










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.19 no.2 São Paulo ago. 2017
http://dx.doi.org/10.5935/1980-6906/psicologia.v19n2p161-173
ARTICLES
HUMAN DEVELOPMENT
Childhood cancer: diagnosis impact analysis
Fernanda Rosalem CapriniI; Alessandra Brunoro MottaII
IFederal University of Espírito Santo, Vitória, ES, Brazil
IIFederal University of Espírito Santo, Vitória, ES, Brazil
ABSTRACT
A cancer diagnosis significantly impacts both patients and their families, as potential stressors place them in a vulnerable condition. In order to analyze the psychosocial impact of a cancer diagnosis, this study included 12 children aged between 6 and 12 years old (M = 8.75, SD = 2.05) and their respective caregivers in a hospital located in Grande Vitória, in the State of Espírito Santo, in Brazil. Coping with hospitalization (Coping with Hospitalization Scale) and psychosocial risk (Psychosocial Assessment Tool/PAT) were assessed. Socio-demographic and clinical data were obtained through medical records. Data were submitted to descriptive statistical analysis. The psychosocial risk of families was at the clinical level. Regarding the need of coping, adaptive strategies were found, such as distraction and social support, as well as less adaptive strategies, such as brooding. This study contributes to the field of coping among children and indicates potential sources of psychological intervention.
Keywords: coping; childhood cancer; psycho-oncology; psychosocial risk; pediatric psychology.
The moment a child's cancer diagnosis is disclosed, it is described as a time in which the family and child feel extremely threatened and have difficulty dealing with the diagnosis (Kohlsdorf & Costa Junior, 2012). The diagnosis is only the first stage of a process that may include various phases: beginning of treatment, remission, end of medical treatment, survival, cure, relapse, terminal phase, death and family adjustment after the patient dies, if that is the case (Katz, Dolgin, & Varni, 1990).
During the diagnosis phase of childhood cancer, both patients and families experience stress and psychological suffering (Hildenbrand, Clawson, Alderfer, & Marsac, 2011; MacLaren & Cohen, 2005; Pai et al., 2008). Such psychological responses may be worsened by stressors arising from the disease and treatment, such as the need to be away from a familiar environment, as the hospital is where diagnosis processes take place and treatment is initiated (Kohlsdorf & Costa Junior, 2012; Silva & Cabral, 2015). Thus, diagnosis disclosure is characterized as a time in which early psychological intervention is necessary so the family can provide important support to the child (Hildenbrand et al., 2011).
Situations that characterize the treatment of childhood cancer also involve the family and its respective affective, social, and economic variables. Cancer treatment is a condition of psychosocial risk for both patient and family (Rech, Silva, & Lopes, 2013). This psychosocial risk, added to the disease's biological risk, makes this population vulnerable to the challenges imposed by the disease and treatment (Kazak et al., 2011).
In light of this, the related literature has indicated priorities in the field regarding the family, highlighting the need to identify families at risk at the time of diagnosis (Kazak et al., 2011). One of the reasons these families need to be identified is that family functioning during diagnosis disclosure is a predictor of later adjustment; i.e., families facing a greater difficulty during diagnosis who present high levels of anxiety, for instance, will continue to experience high levels of psychological suffering even after treatment is concluded (Patenaude & Kupst, 2005).
Studies have sought to meet this priority, especially those using the Psychosocial Assessment Tool (PAT), to assess families' psychosocial risk in the situation of childhood cancer (Kazak et al., 2011; Pai et al., 2008). Findings have shown that families, in general, share suffering and distress when facing cancer, but are able to deal with the challenges and threats imposed by such a diagnosis. There are, however, families who experience higher levels of psychosocial risk, demanding early interventions appropriate to their needs (Kazak et al., 2011).
Given the preceding discussion, a cancer diagnosis impacts the lives of children and families in a way psychosocial characteristics play either the role of risk or protective factors, affecting the use of coping strategies. At this point, coping strategies emerge as a significant variable to understand the phenomenon more deeply. From a developmental perspective, which defines coping as a regulatory process under stress, this study is based on the Motivational Theory of Coping (MTC). According to the MTC, coping strategies are triggered when stressors are perceived by children as a challenge to be overcome or a threat to their psychological needs concerning relationships, autonomy, or competence (Skinner & Zimmer-Gembeck, 2007; Ramos, Enumo, & Paula, 2015).
These strategies may vary in a situation of childhood cancer depending on the phase of treatment (Levy, Kronenberger, & Carter, 2008). Hence, the way a child copes with the disease in each phase of the disease or treatment will affect his/her ability to cope during later phases, making evident the relevance of early interventions in the diagnosis phase to facilitate coping in the subsequent phases, promoting better adaptation in the future (Kusch, Labouvie, Ladisch, Fleischhack, & Bode, 2000).
Studies investigating coping strategies among children with cancer during different phases of treatment verified that distraction and rumination are the coping strategies most frequently reported by children (Hostert, Motta, & Enumo, 2015). There is a gap in the Brazilian literature specifically concerning studies conducted in the period immediately after diagnosis; i.e., there are no studies seeking to understand coping among children during this phase of the process.
Therefore, this study is justified based on its objective to analyze family psychosocial risk and coping strategies of children recently diagnosed with cancer. This longitudinal study is part of a larger longitudinal project conducted during a Master's Degree program and the cross-section presented here refers to the impact of a diagnosis of child cancer.
Method
Participants
Twelve children, both female (58.3%) and male (41.7%), aged between 6-12 years old (M = 8.75; SD = 2.05), diagnosed with cancer in the hematology and oncology service of a public child hospital located in Vitória, ES, Brazil, took part in this study. The children's parents or legal guardians also participated as informants.
The participants composed a convenience sample, selected according to the following inclusion criteria: (a) having received a diagnosis of cancer a month (30 days) ago, at most; and (b) being 6 to 12 years old, at most, considering the need to understand the instruments employed in the study. Children whose diagnosis referred to a relapse, were in the intensive care unit, or were admitted to the hospital in severe condition, were excluded.
Instruments
The Psychosocial Assessment Tool - PAT (Pai et al., 2008), instrument translated to and validated for Portuguese in Brazil by Santos (2012) to assess family psychosocial risk. PAT is composed of seven subscales addressing domains of psychosocial risk, namely: family structure and resources, social support, family problems, response to stress, family beliefs, problems with children, and problems with siblings. These dimensions capture characteristics and functioning patterns that put the families of children with chronic diseases at a psychosocial risk (Pai et al., 2008). The answers to the items of the subscales are of two types: yes/no answers and answers provided through a Likert scale. Each item of the scale is dichotomous, that is, indicates risk or no risk. The total score ranges from 0 to 7 points and the analysis of this score enables classifying the family's psychosocial risk into three categories: (a) Universal, characterized as mild risk, the score of which is less than 1; (b) Target, moderate risk with a total score equal to or greater than 1 and less than 2 (> 1 and < 2); and (c) Clinical, that is, high risk with a total score equal to or greater than 2 (> 2). The instrument's internal consistency is strong (α = 0.81) and test-retest indexes are appropriate (r = 0.78 - 0.87, p < .001), indicating significant correlations for mothers and fathers. PAT 2.0 is answered by one of the parents or legal guardians and its application takes 18 minutes, on average (Pai et al., 2008).
The Instrumento de Avaliação das Estratégias de Enfrentamento da Hospitalização (AEH) [Assessment of Hospitalization Coping Strategies] was developed by Motta (2001, 2007). This instrument is used to assess coping among hospitalized children aged between 6-12 years old. Either a computer or printed version can be used. A bound, printed version was used in this study. In both formats, the AEH is composed of a version directed to boys and another directed to girls, with 20 boards presenting images that represent coping behaviors: playing, watching TV, singing and dancing, praying, studying, talking, listening to music, reading comic books, taking medication, seeking information, crying, becoming angry, hiding, becoming sad, feeling discouraged, making a tantrum, thinking about running away, feeling guilty, being scared, and hoping for a miracle. When each of these boards is presented, the child reports how frequently she/he adopts these behaviors during hospitalization, classifying their occurrence on a Likert scale that ranges from 0 (never) to 4 (always). The children justified responses to each behavior, which enabled classifying coping strategies according to the macro-categories proposed by Ellen Skinner and colleagues (Skinner & Zimmer-Gembeck 2007; Skinner, Edge, Altman, & Sherwood, 2003) and according to the Motivational Theory of Coping (MTC), namely: self-reliance, support seeking, problem-solving capacity, information search, accommodation, negotiation, delegation, isolation, helplessness, escape, submission, and opposition. The 12 coping macro-categories may include a range of coping strategies (Skinner et al., 2003). Hence, examples of strategies can be described in the set of adaptive coping macro-categories, such as "accommodation": distraction, cognitive restructuring, minimization, and acceptance; "self-reliance": emotional regulation, behavioral regulation, and emotional expression; "support seeking": search for contact, search for comfort, and instrumental help; "problem-solving": planning strategies and instrumental action; "information seeking": reading and asking other people; and "negotiation": bargaining and establishing priorities. In turn, the set of maladaptive coping macro-categories contains the following: "delegation" includes complaining, self-blame, and lamentation; "isolation" includes social withdrawal, avoiding others, and becoming paralyzed; "helplessness" includes confusion, cognitive exhaustion and passivity; "escape" includes behavioral avoidance, mental withdrawal, and wishful thinking; "submission" includes rumination, intrusive thinking, rigid persistence; and "opposition" includes blaming others and aggression.
Procedures
Data were collected during the period in which each child was diagnosed; a period of up to a month (30 days) after the diagnosis was established. Data were collected between March and November 2013. After the children who met the criteria to participate in the study were identified, their families were contacted and received clarification regarding the study's objectives. The anonymity of their children's identities was ensured, and they were informed their children's wellbeing would be taken into account, and that their participation was voluntary. Data collection was initiated only after the participation of children was authorized. The children were also informed about the study and signed free and informed consent forms. After both parents and children consented to participate, the instruments were applied to the children's caregivers (PAT) and children (AEH). The study was initiated after approval was provided by the Institutional Review Board in accordance with Regulation No. 196/96, National Health Council - CONEP - National Committee for Ethics in Research - Ministry of Health, CAAE Nº 112580112.5.0000.5542.
The instruments were applied individually with each child by the researcher on the hospital premises (nursing ward or outpatient). The researcher initially applied the PAT to mother, father or other caregiver, such as grandparents, and then the children were approached for the application of the AEH. Note that caregivers did not witness the application of the instrument to the children, nor did the children witness the collection of data concerning psychosocial risk. The application of the instruments took 60 minutes, on average.
Data collected through the instruments (PAT and AEH) were processed and analyzed according to guidance provided in the manuals, standards and/or based on the authors' recommendations. Hospitalization stressors, measured by the AEH, were analyzed according to content analysis. Afterwards, data collected with the aid of all the instruments, together with clinical data, were analyzed using descriptive analysis, calculating frequency, proportion, means, medians and standard deviation.
Results
Data Concerning Assessment of Family Psychosocial Risk
Analysis of the PAT's social score enabled verifying that more than half of the families presented psychosocial risk factors at a clinical level (58.3%), 25% at a target level, and only 16.7% were classified as being at universal level of risk.
A detailed analysis of factors that generated the classification of risk showed that, in the period of recent diagnosis, "Family Problems" (M = 0.50) and "Problems with the child" (M = 0.50) represented contexts that put families of children with cancer in a situation of greater vulnerability. On the other hand, "Family beliefs" regarding the disease (M = 0.03), and "Social Support" (M = 0.11) presented lower means, representing a lower risk for families at the time of diagnosis. Table 1 shows the results found for each of the subscales:
Data Concerning Assessment of Coping among Children with Cancer
The AEH enabled verifying that the stressors most frequently reported in the context of hospitalization were invasive medical procedures (n = 9), as the following the report shows: "the worst here at the hospital is taking blood samples" (girl, 6 years old). In smaller proportions, the following stressors were reported: oral medication (n = 2); body changes (n = 1), and food restrictions (n = 1).
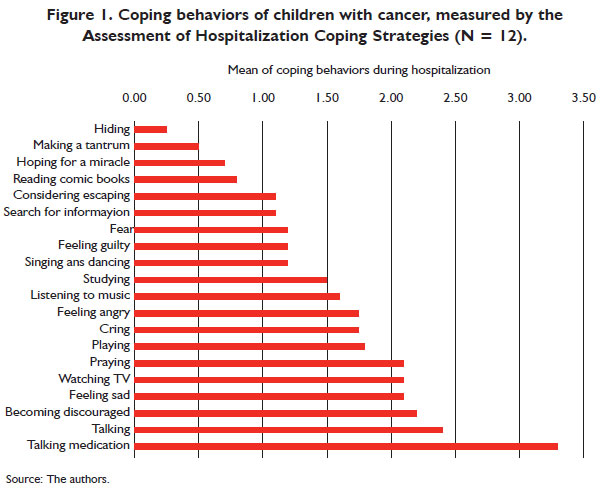
The assessment of coping behaviors showed a prevalence of the following behaviors: taking medication (M = 3.3), talking (M = 2.4), becoming discouraged (M = 2.2), becoming sad, watching TV, and praying (M = 2.1). On the other hand, the behaviors less frequently reported were making a tantrum (M = 0.5) and hiding (M = 0.2) (Figure 1).
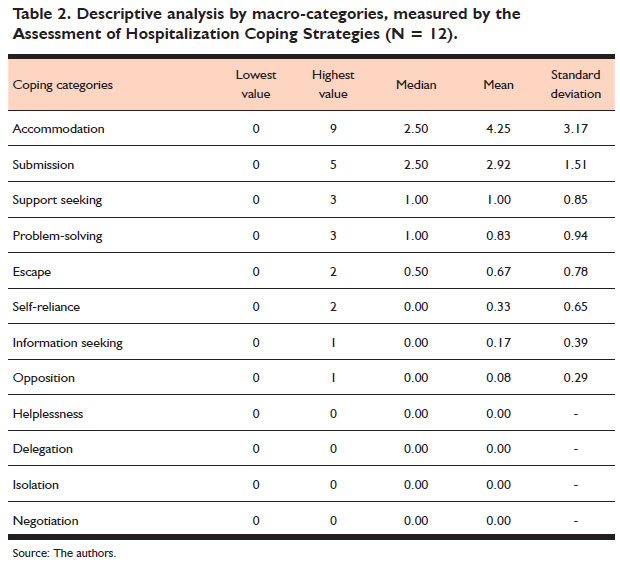
Table 2 presents the coping macro-categories that emerged from an analysis of strategies reported in the justification of children for coping behaviors. In regard to coping strategies measured by AEH, the highest means were obtained for the strategies classified in the macro-categories "accommodation" (M = 4.25; SD = 3.17) and "submission" (M = 2.92; SD = 1.51).
The children's reports revealed the following coping strategies in the macro-category "accommodation": distraction, acceptance, and cognitive restructuring. The report of one of the children regarding watching TV and playing represents the functionality of the distraction strategy: "I always watch TV because I get distracted" and "Because I have fun," respectively (girl, 7 years old).
The macro category "submission" was also evident in the reports, with examples of the rumination strategy, in which the child's focus is on the negative aspects of the stressor. Reports revealed becoming sad and feeling angry, respectively: "I always get sad because it is boring staying here" (girl, 8 years old); and "sometimes because I have to have injections all the time" (girl, 6 years old).
On the other hand, "opposition" (M = 0.08; SD = 0.29), "information seeking" (M = 0.17; SD = 0.39) and "self-reliance" (M = 0.33; SD = 0.65) presented lower means. Note that there are no reports referring to the macro-categories: "helplessness", "delegation", "isolation" and "negotiation" (Table 2).
Discussion
This study's objective was to investigate the impact of a cancer diagnosis on children and their families, intending to better understand one of the phases of cancer treatment with specific demands and of important psychological impact for both children and their families (Katz, Dolgin, & Varni, 1990). We considered that the psychosocial characteristics of the family might be affected by a cancer diagnosis, interfering in the use of coping strategies by children.
In regard to psychosocial risk, most of the sample presented clinical and target levels. This information stood out to the extent it differs from those found in American society, in general (Kazak et al., 2011) and in the study that validated the instrument and was conducted for the Brazilian population (Santos, 2012). The difference found is translated into a more negative psychosocial condition for the sample in this study because the families were in a situation of greater vulnerability in the period of diagnosis, strongly requiring psychosocial support.
Even though the study did not collect information regarding the severity of the children's condition or the stage of the disease, it is known that, when the diagnosis is delayed or the disease is in an advanced stage, the impact of the treatment is greater and chances of a cure are reduced (Zouain-Figueiredo, 2012). This situation characterizes the context under study in which the analysis of 25 years of cancer records indicated that a larger proportion of cases are diagnosed when the disease has already advanced (Zouain-Figueiredo, 2012), which explains a high psychosocial risk in this study's sample, showing that the impact of a late diagnosis is extended to the psychosocial aspects of children and families.
The specific analysis of domains of psychosocial risk indicated responses of prolonged sadness, concerns, and fear, coupled with other problems prior to the diagnosis and specific to each family (e.g., marital conflicts, consumption of alcohol) and to each child (e.g., delayed development, learning problems). These domains presented a greater risk in the study conducted by Santos (2012) and contribute to understanding the period of diagnosis as being a time of important psychological suffering. From a more positive perspective, studies report that suffering becomes less intense after six months of treatment (Kohlsdorf & Costa Júnior, 2012), especially if the need for psychosocial intervention is identified early and incorporated into the treatment process (Kazak et al., 2011).
Once variables from the child's family context were identified (psychosocial risk) during period closely following the diagnosis and then analyzed, we sought to understand coping strategies among hospitalized children. The most frequently reported stressors were invasive medical procedures. International studies report that this stressor is found in broader categories, namely: cancer treatment and side effects (Hildenbrand, et al., 2011) and physical effects (Rodriguez et al., 2012) that include pain and hair loss, among others. The study conducted by Rodriguez et al. (2012) reports that changes in daily life were more frequently reported than invasive medical procedures. These authors note that more than considering cancer as a stressor, it is relevant to identify the subdomains of stressors, which should be measured more than once over the course of treatment since the course of the disease presents shared stressors, though with different intensities and levels of incapacitation (Rodriguez et al., 2012).
In the period closely following a diagnosis, the most frequently reported coping behaviors were: taking medication, talking and becoming discouraged. This information contrasts with that reported in previous studies using AEH in children with cancer (Hostert, Motta, & Enumo, 2015), since becoming discouraged was among the children's most frequent responses. In this study, the focus was on the time of diagnosis, in which responses to suffering, measured in terms of psychosocial risk, are also more frequently presented.
Together with these behaviors and negative feelings (helplessness, sadness, anger, fear and guilt), the children's repertoire of coping strategies included taking medication, talking and watching TV, which were among the most frequently noted.
Taking medication was the most frequently behavior reported by children. In fact, the first month after the diagnosis is a time when the child must be tested to obtain specific clarification of the diagnosis and prognosis, as well as being the time in which medication is initiated. Thus, this agrees with the reports of children that concern taking medication and the routine of hospitals. Therefore, even though taking medication is associated with the invasive medical procedures stressor, children become engaged with pleasant activities, according to the options available in their environment, and favor problem-solving, characterizing a positive adaptive process.
On the other hand, the fact that children watch TV when there is a restriction of movement due to a venous puncture may lead to the employment of coping strategies such as passive distraction (MacLaren & Cohen, 2005). According to the authors, children in a passive condition may become more distracted and suffer less intensively than a child engaged in active distraction. Like watching TV, talking can take place even under restrictive conditions, considering that children always have someone by their side. This person is an adult who is a source of social support, for the most part, the mother.
The coping behaviors described by the children presented functionalities that enabled classifying them in strategies characteristic of the macro-category "accommodation", related to an adaptive outcome and to the macro-category "submission," which is related to a maladaptive outcome (Skinner & Zimmer-Gembeck, 2007; Ramos, Enumo, & Paula, 2015). A treatment's negative effects, as well as imminent painful procedures, may have contributed to the occurrence of emotional responses, such as sadness and fear, measured by the AEH, the justifications of which indicated the presence of rumination and intrusive thinking strategies, which represent the coping macro-category "submission". This information has been found in previous studies employing the AEH, which are unanimous in stating that the presence of these strategies, even in the face of a behavioral repertoire that includes adaptive strategies, indicate the need for interventions over time focused on coping (Hostert, Motta, & Enumo, 2015).
Therefore, on one hand, children considered stressors to be challenging and established actions that tended to be more flexible and active, which led the children to distract themselves, see the positive side of a stressful situation and accept the problem. On the other hand, children also became afraid and may have problems dealing with the resources provided by their context, leading them to maintain a passive and repetitive focus on the negative aspects of a situation, emphasizing harm and losses accruing from stressful events (Skinner et al., 2003).
This study presents a limitation concerning the verification of associations among the variables of interest: family psychosocial risk and children's coping strategies, due to the sample size. Therefore, further studies using larger samples with greater variation in terms of the participants' ages, can test models of relationships among variables and verify developmental differences in the coping strategies of hospitalized children with cancer.
The experience of children with cancer at the time of diagnosis reflects a search for adapting to a situation with an extreme impact. One should consider that the stressors to which children are exposed will continue to affect them and their families for a long period, with the potential to unbalance the relationship between positive and negative coping strategies and increase their psychosocial risk.
This study's findings reinforce the need to assess the psychological characteristics of children and their families at the time a diagnosis is disclosed. The identification of these individuals' psychosocial characteristics can enable the implementation of interventions intended to ensure the healthier development of children despite the adversities presented by cancer. It is believed that the resources of Pediatric Psychology can contribute to changing risk conditions so that the individuals' variables emerge as protective factors. In this way, adaptive results will be observed over time, predicting later psychological adjustments to treatment and during adult life.
References
Hildenbrand, A. K., Clawson, K., Alderfer, M. A., & Marsac, M. L. (2011). Coping with pediatric cancer: Strategies employed by children and their parents to manage cancer-related stressors during treatment. Journal of Pediatric Oncology Nursing, 28(6),344-354. DOI: 10.1177/1043454211430823 [ Links ]
Hostert, P. C. C. P., Motta, A. B., & Enumo, S. F. (2015). Coping da hospitalização em crianças com câncer: A importância da classe hospitalar. Estudos de Psicologia, 32(4),627- 639. Recuperado em 31 Julho, 2017, de http://dx.doi.org/10.1590/0103-166X2015000400006 [ Links ]
Katz, E. R., Dolgin, M. J. & Varni, J. W. (1990). Cancer in children and adolescents. In A. M. Gross & R. S. Drabman (Ed), Hanbook of clinical behavioral pediatrics, (pp. 129-146). New York: Plenum Press. DOI: 10.1007/978-1-4613-0505-7_8 [ Links ]
Kazak, A. E., Barakat, L. P., Hwang, W., Ditaranto, S., Biros, D., Beele,...Reilly, A. (2011). Association of psychosocial risk screening in pediatric cancer with psychosocial services provide. Psycho-Oncology, 20,715-723. DOI: 10.1002/pon.1972 [ Links ]
Kohlsdorf, M. & Costa Junior, A. L. (2012). Impacto psicossocial do câncer pediátrico para pais: Revisão da literatura. Paidéia, 22(51),119-129. Recuperado em 31 Julho, 2017, de http://dx.doi.org/10.1590/S0103-863X2012000100014. [ Links ]
Kusch, M., Labouvie, H., Ladisch, V., Fleischhack, G. & Bode, U. (2000). Structuring psychosocial care in pediatric oncology. Patient Education and Counseling, 40,231-245. Recuperado em 31 Julho, 2017, de http://dx.doi.org/10.1016/S0738-3991(99)00109-3 [ Links ]
Levy, M. C., Kronenberger, W. G. & Carter, B. D. (2008). Brief report: Illness factors and child behavior before and during pediatric hospitalization. Journal of Pediatric Psychology, 33(8),905-909. DOI: 10.1093/jpepsy/jsn039 [ Links ]
MacLaren, J. & Cohen, L.L. (2005). A comparison of distraction strategies for venipuncture distress in children. Journal of Pediatric Psychology, 30,387-396. DOI: 10.1093/jpepsy/jsi062 [ Links ]
Motta, A. B. (2001). Brincar no hospital: Câncer infantil e avaliação do enfrentamento da hospitalização. (Dissertação de Mestrado não publicada). Universidade Federal do Espírito Santo. BR. [ Links ]
Motta, A. B. (2007). Brincando no hospital: Uma proposta de ntervenção psicológica para crianças hospitalizadas com câncer. (tese de doutoramento não publicada). Universidade Federal do Espírito Santo. BR. [ Links ]
Pai A. L., Patiño-Fernández, A. M., McSherry, M., Beele, D., Alderfer, M. A., Reilly, A. T., ... Kazak, A. E. (2008). The Psychosocial Assessment Tool (PAT 2.0): Psychometric properties of a screener for psychosocial distress in families of children newly diagnosed with cancer. Journal of Pediatric Psychology, 33,50-62. DOI: 10.1093/jpepsy/jsm053 [ Links ]
Patenaude, A. F. & Kupst, M. J. (2005). Psychosocial functioning in pediatric cancer. Journal of Pediatric Psychology, 30(1),9-27. DOI: 10.1093/jpepsy/jsi012 [ Links ]
Ramos, F. P., Enumo, S. F., & Paula, K. M. P. (2015). Teoria motivacional do Coping: uma proposta desenvolvimentista de análise do enfrentamento do estresse. Estudos de Psicologia, 32,269-279. Recuperado em 31 Julho, 2017, de http://dx.doi.org/10.1590/0103-166X2015000200011 [ Links ]
Rech, B. C. S., Silva, I. M., & Lopes, R. C. S. (2013). Repercussões do câncer infantil sobre a relação conjugal. Psicologia: Teoria e Pesquisa, 29(3),257-265. Recuperado em 31 Julho, 2017, de http://dx.doi.org/10.1590/S0102-37722013000300003 [ Links ]
Rodriguez, E. M., Dunn, M. J., Zuckerman,T., Vannatta, K., Gerhardt, C. A., & Compas, B. E. (2012). Cancer-related sources of stress for children with cancer and their parents. Journal of Pediatric Psychology 37(2),185-197. DOI: 10.1093/jpepsy/jsr054 [ Links ]
Santos, S. S. (2012). Adaptação transcultural e validação do "Psychosocial Assessment Tool (PAT2.0)": Instrumento de avaliação psicossocial de famílias de pacientes pediátricos recém-diagnosticados com câncer. (dissertação de mestrado não publicada). Fundação Antônio Prudente. BR. [ Links ]
Silva, L. F. & Cabral, I. E. (2015). O resgate do prazer de brincar da criança com câncer no espaço hospitalar. Revista Brasileira de Enfermagem, 68(3),391-397. Recuperado em 31 Julho, 2017, de http://dx.doi.org/10.1590/0034-7167.2015680303i [ Links ]
Skinner, E. A., Edge, K., Altman, J., & Sherwood, H. (2003). Searching for the structure of coping: A review and critique of category systems for classifying ways of coping. Psychological Bulletin, 129,216-269. DOI: 10.1037/0033-2909.129.2.216 [ Links ]
Skinner, E. A. & Zimmer-Gembeck, M. J. (2007).The development of coping. Annual Review of Psychology, 58,119-144. DOI:10.1146/annurev.psych.58.110405.085705 [ Links ]
Zouain-Figueiredo, G. P. (2012). Câncer em crianças e adolescentes no hospital de referência do estado do Espírito Santo: Uma análise de 25 anos. (dissertação de mestrado não publicada). Universidade Federal do Espírito Santo. BR. [ Links ]
Submission: 23.3.2016 Mailling address:
Mailling address:
Fernanda Rosalem Caprini
Av. Fernando Ferrari, 514
Vitória, ES, Brazil, CEP 29060-970
E-mail: fernandacaprini@gmail.com
Acceptance: 20.6.2017


{kind=link}
{kind=link}
{kind=link}