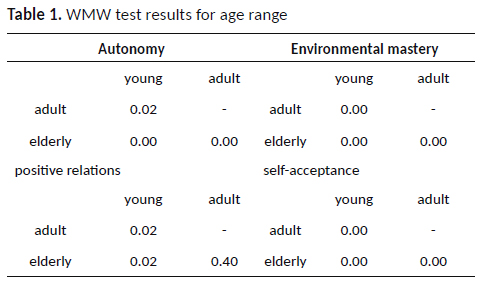
However, statistically significant differences appeared between the dimensions: autonomy (p < 0.01), environmental mastery (p < 0.01), positive relations with others (p = 0.01), and self-acceptance (p < 0.01). Pairwise comparisons were undertaken for these dimensions across the three age groups using the Wilcoxon-Mann-Whitney (WMW) test to detect specific statistically significant differences between them.
The only statistically non-significant median comparison (Table 1) was obtained in the positive relations with others dimension between adults and elderly (p = 0.40). In the remaining dimensions there were a growing statistically significant difference between the age groups – from young to elderly – demonstrating higher autonomy, environmental mastery, and self-acceptance in the elderly group (Figure 2).
Income
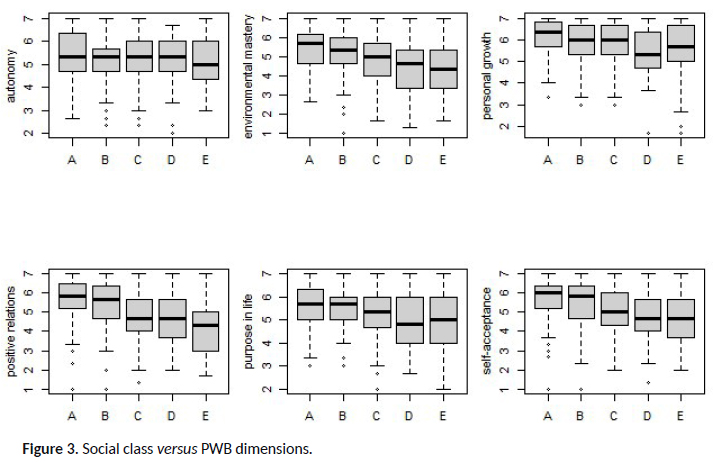
A descriptive analysis of the income variable (Figure 3) shows there was no graphic difference in the autonomy dimension between the different income levels. Regarding personal growth, some income brackets did not seem descriptively distinct. The wealthier social groups seemed to have higher environmental mastery, positive relations with others, purpose in life, and self-acceptance. In order to confirm the descriptive analysis based on graphic visualization, the same above-mentioned tests were run.
As a matter of fact, the results showed that there was no statistically significant difference in the autonomy dimension between the different income levels (p = 0.77). In the other dimensions, at least one income range differed from the others (p-values < 0.05). Pairwise comparisons between the classes yielded no evidence of statistical differences in environmental mastery among individuals from classes A and B, and among individuals from classes D and E. However, the cluster of individuals from classes A and B showed higher environmental mastery as compared to individuals from classes D and E (Figure 3).
Test results showed that classes A, B and C comprise a cohesive group in relation to the personal growth dimension (Table 2). On the other hand, individuals from classes D and E did not differ in this dimension and showed lower personal growth than individuals from classes A, B and C.
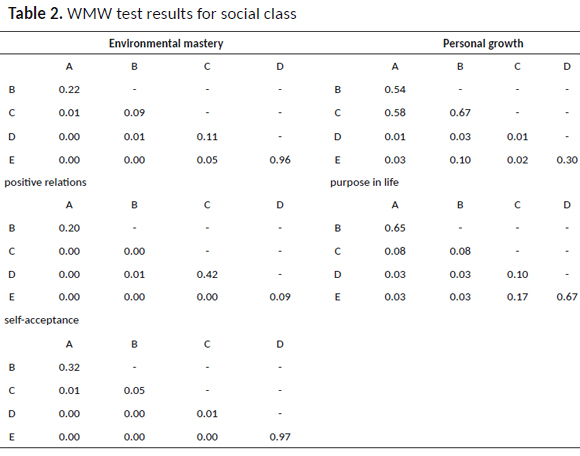
As for the dimensions: positive relations with others, purpose in life, and self-acceptance, no evidence was found to affirm that individuals from classes A and B differed. Nevertheless, there were differences between the other classes, except for class C, which was not different to class D in purpose in life and self-acceptance. No evidence was found to affirm that individuals from classes D and E differed in any of the dimensions under study.
Education
Except for the autonomy dimension (p = 0.68), all the other dimensions showed statistically significant differences (p-values < 0.05) in relation to the educational level: individuals with no college education showed lower environmental mastery, personal growth, positive relations with others, purpose in life, and self-acceptance.
Gender
The analysis of the psychological dimensions by gender applied two filters in order to evaluate the assumption that women had lower perceived PWB than men – a condition that could have worsened due to the number of persons living in the same household –. The first filter was sexual orientation. Only individuals who declared themselves heterosexual were analyzed, since different gender identities could bring to the analysis other sources of variations that were not in the scope of this study. The second filter eliminated individuals who lived with six or more persons in the same household, once there was a lower percentage of male respondents in these conditions; a scenario that prevented comparison of potential worsening of PWB for both genders.
After applying the filters, 343 respondents remained. The tests showed no evidence of statistical differences between genders in the dimensions: autonomy (p = 0.30), personal growth (p = 0.61), positive relations with others (p = 0.24), purpose in life (p = 0.78), and self-acceptance (p = 0.85). The only statistically significant difference appeared in environmental mastery (p = 0.01): women had a lower median (p < 0.05) in this comparison only.
In terms of the number of people living in the same household (excluding the respondent), the test yielded no evidence to affirm that there were significant differences in PWB related to the number of persons living with the respondent (p-values > 0.05 for all dimensions). Therefore, the assumption that PWB worsens as the number of individuals living under the same roof increases was not statistically sustained.
Results discussion
Our data analysis evaluated Brazilians' PWB during the Covid-19 quarantine, thus contributing to investigations on the psychological effects of social isolation among distinct social and demographic strata. In terms of gender, we could not confirm that women have lower perceived PWB than men. Thus, our research does not corroborate results by Taylor et al (2008), but it does support Hawryluck et al. (2004), which shows that the experience of quarantine does not affect men and women differently. Likewise, no difference in PWB was verified according to the number of individuals living in the same household.
However, differences were found in relation to income, age, and education. The analysis of results from the income perspective demonstrates lower PWB levels in the personal growth dimension for individuals in classes D and E; among classes A, B and C, this dimension showed no statistically significant difference. This fact seems to indicate that there is a minimum of access to products and services that may sustain activities linked to personal growth. Something similar has been seen in the environmental mastery dimension, with higher results among classes A and B. Income inequality and its health-related consequences are considerably referred to the literature (Marmot & Furher, 2004; Pickett & Wilkinson, 2015). It should be noted that class C is closer to classes A and B in the personal growth dimension. However, class C is closer to class D in purpose in life and self-acceptance (Pickett & Wilkinson, 2015).
The collected data evidenced higher PWB in environmental mastery, autonomy, and self-acceptance in the elderly population, which reinforces the extant literature reporting this population as "seeing themselves as well-adjusted, or as individuals with positive development, who possess high levels of socioemotional competencies" (Queroz & Neri, 2005, p. 6). By understanding maturity as the search for fulfilling one's potential, Ryff (1995) demonstrates the existence of high standards of social adequacy in the PWB construction. This aspect may help explain the subjective sense of PWB which, according to our collected data, seemed to grow from youth to maturity.
Regarding education, we verified that the higher the level of education (graduate or undergraduate), the higher the PWB in all dimensions, except autonomy, thus corroborating Taylor's (2008) findings that people with lower educational levels tend to suffer more negative effects from the quarantine experience.
Concluding remarks
This research fulfilled its aim to present an initial contribution for investigations on PWB and the psychological effects of the Covid-19 quarantine in Brazil, since there are not studies with a deeper understanding of Brazilians' PWB during the pandemic. These findings may guide new analyses and publications around the theme, for example, discussing PWB differences between genders according to social class, age or educational level. There is enough material to compare data from Brazil and from the state of São Paulo, the country's financial heart and initial epicenter of the Covid-19 outbreak.
Moreover, either the surveyed dataset may be useful for further comparisons inside the same population when the Covid-19 pandemic slows down; or may also be undertaken comparisons of our results to results from other countries.
This research has limitations, especially related to the use of the reduced 18-item scale with lower reliability in the six dimensions (even in its English version) when compared to other variants with more items. Therefore, it may be difficult to compare our results to other studies in the Brazilian context using a PWB scale with different numbers of items.
The study's contributions are the opportunity to draw a PWB profile for the Brazilian population during the pandemic, which could be used in future comparisons with local and international data still to be published. Our data also highlights that the country's evident social and economic inequality was reflected in the PWB results, especially concerning to income, stressing the need to support low-income populations. This is a complex aspect that reinforces understanding health in its plural nature, as well as a social construction, a product of individuals and their relationships in the political and social spheres.
References
Andrade, L. D. F., Morais, S. R. S., & Andrade, A. N. (2012). Profissionais da saúde em campo: revisão integrativa das práticas de educação em saúde na atenção pública primária, secundária e terciária. Revista de Educação do Vale do São Francisco - REVASF, 2(3). Retrieved from http://www.periodicos.univasf.edu.br/index.php/revasf/article/view/325
Barbisch, D., Koenig, K. L., & Shih, F. Y. (2015). Is there a case for quarantine? Perspectives from SARS to Ebola. Disaster Medicine and Public Health Preparedness, 9, 547-553. doi: 10.1017/dmp.2015.38 [ Links ]
Barnes, D. M., & Meyer, I. H. (2012). Religious affiliation, internalized homophobia, and mental health in lesbians, gay men, and bisexuals. American Journal of Orthopsychiatry, 82(4), 505-515. doi: 10.1111/j.1939-0025.2012.01185.x [ Links ]
Bolfarine, H., & Bussab, W. O. (2005). Elementos de amostragem. São Paulo: Edgar Blücher.
Braunack-Mayer, A., Tooher, R., Collins, J. E., Street, J. M., & Marshall, H. (2013). Understanding the school community's response to school closures during the H1N1 2009 influenza pandemic. BMC Public Health, 13, 344. doi: 10.1186/1471-2458-13-344 [ Links ]
Brooks, S. K., Webster, R. K., Smith, L. E., Woodalnd, L., Wessely, S., & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet, 395, 912-920. doi: 10.1016/S0140-6736(20)30460-8 [ Links ]
Caleo, G., Duncombe, J., Jephcott, F., Lokuge, K., Mills C., Looijen, E., ... Greig, J. (2018). The factors affecting household transmission dynamics and community compliance with Ebola control measures: A mixed-methods study in a rural village in Sierra Leone. BMC Public Health, 18, 248. doi: 10.1186/s12889-018-5158-6 [ Links ]
Calvetti, P. U., Muller, M. C., & Nunes, M. L. T. (2007). Psicologia da saúde e psicologia positiva: perspectivas e desafios. Psicologia: Ciência e Profissão, 27(4). doi: 10.1590/S1414-98932007000400011
Cleary, P., Zaborski, L., & Ayanian, J. (2004). Sex diferences in health over the course of midlife. In O. Brim, C. Ryff, & R. Kessler (Eds.), How healthy are we? A national study of well-being at midlife (pp. 37-63). Chicago: University of Chicago Press. [ Links ]
Cochran, W. G. (1977). Sampling techniques (3rd. ed.). Hoboken: John Wiley & Sons. [ Links ]
Coelho, M. (2002). Conceitos de saúde em discursos contemporâneos de referência científica. Revista História, Ciências, Saúde-Manguinhos, 9(2), 315-333. doi: 10.1590/S0104-59702002000200005
Conover, W. J. (1999). Pratical nonparametric statistics (3rd. ed.). Hoboken: John Wiley & Sons. [ Links ]
Costa, F. J. (2011). Mensuração e desenvolvimento de escalas: aplicações em administração. Rio de Janeiro: Ciência Moderna.
DiGiovanni, C., Conley, J., Chiu, D., & Zaborski, J. (2004).Factors influencing compliance with quarantine in Toronto during the 2003 SARS outbreak. Biosecur Bioterror, 2, 265-272. doi: 10.1089/bsp.2004.2.265 [ Links ]
Fave, A. D., Brdar, I., Freire, T., Vella-Brodrick, D., & Wissing, M. P. (2011). The eudaimonic and hedonic components of happiness: qualitative and quantitative findings. Social Indicators Research, 100(2), 185-207. doi: 10.1007/s11205-010-9632-5 [ Links ]
Galinha, I., & Ribeiro, J. (2005). História e evolução do conceito de bem-estar subjetivo. Psicologia, Saúde e Doenças, 6(2), 203-214. Retrieved from https://www.researchgate.net/publication/37650194_Historia_e_Evolucao_do_Conceito_de_Bem-Estar_Subjectivo
Gloria, A., Castellanos, J., & Orozco, V. (2005). Perceived educational barriers, cultural fit, coping responses, and psychological well-being of latina undergraduates. Hispanic Journal of Behavioral Sciences, 27(2), 161-183. doi: 10.1177/0739986305275097 [ Links ]
Hawryluck, L., Gold, W. L., Robinson, S., Pogorski, S., Galea, S., & Styra, R. (2004). SARS control and psychological effects of quarantine. Emerging Infectious Diseases, 10, 1206-1212. doi: 10.3201/eid1007.030703 [ Links ]
Kathleen, A., & Elliott, J. (2009). The role of religious activity and spirituality in the health and well-being of older adults. Journal of Health Psycology, 14(1), 43-52. doi: 10.1177/1359105308097944 [ Links ]
Kertzner, R., Meyer, I., Frost, D., & Stirratt, M. (2009). Social and psychological well being in lesbians, gay men, and bisexuals: The effects of race, gender, age, and sexual identity. Americam Journal of Orthopsychiatry, 79(4), 500-510. doi: 10.1037/a0016848 [ Links ]
Lee, S., Chan, L.Y., Chau, A. M., Kwok, K. P., & Kleinman, A. (2005). The experience of SARS-related stigma at Amoy Gardens. Social Science & Medicine, 61, 2038-2046. doi: 10.1016/j.socscimed.2005.04.010 [ Links ]
Li, R., Kao, C., & Wu, Y. (2015). Gender differences in psychological well-being: Tests of factorial invariance. Quality of Life Research, 24, 2577- 2581. doi: 10.1007/s11136-015-0999-2 [ Links ]
Machado, W., & Bandeira, D. (2012). Bem-estar psicológico: definição, avaliação e principais correlatos. Estudos de Psicologia, 29(4), 587-595. Retrieved from https://www.scielo.br/pdf/estpsi/v29n4/v29n4a13.pdf
Machado, W., Bandeira, D., & J. Pawlowski. (2013). Validação da Psychological Well-being Scale em uma amostra de estudantes universitários. Avaliação Psicológica, 12(2), 263-272. Retrieved from http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1677-04712013000200017
Maggi, B. (2006). Bem-estar. Laboreal, 2(1), 62-63. Retrieved from http://laboreal.up.pt/files/articles/2006_07/pt/62-63pt.pdf [ Links ]
Marjanovic, Z., Greenglass, E. R., & Coffey, S. (2007). The relevance of psychosocial variables and working conditions in predicting nurses' coping strategies during the SARS crisis: An online questionnaire survey. International Journal of Nursing Studies, 44, 991-998. doi: 10.1016/j.ijnurstu.2006.02.012 [ Links ]
Marmot, M., & Furher, R. (2004). Socioeconomic position and health across midlife. In O. Brim, C. Ryff, & R. Kessler (Eds.), How healthy are we? A national study of well-being at midlife (pp. 64-89). Chicago: University of Chicago Press [ Links ]
Martin, H. S. (1986). Manual de salud pública y medicina preventiva. Paris: Masson. [ Links ]
Mihashi, M., Otsubo, Y., Yinjuan, X., Nagatomi, K., Hoshiko, M., & Ishitake, T. (2009). Predictive factors of psychological disorder development during recovery following SARS outbreak. Health Psychology, 28(1), 91-100. doi: 10.1037/a0013674 [ Links ]
Miner-Rubino, K., Winter, D., & Stewart, A. (2004). Gender, social class, and the subjective experience of aging: Self-perceived personality change from early adulthood to late midlife. Personality and Social Psychology Bulletin, 30(12), 1599-1610. doi: 10.1177/0146167204271178 [ Links ]
Moradi, B., & Risco, C. (2006). Perceived discrimination experiences and mental health of Latina/o american persons. Journal of Counseling Psychology, 53(4), 411-421. doi: 10.1037/0022-0167.53.4.411 [ Links ]
Pan, P. J. D., Chang, S. H, & Yu, Y. Y. (2005). A support group for homequarantined college students exposed to SARS: Learning from practice. The Journal for Specialists in Group Work, 30, 363-374. doi: 10.1080/01933920500186951 [ Links ]
Pellecchia, U., Crestani, R., Decroo, T., Van den Bergh, R., & Al-Kourdi, Y. (2015). Social consequences of Ebola containment measures in Liberia. PLOS ONE, 10(12). doi: 10.1371/jornal.pone.0143036 [ Links ]
Pereira, H. P., Lopes, D. G., Gonçalves, M. C., & Vasconcelos-Raposo, J. J. (2017). Bem-estar psicológico e autoestima em estudantes universitários. Revista Iberoamericana de Psicología del Ejercicio y el Deporte, 12(2), 297-305. Retrieved from https://www.redalyc.org/pdf/3111/311151242013.pdf
Pickett, K., & Wilkinson, R. (2015). Income inequality and health: A causal review. Social Science and Medicine Journal, 128, 316-326. doi: 10.1016/j.socscimed.2014.12.031 [ Links ]
Programa das Nações Unidas para o Desenvolvimento (2019). Relatório do Desenvolvimento Humano 2019. Além do rendimento, além das médias, além do presente: desigualdades no desenvolvimento humano no século XXI. New York, USA: Author. Retrieved from http://hdr.undp.org/sites/default/files/hdr_2019_pt.pdf [ Links ]
Queroz, N., & Neri, A. (2005). Bem-estar psicológico e inteligência emocional entre homens e mulheres na meia-idade e na velhice. Psicologia: Reflexão e Crítica, 18(2), 292-299. doi: 10.1590/S0102-79722005000200018
Ryff, C. (1995). Psychological well-being in adult life. Current Directions in Psychological Science, 4(4), 99-104. Retrieved from https://www.jstor.org/stable/20182342?origin=JSTOR-pdf&seq=1 [ Links ]
Ryff, C. D., Almeida, D. M., Ayanian, J. Z., Carr, D. S., Cleary, P, D., Coe, C., ... Williams, D. R. (2010). Midlife in the United States (MIDUS 2), 2004-2006. Inter-university Consortium for Political and Social Research [distributor]. doi: 10.3886/ICPSR04652.v8 [ Links ]
Ryff, C. D., & Keyes, C. L. (1995). The structure of psychological well-being revisited. Journal of Personality and Social Psychology, 69(4), 719-727. Retrieved from http://midus.wisc.edu/findings/pdfs/830.pdf [ Links ]
Ryff, C. D., Singer, B., & Palmersheim, K. (2004). Social inequalities in health and well-being: the role relational and religious protective factors. In O. Brim, C. D. Ryff, & R. Kessler (Eds.), How healthy are we? A national study of well-being at midlife (pp. 90-123). Chicago: University of Chicago Press. [ Links ]
Santana, V., & Godim, S. (2016). Regulação emocional, bem-estar psicológico e bem-estar subjetivo. Estudos de Psicologia (Natal), 21(1), 58-68. doi: 10.5935/1678-4669.20160007
Seifert. T. (2021). The Ryff scales of psychological well-being. Retrieved from https://centerofinquiry.org/uncategorized/ryff-scales-of-psychological-well-being/ [ Links ]
Siqueira, M., & Padovam, V. (2008). Bases teóricas de bem-estar subjetivo, bem-estar psicológico e bem-estar no trabalho. Psicologia: Teoria e Pesquisa, 24(2). doi: 10.1590/S0102-37722008000200010 [ Links ]
Taylor, M. R., Agho, K. E., Stevens, G. J., &Raphael, B. (2008). Factors influencing psychological distress during a disease epidemic: Data from Australia's first outbreak of equine influenza. BMC Public Health, 8: 347. doi: 10.1186/1471-2458-8-347 [ Links ]
Vijai, C. (2004). Estudo exploratório das relações entre avós e netos e o bem-estar psicológico na velhice (Master's thesis, Universidade de Lisboa). Retrieved from http://hdl.handle.net/10451/29727 [ Links ]
World Health Organization. (2020). Constitution. Geneva, SWI. Retrieved from https://www.who.int/about/governance/constitution [ Links ]
Woyciekoski, C., Stenert, F., & Hutz, S. (2012). Determinantes do bem-estar subjetivo. Revista Eletrônica PUC-RS, 43(3). Retrieved from http://revistaseletronicas.pucrs.br/ojs/index.php/revistapsico/article/view/8263 [ Links ]
 Endereço para correspondência:
Endereço para correspondência:
Rua Coronel Oscar Porto, 795, apt.101
CEP 04.003-004
São Paulo – SP
Email: mariana.malvezzi@hotmail.com
Received in 31.may.20
Revised in 23.mar.21
Accepted in 01.jun.21
Mariana Malvezzi, Doutora em Psicologia Social pela Pontifícia Universidade Católica de São Paulo (PUC-SP), é Professora Adjunta I da Escola Superior de Propaganda e Marketing de São Paulo (ESPM-SP).
Flávia Feitosa Santana, Doutora em Psicologia Social pela Universidade de São Paulo (USP), é Professora Adjunta da Escola Superior de Propaganda e Marketing de São Paulo (ESPM-SP). Email: flavia.feitosa@espm.br
Cléber da Costa Figueiredo, Doutor em Estatística pelo Instituto de Matemática e Estatística da Universidade de São Paulo (IME-USP), é Professor Adjunto II da Escola Superior de Propaganda e Marketing (ESPM-SP) e Professor Horista da Fundação Getúlio Vargas (FGV). Email: cleber.data.scientist@gmail.com


{kind=link}
{kind=link}
{kind=link}