










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkTemas em Psicologia
Print version ISSN 1413-389X
Temas psicol. vol.26 no.4 Ribeirão Preto Oct./Dec. 2018
http://dx.doi.org/10.9788/TP2018.4-01Pt
ARTICLE
"Skin-to-skin" contact in pain prevention in preterm infants: systematic review of literature
Camila Regina LottoI; Maria Beatriz Martins LinharesII
IOrcid.org/0000-0003-3914-2439. Universidade de São Paulo, São Paulo, SP, Brazil
IIOrcid.org/0000-0001-5958-9874. Universidade de São Paulo, São Paulo, SP, Brazil
ABSTRACT
The present study is a systematic review of the literature that aimed to analyze the national and international scientific production on the effectiveness of skin-to-skin contact included in the Kangaroo Method for preventive pain management in preterm infants. The literature review was performed in the PubMed, LILACS, SciELO and PsycINFO databases covering the period between 2010 and 2017, using the descriptors kangaroo mother care method, skin-to-skin, pain and infant/newborn. The search returned 12 articles, which constituted the corpus of the review. The results demonstrated the effectiveness of skin-to-skin contact as an acute pain relief technique in preterm infants. The time staying in the Kangaroo position that was more effective for pain relief was 30 minutes prior to the routine painful procedure in the Neonatal Intensive Care Unit. In addition, the most effective way to assess pain was through the systematic observation of behavioral and physiological indicators, highlighting the importance of the use of validated and sensitive psychometric instruments for pain in preterm infants. It was also emphasized that skin-to-skin contact can provide other benefits, such as promoting and strengthening the mother-baby attachment and encouraging breastfeeding.
Keywords: Kangaroo mother care method, skin-to-skin, pain, premature.
Infants born preterm (<37 weeks of gestation age [GA]) can be: extremely preterm (<28 weeks), very preterm (28 to 32 weeks of GA), moderate preterm (32 to 33 weeks of GA) and late preterm (34 to 36 weeks of GA; Cassiano, Gaspardo, & Linhares, 2016; Chabra, 2013; World Health Organization [WHO], 2016). It is estimated that 15 million preterm infants are born annually worldwide, this equating to more than one in 10 neonates, with prematurity being a leading contributor to death in children under five years of age (WHO, 2016). According to data from the Health System (Sistema Único de Saúde - SUS), in 2015, the rate of preterm births in Brazil was 10.83%, in a total of 3,017,668 live births (Ministério da Saúde, 2015).
The Neonatal Intensive Care Unit (NICU) provides protection for the survival of preterm neonates, however, this setting also exposes them to various medical procedures, including painful and stressful stimuli (Klein, Gaspardo, & Linhares, 2006). Infants admitted to an NICU over three months underwent 3,283 invasive procedures, the most frequent being calcaneal puncture for blood collection, endotracheal aspiration and intravenous insertion of the cannula (Barker & Rutter, 1995). Furthermore, considering the total number of manipulations that infants usually undergo in the NICU, a total of 768 manipulations and 1,341 procedures were performed, with each manipulation having a mean of 2.2 multiple procedures (Pereira et al., 2013).
According to the International Association for the Study of Pain (IASP), pain is defined as: "an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage" (1994/2017, IASP Taxonomy para.3). The systematic review of Valeri, Holsti, and Linhares (2015) showed that the larger number of stressful and painful procedures in the neonatal period was associated with several future impacts, such as growth delay after birth and motor and cognitive development impairment. Neonatal pain results in repetition of the nociceptive stimulus, which may lead to exaggerated responses in the infants, with these possibly remaining even after the painful stimulus finishes (Grunau, 2002).
The inclusion of pain assessment and management in intensive care protocols is necessary to protect the development of the infants (Linhares, 2016). In this sense, pain relief prevention strategies should be offered, considering the impact of nociceptive stimuli in the neonatal phase, through pharmacological and non-pharmacological measures (Linhares & Doca, 2010). Non-pharmacological strategies include non-nutritive sucking, oral sucrose (sweet substance), breastfeeding, facilitated touching, skin-to-skin contact, music, swaddling, positioning, and olfactory and multisensory stimulation (Cignacco et al., 2007; Linhares & Doca, 2010).
Specifically, skin-to-skin contact, which is associated with the Kangaroo Method or Kangaroo Mother Care, constitutes one of the strategies for pain relief and can be defined as a naturalistic intervention that may involve the Kangaroo position, breastfeeding and maternal body contact (Warnock et al., 2010). Skin-to-skin contact for pain relief is recommended in the Neonate Health Manual of the Brazilian Ministry of Health (Saúde do Recém-Nascido do Ministério da Saúde do Brasil) as an intervention to be implemented in hospitals (Ministério da Saúde, 2011). According to Charpak et al. (2005), the Kangaroo Method is feasible, available and the preferred intervention to reduce the rate of neonatal morbidity and mortality. As this method includes skin-to-skin contact between mother and infant, there are several positive impacts for the infant, such as: physiological control, body temperature control, behavioral regulation and encouragement of the mother-infant bonding and breastfeeding, among others. A meta-analysis study by Johnston et al. (2014) provided evidence regarding how skin-to-skin contact is effective for pain relief, demonstrating the ability of the infants to move smoothly between the sleep and wake states, showing that this intervention increases the frequency of the infant's calm sleep.
Previous review studies showed positive results related to skin-to-skin contact for pain relief in preterm and full-term infants, analyzing studies published from 2000 to 2009 (Warnock et al., 2010) and until January 2013 (Johnston et al., 2014). It is important to note that these review studies did not exclusively include preterm infants. Therefore, the aim of the present study was to systematically review the studies published from 2010 to 2017, focusing, exclusively on preterm infants and pain relief through the skin-to-skin contact strategy included in the Kangaroo Method during neonatal hospitalization. The current study aimed to answer the following questions: (a) what are the main characteristics of the studies reviewed (country, designs, type of sample, pain measurement, variables measured and pain context)? and (b) what are the main results related to the effectiveness of skin-to-skin contact included in the Kangaroo Method for pain relief in preterm neonates?
Method
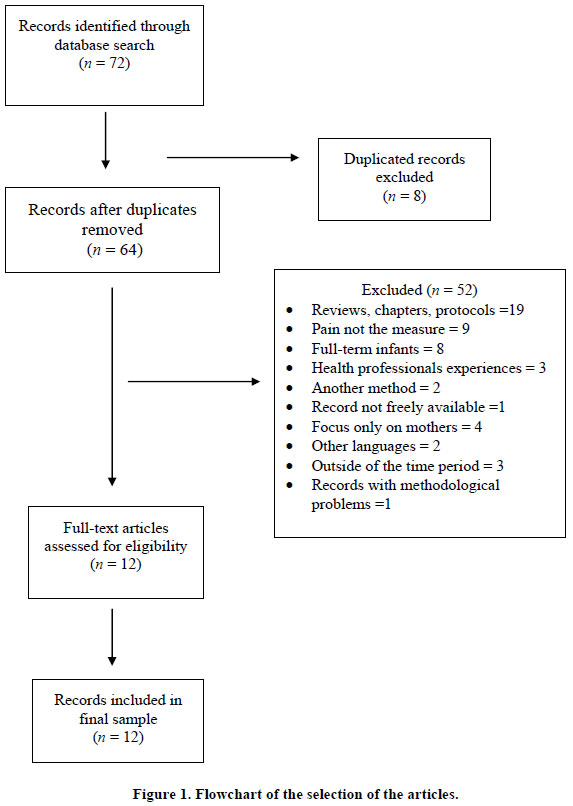
A systematic review of the scientific literature was performed, as a methodological strategy to reach the main objective of the present study, following the procedures recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyzes - PRISMA (Liberati et al., 2009). The present review included empirical articles published from 2010 to 2017, which were indexed in the PubMed, PsycINFO, SciELO and LILACS databases; this period advanced in relation to the previous review studies. In each database, the necessary variations were considered, depending on the specificities of each database to locate the studies. The descriptors and keywords used in the search for the articles were, in general, the same for all the databases: kangaroo mother care method; skin-to-skin; pain; infant/newborn. Furthermore, certain filters were used in the PubMed database, such as: publications from 2010 to 2017 and studies only with humans. In the LILACS, SciELO and PsycINFO databases, no filters were used. The following inclusion criteria were considered: (a) empirical studies evaluating skin-to-skin contact or the Kangaroo method as a pain management strategy in preterm infants; (b) articles published in English, Portuguese or Spanish; (c) articles published within the delimited time frame; and (d) articles referring only to humans. The following exclusion criteria were considered: (a) review articles, meta-analysis, comments, protocols, editorials, letters, book chapters, dissertations, theses, manuals, monographs or critiques; (b) studies focusing on the health professional team and not on the neonates.
Figure 1 shows that a total of 72 studies were found through the search conducted in April 2017. Primarily, eight articles were excluded because they were repeated in the different databases (PubMed, PsycINFO and LILACS), with 64 studies remaining. Next, the titles and abstracts of the studies were read, considering the objectives proposed for the present review, and the inclusion and exclusion criteria were applied independently by two researchers. In cases of disagreement, the authors reached a consensus through discussion. A total of 52 articles were excluded for the following reasons: (a) review articles, book chapters, study protocols, method protocols (n = 19); (b) did not use pain as a measure (n = 9); (c) the sample included only full-term infants (n = 8); (d) the study evaluated the experiences of the health professionals (n = 3); (e) the study used another pharmacological or non-pharmacological pain relief method (n = 2); (f) the article was not freely available (n = 1); (g) the focus of the study was only on the mother, without the measurement of pain (n = 4); (h) articles in languages other than those established as inclusion criteria (n = 2); (i) articles found outside the time frame (n = 3); and article with methodological problems that invalidated the results (n = 1). Finally, 12 studies were selected for analysis.
The selected articles were reviewed and analyzed according to the following topics: objective of the study, study sample, study design, intervention procedure, observed variables, pain measurement, main results of the study and limitations. The articles were read and classified according to these items by the first author and were after independently reviewed by the second author in order to ensure the accuracy of the analysis.
Results
General Characteristics of the Studies
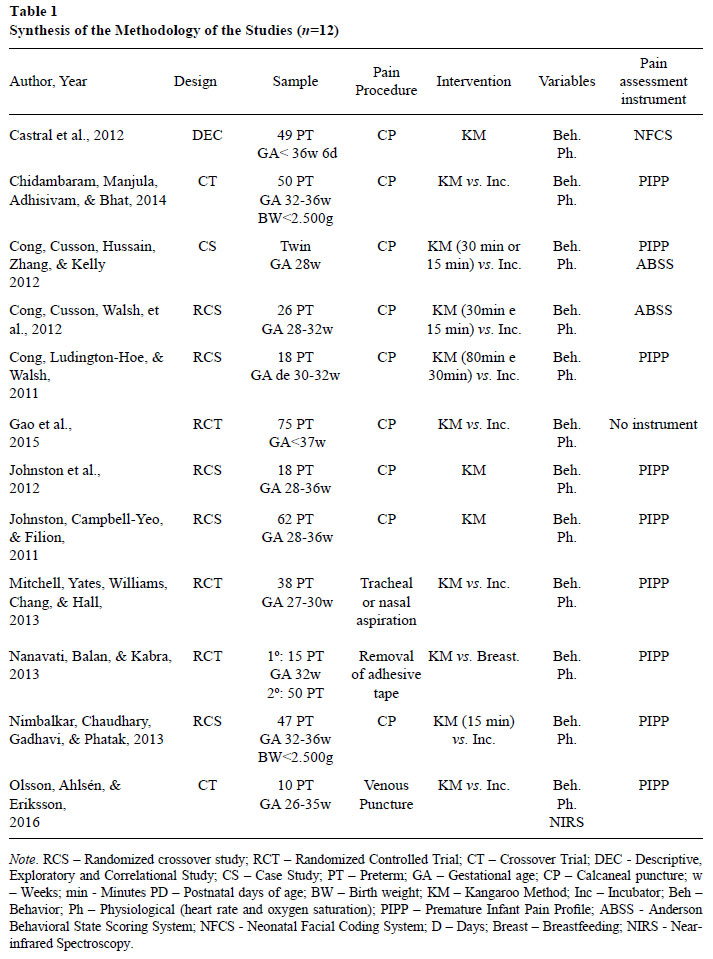
The characteristics of the studies are summarized in the Table 1.
The 12 articles were predominantly published in 2012 (n = 4; 34%) and the others were distributed between 2013 (n = 3; 25%), 2011 (n = 2; 17%), 2014 (n = 1; 8%) 2015 (n = 1; 8%) and 2016 (n = 1; 8%). The majority of the studies were conducted in North America (USA, n = 4 and Canada, n = 2), followed by countries in Asia (India, n = 3 and China, n = 1), South America (Brazil, n = 1) and Europe (Sweden, n = 1).
The studies used the following designs: randomized crossover, in 41% of the studies (Cong, Cusson, Walsh, et al., 2012; Cong et al., 2011; Johnston et al., 2012; Johnston et al., 2011; Nimbalkar et al., 2013), randomized controlled trial, in 25% of the studies (Gao et al., 2015; Mitchell et al., 2013; Nanavati et al., 2013) and crossover trial, in 17% of the studies (Chidambaram et al., 2014; Olsson, Ahlsen, & Eriksson, 2016). The remaining 17% of the studies included one descriptive and exploratory case study (Cong, Cusson, Hussain, et al., 2012) and one descriptive, exploratory and correlational study (Castral et al., 2012).
Regarding the study sample characteristics, in general, the gestational age (GA) of the infants was an important inclusion criterion in the studies, which ranged from 27 to 37 weeks of GA. One study focused on extremely preterm and very preterm infants (Mitchell et al., 2013), three studies analyzed only very preterm infants (Cong, Cusson, Hussain, et al., 2012; Cong, Cusson, Walsh, et al., 2012; Cong et al., 2011), two studies concentrated on moderate and late preterm infants (Chidambaram et al., 2014; Nimbalkar et al., 2013) and five studies adopted a general classification of infants, from 28 to 36 weeks of GA (Castral et al., 2012; Gao et al., 2015; Johnston et al., 2012; Johnston et al., 2011; Olsson et al., 2016). Only one study calculated the mean gestational age, obtaining a moderate preterm classification for the infants (Nanavati et al., 2013).
It is important to highlight the inclusion and exclusion criteria of the study samples. All the studies included clinically stable infants that could participate in the skin-to-skin contact intervention. However, clinically unstable infants were excluded, especially those infants that had been submitted to recent surgery, had received sedatives and analgesics and those that presented severe intraventricular hemorrhage (III or IV grade), congenital anomalies with malformations and/or neurological damage.
In general, the infants born preterm were evaluated prior to 15 days of postnatal age, including: at less than five days (Mitchell et al., 2013), two to nine days (Cong et al., 2011), within 10 days (Johnston et al., 2012; Nimbalkar et al., 2013) and within 15 days (Cong, Cusson, Walsh, et al., 2012; Gao et al., 2015). The other remaining studies did not specify the postnatal age. It is important to note that in some studies the birth weight of the infants was considered as an inclusion criterion; in five of these studies, the infants' birth weight was reported as <2,500g (Chidambaram et al., 2014; Nimbalkar et al., 2013) and <1,500g (Cong, Cusson, Hussain, et al., 2012; Mitchell et al., 2013, Nanavati et al., 2013).
Considering the pain assessment of the infants, the majority of the studies (n = 10; 83%) used psychometric tools validated for pain measurement. Nine studies used the Premature Infant Pain Profile (PIPP), which is a multidimensional instrument composed of behavioral, physiological, and contextual indicators to measure pain in preterm infants (Chidambaram et al., 2014; Cong, Cusson, Walsh, et al., 2012KC30; Cong et al., 2011; Johnston et al., 2012; Johnston et al., 2011; Mitchell et al., 2013; Nanavati et al., 2013; Nimbalkar et al., 2013; Olsson et al., 2016). Only one study used the Neonatal Facial Coding System (NFCS), which is an instrument that measures pain intensity through the facial activity of preterm or full-term infants (Castral et al., 2012). In the remaining two articles, the Anderson Behavioral State Scoring System (ABSS) was used to measure the behavioral state of the infants during painful procedures, which is a scale that measure the behavioral state of the infant through 12 categories (1 = very quiet sleep; 2 = quiet sleep; 3 = active sleep; 4 = very active sleep; 5 = drowsy; 6 = alert inactive; 7 = quiet awake; 8 = active awake; 9 = very active awake; 10 = fussy crying; 11 = crying; 12 = strong crying; Cong, Cusson, Hussain, et al., 2012; Cong, Cusson, Walsh, et al., 2012). In one of these articles, the ABSS was associated with the PIPP. Only one article from the total of 12 studies did not use a validated psychometric instrument for the pain assessment; this study used behavioral indicators of pain, according to the duration of grimacing and crying of the infants (Gao et al., 2015).
Regarding the type of painful procedures, performed due to clinical requirements, the calcaneal puncture was used for the pain assessment in nine articles. It is important to note that there were several designations for this procedure in the studies, such as: heel stick, heel pricking, capillary blood draws, and heel lance procedure. The remaining three articles evaluated pain during the tracheal or nasal aspiration procedure (Mitchell et al., 2013), venipuncture (Olsson et al., 2016), and removal of adhesive tape (Nanavati et al., 2013).
The variables used to assess pain responses showed similar pattern in the studies analyzed. In general, the behavior (facial activity, crying time and grimacing) and physiological measures (heart rate, oxygen saturation and salivary cortisol) were the variables used in the pain assessments. From the 12 studies, nine analyzed both physiological and behavioral indicators (Chidambaram et al., 2014; Cong, Cusson, Hussain, et al., 2012; Cong, Cusson, Walsh, et al., 2012; Gao et al., 2015; Johnston et al., 2012; Johnston et al., 2011; Nanavati et al., 2013; Nimbalkar et al., 2013; Olsson et al., 2016). The physiological measure of salivary cortisol was included in only three studies (Castral et al., 2012; Cong et al., 2011; Mitchell et al., 2013) with other physiological (heart rate and oxygen saturation) and behavioral indicators. In addition to the analysis of pain responses, the studies also analyzed the stress indicators of the preterm infants caused by the painful procedures. One study used a different procedure for pain measurement, using the previously mentioned physiological (heart rate, oxygen saturation) and behavioral measures, supported by Near-infrared spectroscopy (NIRS), which is a non-invasive technique that reflects hemodynamic changes in regions of the brain (Olsson et al., 2016). Thus, in order to have a broad view regarding the impact of painful procedures on the infants and how the intervention acts on the pain, the analysis of variables will be performed in conjunction with the skin-to-skin contact intervention addressed in the studies.
It is important to describe the of skin-to-skin contact method adopted in all the studies. The infants wore only diapers, were placed on the chest of the mothers (or other caregivers) in the skin-to-skin position, inclined from 30 to 40 degrees and both were covered with a cloth or blanket. The time that the infants and mothers remained in this position varied from one study to another, ranging from 15 to 80 minutes. In the majority of the studies, there was no information about the interactions between the mother and infant during the skin-to skin pain relief intervention; only one article reported the requirement for the mothers to avoid any type of interaction with the infants (Nimbalkar et al., 2013), whereas, in two studies the mothers were told that they could freely interact with the infants (Castral et al., 2012; Cong, Cusson, Hussain et al., 2012).
Main Results Regarding the Effectiveness of Skin-to-Skin Contact of the Kangaroo Method for Pain Relief in Preterm Neonates
The main results of the studies are organized into thematic topics, which emerged from the analysis of the articles reviewed. Firstly, the between-group comparison studies of preterm neonates submitted to skin-to-skin contact in the Kangaroo Method for pain relief and control groups are presented. Secondly, the studies about the analysis of the effective length of exposure to the skin-to-skin contact in the Kangaroo Method during painful procedures are shown. Thirdly, the studies are discussed in which the objective was to evaluate the differential effect of skin-to-skin contact in the Kangaroo Method for pain relief comparing mothers and others caregivers. Fourthly, the only study that compared the effectiveness of skin-to-skin contact in the Kangaroo Method with breastfeeding for pain relief in preterm infants is investigated. Finally, the only study that analyzed the association between skin-to-skin contact of the Kangaroo Method for pain relief and maternal indicators is presented.
Kangaroo Care Method for pain relief vs. Standard Routine Care. The Kangaroo Method for pain relief was compared to the incubation condition in five of the 12 articles analyzed. The study of Nimbalkar et al. (2013) compared 47 babies with birth weight less than 2,500 g, between 32 and 36 weeks of gestational age and with 10 days of postnatal age. The Kangaroo Method with 30 minute duration (15 minutes during calcaneal puncture and 15 minutes after this procedure) was used for pain relief in comparison to the standard routine care, in which the infant remained in the incubator without pain management intervention. Video recordings of the face and behavior of the infants were used for the measurement of the pain, as well the heart rate and oxygen saturation recorded by monitors, from the baseline to the recovery phase after the painful procedure. The instrument used for the pain assessment was the Premature Infant Pain Profile (PIPP). Thus, the infants in the Kangaroo position presented significantly lower PIPP scores than the infants who remained in the incubator. Furthermore, the heart rate of the infants was significantly reduced with the skin-to-skin contact.
Similarly, the study of Gao et al. (2015) showed the effectiveness of the skin-to-skin con-tact with duration of 30 minutes for pain relief of preterm infants during the heel stick procedure. The duration of the infants' crying and grimacing (brow bulge, eye squeeze, and nasolabial furrow) and their heart rates were analyzed. There was a combination of physiological and behavioral measures, showing that there was a reduction in the heart rate and in the duration of crying and grimacing during painful procedure in preterm infants in Kangaroo position when compared to infants in the incubator. In the study of Olsson et al. (2016), skin-to-skin contact was effective for pain relief during the venipuncture procedure. In addition to the physiological (heart rate and oxygen saturation) and behavioral measures, the study used the NIRS for the pain evaluation, which is a non-invasive technique that reflects hemodynamic changes in regions of the brain. This study examined 10 preterm infants using the PIPP score. The results were similar to previous studies, showing that the infants in the Kangaroo position presented lower physiological responses to the painful stimulus than those in the incubator. The PIPP scores were higher in the infants receiving standard care than in the infants with skin-to-skin contact, however, there was no statistical significant difference between the groups. Following this line of research, the study of Chidambaram et al. (2014) analyzed moderate and late preterm infants with less than 2,500g in Kangaroo care compared to a control group. Physiological measures (heart rate and oxygen saturation) and PIPP score were used for pain assessment, at 15 minutes before the painful procedure and at 15 and 30 minutes after it. The PIPP scores were significantly lower in the Kangaroo group than in the control group.
The study by Mitchell et al. (2013) pre-sented divergent results from the previously mentioned studies. In this study, 38 infants of 27 and 30 weeks of GA and less than five days of postnatal age were tested in the following two groups: 19 infants in the skin-to-skin contact group were placed in the Kangaroo position for two hours daily for five consecutive days and 19 infants continued to receive standard routine care, however, if the parents requested, they could be placed in the Kangaroo position for 15 minutes daily. Salivary cortisol and the PIPP scores were used for pain assessment. There was a decrease in salivary cortisol when comparing the days of testing, with higher cortisol level in the first day than the final one. However, there was no difference in the infants' cortisol level with regard to the Kangaroo position and incubator groups. The PIPP scores were higher after the painful procedure (tracheal or nasal aspiration) in comparison to the initial phase without the procedure, which remained unchanged throughout the days of testing. It is important to note that the intervention for pain relief management was not performed before or during the aspiration procedure.
Different durations of the Kangaroo position for pain relief. In this topic, three articles investigated the ideal length of time for skin-to-skin contact to be more effective for pain relief in preterm infants. In the study of Cong, Cusson, Hussain, et al. (2012), the effectiveness of the Kangaroo method was verified in a case study with twin infants of 28 weeks of GA with very low birth weight (1,500g). The infants were evaluated in three conditions (i.e.: a long period in the Kangaroo position - 30 minutes, a short period in the Kangaroo position - 15 minutes and the routine standard care - infants in the incubator) without pain relief intervention. Physiological measures (heart and respiratory rates), the behavioral state of the infants, measured through the Anderson Behavior State Scoring System (ABSS), and the PIPP scores were used for the pain assessment. The heart and respiratory rates were measured by electrodes placed on the breasts of the infants, assessing the infants' autonomic nerve responses (heart rate variability). Thus, when in the Kangaroo position the infants presented less pain than when they were in the incubator condition, during the heel stick procedure. The results demonstrated that the Kangaroo position attenuated the autonomic responses to painful stimulus. Regarding the behavioral indicators, observed through the ABSS, the time in the quiet sleep state was longer and more regular in both the long- and short- period Kangaroo positions in comparison to the incubator condition. When the infants were in the incubator during painful procedures they remained in active sleep state more. Regarding the PIPP scores, when the infants were without pain relief they presented higher clinical values than when in both the short and long duration of the Kangaroo position. There was a trend for the infants to present more pain (crying) during the longer Kangaroo position (30 minutes) than the shorter one (15 minutes).
The study of Cong, Cusson, Walsh, et al. (2012) used the same time durations (15 and 30 minutes) in the Kangaroo position in comparison to the incubator condition without pain management. A total of 26 infants of 28 to 32 weeks GA with less than 14 days of postnatal age were evaluated. The infants were exposed to the three conditions previously described, however, in different orders. The physiological measures (heart rate variability) and behavioral indicators (ABSS score) of the infants were used for the pain assessment. The focus of this study was the physiological measures and autonomic responses. In the recovery phase, after the painful procedure, there was no significant difference between the two time durations in the Kangaroo position. However, in comparison to the incubator condition, the heart rate variability was significantly lower in the Kangaroo position with duration of 30 minutes.
In another study by the same group of investigators (Cong et al., 2011), 28 infants with 30 and 32 weeks of GA and two to nine days of postnatal age were analyzed in two groups, i.e.: 18 infants were placed in the Kangaroo position for 80 minutes and compared to the incubator position with no intervention for pain relief and 10 infants were placed in the Kangaroo position for 30 minutes and also compared to the incubator position. The PIPP score and cortisol and salivary serum were measured. There was a decrease in the PIPP score and the cortisol and salivary serum with the Kangaroo position intervention for pain relief. In the first phase of the study, using the Kangaroo position for 80 minutes, the PIPP score did not differ significantly between the Kangaroo and the incubator conditions. However, in the second phase, using the Kangaroo position for 30 minutes, the PIPP score were clinically lower than the incubator condition. Regarding the salivary cortisol rate, it was significantly lower in the Kangaroo position for 30 minutes than in the other two conditions. The decreasing of cortisol levels in the preterm infants demonstrated that the infants receiving skin-to-skin contact with the mothers showed less stress and pain during the blood collection procedure.
Kangaroo Method as a pain relief strategy performed by different caregivers. In this topic, two studies aimed to analyze the effectiveness of the Kangaroo Method with caregivers other than the mothers. The study by Johnston et al. (2011) assessed 62 preterm infants, with 28 to 36 weeks of GA submitted to a heel lance procedure. The study compared mothers and fathers in the Kangaroo position. Physiological (heart rate and oxygen saturation) and behavioral (brow bulge, eye squeeze and nasolabial furrow) indicators were used as pain parameters in the PIPP score. A marginal difference between the caregivers was indicated in the results showing that, in the Kangaroo position, the mothers had a greater effect on pain relief than the fathers. In the seconds after the heel lance, in the recovery phase, the PIPP score was lower and the heart rate returned more rapidly to the same value as the baseline, in the infants with the mothers than in those with the fathers.
Another study by Johnston et al. (2012) compared the use of the Kangaroo position by mothers and other females who were chosen by the mothers (mother-in-law, sister-in-law, mothers' friend, other mother or health professional in the hospital), in a sample of 18 preterm infants from 28 to 36 weeks of GA. The study sample was small, an aspect that was highlighted by the authors as a relevant limitation, due to the high number of mothers that refused to participate in the study during the recruitment phase. The pain assessment was performed using physiological (heart rate and oxygen saturation) and behavioral (brow bulge, eyes squeeze, and nasolabial furrow) measures of the PIPP score. The physiological and behavioral indicators changed with the Kangaroo intervention for pain relief, however, the findings were inconclusive with regard to a greater pain relief effect of the Kangaroo position with the mothers compared to the others females.
Kangaroo Method versus Breastfeeding for pain relief. The study of Nanavati et al. (2013) evaluated 50 preterm infants with a mean of 32 weeks GA and birth weight of 1,250g aiming to compare the effectiveness of the Kangaroo method and breastfeeding as non-pharmacological methods for pain relief. Initially, they assessed whether the removal of adhesive tape was a painful procedure for preterm and extremely low birth weight infants and subsequently the comparison between the two modalities of pain relief was performed. Physiological (heart rate and oxygen saturation) and behavioral (infants' body activity, open or closed eyes, and facial movements) indicators were used for the pain assessment. Firstly, the removal of adhesive tape in the extremely preterm and low birth weight infants was found to be a painful procedure, considering the PIPP score. Secondly, the pain scores were significantly lower after both interventions for pain relief, indicating minor or no pain. The heart rate and oxygen saturation levels remained stable, demonstrating positive results for the use of both interventions. In conclusion, the Kangaroo position and breastfeeding interventions were equally effective for pain relief, with no significant differences between the groups.
Kangaroo Method for pain relief related to the maternal characteristics. In this topic, only one study evaluated the pain responses related to the characteristics of both the infants and mothers in skin-to-skin contact. The study of Castral et al. (2012) analyzed 49 clinically stable infants of less than 36 weeks of GA and their mothers, who had the cognitive ability to understand the instructions of the instruments and did not present psychiatric diagnosis, except for depression and anxiety symptoms. The associations between maternal factors (behavior during the painful event of the infant, depression and/or anxiety and stress) and the pain responses of the infants while in the Kangaroo position were examined. The behavioral (facial expressions, sleep and wake states and crying) and physiological (heart rate and salivary cortisol) indicators were observed. The NFCS assessed the infants' pain. The Maternal Mood and Behavior during her Infant's Pain Coding System (MMBIPCS) assessed the depressive symptoms of the mothers, the Beck Depression Inventory (BDI) and the Beck Anxiety Inventory (BAI) evaluated the depression and anxiety symptoms, respectively, and the Structured Clinical Interview for DSM-IV-SCID-CV was used to describe the mothers' psychiatric history. Significant associations were found, suggesting a co-regulation process between the mothers and infants in this neonatal context. There was an association between the maternal cortisol level and the analyzed indicators of the neonates, such as the NFCS pain score, length of crying, heart rate, and salivary cortisol. The cortisol level of the mother in the night prior to the pain assessment was associated with the heart rate of the infant when performing the skin-to-skin contact during the pain assessment; this finding suggests the mediation of the Kangaroo position on the autonomic nervous system of the infants. Furthermore, the mothers' behavior (typical/typically depressive) and the depression and/or anxiety symptoms did not affect the pain and stress responses of the infants. The skin-to-skin contact between the mother and baby may have softened the negative effects of the depression and anxiety symptoms of the mothers.
Discussion
The findings of the present systematic literature review demonstrate the effectiveness of skin-to-skin contact as a non-pharmacological strategy for pain relief management in preterm neonates, during the neonatal intensive care. Regarding the designs of the studies, five of them used a randomized crossover design, showing high methodological rigor in these studies. Randomized clinical trials are considered the "gold standard" in clinical and health studies and are recommended for the examination of the effectiveness and efficacy of interventions (Greenhalgh, 2013).
In 11 of the 12 studies, positive results were found regarding the effectiveness of the skin-to-skin contact intervention for pain relief during acute painful procedures. Only one study presented negative findings; however, in this study the skin-to-skin contact was not performed during the invasive and painful procedure, but at other times during the day regardless of the painful event. Another possible explanation for the lack of positive results could be related to the fact that, at the request of the parents, the infants that were in the incubator condition (control group) could also be placed in the Kangaroo position for 15 minutes per day. It was important to include this study in the present systematic review to demonstrate that skin-to skin contact for pain relief intervention is effective when it is directly associated with the painful procedures. It should be mentioned that the painful procedures were performed through the prescription of physicians according to the clinical demands of each patient. The skin-to-skin contact for pain management was used when the infants were clinically stable and upon medical recommendation and release, an important aspect to be observed when using this intervention procedure in the context of pain relief.
Focusing on the duration of the skin-to-skin contact, the studies analyzed different times, with them all presenting positives results for pain relief, however, the 30 minute duration was found to be the most effective length of time. Skin-to-skin contact with the mother was shown to be effective for pain relief and some studies demonstrated the effectiveness of the strategy with others people, besides the mothers. Preliminary findings showed that skin-to-skin contact, with both mothers and fathers, was effective in decreasing pain in preterm infants. However, the results were inconclusive when skin-to-skin was performed by other women. It is interesting to note that many mothers refused to participate in the studies that were dedicated to this question of comparing the mother and other women in the skin-to-skin position. In general, the mothers presented difficulty accepting that another woman would remain in such intimate skin-to-skin contact with their newborn. The majority of the mothers that agreed to participate in the study, requested that the other female be a member of the nursing team, presumably because these mothers felt more secure with a trained nurse who had daily contact with their infants. It should be noted that the study complied with the ethical principle of voluntary participation, with the signing of a consent form. The assessment of the effects of skin-to-skin contact with other people, apart from the mothers, may be a useful strategy in cases where the mother has disabilities, is limited regarding her presence in the NICU or presents a severe clinical health condition. It is also emphasized that the samples in these studies were very small, which contributed to the results not being conclusive with regard to the effectiveness of skin-to-skin contact with other people besides the mother. Further studies could address the question about the effects of skin-to-skin contact with people other than the mother for pain relief management in preterm infants.
Regarding the analysis strategies of the effectiveness of the skin-to skin position, the studies used several measures for pain assessment. The procedures for measuring pain, using behavioral and physiological parameters, were appropriate and, consequently, similar results were found in the majority of the studies reviewed. It is emphasized that in order to assess pain adequately it is necessary to use standardized and psychometrically validated instruments. The Premature Infant Pain Profile scale was the most used instrument, which is appropriate and validated for the pain assessment of preterm infants. Of the 12 studies analyzed, 10 used scales to measure pain, with systematic measures to identify pain related behaviors. In one of the studies, which did not use a scale, the frequency and duration of some standard behaviors (grimacing and crying duration) were measured (Gao et al., 2015). If a standardized pain measure is not used, it is not possible to be sure about the specificity of the infants' pain response. That is, the infants' reaction could be related to another environmental stimulus. One study used only a scale to observe the infants' behavioral states and theirs reactions to painful stimuli (Cong, Cusson, Walsh, et al., 2012), which limits the specificity and sensitivity of these responses in relation to the pain evaluation.
Some limitations could be identified in the studies of the present review, such as: some of them did not use standardized and validated instruments for the pain assessment of preterm infants, some studies had small samples that did not allow conclusive results and, consequently, it was difficult to generalize the findings. Also, the studies did not aim to analyze the effectiveness of skin-to-skin contact for pain relief according to the gestational age of the infants, considering the level of prematurity (extremely premature, very premature or moderately premature); the majority of the studies used a general clas-sification of the infant's gestational age. Thus, future studies should address this question and analyze the differences in pain responses of preterm infants divided into groups differentiated by the gestational age.
It is also recommended for future studies to use the randomized crossover design in order to strengthen the methodological aspects of the literature, increasing the quality of the scientific evidence regarding the skin-to-skin contact intervention for pain relief. It is also suggested that samples could be enlarged to obtain more powerful sample sizes. In addition, longitudinal studies could be an advance, in comparison to cross-sectional studies, aiming to detect the protective effects of the skin-to-skin contact pain at neonatal phase on the medium-term development of preterm infants.
Regarding the scientific evidence obtained up to the present moment, it is possible to affirm the effectiveness of skin-to-skin contact between mothers and neonates for pain relief in the hospital context. The transfer of scientific knowledge regarding skin-to-skin contact to the clinical practice is absolutely necessary, as previously recommended by the Brazilian Ministry of Health (Ministério da Saúde, 2011). However, there are some challenges for the training of professionals and the implementation and maintenance of this pain relief protocol in hospitals. Therefore, there is a requirement for skin-to-skin contact to become used in the clinical routine of the hospital, since it is a low-cost strategy and additionally presents several benefits regarding the mother-infant interactions, promoting bonding and healthcare with a more sensitive and humanized approach.
Finally, the restriction of the time period and the previously established criterion for specific languages, as well as the difficulty in obtaining some studies, constituted some limitations of the present review. Another aspect was that there was no restriction regarding the study design, with non-randomized controlled articles included in the analysis. A meta-analysis was not performed in the present study, remaining a possible statistical analysis of the results that can be carried out in future review studies.
References
Associação Internacional para o Estudo da Dor. (2017). IASP Terminology. (Reprinted and updated from Classification of Chronic Pain: IASP Task Force on Taxonomy, Pt. III, pp. 209-214, by H. Merskey & N. Bogduk, Eds., 1994, Seattle, WA: International Association for the Study of Pain Press). Retrieved from http://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1698&navItemNumber=576 [ Links ]
Barker, D. P., & Rutter, N. (1995). Exposure to invasive procedures in neonatal intensive care unit admissions. Archives of Disease in Childhood. Fetal and Neonatal Edition, 72,47-48. doi: https://doi.org/10.1136/fn.72.1.F47 [ Links ]
Cassiano, R. G. M., Gaspardo, C. M., & Linhares, M. B. M. (2016). Prematurity, neonatal health status, and later child behavioral/emotional problems: A systematic review. Infant Mental Health Journal, 37(3),274-288. doi: https://doi.org/10.1002/imhj.21563 [ Links ]
Castral, T. C., Warnock, F. F., Ribeiro, L. M., Vasconcelos, M. G. L., Leite, A. M., & Scochi, C. G. S. (2012). Maternal factors regulating preterm infants' responses to pain and stress while in maternal kangaroo care. Revista Latino-Americana de Enfermagem, 20(3),435-443. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/22991104 [ Links ]
Chabra, S. (2013). Subsets of preterm and term infants: Call for consistency in terminology. Developmental Medicine and Child Neurology, 55(7),673. doi: https://doi.org/10.1111/dmcn.12126 [ Links ]
Charpak, N., Ruiz, J. G., Zupan, J., Cattaneo, A., Figueroa, Z., Tessier, R., ...Worku, B. (2005). Kangaroo Mother Care: 25 years after. Acta Paediatrica (Oslo, Norway), 94(5),514-522. doi: https://doi.org/10.1080/08035250510027381 [ Links ]
Chidambaram, A. G., Manjula, S., Adhisivam, B., & Bhat, B. V. (2014). Effect of Kangaroo mother care in reducing pain due to heel prick among preterm neonates: A crossover trial. The Journal of Maternal-Fetal & Neonatal Medicine, 27(5),488-490. doi: https://doi.org/10.3109/14767058.2013.818974 [ Links ]
Cignacco, E., Hamers, J. P. H., Stoffel, L., van Lingen, R. A., Gessler, P., McDougall, J., & Nelle, M. (2007). The efficacy of non-pharmacological interventions in the management of procedural pain in preterm and term neonates. A systematic literature review. European Journal of Pain, 11, 139-152. doi: https://doi.org/10.1016/j.ejpain.2006.02.010 [ Links ]
Cong, X., Cusson, R. M., Hussain, N., Zhang, D., & Kelly, S. P. (2012). Kangaroo care and behavioral and physiologic pain responses in very-low-birth-weight twins: A case study. Pain Management Nursing, 13(3),127-138. doi: https://doi.org/10.1016/j.pmn.2010.10.035 [ Links ]
Cong, X., Cusson, R. M., Walsh, S., Hussain, N., Ludington-Hoe, S. M., & Zhang, D. (2012). Effects of Skin-to-skin contact on autonomic pain responses in preterm infants. The Journal of Pain, 13(7),636-645. doi: https://doi.org/10.1016/j.jpain.2012.02.008 [ Links ]
Cong, X., Ludington-Hoe, S. M., & Walsh, S. (2011). Randomized crossover trial of kangaroo care to reduce biobehavioral pain responses in preterm infants: A pilot study. Biological Research For Nursing, 13(2),204-216. doi: https://doi.org/10.1177/1099800410385839 [ Links ]
Gao, H., Xu, G., Gao, H., Dong, R., Fu, H., Wang, D., ...Zhang, H. (2015). Effect of repeated Kangaroo Mother Care on repeated procedural pain in preterm infants: A randomized controlled trial. International Journal of Nursing Studies, 52(7),1157-1165. doi: https://doi.org/10.1016/j.ijnurstu.2015.04.006 [ Links ]
Greenhalgh, T. (2013). Chegando ao ponto: Do que trata este artigo? In Como ler artigos científicos: Fundamentos da medicina baseada em evidências (pp. 50-66). Porto Alegre, RS: Artmed. [ Links ]
Grunau, R. V. E. (2002). Early pain in preterm infants. A model of long-term effects A model of long-term effects. Clinics in Perinatology, 29,373-394. [ Links ]
Johnston, C., Byron, J., Filion, F., Campbell-Yeo, M., Gibbins, S., & Ng, E. (2012). Alternative female kangaroo care for procedural pain in preterm neonates: A pilot study. Acta Paediatrica, 101(11),1147-1150. doi: https://doi.org/10.1111/j.1651-2227.2012.02813.x [ Links ]
Johnston, C., Campbell-Yeo, M., Fernandes, A., Inglis, D., Streiner, D., & Zee, R. (2014). Skin-to-skin care for procedural pain in neonates. In C. Johnston (Ed.), Cochrane Database of Systematic Reviews (Vol. 1, pp. 1-82). Chichester, UK: John Wiley & Sons. doi: https://doi.org/10.1002/14651858.CD008435.pub2 [ Links ]
Johnston, C., Campbell-Yeo, M., & Filion, F. (2011). Paternal vs maternal kangaroo care for procedural pain in preterm neonates: A randomized crossover trial. Archives of Pediatrics & Adolescent Medicine, 165(9),792-796. doi: https://doi.org/10.1001/archpediatrics.2011.130 [ Links ]
Klein, V. C., Gaspardo, C. M., & Linhares, M. B. M. (2006). Dor, Autorregulação e temperamento em recém-nascidos pré-termo de alto risco. Psicologia: Reflexão e Crítica, 24(3),504-512. doi: https://doi.org/10.1590/S0102-79722011000300011 [ Links ]
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P. A., ...Moher, D. (2009). The PRISMA Statement for Reporting Systematic Reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Medicine, 6(7),e1000100. doi: https://doi.org/10.1371/journal.pmed.1000100 [ Links ]
Linhares, M. B. M. (2016). Estresse precoce no desenvolvimento: Impactos na saúde e mecanismos de proteção. Estudos de Psicologia (Campinas), 33(4),587-599. doi: https://doi.org/10.1590/1982-02752016000400003 [ Links ]
Linhares, M. B. M., & Doca, F. (2010). Dor em neonatos e crianças: Avaliação e intervenções não farmacológicas. Temas em Psicologia, 18(2),307-325. Recuperado em http://pepsic.bvsalud.org/scielo.php?pid=S1413-389X2010000200006&script=sci_arttext&tlng=en [ Links ]
Ministério da Saúde. (2011). Dor no recém-nascido. In Atenção à Saúde do Recém-Nascido: Guia para os profissionais de saúde. Intervenções comuns, icterícia e infecções: Vol. 2 (pp. 33-45). Brasília, DF: Autor. [ Links ]
Ministério da Saúde. (2015). Nascidos Vivos - Brasil. Recuperado em http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinasc/cnv/nvuf.def [ Links ]
Mitchell, A. J., Yates, C. C., Williams, D. K., Chang, J. Y., & Hall, R. W. (2013). Does daily kangaroo care provide sustained pain and stress relief in preterm infants? Journal of Neonatal-Perinatal Medicine, 6(1),45-52. doi: https://doi.org/10.3233/NPM-1364212 [ Links ]
Nanavati, R. N., Balan, R., & Kabra, N. S. (2013). Effect of kangaroo mother care vs expressed breast milk administration on pain associated with removal of adhesive tape in very low birth weight neonates: A randomized controlled trial. Indian Pediatrics, 50, 1011-1015. Retrieved from http://www.indianpediatrics.net/nov2013/1011.pdf [ Links ]
Nimbalkar, S. M., Chaudhary, N. S., Gadhavi, K. V., & Phatak, A. (2013). Kangaroo mother care in reducing pain in preterm neonates on heel prick. Indian Journal of Pediatrics, 80(1),6-10. doi: https://doi.org/10.1007/s12098-012-0760-6 [ Links ]
Olsson, E., Ahlsén, G., & Eriksson, M. (2016). Skin-to-skin contact reduces near-infrared spectroscopy pain responses in premature infants during blood sampling. Acta Paediatrica, 105(4),376-380. doi: https://doi.org/10.1111/apa.13180 [ Links ]
Pereira, F. L., Goes, F. D. S. N. de, Fonseca, L. M. M., Scochi, C. G. S., Castral, T. C., & Leite, A. M. (2013). A manipulação de prematuros em uma Unidade de Terapia Intensiva Neonatal. Revista da Escola de Enfermagem da USP, 47(6),1272-1278. doi: https://doi.org/10.1590/S0080-623420130000600003 [ Links ]
Valeri, B. O., Holsti, L., & Linhares, M. B. M. (2015). Neonatal pain and developmental outcomes in children born preterm: A systematic review. The Clinical Journal of Pain, 31(4),355-362. doi: https://doi.org/10.1097/AJP.0000000000000114 [ Links ]
Warnock, F. F., Castral, T. C., Brant, R., Sekilian, M., Leite, A. M., Owens, S. de la P., & Scochi, C. G. S. (2010). Brief report: Maternal kangaroo care for neonatal pain relief: A systematic narrative review. Journal of Pediatric Psychology, 35(9),975-984. doi: https://doi.org/10.1093/jpepsy/ jsp123 [ Links ]
World Health Organization. (2016). Preterm birth. Retrieved from http://www.who.int/mediacentre/factsheets/fs363/en/ [ Links ]
 Mailing address:
Mailing address:
Maria Beatriz Martins Linhares
Universidade de São Paulo, Faculdade de Medicina de Ribeirão Preto
Rua Tenente Catão Roxo, 2650, Vila Monte Alegre
Ribeirão Preto, SP, Brazil 14051140
Phone: (16) 3315-4610; Fax: (16) 3315- 4504
E-mail: linhares@fmrp.usp.br
Received: 22/08/2017
1st revision: 04/10/2017
Accepted: 18/10/2017


{kind=link}