










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.21 no.1 São Paulo jan./abr. 2019
http://dx.doi.org/10.5935/1980-6906/psicologia.v21n1p137-153
ARTICLES
HUMAN DEVELOPMENT
Pediatric rehabilitation: social support and stress in cases of cerebral palsy
Rehabilitación pediátrica: apoyo social y estrés en casos de parálisis cerebral
Juliana M. da SilvaI; Tereza Cristina C. F. de AraujoII
IPsycho Pedagogy, Rede Sarah de Hospitais de Reabilitação (Rede SARAH)
IIDepartment of Clinical Psychology, University of Brasília (UnB)
ABSTRACT
In pediatric rehabilitation, cerebral palsy constitutes one of the most diagnosed clinical conditions, however, further research is still necessary to improve care quality in the Brazilian context. Therefore, the present study aimed to: characterize, evaluate, and correlate social support and stress in family caregivers; and compare two care modalities (individual and group) of a rehabilitation program. In Study 1, 22 family members received individual and group care. In Study 2, 29 family members received only individual care. The instruments used were Sociodemographic Questionnaire, Social Support Perception Scale, Parental Stress Scale, Question about the Source of Social Support, and Case Reports. Researchers found no differences between the participants in Studies 1 and 2. The analysis of the entire sample revealed low-stress levels. Limited sources of support were observed, with family support being predominant. It was possible to identify a negative correlation between social support and stress.
Keywords: rehabilitation; cerebral palsy; social support; stress; caregivers.
RESUMEN
En rehabilitación pediátrica, la parálisis cerebral constituye una de las condiciones clínicas más diagnosticadas, pero se requiere pesquisas para mejorar la calidad asistencial brasileña. Por eso, la presente investigación tuvo como objetivos: caracterizar, evaluar y correlacionar apoyo social y estrés de familiares cuidadores; y comparar dos modalidades asistenciales (individual y grupal) en un programa de rehabilitación. En el Estudio 1, 22 familiares recibieron atenciones individuales y grupales. En el Estudio 2, 29 familiares frecuentaron solamente atenciones individuales. Se adoptaron como instrumentos: Cuestionario Sociodemográfico, Escala de Percepción del Apoyo Social, Escala de Estrés Parental, Cuestión sobre Fuente de Apoyo y Registros de Casos. No se constató diferencia entre participantes del Estudio 1 y del Estudio 2. El análisis del total de muestras reveló bajo nivel de estrés. Se percató limitación de las fuentes de apoyo, habiendo predominio del apoyo familiar. Fue posible identificar correlación negativa entre apoyo social y estrés.
Palabras clave: rehabilitación; parálisis cerebral; apoyo social; estrés; cuidadores.
1. Introduction
Despite important technological and clinical achievements in the area of Rehabilitation, it is not possible to overcome the limitations caused by certain pathological conditions, such as cerebral palsy, which affects two to three individuals per 1,000 live births in developed countries. In Brazil, the data indicates 30,000 to 40,000 new cases identified per year (Brasil, 2013 cited by Silva, 2016; Ferreira et al., 2015). In fact, cerebral palsy is one of the most diagnosed clinical conditions in this area.
Originally described by Little in 1861, it is defined by the existence of a non-progressive injury that causes delay or absence of expected acquisitions in human development. Cerebral palsy encompasses varied symptoms that manifest different degrees of impairment - in the motor, cognitive, and language areas - with multiple consequences for both the patient and the family group, due to the impositions associated with parental care, self-care, learning, communication, and social integration (Ferreira et al., 2015; Morris, 2007).
Considering this, it is indispensable to provide continuous and integral monitoring, based on up-to-date research, properly practiced by a multidisciplinary team specializing in Pediatric Rehabilitation. It should be mentioned that Division 22 of the American Psychological Association defines the field of Rehabilitation Psychology as one that encompasses the production and application of knowledge aimed at improving the quality of life of people with disabilities. Within the scope of this division, the Pediatric Rehabilitation section structures and organizes works aimed at promoting the healthy development and the rights of children with disabilities, in addition to establishing collaborative articulations with divisions 40 - Clinical Neuropsychology and 54 - Pediatric Psychology (American Psychological Association, 2017).
Taking into account that the care of people with disabilities may produce risk factors that influence the health and performance of those involved in this process, it is crucial to better comprehend parental stress in this context. According to Ribeiro, Porto, & Vandenberghe (2013), this type of stress derives from the functions performed by the parents with their children and is modulated by many variables, such as: characteristics of the child (e.g., severity of the disability) and of the parents (e.g., self-perception), family functioning, and other factors of the social and cultural contexts. In Ireland, Byrne, Hurley, Daly, & Cunningham (2010) have shown worse health status among caregivers of children with cerebral palsy, especially women, when compared to the general population. For Bemister, Brooks, Dyck, & Kirton (2015), researchers in Canada, the predictors of the psychological state of mothers in these conditions are the amplitude of the patient's physical and psychosocial impairment; the age of the child and the schooling of the caregivers. In Brazil, Santos, Oliveira, Vargas, & Macedo (2010) verified that more than half of the caregivers presented rates of intense overload, usually due to a lack of financial resources and feelings of helplessness. Ribeiro, Sousa, Vandenberghe, & Porto (2014) also found high levels of stress among 223 mothers of children and adolescents with cerebral palsy. Conversely, when applying the Beck Inventories with a sample of 27 mothers, Pereira and Kohlsdorf (2014) found that: a) the majority of the participants (n = 18) had scores corresponding to minimal anxiety and the remainder showed scores related to moderate anxiety; and b) 17 participants had no degree of depression and 10 indicated mild depression. In view of the above, it should be highlighted that a critical analysis of the international and national literature on cerebral palsy warned that, due to the heterogeneity of the sample composition of the studies (e.g., patient age and symptom manifestation), the contributions provided for clinical interventions are still restricted.
It is not enough to know the risk factors that interfere in dealing with the disability. Increasing the protective factors is also essential, especially those factors provided by the social environment (family and health services). Considering this relevance, especially at the national level, a search was conducted in the PubMed and Lilacs databases regarding social support in rehabilitation up to July 2015.There was growing interest in the subject, however, most of the publications were case reports, which revealed a shortage of other methodological delineations. No publication was located that included the descriptors "social support," "rehabilitation," and "pediatrics" (Silva, 2016).
It is interesting to note that, since the 1970s, many scholars have dedicated themselves to the investigation of social support, defined as the support received or perceived in various contexts. It is agreed that the concept is multidimensional, since it involves aspects related to emotional, instrumental and/or informative help. At the beginning of its theoretical development, it was highlighted that the subjective perception of being cared for, appreciated, and recognized in a network of relationships influences how one deals with the health-disease process. Briefly, it is pertinent to discern two models that seek to clarify the influences of social support on health. The first is based on the idea of "cushioning," where there would be a decrease in the adverse effects of the stressors in the situation experienced; while the second model underlines the positive factors of social support regardless of stress (Chwalisz & Vaux, 2000; Silva, 2016). Similarly, Gonçalves, Pawlowski, Bandeira, & Piccinini (2011) verified that social support is classified in the literature as emotional (affective valorization), instrumental (practical and direct assistance), informational (information and advice aimed at solving problems), and cognitive (posture of encouragement, listening, and reinforcement). From that mentioned above, the study had the following aims: a) to characterize, evaluate, and correlate the social support and stress of family caregivers of children diagnosed with cerebral palsy; and b) to compare two types of care (individual and group) in a pediatric rehabilitation program.
2. Method
2.1 Participants
Descriptive-correlational study, in which the sample, selected by convenience, was composed of 51 family members of patients diagnosed with cerebral paralysis undergoing monitoring at a rehabilitation center. According to the modality of intervention implemented, these participants were distributed in two studies:
Study 1 (n = 22): family members that had attended at least six sessions of a care program, in which activities of cognitive stimulation of the patients and psychoeducational interventions were conducted by the multidisciplinary rehabilitation team for groups of caregivers.
Study 2 (n = 29): this subsample did not participate in the group activities. That is, only individual patient stimulation and caregiver guidance were provided based on the needs of each case.
2.2 Instruments
The following instruments were used in both studies:
Sociodemographic Questionnaire: intended for the collection of general information, such as: family member's age, marital status, relationship with patient, place of residence, educational level, and work activity.
Electronic medical records: to obtain data on the patients' clinical and psychosocial conditions.
Case reports: corresponding to spontaneous reports from the participants at the end of each session.
Social Support Perception Scale: aims to investigate the 'practical' (factor 1) and 'emotional' (factor 2) dimensions of the social support through 29 items that explore how often the participant perceives the support of another person. The score ranges from 1 to 4 for each item: never (1),sometimes (2),often (3),or always (4). The mean score of each participant is obtained by summing the values indicated and dividing by the number of items in both factor 1 and factor 2. The mean factor scores with values between 1.0 and 2.9 indicate a low frequency of perception of the occurrence of emotional support, and values of 3.0 or above indicate more consistency in the perception of the occurrence of support (Siqueira, 2008).
Parental Stress Scale: this instrument, proposed in 2010 by Mixão, Leal, & Maroco (Rocha, 2012), presents 18 items that evaluate the relationship between the family member and the patient, assigning a score of 1 to 5 for each item, from 'totally disagree,' 'disagree,' 'undecided,' 'agree' to 'totally agree'. The parameters examined cover four factors: 1 - parental concerns; 2 - satisfaction with parental role; 3 - lack of control; and 4 - fears and anxieties. The total score of the scale can vary between 18 and 90. Three levels of stress are identified, according to the score obtained: 18-42 = low, 43-66 = intermediate and 67-90 = high.
Question about the Source of the Social Support: specifically prepared for this study (after a preliminary study), proposes 10 options (church/religion; spouse; health service; patient's grandparents; patient's uncles/aunts; government agency (e.g., councils and departments); other sons/daughters; friends; school; and an item called 'other'), with the participant attributing a level of importance (from 1 to 10) to each source of social support based on their perception of the degree of support received.
2.3 Data collection and analysis procedures
The study was authorized by the Ethics Committee for Research with Human Subjects (CAAE No. 48237315.4.0000.5540). Primarily, all the family members expressed their agreement to participate by reading and signing the consent form.
Study 1: the invitation to participate in the study was made by the first researcher by telephone. The aforementioned instruments were applied during a scheduled meeting in a rehabilitation unit.
Study 2: once the individual consultation was completed, the care team members provided the first researcher's contact to begin the data collection.
The analysis of the material obtained was carried out with the aid of the SPSS - version 21 program. For the comparison of the means of the factors of the Social Support Perception Scale and the Parental Stress Scale - considering Studies 1 and 2 - Student's t-test was used. Associations between the indicators of parental stress and social support were tested using Spearman's coefficient. The qualitative data of the case reports were submitted to thematic content analysis.
3. Results
First, the quantitative data will be explained. In this way, Table 3.1 presents the sociodemographic characterization of the participating family members. The majority were women (81.8% and 93.1%, in Studies 1 and 2, respectively), which converges with the specialized literature. The majority reported performing some paid activity (with formal or non-formal contracts), contributing regularly to the family income. Regarding education, there was a predominance of people with higher education in Study 1 (40.9%) and with high school education in Study 2 (31.0%).
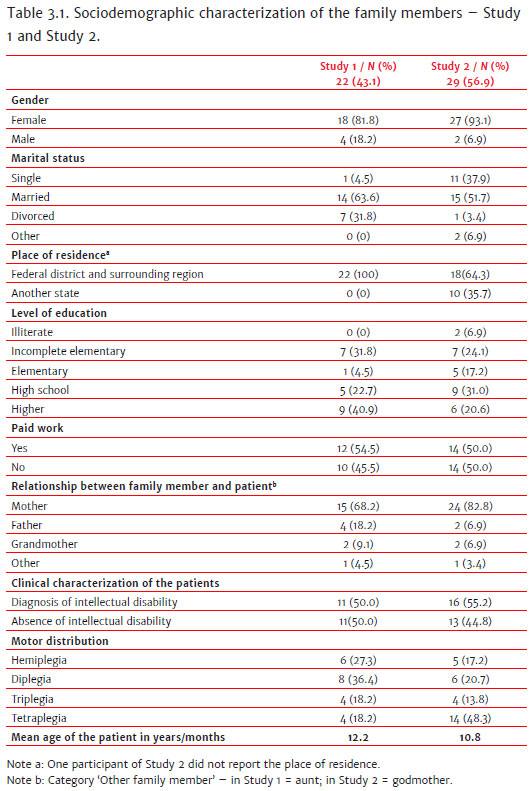
Data on the clinical and psychosocial conditions of the patients extracted from the electronic medical records are shown in Table 3.1. This information on cognitive performance refers to the application of the Wechsler Intelligence Scale (WISC) and Raven's Progressive Matrices (intellectual/cognitive components), as well as the results of the diagnosis of topographic motor impairment due to brain injury, performed by the functional therapy team (see Table 3.1). In addition, in relation to school inclusion, it should be noted that most of the patients were attending a learning environment, either in the regular education network or in special education (100% in Study 1 and 79.3% in Study 2).
3.1 Social Support Perception Scale
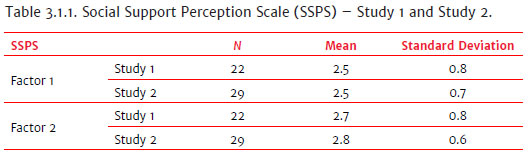
The results shown in Table 3.1.1 correspond to the mean scores for factor 1 (practical support) and factor 2 (emotional support). The means obtained were below 3.0, which indicate a low frequency of perception of social support by the family member. That is, the perceptions of the family members studied tend to reveal that the support received is not sufficient.
3.2 Parental Stress Scale
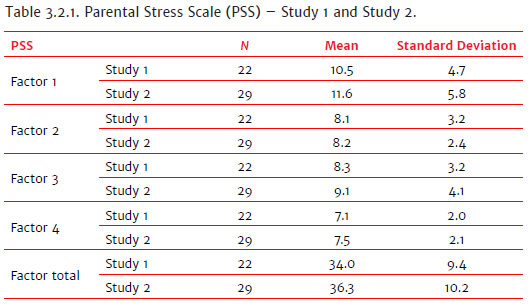
The Parental Stress Scale evaluates different stressors grouped into four general factors: parental concerns (factor 1), satisfaction with parental role (factor 2), lack of control (factor 3), and fears and anxieties (factor 4). The results of this investigation indicated a low level of stress among the participants (mean total score of 34.0 in Study 1 and 36.2 in Study 2), with no significant statistical difference. When the mean factor scores were compared between the participants of Study 1 and Study 2, no significant differences were found either (see Table 3.2.1). It is valid to conclude that the sample studied was part of a structured rehabilitation program, which possibly influenced the results in a positive way and contributed to reduce the level of stress of the caregivers. In addition, in the present study, there may have been a process of progressive adaptation of the family members to the situation of the child's disability, since the patients were, on average, 12 years of age in Study 1 and 10 years of age in Study 2, with the diagnosis of cerebral palsy possibly having been made at birth or in the first months of life.
3.3 Comparison between Sociodemographic Data, Social Support, and Parental Stress
As no differences were observed between Study 1 and Study 2 when analyzing the data generated by the scales separately, it was decided to consider the sociodemographic characteristics and the responses to the scales of the general sample (n = 51). It was verified that there was no correlation between social support and intellectual disability or between stress and intellectual disability. There were also no statistically significant differences between the mean score of social support and stress, and the motor distribution of the patients (grouped in cases of tetraplegia and non-tetraplegia). The mean social support score in patients classified as non-tetraplegic was 76.1 (SD = 20.8) and for the tetraplegic patients the mean score was 74.0 (SD = 18.9). The mean stress score for the tetraplegic patients was 37.1 (SD = 9.6) and for the non-tetraplegic patients the mean score was 34.4 (SD = 10.0).
Both social support scores and stress scores were classified as low. An inverse proportional correlation between social support indicators and parental stress indicators was observed. The correlation between the scores of the Social Support Perception Scale and the Parental Stress Scale was -0.454 (p = 0.03) among the participants of Study 1 and -0.458 (p = 0.01) among the participants of Study 2.
3.4 Issue of scoring the degree of importance of the social support
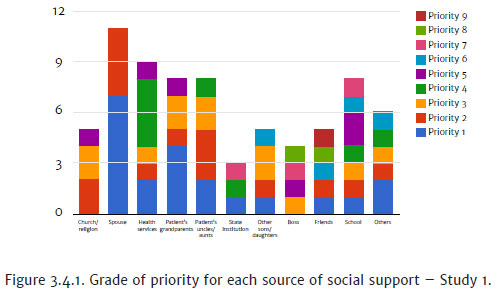
In Study 1, the spouse was the most cited source of support in priority 1 and 2, and health services were recognized in third place. When the sources of family support (spouses, grandparents, uncles and other children) were grouped, an expressive source of support was found (Figure 3.4.1).
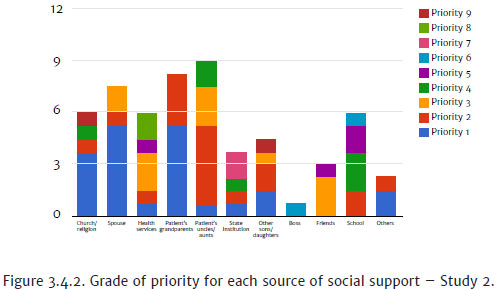
In Study 2, the patient's aunts/uncles were the most cited source of support (priority 1, 2, 3 and 4). Next, grandparents and spouses were also indicated by this subsample, which reaffirms the relevance of family support (Figure 3.4.2). In this sense, it should be remembered that, for Dessen and Braz (2000), support from the family can present itself in several ways: material and financial support, help with domestic tasks, childcare, guidance and emotional support.
3.5 Case records
The categorization of this qualitative material was based on the main axes of interest of the current literature on social support in health. Here are some excerpts from these experiences of caregivers:
• Emotional support category
"If I did not believe in God, I would not be here. Sarah's Project was a blessing."
"In the church, we find more comfort."
"You always need help from relatives, from the family."
"Psychological support always, groups to let it all out."
"We have to accept it as later they will accept it as well." "I think I need psychological support more than financial."
• Instrumental support category
"You have to chase after the professionals [...]."
"I'll dedicate as much as I can, I'll go by bus to the bus station, take another one until I get to the school. I'll be home by 8pm. There are people who think that it is not worth going to school, but I take him, he does not talk, but he sees someone with a backpack and he starts smiling. He has a friend who dropped out of school."
• Informational support category
"To seek the rights the child has."
"Information about cerebral palsy. There are many mothers who have no information about their own child."
There were 42 reports from participants in Study 1 and 54 in Study 2, with the predominance of the 'emotional support' category. Some participants were not able to recognize a source of social support. These reports denote personal suffering:
"I'm jealous of the people, because I do not have the support of the family."
"It's just me, because my family live far away."
"If anyone cares, they don't show it."
"It's very hard to get help."
Finally, it is relevant to note that there were no differences in relation to the care modalities: individual versus group. However, finding low levels of parental stress in Studies 1 and 2 may reveal that an established and consistent practice by a multidisciplinary rehabilitation team is a condition to ensure these benefits for the users.
4. Discussion
Initially, in relation to the patient's physical condition, the analysis of the variable 'motor distribution' of the injury was inconclusive, considering the size and heterogeneity of the sample. However, it is important to consider that, in many circumstances, this topographic distribution does not reflect the degree of functionality of the behavioral repertoire, since an individual diagnosed, for example, with diplegia and severe intellectual disability may require more help than another with tetraplegia without associated disorders (Braga & Campos da Paz, 2008, cited by Silva, 2016). Particularly regarding intellectual disability, the results obtained were also insufficient to confirm any association with the level of stress of the caregivers. That is, it was not possible to correlate the patients' clinical conditions with the level of stress or the need for social support among the caregivers.
The majority of the caregivers of this study were women (almost always mothers of the patients), which testifies to the female participation in the health care activities, either among the professionals who form the specialized teams, or as a member of the social support network of the patient (Dantas, Pontes, Assis, & Collet, 2012; Polita & Tacla, 2014; Silva, Amorim, Silva, & Correia, 2013). It should be mentioned that for Ribeiro et al. (2014), paid work and leisure were factors that reduced the stress of mothers of children and adolescents with cerebral palsy. In the present study, there was no correlation between these variables. However, the work activity indicators found were better than those of the data obtained by Pfeifer et al. (2014), in which 80% of the family caregivers did not have paid work as a result of the multiplicity of functions performed during the care.
A significant number of fathers were found to be the main source of support offered to the mothers and the rest of the family group, which converges with the perspective of Dessen and Braz (2000) on the subject. These results seem to indicate that the collaboration of the fathers can be stimulated in rehabilitation services through guidance that favors the inclusion of males. That is, social evolution requires health teams to develop monitoring protocols that are adapted to gender differences (e.g., health belief models, cognitive functioning and socio-cultural roles) in order to foster the diversification of the support network, as well as the reduction of the stress of the progenitor (Silva, 2016).
It should be emphasized that in Study 1 and Study 2, the subsamples reported a perception of limited social support. This result is in contrast with the notion that there is a need for diversified and consistent sources of support, since monitoring should be provided throughout the development cycle of both the patient and the family member (Dantas et al., 2012; Ogden, 2014; Polita & Tacla, 2014; Silva et al., 2013). Thus, the multidisciplinary rehabilitation team should plan actions in favor of expanding the social support network. This presupposes encouraging the active participation of the family members that are more available and able to provide the care necessary during certain periods. In addition, considering the primacy of the support perceived in the family context, it is essential that rehabilitation professionals implement measures aimed at extending the resources available in the socio-community settings, either through the articulation of the services provided in the ongoing health care, or through the improvement of public policies for the sector.
As a limitation of this work, it should be mentioned that the two studies were performed in the same institutional rehabilitation network. Therefore, the similarity of the care procedures adopted may have induced more satisfactory results with respect to stress. It should also be emphasized that the literature recommends that stress assessment should also be carried out at the time of the adverse event. However, in the present study, the family members had already dealt with the clinical condition of the children when they were invited to participate in the study. As a result, there may have been some adaptation and, therefore, a positive influence on the reactions of a population that was undergoing rehabilitation monitoring.
Regarding the composition and size restrictions of the sample, it is important to highlight that this constitutes an existing challenge in research carried out in health services. In fact, the present study was a descriptive, exploratory study, including secondary data produced through the routine monitoring of the patients, which reduces the generalization of the analyses. Therefore, more comparative studies of different modalities of care in rehabilitation are recommended. Attention is drawn to the contributions of the family-centered approach, which proved to be significant in both the group and individual consultations in this study.
Finally, the performance of multicenter studies in several rehabilitation units dedicated to the care of children with cerebral palsy are suggested in order to identify parameters that are more appropriate to the different socio-cultural and care conditions, thus extrapolating the focus to the biological and individual dimensions. For this, it will be important to create specific instruments to assess the social support and stress of the caregivers in rehabilitation. Such resources could contribute to the improvement of services engaged in serving the populations in developed and developing countries. In short, this study provides elements to support this assessment in future investigations.
References
American Psychological Association. (2017). Rehabilitation psychology. Retrieved from www.apa.org/about/division/div22.aspx [ Links ]
Bemister, T. B., Brooks, B. L., Dyck, R. H., & Kirton, A. (2015). Predictors of caregiver depression and family functioning after perinatal stroke. BioMed Central Pediatrics, 15(75),1-11. doi :10.1186/s12887-015-0397-5 [ Links ]
Brasil. Ministério da Saúde. (2013). Diretrizes de atenção à pessoa com paralisia cerebral. Retrieved from http://bvsms.saude.gov.br/bvs/publicacoes/diretrizes_atencao_paralisia_cerebral.pdf [ Links ]
Byrne, M. B., Hurley, D. A., Daly, L., & Cunningham, C. G. (2010). Health status of caregivers of children with cerebral palsy. Child Care, Health and Development, 36(5),696-702. doi: 10.1111/j-1365-2214.2009.01047.x [ Links ]
Chwalisz, K., & Vaux, A. (2000). Social support and adjustment to disability. In R. G. Frank & T. R. Elliott (Eds.), Handbook of rehabilitation psychology (pp. 537-552). Washington, DC: American Psychological Association. [ Links ]
Dantas, M. S. A., Pontes, J. F., Assis, W. D., & Collet, N. (2012). Facilidades e dificuldades da família no cuidado à criança com paralisia cerebral. Revista Gaúcha de Enfermagem, 33(3),73-80. doi: 10.1590/51983-14472012000300010 [ Links ]
Dessen, M. A., & Braz, M. P. (2000). Rede social de apoio durante transições familiares decorrentes do nascimento de filhos. Psicologia: Teoria e Pesquisa, 16(3),221-231. doi: 10.1590/S0102-37722000000300005 [ Links ]
Ferreira, M. C., Di Naccio, B. L., Otsuka, M. Y. C., Barbosa, A. M., Corrêa, P. F. L., & Gardenghi, G. (2015). Avaliação do índice de sobrecarga de cuidadores primários de crianças com paralisia cerebral e sua relação com a qualidade de vida e aspectos socioeconômicos. Acta Fisiátrica, 22(1),9-13. doi: 10.5935/0104-7795.20150003 [ Links ]
Gonçalves, T. R., Pawlowski, J., Bandeira, D. R., & Piccinini, C. A. (2011). Avaliação de apoio social em estudos brasileiros: Aspectos conceituais e instrumentos. Ciência & Saúde Coletiva, 16(3),1755-1769. doi: 10.1590/51413-81232011000300012 [ Links ]
Morris, C. (2007). Definition and classification of cerebral palsy: A historical perspective. Developmental Medicine & Child Neurology, 49(6),3-7. doi: 10.1111/j.1469-8749.2007.tb12609.x [ Links ]
Ogden, J. (2012). Health psychology: A textbook. (5th ed.). London: Open University Press. [ Links ]
Pereira, L. M., & Kohlsdorf, M. (2014). Ansiedade, depressão e qualidade de vida de pais no tratamento da paralisia cerebral infantil. Interação Psicológica, 18(1),37-46. doi: 10.5380/psi.v18i1.28823 [ Links ]
Pfeifer, L. I., Silva, D. B. R., Lopes, P. B., Matsukura, T. S., Santos, J. L. F., & Pinto, M. P. P. (2014). Social support provided to caregivers of children with cerebral palsy. Child Care, Health and Development, 40(3),363-369. doi: 10.1111/cch.12077 [ Links ]
Polita, N. B., & Tacla, M. T. G. M. (2014). Rede e apoio social às famílias de crianças com paralisia cerebral. Escola Anna Nery Revista de Enfermagem, 18(1),75-81. doi: 10.5935/1414-8145.20140011 [ Links ]
Ribeiro, M. F. M., Porto, C. C., & Vandenberghe, L. (2013). Estresse parental de crianças com paralisia cerebral: Revisão integrativa. Ciência & Saúde Coletiva, 18(6),1705-1715. doi: 10.1590/S1413-81232013000600022 [ Links ]
Ribeiro, M. F. M., Sousa, A. L. L., Vandenberghe, L., & Porto, C. C. (2014). Estresse parental em mães de crianças e adolescentes com paralisia cerebral. Revista Latino-Americana de Enfermagem, 22(3),440-447. doi: 10.1590/0104-1169.3409.2435 [ Links ]
Rocha, C. M. S. F. (2012). Stress parental em pais de crianças hospitalizadas: Influência de variáveis sociodemográficas e clínicas (Dissertação de Mestrado não publicada). Escola Superior de Saúde de Viseu, Viseu, Portugal. [ Links ]
Santos, A. A. S., Oliveira, C. C. C., Vargas, M. M., & Macedo, I. A. B. (2010). Avaliação da sobrecarga dos cuidadores de crianças com paralisia cerebral. Ciência, Cuidado e Saúde, 9(3),503-509. doi: 10.4025/cienccuidsaude.v9i3.9405 [ Links ]
Silva, G. G., Amorim, E. C., Silva, A. C. S., & Correia, D. S. (2013). Estresse e suporte social entre os cuidadores de crianças com retardo mental no estado de Alagoas. Revista da Sociedade Brasileira de Clínica Médica, 11(2),135-139. Retrieved from http://files.bvs.br/upload/S/1679-1010/2013/v11n2/a3565.pdf [ Links ]
Silva, J. M. (2016). Suporte social e reabilitação pediátrica: Uma análise sobre familiares de pacientes com diagnóstico de paralisia cerebral (Unpublished master's thesis). Universidade de Brasília, Brasília, DF, Brasil. [ Links ]
Siqueira, M. M. M. (2008). Construção e validação da Escala de Percepção de Suporte Social. Psicologia em Estudo, 13(2),381-388. doi: 10.1590/S1413-73722008000200021 [ Links ]
 Mailling address:
Mailling address:
Tereza Cristina Cavalcanti Ferreira de Araujo
Universidade de Brasília, Campus Darcy Ribeiro, Departamento de Psicologia Clínica
Brasília, DF, Brazil. CEP 70910-900
E-mail: araujotc@unb.br
Submission: 09/06/2017
Acceptance: 10/10/2018
There are no conflicts of interest to be declared.

