










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkTemas em Psicologia
versão impressa ISSN 1413-389X
Temas psicol. vol.24 no.3 Ribeirão Preto set. 2016
http://dx.doi.org/10.9788/TP2016.3-13Pt
ARTIGOS
Analysis of recommendations from breastfeeding handbooks: possibilities and challenges
Veronica Aparecida PereiraI; Olga Maria Piazentin Rolim RodriguesII; Millena Lima DonatoIII; Fabiana Calixtro MaruchiIII; Priscilla Joyce Vieira do AmaralIII
IFaculdade de Ciências Humanas da Universidade Federal da Grande Dourados, Dourados, MS, Brazil
IIDepartamento de Psicologia da Universidade Estadual Paulista Júlio de Mesquita Filho, Bauru, SP, Brazil
IIIUniversidade Federal da Grande Dourados, Dourados, MS, Brazil
ABSTRACT
Despite the encouragement of the World Health Organization to ensure breastfeeding, there are contraindications that may make it temporarily or unfeasible. Considering the efforts of Brazilian public agencies to meet this goal, we sought to in this paper intends to (a) analyze official documents of the Ministry of Health and State Departments in Brazil, relevant information on natural and artificial feeding; (b) identify in what measure available documents present information to breastfeeding mothers and to mothers that provide artificial feeding. Eleven national manuals and eight state was selected, published from 2007 to 2013, from the online addresses of Health Departments at the national and State levels in Brazil. In all of there was a great emphasis on the benefits of exclusive breastfeeding until the sixth month of life. Other pieces of information refer to the criterion of complementary feeding, care for the mother provided by healthcare professionals, dissemination of pro breastfeeding programs, rights of the mothers and cultural and ethnic features. Information on artificial feeding is limited to report contraindications to it.
Keywords: Contraindications for breastfeeding, breastfeeding, artificial feeding.
Currently, the debate about the importance of breastfeeding is growing, from both a cultural (Almeida & Novak, 2004) and nutritional point of view (Corona & Conde, 2013). The World Health Organization (WHO) advises that the baby should be exclusively breastfed until six months of age. After this period, the introduction of food complementary to breastfeeding, whenever possible, is recommended and that this should be maintained until two years of age. This measure is mainly designed to reduce the high global rates of childhood malnutrition, to increase immunity and to decrease infant mortality (WHO, 2009). Almeida and Novak (2004) warned that biological factors need to be contextualized to the reality of the wifemother-nurturer and the relationship established with the baby, in order to favor the adaption to the maternal condition and interposed new requirements.
Santiago (2013) presented worrying data on the mean duration of breastfeeding in Brazil. According to a study conducted in 2008, the mean duration of exclusive breastfeeding in Brazil is only 54.11 days, and the prevalence of mothers who continue to breastfeed until four or six months is 23.3% and 9%, respectively. This was observed even after a long media campaign aiming to increase public awareness regarding the importance of breastfeeding. The comprehension of these rates, according to the author, may be associated with lack of preparation of the health network regarding guidance to mothers, health problems of the mother and maternity leave for a shorter period than is required by the baby.
In contrast, researchers indicate other concerns in countries with full adherence to exclusive breastfeeding, such as in India. Thakur, Holambe and Wadagale (2015), in a study conducted with a population of 197 Indian mothers, with a mean age of 24.17 years, found exclusive breastfeeding until the baby was five months of age. The concern was related to the 53.63% of mothers who had not introduced complementary foods to their infants after six months, as this is important for their development. In this case, the concern is related to the greater risk of malnutrition and vulnerability of babies due to lack of nutrients essential for their growth and unavailable from exclusive breastfeeding at this age.
The targets established by the WHO (2009), regarding the maintenance of exclusive breast-feeding up to six months of life of the baby, require actions, in the context of public policies, that not only guarantee breastfeeding but also meet the nutritional needs of the baby after this period.
With regard to the lack of preparation of health professionals, the WHO highlighted a lack of expertise to properly guide the puerpera faced with the difficulties at the initiation of breastfeeding. The professionals may not know how to help the mother to initiate and maintain exclusive breastfeeding, recommending early introduction of supplements or even, openly or covertly, promoting breast milk substitutes (WHO, 2009). Almeida and Novak (2004) state that this behavior leads to the importation of a culture of early weaning and strengthens myths about breastfeeding.
As a positive experience of the training of professionals given this demand, Davanzo, Pierpaolo and Travan (2014) described a study conducted in Italy. The authors stress the importance of the training of health professionals in guidance and management of issues related to the initiation of breastfeeding. For this, they established protocols for the registration of the mothers needs in the postpartum period and technical team practices that could favor the initiation and maintenance of breastfeeding. Among the concerns identified, the following stood out: essential care to the mother in the postpartum period, which should favor the contact between mother and baby through touch, 'skin to skin' contact; care and guidance during the period when the baby presents weight loss and the mother may be afraid of not providing sufficient milk; guidance when the mother needs to take medication that can have side effects for the baby, and advice regarding problems related to the health of the baby, such as malabsorption and allergies. For the issues presented, the technical team, in the hospitalization period of the mother, should be sufficiently prepared to advise her about possible periods of temporary interruption of the breastfeeding, provision of human milk from the milk bank or specialized formulas and the maintenance of production and expression of the breast milk to give to the baby in the future.
From the indications of Davanzo et al. (2014), it should be noted that guidance may be extended to the post-hospitalization period, indicating care programs for the mothers during early breastfeeding. Considering the time required for the milk let-down reflex, which in some cases can reach up to 72 hours (United Nations Children's Fund [UNICEF], 2008), it is common that many mothers leave the maternity unit without having actually initiated breastfeeding, facing alone a number of difficulties regarding hand expression, nipple shape, pain, and cracked nipples, among others.
Guidance for mothers is necessary since women often find themselves improperly prepared and informed about breastfeeding. Rahalkar, Phalke and Phalke (2014) report that the benefits of breastfeeding will depend on factors such as the initiation, duration and age at which weaning occurs, with it being important to understand that cultural and economic factors are directly linked to these practices. A study of 150 breastfeeding women in India, over a two month period, identified, through the application of a questionnaire, that the most adequate breastfeeding practices were related to higher levels of education of the mothers.
The strong emphasis on breastfeeding is based on numerous studies that consider it to be an ideal food mainly due to its nutritional benefits and immunity properties. The Brazilian Ministry of Health and the Pan American Health Organization (PAHO) reaffirmed the WHO recommendations regarding the importance of exclusive breastfeeding until the sixth month of life of the baby (Ministério da Saúde, 2002; PAHO, 2013). In addition to the biological and nutritional benefits, studies have highlighted the contribution to the overall healthy development of the baby (Cotrim, Venancio, & Escuder, 2002; PAHO, 2013). Studies have also highlighted its influence on the psychomotor, cognitive and affective development of the child (Araujo, Del Fiaco, Pimentel, & Schmitz, 2004; Bayardo, Peixoto, & Corrêa, 2003; Carrascoza, Costa, & Moraes, 2005; PAHO, 2013).
In addition to the above factors arising from breastfeeding, cultural factors are also present, which attribute to the mother the obligations of full dedication to motherhood. In this context, the inability to breastfeed may be interpreted by some women as if they were in social and biological debt to their child. In a certain way, the woman feels this pressure, even if implicitly, from professional and family members (Bispo, Bispo, & Pepe, 2010).
The effective impossibility of breastfeeding mainly arises due to high rates of infection presented by the mother, which would be transmitted through the breast milk. In this situation, the WHO established some measures to prevent the transmission of diseases such as, the indication of the substitution of breastfeeding for the use of appropriate formulas until the second year of life for children born to mothers with diseases such as AIDS, hepatitis B and other diseases that could lead to contamination through human milk (UNICEF, 2008). However, these formulas are not always accessible, due to their high cost. What is often perceived, is the incidence of improper artificial feeding, using milk that is unfit for consumption by infants. The use of improper milk is associated with malnutrition and high rates of allergies, illness and child mortality (Diaz, Patrício, & Fagundes-Neto, 2002; Santiago, 2013).
While not being an interruption of breast-feeding, the return to work of the mother is often associated with early weaning. According to Brasileiro, Ambrosano, Marba and Possobon (2012), the index of breastfeeding-working mothers providing exclusive breastfeeding is less than 10%. In Brazil, in 1988, legislation presented significant advances, guaranteeing women 120 days maternity leave (Senado Federal, 1988). In 2008, Federal Law No. 11.770 sought to encourage companies to grant six months maternity leave, a period that would meet the first requirement of the WHO. Added to this initiative it was suggested that companies provide childcare vouchers to breastfeeding mothers, with thirty-minute breastfeeding breaks during the work shift. However, the conditions of access to crèches are usually insufficient for effective maintenance of breastfeeding after six months. In the sample investigated by Brasileiro et al. (2012), the majority of the mothers performed the weaning prior to four months, preparing themselves to return to work.
Although the change in Brazilian law does not fully meet the requirements of the WHO, the initial measures point to decreased illness and infant mortality, which were high in the 1980s. According to Batista and Silva (2007), the Ministry of Health initiatives based on the defense of breastfeeding were responsible for creating the National Program to Encourage Breastfeeding, valorizing and disseminating this practice for the Brazilian culture (PAHO, 2013).
Knowing the importance of breastfeeding and the impossibility for some mothers to perform this practice, it is possible that mothers who are unable to breastfeed may feel guilty due to not being able to feed their child and provide the necessary conditions for normal development. Pregnant women and puerperae who can not breastfeed, have stated that this restriction causes guilt, frustration, suffering, interrupted wishes, impotence and broken dreams (Paiva & Galvão, 2004). The interruption of breastfeeding can cause various psychological repercussions for the mother, with it being necessary to promote conscientization of the behaviors present during breastfeeding that are favorable for the structuring of the mother-infant bond, regardless of the form of breastfeeding. In this task, the practice of the health professionals is of utmost importance, uncovering and addressing myths and fears of the mother about this interruption.
Seeking to indicate subsidies for mothers unable to breast-feeding, this study aimed to: (a) perform an analysis of information available in handbooks on breastfeeding for babies, published in Brazil from 2007 to 2014, in order to identify information on milk quality, quantity, hygiene conditions, position of the baby and psychological benefits of natural and artificial breastfeeding, and (b) compare the results and indicate information important for mothers unable to breastfeed.
Method
To carry out the literature review breast-feeding handbooks available on the websites of the National and State Health Departments of Brazil, from 2007 to 2014, were selected.
Eleven national and eight state handbooks were selected. The selection criterion for the national handbooks was the time period. In the state departments, it was realized that the majority referred to the national handbooks. Therefore, those that indicated their own handbooks on the breastfeeding theme (booklet or handbook), within the study period, were selected. In the state of Paraná a handbook of the city of Curitiba was selected due to the fact that this was recommended by the state health department.
Data analysis was organized in two ways. Initially categories of analysis were pre-established for the content related to breastfeeding and artificial feeding, these being: (a) quality of milk; (b) quantity to be provided to the baby; (c) hygiene conditions; (d) frequency; (e) position of the baby; (f) introduction of food supplements and, (g) psychological benefits. The categories were quantified and described in relation to their content. In the second analysis, it was sought to identify the main contents provided by the handbooks that extrapolated the categories studied. In both analyzes quantitative and qualitative descriptions were performed.
Results and Discussion
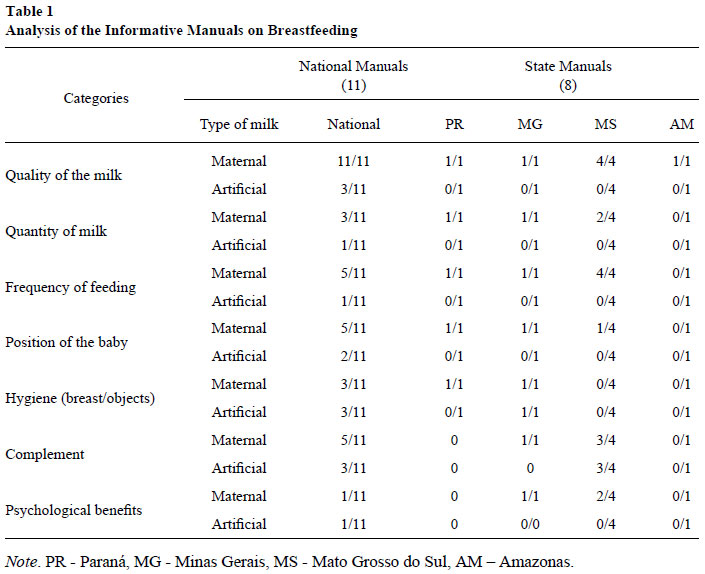
After reading the national and regional handbooks, the occurrence of the categories previously selected in this study was quantified. As presented in Table 1, the first category of analysis relates to the quality of the milk. All the national handbooks emphasized the quality of breast milk regarding its nutritional properties, its reduction of the risk of illness and its adequacy for the needs of the baby (Ministério da Saúde, 2007, 2009, 2010a, 2010b, 2010c, 2011a, 2011b, 2012a, 2012b, 2013a, 2013b; UNICEF, 2008). Although the UNICEF Handbook (2008) is international, it was disseminated through a national portal, therefore was considered for the analysis. Regarding artificial milk, some handbooks highlighted formulas, when breastfeeding is contraindicated for the baby (Ministério da Saúde, 2009, 2010c, 2013b). The quality of the formulas in the handbooks was shown to be inferior to breast milk with regards to immunity and availability, the latter also being highlighted in the state handbooks (Secretaria Estadual de Saúde de Minas Gerais, 2012; Secretaria Estadual de Saúde do Mato Grosso do Sul, 2007a, 2007b, 2007c, 2007d). There was also a warning about the use of improper campaigns by commercial establishments, which could encourage the use of formulas independent of the condition of the mother and baby (Ministério da Saúde, 2013b).
Regarding the quantity of milk provided to the baby, it was observed that a minority (7/18) of national handbooks addressed this category in relation to breast milk. Indications of the amount were not precise, requiring the mother to have the ability to recognize when her child is hungry. The UNICEF handbook (2008) describes the condition of the newborn which will initially have its sleep cycle interrupted by hunger. The mother, in turn, should pay attention that the sleep interval does not exceed three hours in the first month of life. This handbook states that the time for a baby to empty one breast is four minutes, which changes due to the time it actually sucks the milk and the time it uses the breast as a 'pacifier'. There is the indication that the breast feeding regime should be on free demand, with flexible hours, meeting the needs of the baby (Ministério da Saúde, 2009; UNICEF, 2008). This may result in multiple daily feedings, requiring the mother to be rested and completely free for this act. The free demand regime is endorsed by 50% of the state handbooks (Secretaria Estadual de Saúde do Mato Grosso do Sul, 2007a, 2007b; Secretaria Estadual de Saúde de Minas Gerais, 2012; Secretaria Municipal da Saúde de Curitiba - PR, 2011). Regarding the quantity to be provided in an artificial feeding regime, the topic was hardly discussed, only appearing in one of the national handbooks (Ministério da Saúde, 2013b). This statement appears in the part that deals with restrictions on breastfeeding. In other handbooks, such as that of UNICEF (2008), questions relating to the temporary restriction of breastfeeding are dealt with more, for which the provision of pasteurized human milk by trans-lactation is recommended. This "consists of a receptacle containing milk (preferably pasteurized human milk) placed between the breasts of the mother with a tube fixed next to the nipple" (Ministério da Saúde, 2009, p. 38). Another indication points to the use of formulas provided using a cup or spoon, maintaining the stimulation of the production of breast milk through hand expressing (UNICEF, 2008). When the restriction is definitive, the use of formulas is recommended, however, without indication of specific amounts.
The frequency of the breastfeeding was addressed by the majority of the handbooks, especially highlighting the provision on free demand, respecting the rhythm and needs of each baby (Ministério da Saúde, 2009, 2010a; Secretaria Estadual de Saúde de Minas Gerais, 2012; Secretaria Estadual de Saúde do Mato Grosso do Sul, 2007a, 2007b, 2007c, 2007d). The frequency of artificial feeding was addressed by only one national handbook (Ministério da Saúde, 2013b).
The position of the baby was addressed in the national and regional handbooks. When this appeared, during breastfeeding, it was found to be associated with explanations about the formation of the breast, latching-on of the baby, ventilation and breathing positions. Other comments pointed to the need to observe the behavior of the baby during breastfeeding in order to ensure good suction (Ministério da Saúde, 2009, 2010a, 2012a). The position of the baby in the artificial feeding was hardly cited and, when this occurred, was associated with the interests of good swallowing and prevention of choking, reflux and infections of the ear canal (Ministério da Saúde, 2009; UNICEF, 2008). In both situations the subjective aspects of this contact, such as the possibility of non-verbal communication between mother and baby, eye contact, touch and attention that are needed, were not addressed. The position of the baby with regard to the safety criteria was also addressed in the state and municipal handbooks evaluated (Secretaria Estadual de Saúde do Mato Grosso do Sul, 2007b; Secretaria Municipal da Saúde de Curitiba, 2011). This last statement refers to the fact that indigenous women can be seated during feeding, which eliminates the effort of preparing the formula. Therefore, it deals more with the position of the mother than that of the baby itself. The emphasis is on freedom of the indigenous woman in breastfeeding under any circumstances, since the milk is always ready and in the ideal conditions for the baby.
Hygiene practices were more fully explained in the handbook of the Ministry of Health (Ministério da Saúde, 2012a). The other national handbooks addressed the topic when discussing care of the breasts, especially during the activities of hand expression and milk storage for pasteurization. Hygiene practices related to the care and supply of formula or pasteurized breast milk mainly referred to the sterilization of glasses, utensils and bottles (Ministério da Saúde, 2009, 2010a; UNICEF, 2008). Among the state handbooks, this category was addressed in the handbooks of Minas Gerais and Paraná (Secretaria Estadual de Saúde de Minas Gerais, 2012; Secretaria Municipal da Saúde de Curitiba, 2011).
In the handbooks of Mato Grosso do Sul state, the use of bottles is identified as a major cause of infection, diarrhea and even infant mortality, however, specific information about the hygiene of the bottles is not described (Secretaria Estadual de Saúde do Mato Grosso do Sul, 2007a, 2007b, 2007c).
Complementary feeding was partially addressed in the national handbooks and the state handbooks of Minas Gerais and Mato Grosso do Sul. The statements related to breast milk indicated the introduction of complementary foods after six months of exclusive breastfeeding as an important measure for the nutrition and health of the child (Ministério da Saúde, 2009, 2010a, 2010b; Secretaria Estadual de Saúde de Minas Gerais, 2012; Secretaria Estadual de Saúde do Mato Grosso do Sul, 2007a, 2007b, 2007c), corroborating the study of Thakur et al. (2015) and the guidelines of the PAHO (2013). In the handbooks of indigenous groups (Secretaria Estadual de Saúde do Mato Grosso do Sul, 2007a, 2007b, 2007c), the type of complementary food was carefully described, related to the products available in the village, valorizing products produced there and free from preservatives and pesticides. Artificial feeding was primarily cited as an alternative due to breastfeeding contraindications (Ministério da Saúde, 2010a, 2010c, 2013b).
Regarding the psychological benefits of breastfeeding or artificial feeding, it was found that this was the item least discussed in the national handbooks (Ministério da Saúde, 2009; UNICEF, 2008). The behaviors performed in the act of feeding the baby, in the way in which they are presented, are more related to survival and nutrition, without considering the aspects of the very strong bonding between mother and child that takes place during this activity. Among the state handbooks, in the indigenous health handbooks, the notes of the Kaiwá people highlighted the provision of breast milk as an act that is also able to convey love and affection (Secretaria Estadual de Saúde do Mato Grosso do Sul, 2007a). In the handbook of the Terenas people, as well as covering nutritional issues, immunity and emphasizing healthy complementary feeding with natural products, also present in other handbooks (2007a, 2007c), breastfeeding is described as capable of promoting the "affective bond between mother and child" (2007b, p. 14). The picture following the statement does not show the provision of the breast but other food being given to an older child, suggesting that this bond goes beyond the condition of breastfeeding. The handbook of the state of Minas Gerais points out that babies who are breastfed, in addition to health benefits as a whole, present "better emotional, social, motor and intelligence development"(Secretaria Estadual de Saúde de Minas Gerais, 2012, p. 5).
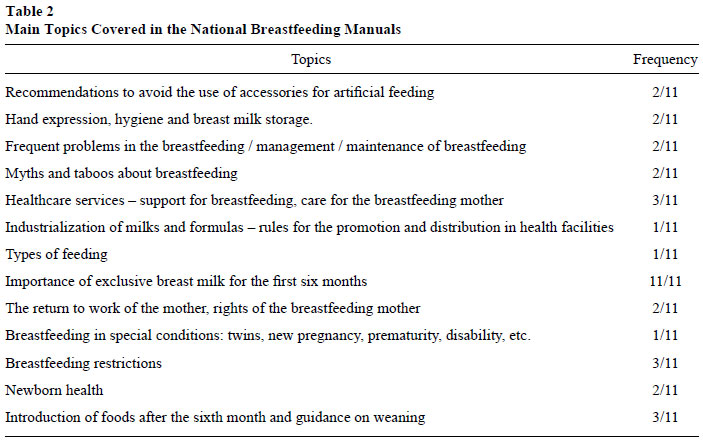
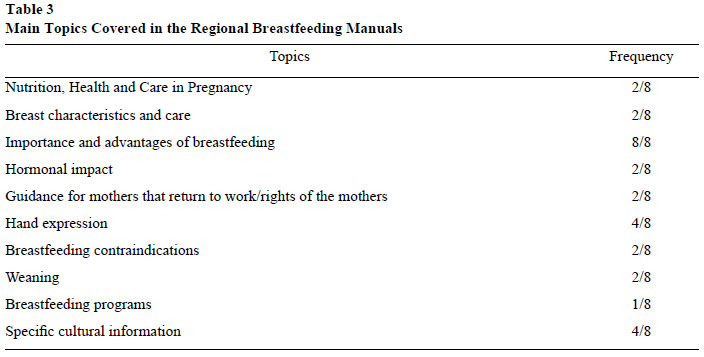
In the second analysis, other aspects were highlighted as relevant in the breastfeeding handbooks. The result of this analysis, with structuring of the categories after reading the handbooks, is divided into two parts: Table 2, analysis of the national handbooks and Table 3 analysis of the regional handbooks.
Among the topics highlighted in Table 2, the strong emphasis on the importance of exclusive breastfeeding up to six months can be identified, in agreement with the PAHO (2013) and WHO (2009) recommendations. Three of them refer to the importance of guiding mothers on the initial weaning process, by also introducing foods that are important for the health and nutrition of the baby, given that after six months the exclusive maintenance of breastfeeding would be insufficient (PAHO, 2013; Thakur et al., 2015) and also difficult due to mothers returning to work. Also present were contraindications to breastfeeding and support services for breastfeeding mothers, mainly from milk banks, stressing the importance of training the technical staff to monitor the breastfeeding mother (Davanzo et al., 2014; Santiago, 2013). Some approached the rights of the mother returning to work and the other topics indicated the care necessary for the maintenance of the breastfeeding.
In addition to the guidance outlined in the national handbooks, especially regarding the importance of exclusive breastfeeding, the state handbooks highlight some specific conditions regarding the prenatal period, health of the mother (breast care, hand expression, hormonal impact), return to work and contraindications for breast-feeding (Table 3). The link of the State Health Department of Amazonas directs to the State Health Plan, in which the Brazil Breastfeeding Program was presented as a priority in primary healthcare, related to the strategies to promote maternal and child health (Secretaria Estadual de Saúde do Amazonas, 2012). The specific cultural information refer to the care in disclosing information about breastfeeding respecting the indigenous culture with regard to the Kaiwá, Terena and Kadweu populations (Secretaria Estadual de Saúde do Mato Grosso do Sul, 2007a, 2007b, 2007c) as well as the culture of deaf people, making the information accessible through Brazilian Sign Language (Secretaria Estadual de Saúde do Mato Grosso do Sul, 2007d).
Final Considerations
The analysis of selected handbooks highlighted a variety of information related to the importance of exclusive breastfeeding until the sixth month of life of the baby and recommendations for complementary feeding up to two years of age, in agreement with the PAHO and WHO (PAHO, 2013; WHO, 2009) recommendations.
However, in cases of contraindications for breastfeeding, temporary or permanent, the information to mothers who have to resort to artificial feeding seems insufficient. Knowing that the human milk bank reserves would be insufficient to meet the demand for mothers unable to breastfeed, precise and safe information about using formulas and programs in the public network that can offer alternative milk is essential. In addition, it is necessary to minimize possible feelings of guilt and failure of the mothers who do not breastfeed, guiding them about behaviors that are possible in the artificial feeding and how these will favor the mother-infant bond. A more detailed description of these behaviors, such as touch, eye contact, affection and responsiveness should be present in all handbooks dealing with breastfeeding.
Caressing, kissing, touching and looking at the baby in order to maintain contact and demonstrate the affection of the mother toward her child are why breastfeeding is considered an important milestone for the formation of the mother-infant bond and for the maintenance of an affective and healthy interaction between the dyad. When this occurs successfully, breastfeeding may be considered to be a facilitator of the maternal function of bonding with the newborn, meeting the basic needs of the baby and enabling the development of this ability to relate to other objects of affection (Locatelli & Costa, 2008).
The mothers that provide artificial milk also need to know how to do this, as caress, touch, eye contact and the demonstration of affection are not connected to the maternal breast. To care for the newborn in a responsive way, even when it is necessary to use an instrument for its feeding (bottle, cup or spoon), may be effective if this behaviors bring the baby closer to the caregiver.
It is hoped that the findings of this study can highlight information of great relevance for breastfeeding and encourage proposals for breastfeeding campaigns that also consider the reality of the mothers who can not breastfeed.
References
Almeida, J. A. G., & Novak, F. R. (2004). Amamentação: Um híbrido natureza-cultura. Jornal de Pediatria, 80(5),119-125. doi:10.2223/JPED.1242 [ Links ]
Araujo, M. F. M., Del Fiaco, A., Pimentel, L. S., & Schmitz, B. A. S. (2004). Custo e economia da prática do aleitamento materno para a família. Revista Brasileira de Saúde Materno Infantil, 4(2),135-141. doi:10.1590/S151938292004000200003 [ Links ]
Batista, B. C., & Silva, L. R. (2007). Sentimentos de mulheres soropositivas para HIV diante da impossibilidade de amamentar. Escola Anna Nery Revista de Enfermagem, 11(2),268-275. doi:10.1590/s1414-81452007000200013 [ Links ]
Bayardo, R. A., Peixoto, L. F. S., & Corrêa, M. S. N. P. (2003). Aleitamento natural e artificial: Considerações gerais [Resumo]. JBC Jornal Brasileiro de Clínica Odontológica Integrada, 7(39),257-290. [ Links ]
Bispo, T. M. S., Bispo, R. G., & Pepe, A. L. (2010). Os aspectos psicológicos da interdição à amamentação. Psicologia. PT, O portal dos Psicólogos. Recuperado em http://www.psicologia.pt/artigos/textos/TL0163.pdf [ Links ]
Brasileiro, A. A., Ambrosano, G. M. B., Marba, S. T. M., & Possobon, R. F. (2012). A amamentação entre filhos de mulheres trabalhadoras. Revista de Saúde Pública, 46(4),642-648. doi:10.1590/S0034-89102012000400008 [ Links ]
Carrascoza, K. C., Costa, A. L., Jr., & Moraes, A. B. A. (2005). Fatores que influenciam o desmame precoce e a extensão do aleitamento materno. Estudos de Psicologia (Campinas), 22(4),433-440. doi:10.1590/S0103-166X2005000400011 [ Links ]
Corona, L. P., & Conde, W. L. (2013). O efeito do aleitamento materno na composição corporal de menores de três anos em São Paulo, Brasil. Journal of Human Growth and Development, 23(3),276-281. [ Links ]
Cotrim, L. C., Venancio, S. I., & Escuder, M. M. L. (2002). Uso de chupeta e amamentação em crianças menores de quatro meses no estado de São Paulo. Revista Brasileira de Saúde Materno Infantil, 2(3),245-252. doi:10.1590/S151938292002000300005 [ Links ]
Davanzo, R., Pierpaolo, B., & Travan, L. (2014). Integrating health care practices with the promotion of breastfeeding. Journal of Pediatric and Neonatal Individualized Medicine, 3(2),1-5. [ Links ]
Diaz, N. J., Patricio, F. S., & Fagundes-Neto, U. (2002). Colite alérgica: Características clínicas e morfológicas da mucosa retal em lactentes com enterorragia. Arquivos de Gastroenterologia, 39(4),260-267. doi:10.1590/S0004-28032002000400010 [ Links ]
Fundo das Nações Unidas para a Infância. (2008). Manual de aleitamento materno. Recuperado em https://www.unicef.pt/docs/manual_aleitamento.pdf [ Links ]
Locatelli, B. M. E. S., & Costa, P. J. (2008). O processo de amamentação e suas implicações para a mãe e seu bebê. Mental, 10(6),85-102. [ Links ]
Ministério da Saúde. (2002). Guia alimentar para crianças menores de 2 anos. Brasília, DF: Autor. Recuperado em http://bvsms.saude.gov.br/bvs/publicacoes/10_passos.pdf [ Links ]
Ministério da Saúde. (2007). Promovendo o aleitamento materno. Brasília, DF: Autor. Recuperado em http://www.redeblh.fiocruz.br/media/albam.pdf [ Links ]
Ministério da Saúde. (2009). Saúde da criança: Nutrição infantil, aleitamento materno e alimentação complementar. Cadernos de Atenção Básica, 23. Recuperado em http://bvsms.saude.gov.br/bvs/publicacoes/saude_crianca_nutricao_aleitamento_alimentacao.pdf [ Links ]
Ministério da Saúde. (2010a). Dez passos para uma alimentação saudável. Guia alimentar para crianças menores de dois anos. Brasília, DF: Autor. Recuperado em http://bvsms.saude.gov.br/bvs/publicacoes/10_passos.pdf [ Links ]
Ministério da Saúde. (2010b). Cartilha para a mãe trabalhadora que amamenta. Brasília, DF: Autor. Recuperado em http://bvsms.saude.gov.br/bvs/publicacoes/cartilha_mae_trabalhadora_amamenta.pdf [ Links ]
Ministério da Saúde. (2010c). Amamentação e uso de medicamentos e outras substâncias: Série A. Normas e Manuais Técnicos (2. ed.). Brasília, DF: Autor. Recuperado em http://bvsms.saude.gov.br/bvs/publicacoes/amamentacao_uso_medicamentos_2ed.pdf [ Links ]
Ministério da Saúde. (2011a). Além da sobrevivência: Práticas integradas de atenção ao parto, benéficas para a nutrição e a saúde de mães e crianças. Brasília, DF: Autor. Recuperado em http://bvsms.saude.gov.br/bvs/publicacoes/alem_sobrevivencia_atencao_parto.pdf [ Links ]
Ministério da Saúde. (2011b). Rede amamenta Brasil, os primeiros passos (2007-2010). Série I. História da Saúde. Brasília, DF: Autor. Recuperado em http://www.ibfan.org.br/legislacao/pdf/doc-750.pdf [ Links ]
Ministério da Saúde. (2012a). Saúde da criança: Crescimento e desenvolvimento. Brasília, DF: Autor. Recuperado em http://bvsms.saude.gov.br/bvs/publicacoes/saude_crianca_crescimento_desenvolvimento.pdf [ Links ]
Ministério da Saúde. (2012b). Aleitamento materno, distribuição de leite e fórmulas infantis em estabelecimentos de saúde e a legislação. Brasília, DF: Autor. Recuperado em http://bvsms.saude.gov.br/bvs/publicacoes/aleitamento_materno_distribuicao_leite.pdf [ Links ]
Ministério da Saúde. (2013a). Atenção à saúde do recém-nascido: Guia para os profissionais de saúde. Intervenções comuns, icterícia e infecções. Brasília, DF: Autor. Recuperado em http://bvsms.saude.gov.br/bvs/publicacoes/atencao_saude_recem_nascido_profissionais_v3.pdf [ Links ]
Ministério da Saúde. (2013b). PNAN: Política Nacional de Alimentação e Nutrição. Brasília, DF: Autor. Recuperado em http://bvsms.saude.gov.br/bvs/publicacoes/politica_nacional_alimentacao_nutricao.pdf [ Links ]
Organização Pan-Americana de Saúde. (2013). La OPS/OMS llama a apoyar a las madres que amamantan para asegurar la lactancia exclusiva hasta los 6 meses. Recuperado em http://www.paho.org/hq/index.php?option=com_content&view=article&id=8914%3Apahowho-urges-support-for-nursing-mothers-to-ensure-exclusive-breastfeeding-up-to-six-months-&catid=740%3Anews-press-releases&Itemid=1926&lang=es&Itemid=1926 [ Links ]
Paiva, S. S., & Galvão, M. T. G. (2004). Sentimentos diante da não amamentação de gestantes e puérperas soropositivas para HIV. Texto Contexto Enfermagem, 13(3),414-419. doi:10.1590/S0104-07072004000300011 [ Links ]
Rahalkar, A., Phalke, D. B., & Phalke, V. D. (2014). A study of breastfeeding and complementary feeding practices with emphasis on misconceptions amongst the women with under two year children in rural area. International Journal of Medical Research & Health Sciences, 3(4),851-855. doi:10.5958/2319-5886.2014.00013.7 [ Links ]
Santiago, L. B. (2013). Manual de aleitamento materno. Barueri, SP: Manole. [ Links ]
Secretaria Estadual de Saúde de Minas Gerais. (2012). Cartilha da gestante. Mães de Minas: A vida merece esse cuidado. Recuperado em http://www.saude.mg.gov.br/images/documentos/Cartilha%20da%20gestante.pdf [ Links ]
Secretaria Estadual de Saúde do Amazonas. (2012). Plano estadual de saúde: PES- 2012-2015. Recuperado em http://www.saude.am.gov.br/docs/pes/pes_2012-2015.pdf [ Links ]
Secretaria Estadual de Saúde do Mato Grosso do Sul, Fundação Nacional de Saúde, Departamento de Saúde Indígena. (2007a). Cartilha aleitamento materno:Alimento da mãe para o filho. Etnia: Guarani/Kaiowá. Campo Grande, MS: Secretaria Estadual de Saúde do Mato Grosso do Sul. [ Links ]
Secretaria Estadual de Saúde do Mato Grosso do Sul, Fundação Nacional de Saúde, Departamento de Saúde Indígena. (2007b). Cartilha aleitamento materno e introdução de novos alimentos: Sua importância. Etnia: Terena. Campo Grande, MS: Secretaria Estadual de Saúde do Mato Grosso do Sul. [ Links ]
Secretaria Estadual de Saúde do Mato Grosso do Sul, Fundação Nacional de Saúde, Departamento de Saúde Indígena. (2007c). Cartilha aleitamento materno e introdução de novos alimentos: Sua importância. Etnia: Kadiweu. Campo Grande, MS: Secretaria Estadual de Saúde do Mato Grosso do Sul. [ Links ]
Secretaria Estadual de Saúde do Mato Grosso do Sul. (2007d). Amamentação em Libras. Campo Grande, MS: Autor. [ Links ]
Secretaria Municipal da Saúde de Curitiba - PR. (2011). Alimentação infantil: Cartilha de orientação aos pais (2. ed.). Recuperado em http://www.crn8.org.br/uploads/arquivo/b517902a83b8b7acd6cf009cb1779dc0.pdf [ Links ]
Senado Federal. (1988). Constituição da República Federativa do Brasil. Brasília, DF: Autor. Recuperado em http://www.planalto.gov.br/ccivil_03/constituicao/constituicaocompilado.htm [ Links ]
Thakur, N. A., Holambe, V. M., & Wadagale, A. V. (2015). Survival analysis of duration of exclusive breast feeding using life table and hazard function. JKIMSU, 4(1),88-94. [ Links ]
World Health Organization. (2009). Infant and young child feeding: Model chapter for textbooks for medical students and allied health professionals. Retrieved from http://www.who.int/maternal_child_adolescent/documents/9789241597494/en/ [ Links ]
 Mailing address:
Mailing address:
Veronica Aparecida Pereira
Rua Portugal, 445
Dourados, MS, Brazil 79826-370
Phone: (67) 2310-2310
E-mail: veronica.ufgd.tci@gmail.com, olgarolim@uol.com.br, mi_donatto@hotmail.com, fabimaruchi@hotmail.com and pri-joyce@hotmail.com
Recebido: 05/02/2015
1ª revisão: 24/08/2015
Aceite final: 02/09/2015


{kind=link}
{kind=link}
{kind=link}