










Services on Demand

article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Curriculum ScienTI
Curriculum ScienTIIndicators
Share

 Permalink
PermalinkBoletim - Academia Paulista de Psicologia
Print version ISSN 1415-711X
Bol. - Acad. Paul. Psicol. vol.35 no.88 São Paulo Jan. 2015
THEORIES, RESEARCHES AND CASE STUDIES
A comparative study about mother-child interaction with groups of asthmatic, congenital heart disease and healthy children
Estudio comparativo sobre la interacción madre-hijo entre grupos de niños asmáticos, cardiópatas congénitos y sanos
Um estudo comparativo sobre a interação mãe-filho em grupos de crianças asmáticas, com doenças cardíacas congênitas, e saudáveis
Dóris Lieth PeçanhaI,1; César Augusto PiccininiII,2; William Stuart MillarIII,3
I(Chair nº19 Sao Paulo Academy of Psychology - A.P.P.)
IIFederal University of San Carlos (UFSCar), Federal University of Rio Grande do Sul
III(UFRGS)& London Metropolitan University
ABSTRACT
Mother-child interaction has been extensively examined by theoretical, empirical and clinical studies. Nonetheless, to date little has been reported about the impact of childhood chronic illness on mother-child interaction. A chronic childhood illness is a medical condition that is long term or permanent, is rarely able to be completely cured and is doubling in prevalence. Thus, the objective of this study was to compare mother-child and stranger-child interaction in different childhood health conditions using micro analytic coding of videotaped mother-child interactions. Two groups of children (M age = 4 years) suffering from chronic illness: asthma and congenital heart disease (CHD) were compared with a group of healthy children in a sequence of videotaped play interaction with the mother and with a stranger. The findings revealed significant differences in the mutual interaction between mother and the asthmatic child compared to the heart disease and healthy groups. Mothers of the asthmatic group were significantly more directive of their child in the play situation compared to the other groups. There were no differences among the three groups of children when interacting with the stranger. The findings suggest that there are specific dynamics associated with asthmatic child-mother dyads.
Keywords: Mother-child interaction, asthma, heart disease, childhood chronic illness
RESUMEN
La interacción madre-hijo ha sido ampliamente analizado en estudios teóricos, empíricos y clínicos. Sin embargo, hasta la fecha, poco se ha informado sobre el impacto de la cronicidad de las enfermedades en la infancia en la interacción madre-hijo. La enfermedad crónica infantil es una condición médica de largo plazo o permanente, rara vez se puede curar completamente. El objetivo de este estudio es comparar la interacción madre-hijo (Media de edad = 4 años de edad) y la interacción del niño con un desconocido en diferentes condiciones de salud de los niños, mediante el proceso de micro análisis de las interacciones grabadas en vídeo. Dos grupos de niños que sufren de enfermedades crónicas: asma y enfermedad cardiaca congénita (ECC) se comparan con un grupo de niños sanos en una secuencia de interacción en una situación de juego, documentada en video con la madre y el extraño. Los resultados muestran diferencias significativas en la interacción entre la madre y los niños asmáticos en comparación con el grupo de niños con ECC y el de niños saludables. Las madres del grupo de asma se muestan significativamente más directivas en relación a los niños en la situación de juego, en comparación con los otros grupos. No hubo diferencias entre los tres grupos de niños para interactuar con el extraño. Los resultados sugieren que existe una dinámica específica asociada con el asma díadas madre-hijo.
Palabras clave: Interacción madre-hijo, asma, cardiopatía, enfermedad crónica en la infancia.
RESUMO
A interação mãe-filho tem sido amplamente analisada em estudos teóricos, empíricos e clínicos. No entanto, até o momento, pouco é relatado sobre o impacto da cronicidade de uma doença na infância sobre a interação mãe-filho. A doença crônica infantil é uma condição médica de longa duração ou permanente, raramente pode ser completamente curada e está dobrando em prevalência. Assim, o objetivo deste estudo é comparar a interação mãe-filho (M Idade = 4 anos) e a interação dessa criança com uma pessoa estranha, em diferentes condições de saúde na infância, utilizando o processo de micro análise de interações gravadas em vídeo. Dois grupos de crianças que sofriam de doenças crônicas: asma e doença cardíaca congênita (DCC) são comparados com um grupo de crianças saudáveis em uma sequência de interação, numa situação de brinquedo, gravada em vídeo com a mãe e com a estranha. Os resultados mostram diferenças significativas na interação entre a mãe e a criança asmática em relação aos grupos com doença cardíaca e saudáveis. As mães do grupo de asmáticos mostam-se significativamente mais diretivas em relação à criança, na situação de brinquedo, em comparação com as dos outros grupos estudados. Não há diferenças entre os três grupos de crianças ao interagir com a estranha. Os resultados sugerem que há uma dinâmica específica associada com as díades mãe-criança asmática.
Palavras-chave: interação mãe-criança, asma, cardiopatia.
I. Introduction
Mother-child interaction has been extensively examined by theoretical, empirical and clinical studies. Nonetheless, there is a dearth of data concerning the interaction between mothers and children with chronic diseases (Laing et al., 2010). A chronic childhood illness is a medical condition that is long term or permanent, is rarely able to be completely cured and is doubling in prevalence.
Asthma is the most common chronic illnesses of childhood (Crespo, Ayala, Vercammen-Grandjean, Slymen & Elder, 2011; Stewart, Masuda, Letourneau, Anderson & McGhan, 2011; WHO, 2011) with marked increase over the past 25 years (Cloutier, 2008). Racial and ethnic disparities in asthma prevalence and severity exist and are partially explained by genetic, environmental, social, cultural, and economic factors (Crespo et al., 2011). Meanwhile the impact of asthma on African-Americans and Latino subgroups has been highlighted in the literature (Garro, 2011).
Asthma is characterized by reversible airway obstruction, airway hyperresponsiveness, and airway inflammation. Further it can be more than an inflammatory disease (Faffe, 2008). Studies demonstrated only a weak correlation between the degree of airway obstruction and the magnitude of asthma symptoms. Changes in inflammatory makers would point to a biological mechanism underlying associations between parental distress and child asthma morbidity (Wolf, Miller & Chen, 2008). The asthma is considered a multifactorial illness in which organic factors interact with psychological factors (Gustaffson, Kjellman & Bjorksten, 2002; Klinnert et al., 2001; Klinnert, Kaugars, Strand & Silveira, 2008; Minuchin et al., 1975; Mrazet & Klinnert, 1996; Nagano et al., 2010; Nogueira & Lopes, 2010; Peçanha & Lacharité, 2007; Peçanha, in press) although the etiological and developmental factors related to this condition are not fully understood. The multifactorial approach (Guerra & Martinez, 2008) emphasizes the interdependence of genetic, allergic, infectious and psychological factors in the onset and development of asthmatic symptoms. This is supported by increasing evidence that there is a genetic liability to the development of asthma, but that additional psychosocial factors may be required for phenotypic expression (Klinnert et al., 2001; Mrazek & Klinnert, 1996). A static model in which the DNA sequence is associated with disease risk in a linear fashion fails to consider the interdependence of the diverse components of asthma risk (Guerra & Martinez, 2008). Prospective studies with children who were genetically at risk for developing asthma found evidence that problems of parenting and coping with the infant in the postnatal period were significantly predictive of the onset of asthma in later childhood (Klinnert et al., 2001; Mrazek & Klinnert, 1996).
Psychosocial stressors such as communication patterns have been shown to have an adverse effect on the functioning of the immune system and to increase the individual's vulnerability to infections and allergic disease (Gustafsson, Kjellman & Bjorksten, 2002; Nagano et al., 2010; Peçanha, Pérez-Ramos & Lacharité, 2003; Peçanha & Lacharité, 2007; Wolf et al., 2008). Additionally Fiese, Winter, Anbar, Howell and Poltrock (2008) found that the burden of routine asthma care negatively affected children through dyadic mother-child interaction. Under this condition mothers expressed more critical attitudes and rejection of the asthmatic child.
Negative mother-child interactional patterns for asthmatic were reported (Debray, 2008; Gustafsson et al., 2002; Madrid, 2006; Madrid & Schwartz, 1991; Szwec, 1993). Maternal rejection and over-protection have been associated with childhood asthma (Kreisler, 1976/1992; Madrid, 2006; Madrid & Schwartz, 1991) although generalizations about mother and child personalities are not accepted (Debray, 2008; Kreisler, 1976/1992; Szwec, 1993). In a study classic Kreisler, Fain and Soulé (1987) observed that: mothers on occasion provided excessive stimulation while on other occasions showed disinterest and inconsistency towards the child. A prospective investigation conducted with mothers of asthmatic child (212 years) showed a mothers' high active rejection for her child aged < 7 years (Nagano et al., 2010). The associations between a mother's psychosocial characteristics and her child's asthma were different according to the child's age. For children aged < 7 years, a mothers' high active rejection or interference score was correlated with more severe disease at baseline.
Retrospective findings have shown that infants who developed asthma when older were more likely to have early bonding difficulties with their mothers compared with healthy children (Debray, 2008; Kreisler, 1976/1992; Madrid & Schwartz, 1991; Peçanha, in press; Szwec, 1993). In the histories of asthmatic children some postnatal events seem to interfere with mother-infant bonding like mother-infant physical or emotional separation, premature introduction of a stranger in the baby's life and mother´s difficulty to accept the presence of a third person with your baby (Kreisler, 1976/1992). With respect to the contribution of the child, there is evidence of an association between behavioral disorders and asthma, irrespective of sex, age and severity of asthma (Salomão Júnior, Miyazaki, Cordeiro, Domingos & Valerio, 2008). This finding raises the question of whether the asthmatic child's behavioral problems are circumscribed to the relationship with the mother.
With respect to the procedure to analyze interactions the major part of investigations used videotaped mother-child sessions (Duhalde, Tkach, Esteve, Huerin & R. de Schejtman, 2011). A study classic (Hermanns, Florin, Dietrich, Rieger & Hahlweg, 1989) analyzed videotaped mother-child talk and concluded that mothers whose children had more frequent asthma attacks tended to show more critical attitudes to them. Mäntymaa et al. (2003) investigated the impact of the quality of early mother-infant interaction on the subsequent physical health of the child. The results indicated that poor dyadic mother-infant interaction and infant's poor interactive behavior were separately associated with the physical health of the child during follow-up. Further infant's poor interactive behavior remained as a significant predictor of chronic health problems in the child.
Although these comparative studies point to potentially differences in parental behavior towards the child, they fail to determine the degree to which the chronicity of the illness may act as a stressor and interfere with the mother-child relationship. In order to examine the influence of the chronicity factor on the mother-child interaction this investigation compares children suffering from two chronic medical conditions: chronic asthma and congenital heart disease (CHD), with a group of healthy children.
Congenital heart disease (CHD) is a commonly diagnosed problem affecting between 4 and 14 per 1,000 full term live born infants (Rosa, Zen, Graziadio & Paskulin, 2011). A CHD is a defect in the structure of the heart and great vessels, which is present at birth. Heart malformations are among the most common birth problems. Many defects do not need treatment, others require medication or surgery. The cause of CHD may be either genetic or environmental, but is usually a combination of both. Genetically, the mother plays a greater part in CHD than the father does. Known antenatal environmental factors include maternal infections (Rubella), drugs (alcohol, hydantoin, lithium and thalidomide) and maternal illness (diabetes mellitus, phenylketonuria, and systemic lupus erythematosus) (Hoffman, 2005). Due to medical advances mortality rates for children with heart disease have decreased. Despite of that, morbidities significantly affect the child's neurodevelopmental, psychosocial, and physical functioning (Marino, Uzark, Ittenbach & Drotar, 2010). Unlike chronic asthma, congenital heart disease seems organic in origin. Yet both are chronic illnesses which are likely to constitute a significant stressor in the child's life.
Studies suggested that mothers promote their children's global development by engaging in highly responsive interactions with them. This is facilitated by mothers having good mental health and social support, and not being unduly stressed by a childhood chronic disease (Mahoney, Kim & Lin, 2007; Mahoney, Perales, Wiggers & Herman, 2006). Then it was predicted that chronicity of the illness would have an adverse effect on the mother-child interaction for the asthmatic and chronic heart disease groups compared to the healthy children. The study also investigates whether the interactional patterns of the chronic illness groups are circumscribed to their interactions with the mother by comparing mother-child and stranger-child interactions.
II. Method
II.1 Participants
Thirty-seven mothers and their children (19 males, 18 females, Mean = 4 years old) were recruited from hospital out-patient and community pediatric clinics in Porto Alegre, Brazil. They represented all eligible participants who agreed to take part in the project. The physical, motor and emotional development was assessed from pediatric records and also from a structured interview conducted with the mother. Children in the three groups (asthmatic, CHD and healthy) lived with their biological parents.
Mothers' ages ranged from 29-40 years (Mean = 34 years, SD = 5.5). On the basis of parental education (M = 15 years), fathers occupation and family income, all participants came from middle income socioeconomic backgrounds based on Hollingshead's Socioeconomic Status (SES) index (Hollingshead, 1975). This index has been used since it appeared as an unpublished paper (1975) until it becomes a citation classic (Adams & Weakliem, 2011; Eid et al., 2013). SES was controlled because associations between lower SES and physical health have been documented in childhood, including asthma hospitalizations and cardiovascular disease (Chen & Matthews, 2001).
Seventeen asthmatic children were recruited from an out-patient facility for asthmatic children (M age = 4 years 2 months, SD = 10 months; 9 boys, 8 girls). Asthma diagnosis was given by the child's doctor for longer than one year and children had no other chronic medical condition. Seven were reported to have had up to four asthmatic crises in the preceding year, six between five and ten crises, and four in excess of eleven crises. All asthmatic children had previously been hospitalized for the condition at least once and seven had required hospital treatment on two or more occasions.
The congenital heart disease (CHD) sample comprised nine children (M age = 4 years 7 months, SD = 11 months; four boys, five girls) recruited from an outpatient clinic of a major heart disease institute. Heart disease children with other health problems were excluded from the study.
All children had undergone successful heart surgery at least one year prior to the study. This group was in a clinically stable condition having no current medical problems when the study was carried out.
A sample of 11 healthy children (M age 4 = years 4 months, SD = 11 months; six boys, five girls) was recruited from a community pediatric clinic. These children were not suffering from chronic medical condition, or other allergic problem that could pose a threat to the validity of an investigation with asthmatics (Peçanha & Lacharité, 2007). Their medical records indicated no important medical history. The criterion for inclusion in this group was the absence of physical, motor and mental symptoms and the absence of any request for psychological intervention in respect of the child and his nuclear family. The physical, motor and emotional development was assessed from pediatric records and also from a structured interview conducted with the mother.
Design and Procedure
A 3 x 3 factorial design was used, with three levels of child health condition (asthmatic, CHD and healthy) and a sequence of three interaction episodes as the within-group factor (mother-child-1, stranger-child, and mother-child-2). This study followed the National Health Council (CNS no. 196 in 1996) resolution about ethics in research with human beings. Then all potential participants were informed that participation in the study was voluntary and mothers gave consent for the dyadic (mother-child) study participation. To protect the children and mothers´ identity instead of name them a numeric protocol was implemented. Access to the data was limited to investigators.
II.2 Mother/stranger-child interaction episodes
Social interaction sequences of episodes took place in a playroom (4.5 m x 5.5 m) equipped with two remote-controlled cameras, a one-way observation screen, two chairs, a child's chair and a set of toys suitable for children age. It was used multipurpose toys such as blocks and role-play materials including dolls and toy cars. The material has been arranged on the floor in the center of the room. The mother and child, and the female stranger and child were videotaped during a 21 minutes session that consisted of three consecutive interaction episodes: (a) 8 minutes mother-child interaction (M-C1); (b) 5 minutes mother-child-stranger interaction with 2 minutes of stranger-child alone (S-C); and (c) 8 minutes postseparation mother-child-stranger interaction, 6 minutes of which involved the mother and child alone (M-C2).The sequence of interactions episodes was similar to the classic strange situation (Ainsworth, Blehar, Waters & Wall, 1978). Moreover, the behavioral observation considered Keller's suggestions (2003) concerning the interval recording and the time sample.
The stranger-child interaction was shortened to two minutes since the pilot study showed that the chronically children groups were more likely to become upset in the situation with the stranger. With regard to mother-child videotaped interaction 8 minutes has also been examined in similar studies (Duhalde et al., 2011; Raznoszcyk de Schejtman et al., 2005). These authors videotaped motherinfant dyads and the affective regulation was studied through the microanalysis of 3 minutes face to face interaction and 5 minutes free play.
On arrival at the laboratory the mother and child were taken to a waiting room. The mother was given a card on which was written brief instructions about the sequence of interaction episodes, the cues which would signal separation, and the instruction that she would engage in play with the child making use of the toys as she would do at home. After a few minutes, the mother and child were taken to an adjacent playroom where the observation session was planned to take place. At the end of the first 8 minutes mother-child interaction episode (M-C1) a white undergraduate female stranger (20 years old) entered the room, introduced herself and sat on the floor near to the mother and child and started talking to the mother about a set of everyday issues (e.g., how they had arrived at the laboratory). One minute later the stranger approached and initiated play with the child. After 2 minutes, a cue-light signaled to the mother that as previously instructed she should tell the child that she was going to leave the room to talk to the researcher. The mother left the child with the stranger. The stranger had continued to play with the child for a further 2 minutes (S-C). At the end of this period the mother re-entered the room, she was re-united with the child and after 2 minutes the stranger left the room. Mother and child interacted for a further six minutes (M-C2). The same stranger interacted with all mother-child dyads and she was unaware of the aim of the study as well as of the health condition of each child.
II.3 Coding the social interactions
The micro analytical procedure is suitable for sampling short periods of time as indicated by similar methodological designs. Short periods of time have been shown to provide a good representation of the dyadic interaction despite the level of child developmental functioning (Mahoney et al., 2007). In addition, this procedure has been used extensively in the study of mother-child interaction (Duhalde et al., 2011; Mahoney et al., 2007; Raznoszczyk de Schejtman et al., 2005). Likewise the final 3 minutes of each of the two mother-child episodes and the 2 minutes of the stranger-child episode were examined. In the case of the mother-child episodes, it was assumed that the child would have adapted to the novel situation by the last 3 minutes.
The three adult-child episodes were divided into 15 second consecutive intervals in which the last behavior (of the adult or child) was recorded. For example, in the case of the mother's behavior the observer would rewind the tape to determine the antecedent behavior of the child and this was recorded on the mother's matrix. The tape was further rewound to determine the mother's antecedent behavior and this was recorded on the child's matrix. This was undertaken for the sequence of interactions that occurred during the episode. Data were placed in a response class matrix. Thirteen dependent measures were derived from the coding matrices. They were used to describe the contingent interactions between mother and child. These categories were: mother interacts, mother questions, mother praises, mother directs, mother responds to interaction, mother facilitates play, mother controls play, child responds to interaction, child responds to question, child compliant, child interacts, child plays independently. For the stranger-child episodes fewer categories were required to describe the stranger-child interaction. These categories were: stranger interacts, stranger questions, stranger responds to interaction, stranger facilitates play, child responds to interaction, child responds to question, child interacts, child plays independently.
II.4 Reliability
Videotaped observations were coded by two raters using videos from the pilot study. Each was psychologist taking masters' degree in developmental psychology. Coders were trained on this system for approximately 12 hours until they had attained interrater agreement of at least 80% on each category of the matrices (mother-child and stranger-child interaction). Percentage of agreement between coders for each category was calculated on a sample of 30% of cases. Mean intercoder reliabilities [number of agreements/number of agreements + number of disagreements)] exceeded 80% for all categories (M= 84%, range = 82% and 90%).
III. Results
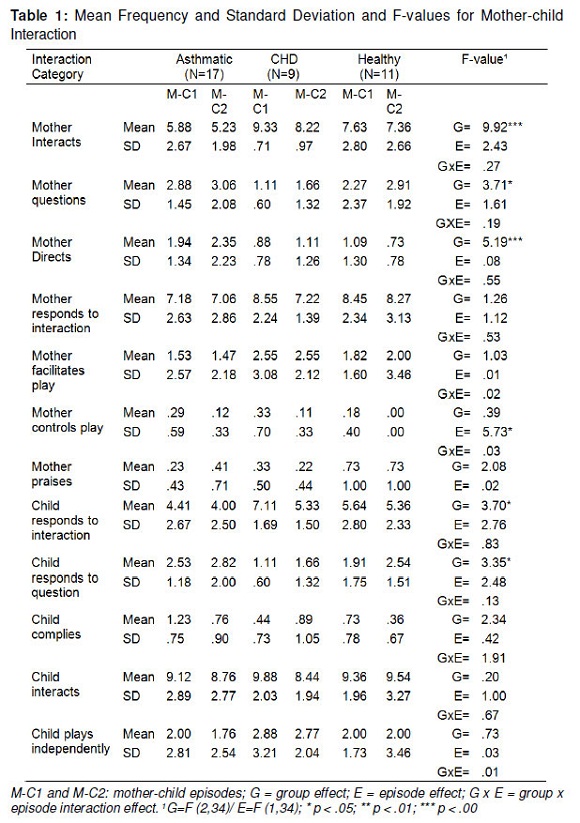
Analyses of the frequencies of interaction categories were undertaken separately for mother-child and stranger-child episodes. This was done because some interaction categories did not occur during the stranger-child episodes and the duration of the coding period for mother-child and stranger-child episodes differed.To examine the overall effects of health condition on interaction categories a multivariate analysis was performed on groups: asthmatic, congenital heart disease (CHD), and healthy using separate total scores of mother's categories and total score of children's categories during the two mother-child interaction episodes. The analysis revealed that there was a reliable group effect for the total score of mother's categories (F (2,36) = 4.39, p < .02), but no difference for children's total score. Mothers total score was higher for the healthy (p < .04) and CHD (p < .06) groups than for the asthmatic (Healthy group: Mean = 44.18; CHD group: M = 44.22; Asthmatic group: M = 39.64). Mothers of asthmatic children interacted less with the child compared to mothers of children in the CHD and healthy groups. In order to examine the effect of health condition on each response category a MANOVA (3 x 2) was performed on health condition group (asthmatic, CHD, healthy) with mother-child episodes as the repeated measure for each interaction category. Appropriate Tukey/Kramer-TK tests were used for post hoc comparisons.
There were significant main effects for health condition group for the categories: mother interacts and mother directs (F (2, 34) = 9.92, p < .001; F (2, 34) = 5.19, p < .01, respectively). For both categories there was no statistical interaction with episode. During both episodes mothers of the asthmatic children interacted reliably less with the child and engaged in more direction of the child compared to the mothers of the heart disease group (p < .01 for both categories) and mothers of the healthy group (p < .01 for both categories; mother interacts: asthmatic: M = 5.55; heart disease: M = 8.77; healthy: M = 7.49; mother directs: asthmatic: M = 2.15; heart disease: M = 1.00; healthy: M = .91). A main effect was also revealed for the mother questions category (F (2, 34) = 3.71, p < .03), but no statistical interaction with episode. During both episodes mothers of the heart disease group were reliably less likely to ask questions to the child compared to mothers of the asthmatic (p < .01) and healthy children (p < .01). Finally, for the mother controls play category there was a reliable effect for episode (F (1, 34) = 5.73, p < .02). For all groups mothers controlled play significantly more during the first compared to the second episode indicating a greater amount of initial maternal supervision.
The analysis of child response categories revealed main effects for group for categories: child responds to interaction (F (2, 34) = 3.70, p < .03) and the child responds to question categories (F (2, 34) = 3.35, p < .04). For both categories there was no statistical interaction with episode. For the category: child responds to interaction, the asthmatic group responded reliably less to interaction compared to the heart disease (p < .01) and healthy children (p < .01; means: asthmatic: M = 4.20; heart disease: M = 6.22; healthy: M = 5.50). For child responds to question, the heart disease group responded significantly less to the mother's questions compared to the asthmatic group (p < .05).
To examine the overall effect of health condition on the stranger-child interaction a multivariate analysis was performed on groups (asthmatic, CHD and healthy) using total scores of stranger categories and total scores of children's categories during the child-stranger episode. The analysis revealed no reliable group effect for either stranger or child categories. One-way analyses of variance performed for groups on each interaction categories revealed no reliable effects for health condition group. In summary, the frequency of interaction measures obtained during the stranger-child episode did not differ for the three groups.
VI. Discussion
Caring for a child with a chronic illness presents a host of challenges for mothers. It was expected that the burden of a chronic disease will lead to less adaptive mother-child interactions when compared with a healthy group. In some way this hypothesis was supported by the empirical findings. However, there were important differences in the chronic illness groups. In addition, the interactional patterns of the asthmatic group appeared circumscribed to their interactions with the mother by comparing mother-child and stranger-child interactions.
Mothers of asthmatic children engaged in significantly less spontaneous interaction with their child compared with mothers of children with chronic heart disease and mothers of healthy children. Furthermore, the asthmatic children revealed a reliably lower level of response to mother-initiated interaction compared with the CHD or healthy groups. These results support Mäntymaa et al. (2003) finding of a lower level of mutual interaction between mothers and their asthmatic child. The mother-child interaction appeared to be less responsive and this may have implications for the manner in which mothers handle issues of autonomy and dependence in relation to the asthmatic child (Kreisler, 1976/1992; Madrid, 2006; Nagano et al., 2010; Peçanha & Lacharité, 2007).
In general, mothers of infants with special needs have been described in the literature as less responsive and more directive in their interaction with the child (Mahoney et al., 2006). The present results confirmed this for the asthmatic group but not for the heart disease group when compared to the healthy group. It is not evident to what extent this pattern is in response to the lower levels of interaction by the mothers or a characteristic of those asthmatic children. However, the fact that there were no differences between the asthmatic, CHD and healthy children in their interaction with the stranger indicates some specific features of the dynamics of asthmatic child-mother dyads. Alternatively, the results may lend credence to the lead-role of the mother's interactive behavior for the asthmatic group. By contrast, the pattern of stranger-child interaction was quite similar for the three groups. The absence of differences among the groups for the stranger-child episode does not support the view that infants with special needs (e.g., medically compromised) tend to be socially less responsive and initiating compared to their healthier peers (Mahoney et al., 2006).
The present study showed that the asthmatic children but not the chronic heart disease children revealed less responsiveness in interaction involving the mother but not with the stranger. This finding indicates that some interactional patterns may be circumscribed to the mother-child interaction. Alternatively, the failure to find differences in interaction with the stranger across the three groups may be explained by the brevity of the interaction episode and by the children´s age (Kreisler, Fain & Soulé, 1987; Nagano et al., 2010).
This study also found that mothers of the asthmatic group were significantly more directive of their child (commands, imperatives and directions) compared to mothers of the CHD and the healthy groups. Maternal intrusiveness and regulation have been shown to distinguish mothers of asthmatic from mothers of healthy children (Kreisler, 1976/1992; Nagano et al., 2010), and may be linked to the finding that mothers of asthmatic tended to adopt a more critical attitude towards the child (Fiese et al., 2008; Hermanns et al., 1989; Madrid, 2006). The results revealed that there were specific characteristics of the mother-child interaction for the asthmatic group which cannot be attributed solely to the long standing medical condition, but must in part represent a psychological aspect of childhood asthma. The findings also highlighted inconsistency in maternal behavior towards the asthmatic child in terms of less interaction (Mäntymaa et al., 2003) and greater child direction (Nagano et al., 2010; Kreisler, 1976/1992). The lower occurrence of interaction for the asthmatic group may indicate that interactions were generally less successful. The didactic pattern of the mothers of the asthmatic children during play may be in response to the difficulties encountered when engaging in social interaction. Mothers of the asthmatic group may be driven to adopt a more pragmatic interactional pattern because of these difficulties. The mother was predominantly directive in her social interactions with the child, who in turn tended to be reactive to her directions leaving little scope for the emergence of a more responsive interactive engagement. With respect to the greater 'directiveness' showed in this study by mothers of asthmatic children, the failure to find reliable differences between both the heart disease condition and healthy groups suggests that this characteristic may be specific to the asthmatic mother-child social interaction.
In summary, the present paper indicates that although the presence of a chronic illness may be an important stressor, this alone does not account for the differences in mother-child interaction among the groups (Klinnert et al., 2008; Wolf et al., 2008). There was a more adverse effect on the interactional pattern for the asthmatic child-mother dyads compared to the CHD child-mother social interaction. This may suggest that there are specific characteristics of asthmatic illness itself or factors circumscribed to the mother-child social interactional pattern associated with this illness (Klinnert et al., 2001; Madrid, 2006; Mrazek & Klinnert, 1996; Nagano et al., 2010; Peçanha & Lacharité, 2007). Although asthma and CHD represent chronic long standing childhood illnesses there remains the issue of how these medical conditions are perceived by caregivers with regard to their psychosomatic characteristics, and the extent to which these factors may influence the mother's responsiveness towards the child. Asthmatic episodes may be perceived by the mother as more psychologically-based, and unpredictable, whereas, the heart disease may be perceived by parents as falling into the more conventional pattern of physical illness.
In this study the analyses were limited to mother-child pairs although chronic illness affects everyone in the family. It was adopted this strategy (mother-child and stranger-child interactions) for controlling the number of observations. Noteworthy is that the relatively small size of the sample was similar to others studies using videotaped mother-infant dyads as well as the microanalysis of some minutes face to face interaction (Duhalde et al., 2011; Raznoszczyk de Schejtman et al., 2005). In addition, this investigation relied on a single laboratory observation at one point in time, therefore causality cannot be inferred from these results. Future research with longitudinal datasets and larger samples would provide more conclusive results. Nonetheless, despite these limitations the evidenced path from mother-child and stranger-child interaction through chronic and healthy conditions held for both emotional factors in the asthmatic disease and the importance of clinical interventions to promote children's development by engaging mother-child in highly responsive interactions.
References
Adams, J., & Weakliem, D. L. (2011). August B. Hollingshead's "Four Factor Index of Social Status": From unpublished paper to citation classic. Yale Journal of Sociology, 8, 11-20. [ Links ]
Ainsworth, M. D. S., Blehar, M. C. Waters, E., & Wall, S. (1978). Patterns of attachment: a psychological study of the Strange Situation. Hillsdale, NJ: Erlbaum. [ Links ]
Chen, E., & Matthews, K. A. (2001). Cognitive appraisal biases: an approach to understanding the relation between socioeconomic status and cardiovascular reactivity in children. Annals of Behavioral Medicine, 23 (2), 101-111. [ Links ]
Cloutier, M. (2008). Considerations in culturally directed asthma disease management programs. Disease Management & Health Outcomes, 16 (2), 95-105. [ Links ]
Crespo, N. C., Ayala, G. X., Vercammen-Grandjean, C. D., Slymen, D., & Elder, J. P. (2011). Socio-demographic disparities of childhood asthma. Journal of Child Health Care, 15 (4), 358-369. Retrieved in November 19, 2011, from: http://chc.sagepub.com/content/early/2011/08/09/1367493510397680. [ Links ]
Debray, R. (2008). La psychosomatique du bebe. Paris, FR: Press Universitaires de France. [ Links ]
Duhalde, C., Tkach, C.; Esteve, M.J., Huerin, V., & R. de Schejtman, C. (2011). El jugar en la relación madre-hijo y los procesos de simbolización en la infancia. Anuario de investigaciones, 18, 239-246. [ Links ]
Eid, L., Heim, K., Doucette, S., McCloskey, S., Duffy, A., & Grof, P. (2013). Bipolar disorder and socioeconomic status: what is the nature of this relationship? International Journal of Bipolar Disorders, 1 (9). Retrieved in August 10, 2013, from http://www.journalbipolardisorders.com/content/1/1/9 [ Links ]
Faffe, D. S. (2008). Asthma: where is it going? Brazilian Journal of Medical and Biological Research, 41 (9), 739-749. Retrieved in September 4, 2010, from http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0100879X2008000900001&lng=en&nrm=iso. [ Links ]
Fiese, B., Winter, M., Anbar, R., Howell, K., & Poltrock, S. (2008). Family climate of routine asthma care: associating perceived burden and motherchild interaction patterns to child well-being. Family Process, 47 (1), 63-79. [ Links ]
Garro, A. (2011). Health-related quality of life (HRQOL) in latino families experiencing pediatric asthma. Journal of Child Health Care. 15 (4) 350-357. Retrieved in October 31, 2011 from http://chc.sagepub.com/content/15/4/ 350.full.pdf+html. [ Links ]
Guerra, S., & Martinez, F. D. (2008). Asthma genetics: from linear to multifactorial approaches. Annual Review of Medicine, 59, 327-341. [ Links ]
Gustafsson, P. A., Kjellman, N. -I. M., & Björkstén, B. (2002). Family interaction and a supportive social network as salutogenic factors in childhood atopic illness. Pediatric Allergy and Immunology, 13 (1), 51-57. [ Links ]
Hermanns, J., Florin, I., Dietrich, M., Rieger, C., & Hahlweg, K. (1989). Maternal criticism, mother-child interaction, and bronchial asthma. Journal of Psychosomatic Research, 33, 469-476. [ Links ]
Hoffman, J. (2005). Essential cardiology: principles and practice (pp. 393).Totowa, NJ: Humana Press. [ Links ]
Hollingshead, A. B. (1975). Four factor index of social status. Department of Sociology, Yale University. New Haven, CT. [ Links ]
Keller, H. R. (2003). The behavioral observation approche to personality assessement. In H. M. Knoff (Ed), The assessment of child and adolescent personality (pp. 353-397). New York, USA: The Guilford Press. [ Links ]
Klinnert, M. D, Nelson, H. S, Price M. R., Adinoff, A. D., Leung, D. Y. M., & Mrazek, D. A. (2001). Onset and persistence of childhood asthma: predictors from infancy. American Academy of Pediatrics, 108 (4), e.69. [ Links ]
Klinnert, M. D., Kaugars, A. S., Strand, M., & Silveira, L. (2008). Family psychological factors in relation to children's asthma status and behavioral adjustment at age 4. Family Process, 47 (1) 41-61. [ Links ]
Kreisler, L., Fain, M., & Soulé, M. (1987). L'enfant et son corps. Paris, FR: Press Universitaires de France. [ Links ]
Kreisler, L. (1992). La psychossomatique de l'enfant (4a revised ed.). Paris, FR: Press Universitaires de France (Original published in 1976). [ Links ]
Laing, S., McMahon, C., Ungerer J., Taylor, A., Badawi, N., & Spence, K. (2010). Mother-child interaction and child developmental capacities in toddlers with major birth defects requiring newborn surgery. Early Human Development, 86, 793-800. [ Links ]
Madrid, A., & Schwartz, M. (1991). Maternal-infant bonding and pediatric asthma: an initial investigation. Pre-and Peri-Natal Psychology, 5, 347-358. [ Links ]
Madrid A. (2006). Helping children with asthma by repairing maternal-infant bonding problems. American Journal of Clinical Hypnosis, 48 (2-3), 199-211. [ Links ]
Mahoney, G., Perales, F., Wiggers, B., & Herman, B. (2006). Responsive teaching: early intervention for children with Down syndrome and other disabilities. Down Syndrome Research and Practice, 11 (1), 18-28. Retrieved in August 16, 2013, from http://www.down-syndrome.org/perspectives/311/ [ Links ]
Mahoney, G., Kim, J.M., & Lin, C.S. (2007). Pivotal behavior model of developmental learning. Infants & Young Children, 20 (4), 311-325. [ Links ]
Mäntymaa, M., Puura, K., Luoma, I., Salmelin, R., Davis, H., Tsiantis, J., Ispanovic-Radojkovic, V., Paradisiotou, A., & Tamminen, T. (2003). Infant-mother interaction as a predictor of child's chronic health problems. Child: Care, Health, and Development, 29, 181-191. [ Links ]
Marino, B.S., Uzark, K., Ittenbach, R., & Drotar, D. (2010). Evaluation of quality of life in children with heart disease. Progress in Pediatric Cardiology, 29 (2), 131-138. [ Links ]
Minuchin, S., Baker, L., Rosman, B. L., Liebman, R., Milman, L., Thomas, L., & Todd, T. C. (1975). A conceptual model of psychosomatic illness in children: family organization and family therapy. Archives of General Psychiatry, 32, 1031-1038. [ Links ]
Mrazek, D. A., & Klinnert, M. (1996). Emotional stressors and the onset of asthma. In C. R. Pfeffer (Org.), Severe stress and mental disturbance in children (pp.211-224).Washington: American Psychiatric Press. [ Links ]
Nagano, J., Kakuta, C., Motomura, C., Odajima ,H., Sudo, N., Nishima, S., & Kubo, C. (2010). The parenting attitudes and the stress of mothers predict the asthmatic severity of their children: a prospective study. BioPsychoSocial Medicine, 4 (12), 1-10. [ Links ]
Nogueira, K. T., & Lopes, C. S. (2010). Associação entre transtornos mentais comuns e qualidade de vida em adolescentes asmáticos. Revista Brasileira de Epidemiologia,13 (3), 476-486, Retrieved in July 6, 2012, from http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1415790X2010000300011&lng=en&nrm=iso [ Links ]
Peçanha, D. L., Pérez-Ramos, A. M. Q., & Lacharité, C. (2003). Une méthode systémique d´évaluation du fonctionnement familial: étude portant sur les familles des enfants asthmatiques. Revue Québécoise de Psychologie, 24 (2), 89-112. [ Links ]
Peçanha, D. L., & Lacharité, C. (2007).The systemic family assessment system: its validity with asthmatic children and their families. Psicologia em Estudo, 12 (3),503-512. Retrieved in May 2, 2011, from http://www.scielo.br /scielo.php?script=sci_arttext&pid=S1413-73722007000300007&lng= en&nrm=iso. [ Links ]
Peçanha, D. L. A criança com asma e sua família: avaliação psicossomática e sistêmica. São Carlos: EdUFSCar/FAPESP (in press). [ Links ]
Raznoszcyk de Schejtman, C.; Lapidus, A.; Vardy, I.; Leonardelli, E., Silver, R., Umansky, E., Mindez, S., Duhalde, C., Huerin, V., Mrahad, M.C., & Zucchi, A. (2005). Estudio de la expresividad emocional y la regulación afectiva en díadas madre-bebé durante el primer año de vida y su relación con la autoestima materna. Anuario de investigaciones, 12, 327-336. [ Links ]
Rosa, R. F. M., Zen, P. R. G., Graziadio, C., & Paskulin, G. A. (2011). Síndrome de deleção 22q11.2 e cardiopatias congênitas. Revista Paulista de Pediatria, 29 (2), 251-260. Retrieved in November 23, 2011 from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-05822011000200018& lng=en&nrm=iso [ Links ]
Salomão Júnior, J.B., Miyazaki, M.C.O.S., Cordeiro, J.A., Domingos, N.A.M., & Valerio, N.I. (2008). Asma, competência social e transtornos comportamentais em crianças e adolescentes. Estudos de Psicologia, 25 (2), 185-192. Retrieved in September 4, 2010 from http://www.scielo.br/scielo.php?pid=S0103166X2008000200003&script=sci_abstract&tlng=es. [ Links ]
Stewart, M., Masuda, J.R., Letourneau, N., Anderson, S., & Mc Ghan, S. (2011). "I want to meet other kids like me": support needs of children with asthma and allergies. Issues in Comprehensive Pediatric Nursing, 34, 62-78. [ Links ]
Szwec, G. (1993). L'enfant asthmatique. Paris, FR: Press Universitaires de France. [ Links ]
WHO - World Health Organization (2011). Asthma. Fact Sheet nº 307. Geneva. Retrieved in October 20, 2011 from http://www.who.int/topics/asthma/en [ Links ]
Wolf, J., Miller, G., & Chen, E. (2008). Parent psychological states predict changes in inflammatory markers in children with asthma and healthy children. Brain, Behavior, and Immunity, 22 (4), 433-441. [ Links ]
Recebido: 29/01/2015 / Corrigido: 18/02/2015 / Aceito: 02/03/2015.
1 Academy Award for her Thesis by the Sao Paulo Academy of Psychology (APP), Psychologist, PhD in Clinical Psychology, Professor in the Department of Psychology - Federal University of São Carlos- UFSCar. Contact: Alameda das Crisandálias, 616/32 - Cidade Jardim - CEP 13566-570, São Carlos, São Paulo, Brasil. E-mail: doris@ufscar.br
2 Director of the Psychology Institute of the Federal University of Rio Grande do Sul (UFRGS), Psychologist, PhD in Psychology from the University of London, CNPq Researcher, Professor (UFRGS). Contact: Institute of Psychology - UFRGS, Ramiro Barcelos 2600/111, Porto Alegre, CEP 90035-003, Rio Grande do Sul, Brasil. Phone: (51) 33165066, Fax: (51) 33309507. E-mail: piccinini@portoweb.com.br
3 PhD Emeritus Professor of Psychology. London Metropolitan University, Faculty of Life Sciences and Computing 166-220 Holloway Road, London N7 8DB.

