










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.21 no.2 São Paulo maio/ago. 2019
https://doi.org/10.5935/1980-6906/psicologia.v21n2p99-121
ARTICLES
PSYCOLOGICAL EVALUATION
Evidences of reliability and validity of the sensory assessment instrument Sensory Profile: a preliminary study
Evidencias de confiabilidad y validez de la herramienta de evaluación Sensory Profile: un estudio preliminar
Jací C. MattosI; Maria Eloísa F. D'AntinoII; Roberta M. CysneirosIII
IDevelopment Disorders Postgraduate Program, Mackenzie Presbyterian University (UPM)
IIDevelopment Disorders Postgraduate Program, Mackenzie Presbyterian University (UPM)
IIIDevelopment Disorders Postgraduate Program, Mackenzie Presbyterian University (UPM)
ABSTRACT
Considering the importance and need for studies that analyze the psychometric properties of assessment tools, this study investigated the psychometric parameters of reliability and validity of the Sensory Profile. The sample was composed of 336 children from the São Paulo metropolitan area, Brazil, aged from 5 to 10, from both genders, 298 of which did not have neurodevelopmental disorders and 38 of which had Autistic Spectrum Disorder (ASD). The tool showed satisfactory internal consistency with alpha values above 0.60 in most categories and factors. The mean scores of the sample of Brazilian children without neurodevelopmental disorders differed from the American normative sample. Children with ASD had lower sensory processing performance than children without neurodevelopmental disorders. The results showed that the Sensory Profile as translated and culturally adapted to Brazilian Portuguese pointed to the presence of sensory impairments in children with ASD investigated in this research.
Keywords: Sensory Profile; assessment; sensory processing; reliability; validity
RESUMEN
Teniendo en cuenta la necesidad e importancia de trabajos que analicen propiedades psicométricas de herramientas de evaluación, en este estudio se han investigado los parámetros psicométricos de confiabilidad y validez del Sensory Profile. La muestra estuvo compuesta de 336 niños de la región metropolitana de São Paulo, Brasil, de 05 a 10 años, ambos sexos, 298 sin trastornos del neurodesarrollo y 38 con Trastorno del Espectro Autista (TEA). La herramienta demostró consistencia interna satisfactoria con valores de alfa superiores a 0,60 en la mayoría de las categorías y factores. La media de puntajes de la muestra de niños brasileños sin trastornos del neurodesarrollo se diferenció de la muestra normativa americana. Los niños con TEA lograron desempeño del procesamiento sensorial inferior al de los niños sin trastornos del neurodesarrollo. Los resultados mostraron que el Sensory Profile traducido y adaptado culturalmente para el portugués de Brasil señaló la presencia de daños sensoriales en los niños con TEA de esta investigación.
Palabras clave: Sensory Profile; evaluación; procesamiento sensorial; confiabilidad; validez.
1. Introduction
Sensory integration therapy, outlined to guide the intervention in children who present significant difficulties in sensory processing and who restrict their participation in activities of daily living, is based on the theory of sensory integration developed by the occupational therapist Anne Jean Ayres (Ayres, 1972), based on her clinical experience to explain possible interactions between the neural processes of sensory reception, modulation, and integration with adaptive behavior.
Ayres (1972) describes sensory processing as a complex neurological process in which sensory information from the environment and the body itself is recorded, organized, modulated and interpreted by the brain to be subsequently utilized in response to different environmental demands. Information processing enables individuals to respond automatically and efficiently to specific sensory information received. The neurobiological process of sensory integration comprises a series of five stages: registration, modulation, discrimination, integration, and praxis, being essential for attention, visual perception, memory and action planning (Cabrera, Ayuso, Gil, & Juárez, 2017). Ayres' theory (1972) postulates that adequate processing and integration are fundamental for adaptive behavior, development, and learning and that losses in these processes may result from failures in the integration of the sensory information and the inability of higher centers to modulate and regulate the sensorimotor circuits (Ayres, 1972).
Ayres (1972) already indicated, in her initial studies, that 10% of children present adaptive and learning problems related to difficulties in sensory processing, nowadays called Sensory Processing Disorders (SPD). The SPDs are subdivided into three distinct types: sensory modulation disorder, sensory discrimination disorder, and sensory-based motor disorders. Each of them has subtypes which differ by the reaction to the sensory stimuli or by the behaviors resulting from such stimuli.
Parham and Mailloux (2001 as cited in Cabrera et al., 2017) listed five functional impairments related to SPD: decreased social participation and occupational engagement; reduction of the magnitude, frequency, or complexity of adaptive responses to an environmental challenge; loss of self-confidence and/or self-esteem; difficulties in daily life skills and in the family relationship; and delay in the development of sensory-motor skills and in the global and fine motor coordination. All these impairments negatively affect the behavioral, emotional, motor, and cognitive domains, according to Cabrera et al. (2017).
Losses in sensory processing are most often observed in children diagnosed with disorders such as Autism Spectrum Disorder (ASD), Down Syndrome (DS), Attention Deficit/Hyperactivity Disorder (ADHD), and schizophrenia when compared to their peers without disorders (Cabrera et al., 2017; Cervera, Cerezuela, Sala, Minguez, & Andrés, 2017). More specifically, individuals with ASD often find difficulties to regulate responses to specific sensations and stimuli which result in a profound impact on daily living activities and emotional regulation (Ashburner, Ziviani, & Rodger, 2008). Atypical sensory responses affect 42% to 88% of individuals with ASD (Baranek et al., 2002; Pfeiffer, Koening, Kinnealey, Sheppard, & Henderson, 2011) and were included as criteria for the diagnosis of ASD in the American Psychiatric Association/Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (American Psychiatric Association, 2014). The commonly utilized tools to aid in the diagnosis of ASD, such as ADOS (Autism Diagnostic Observational Schedule) and ADI-R (Autism Diagnostic Interview - Revised), contain items related to sensory processing, but do not provide specific information about the nature of sensory processing difficulties and their impacts on the behavioral, emotional, motor and cognitive domains (Dubois, Lymer, Gibson, Desarkar, Nalder, 2017), highlighting the importance of specific instruments, such as the Sensory Profile.
The Sensory Profile developed by Dunn (1999a) is a questionnaire intended for parents/caregivers to measure behaviors associated with responses to sensory stimuli in children aged from 3 to 10 years old. It is one of the most utilized instruments for the evaluation of the sensorial profile, and together with the clinical evaluation and other instruments for cognitive and behavioral analysis, it assists in the establishment of diagnoses and in the planning and proposition of activities, considering the sensory preferences or aversions of the affected children, aiming at improving the engagement in daily routines (Dunn, 1999b, Baranek et al., 2002).
The specificity of the questionnaire in the evaluation of sensory difficulties has mobilized professionals from different areas and in different countries to conduct studies aimed at its utilization in an appropriate manner, translating it, adapting it and verifying its credibility/reliability and validity (Neuman, Greenberg, Labovitz, & Suzuki, 2004; Chung, 2006, Engel-Yeger, 2012, Almomani, Brown, Dahab, Almomani, & Nadar, 2014; Ganapathy & Priyadarshini, 2014, Kayihan, Akel, Salar, Huri, Karahan, Turker, & Korkem, 2015; Ee, Loh, Chinna, & Marret, 2016). The inexistence of translated and validated instruments in our country to evaluate the abilities of sensory processing motivated the research of Mattos, D'Antino, & Cysneiros (2015) - briefly described below - and its continuity in the present study. The Sensory Profile, as translated and culturally adapted from English into
Brazilian Portuguese by Mattos, D'Antino, & Cysneiros (2015), in a previous study, involved 50 children, 47 of whom had no neurodevelopmental disorders, two with Down Syndrome and one with ASD, all aged between 5 and 10 years old, regularly enrolled in a private elementary school in the city of São Paulo. The analysis of the total score of the instrument translated and adapted resulted in the Cronbach's Alpha value of 0.76, indicating a satisfactory internal consistency of the instrument. The purpose of the present study was to investigate evidence of reliability and validity of the Sensory Profile employing a larger caseload of children without neurodevelopmental disorders and with ASD. For this purpose, the internal consistency of the instrument was measured by categories and factors, mean scores were compared between Brazilian children and those of the American normative sample without neurodevelopmental disorders, and the scores of Brazilian children with and without ASD were also compared.
2. Method
2.1 Attendees
A total of 336 children from the metropolitan region of São Paulo, from 05 to 10 years old, participated in the study, 298 of them without neurodevelopmental disorders (149 boys and 149 girls) and 38 with Autism Spectrum Disorder (28 boys and 10 girls).
The children without neurodevelopmental disorders were enrolled in six schools in São Paulo, two private schools (one located in the central area of the city and the other in the eastern zone) and four public schools in the city of Barueri/SP. From the 298 children without neurodevelopmental disorders, that is, without complaints from parents or teachers, nor submitted for evaluation and/or possible diagnosis, 47 composed the caseload of the previous research (Mattos, D'Antino, & Cysneiros, 2015). Of the 298 children, 186 attended public schools and 112 attended private schools. The inclusion criterion for the participation of the respondents consisted of being one of the people responsible for and living daily with the child. The exclusion criterion was based on the fact that the child had some neurodevelopmental disorder or was in the process of diagnosis evaluation. Participation was voluntary; that is, the parents/caregivers of the children were invited to fill out the instrument.
The parents/caregivers of children with ASD were recruited at an institution for assistance to people with ASD located in the central region of the city of São Paulo. The institution has a multidisciplinary team, which includes speech and language therapists, pedagogues, psychologists, and occupational therapists. The diagnosis of ASD carried out by neurologists/psychiatrists and the multidisciplinary team according to the criteria of DSM-5 (American Psychiatric Association, 2014), is an essential condition for the admission of these children to specialized care three times a week, in the regular school shifts, totalizing twelve hours per week.
2.2 Instrument
The version of the Sensory Profile utilized in this research was translated and culturally adapted to Brazilian Portuguese by Mattos, D'Antino, & Cysneiros (2015). The Sensory Profile was created by Winnie Dunn in 1994, and after extensive research between 1993 and 1999 on performance in sensory processing, the questionnaire was finalized with 125 questions (Dunn, 1999a). The research conducted for the development and improvement of the original instrument in English involved 155 occupational therapists, 1037 children without neurodevelopmental disorders, 61 children with Attention Deficit/Hyperactivity Disorder (ADHD), 32 children with Autism Spectrum Disorder (ASD), 24 children with Fragile X Syndrome and 21 children with Modular Sensory Disorder, aged between 3 and 14.
The instrument is organized into three areas: sensory processing, subdivided into six categories (hearing, sight, movement, touch, multisensory and oral), modulation, subdivided into five categories (tone, body position/movement, activity level, emotional responses, visual stimulus) and emotional behavior and responses, subdivided into three categories (emotional/social, behavioral effects on the sensory processing, and thresholds for responses). Besides the 14 categories described above, the instrument has nine factors which were organized based on an analysis of the main components of the questionnaire, obtained during the interpretation of the results of its application in the American normative sample (of children without neurodevelopmental disorders), studied by Dunn (1999b). According to the instrument manual, the factors provide an additional way to consider the obtained scores. They reveal patterns related to responsiveness to environmental stimuli (Dunn, 1999b).
The Sensory Profile is a questionnaire based on judgment and must be applied to those who have daily contact with the child/teenager and are responsible for them. Each question describes the children's responses to various sensory experiences. The responses must consider how often (always, often, occasionally, rarely, never) behaviors occur, and the scores are given from one to five (one corresponding to always and five to never). The lower the score, the more signs of sensory difficulties, that is, lower scores indicate greater severity of sensory problems, and the higher the score, the less evidence of sensory difficulties. The highest possible score obtained in the sum of the 125 questions is that of 625 points, and the lowest possible score is 125 points.
2.3 Procedures
The descriptive and cross-sectional study was approved by the Research Ethics Committee of Mackenzie Presbyterian University, under No. 1.593.863 and authorized by Pearson Publisher, which owns the instrument's copyright, through a signed contract (11486-U) between the parts.
2.4 Application
The utilized procedures were the same as described by Mattos, D'Antino, & Cysneiros (2015). In-person meetings were held with the school board and the ASD support institution to present the research goals and the original instruments in the English language and the ones translated and culturally adapted into Brazilian Portuguese by Mattos, D'Antino, & Cysneiros (2015). It was established that the application of the instrument would occur at the end of the meetings between parents and teachers and/or between parents and coordinators. The application of the questionnaire to the parents/caregivers of the children without neurodevelopmental disorders occurred from August 2016 to February 2018. For the parents/caregivers of the children with ASD, the application of the instrument occurred in the months of May and June of 2017.
The legal representatives of the schools and the ASD support institution, as well as the children's parents, signed the Free and Informed Consent Term (FICT). The instrument was filled out by the parents/caregivers of children from 5 to 10 years old, in the presence of the researcher to assist the respondents if they presented any difficulties regarding the language of the questionnaire or interpretation of the questions. No difficulties were observed in filling out the instrument. The average time for filling out was about thirty minutes.
2.5 Data analysis
The scores for each of the instrument questions were obtained by following the instructions in Chapter four of the Sensory Profile manual and utilizing the Scoring Summary Sheet: always = 1 point; often = 2 points; occasionally = 3 points; rarely = 4 points and never = 5 points.
To evaluate the reliability of the instrument through the verification of its internal consistency, the Cronbach's Alpha coefficients were calculated, from the group of children without neurodevelopmental disorders, in relation to the 14 cat egories and the nine factors of the instrument, and they were compared with those obtained in the American normative sample.
The scores of the sample of Brazilian children without neurodevelopmental disorders among the six age groups were compared by the one-way ANOVA, followed by the Bonferroni post-hoc test. In addition, the sample scores of Brazilian children without neurodevelopmental disorders, in each of the 14 categories and by age group, were compared with the scores of the American normative sample, available in the Sensory Profile manual (Dunn, 1999b), by the Student's t-test (one sample), as well as conducted by Neuman (2006). Additionally, and for analytical validity purposes in relation to the clinical group scores of a sample of Brazilian children without neurodevelopmental disorders, each of 14 categories was compared with the scores of the Brazilian sample with ASD by the Student's t-test for independent samples. Cohen's d values were also calculated to indicate the magnitude of the effect of the significant differences, that is, the size of the effect of the observed results. For the interpretation of the results in relation to the size of the effect, were considered: up to 0.20 = small; 0.50 = average; 0.80 or greater = large (Conboy, 2003). Furthermore, values were established referring to a sensory performance classification system in which the scores are organized into three groups: typical performance, probable difference, and definite difference. Typical sensory performance corresponds to scores greater than one standard deviation below the mean; probable difference corresponds to scores lower than one standard deviation below the mean; definite difference corresponds to scores lower than two standard deviations below the mean, and the means and standard deviations refer to the group of children without neurodevelopmental disorders of the American normative sample (Dunn, 1999b). To evaluate the presence of sensory difficulties in the group of children with Autism Spectrum Disorder, the means of these children were analyzed in relation to the three ranges of sensory performance: typical performance, probable difference, and definite difference.
P values with significance level adopted at 5%, that is, p < 0.05. were considered as significant values.
The data was analyzed utilizing the SPSS/version 24.0.
3. Results
The sample of children without neurodevelopmental disorders was composed of 298 subjects, being 149 males (50%). Regarding the ages, the smallest groups were those of five and seven years old, both with 48 subjects (16.2% each group) and the largest group was the 10-year-old group with 52 subjects (17.5%), followed by the groups of six, eight and nine years old, with 50 subjects (16.7% each group). A comparison was made in the composition of this sample in relation to the number of participants by gender and age groups, and it was possible to reach very close numbers in the two variables: gender and age (Table 3.1).
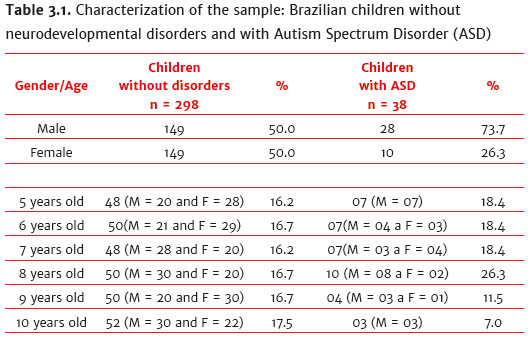
The sample of children with ASD was composed of 38 subjects, being 28 males (73.7%). Regarding the ages, the smallest groups were those of 10 years old, with three subjects (7.0%) and nine years old, with four subjects (11.5%). The largest group was the one of eight years old, with 10 subjects (26.3%) followed by five, six and seven years old, with seven subjects each (18.4%). In this sample, it was not possible to compare the number of subjects by gender, considering the higher prevalence of males with this disorder (Table 3.1).
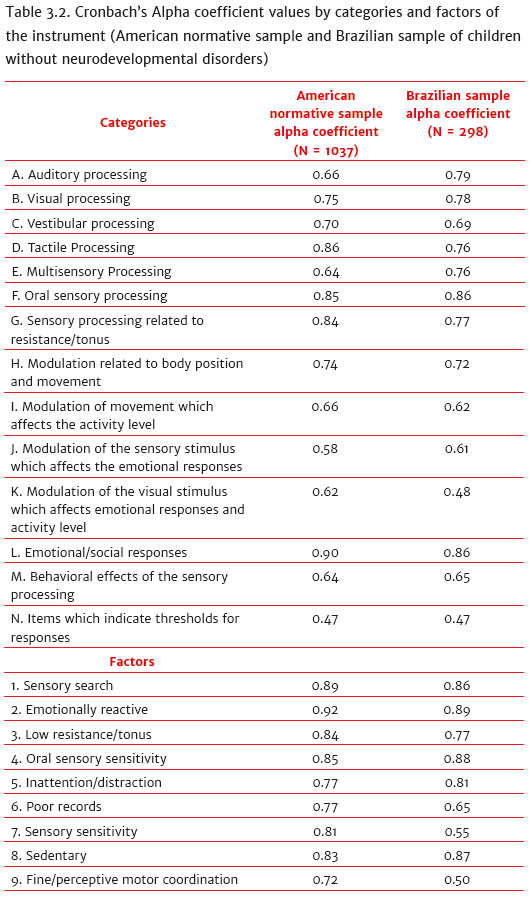
Regarding the reliability, Table 3.2 presents the alpha coefficient values for the 14 categories and for the nine factors of the instrument. In the American normative sample, the values varied between 0.47 and 0.91 and in this Brazilian sample of children without neurodevelopmental disorders, between 0.47 and 0.89. The lowest alpha value was found in category N for the American sample and for the Brazilian sample. The highest alpha value was found in factor two - in both samples. The Cronbach's Alpha values in this Brazilian sample of children without neurodevelopmental disorders, in the majority of the categories (12 out of 14) and in most of the factors (seven out of nine) were above 0.60. Exceptions occurred only in categories K and N and factors seven and nine (alpha between 0.47 and 0.55). The minimum acceptable internal consistency for an instrument verified based on the Cronbach's Alpha coefficient is not consensually established in the literature. According to Souza, Alexandre and Guirardello (2017), there are studies which determine that alpha values above 0.70 are ideal, but some studies consider values below 0.70 - but close to 0.60 - as satisfactory. In such analysis, the results of this Brazilian sample of children without neurodevelopmental disorders are similar to those of the American normative sample regarding alpha values and were between the satisfactory and the ideal - in 12 categories and in seven factors of the instrument.
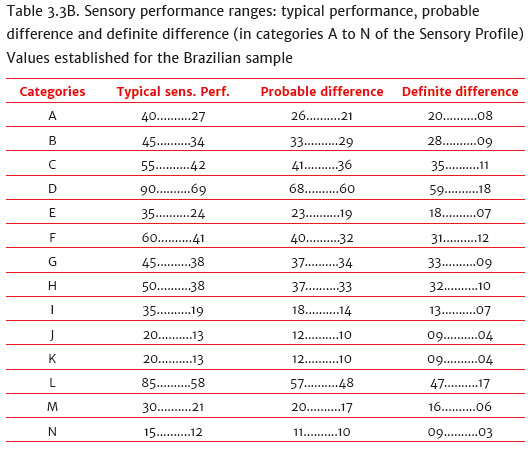
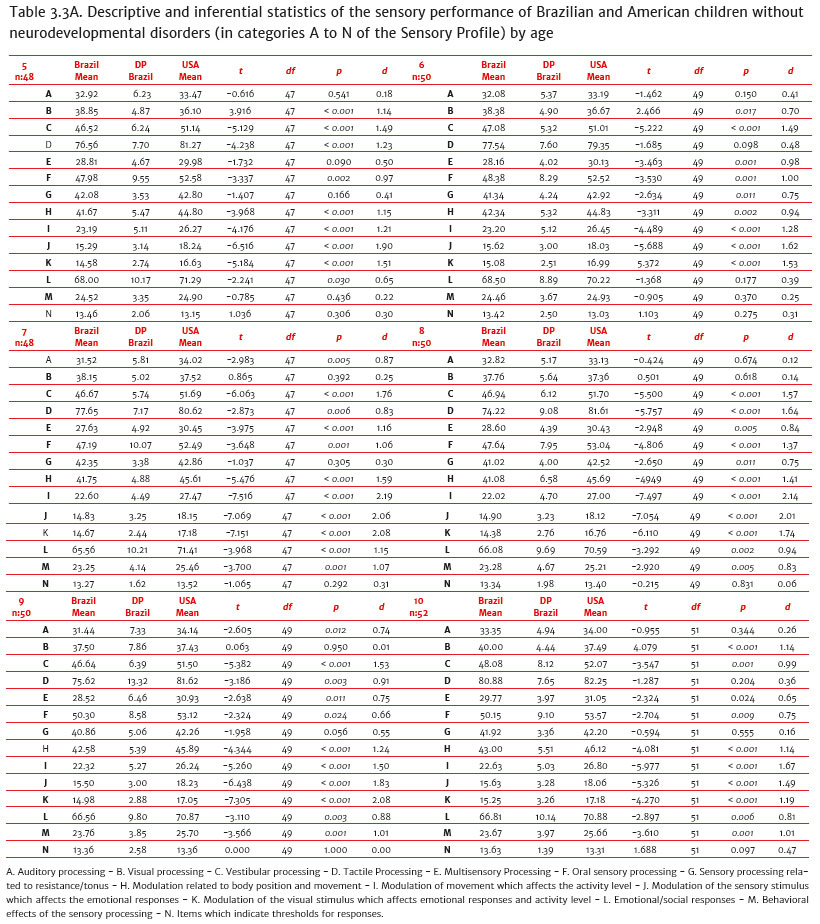
Regarding the comparison of mean scores by category among the six age groups of children without neurodevelopmental disorders through the one-way ANOVA, there were no statistically significant differences in almost all the analyzed age groups and categories, except for category D (F (5.292) = 3.215, p = 0.008). Exclusively in this category, the post hoc revealed that the mean scores of the 10-year-old children were significantly higher than the 8-year-old (t = 6.665, p = < 0.001) and 9-year-old children (t = 5.265, p = 0.003), but did not differ from the American normative sample (table 3.3A). Although the mean scores of eight-yearold and nine-year-old children in category D are statistically smaller than those of 10-year-old children, they are within the typical sensory performance range (Table 3.3B). As to the comparison of the mean scores of the sample of Brazilian children without neurodevelopmental disorders with the means of the American normative sample, by age group and in each category of the instrument (table 3.3A), it is observed that the means of the Brazilian sample were lower in most of the categories and for all the age groups, except for category B (5, 7, 8, 9 and 10year-olds) and category N (5, 6 and 10-year-olds). In order to interpret these differences, it was verified in the instrument manual that in category B, the visual responses of the children are tracked (for example, being bothered with bright lights after others have already adapted to brightness) and category N, the child's level of modulation is verified (for example, if he/she skips from one activity to another so that it interferes with a game) (Dunn, 1999b). Upon the ascertainment that the means of the Brazilian sample without neurodevelopmental disorders were higher than the American ones only in the two categories and age groups mentioned above (5, 7, 8, 9 and 10-year-olds) and N (5, 6 and 10-year-olds), it was inferred that in these two categories the Brazilian children without neurodevelopmental disorders of this sample have less sensory difficulties when compared to the children, also without disorders, of the normative sample. Due to the fact that the mean scores of the Brazilian sample were lower than the normative sample in almost all the categories and ages, scores were calculated for the three ranges of sensory performance (Table 3.3B). The referred values - as well as the values for the normative sample - were determined following the guidelines of the instrument manual, as follows: typical sensory performance corresponds to scores greater than one standard deviation below the general mean by category (of the sample of children without neurodevelopmental disorders); probable difference corresponds to scores lower than one standard deviation below the general mean by category; definite difference corresponds to scores lower than two standard deviations below the general mean by category (Dunn, 1999b). The maximum values of the typical sensory performance range are the same as those of the American sample (adding the maximum values of the fourteen categories, we reach the maximum possible score of the instrument: 625) as well as the minimum values of the definite difference range (adding the minimum values of the fourteen categories, we reach the minimum possible score of the instrument: 125); all the other values were calculated according to the means and standard deviations of the Brazilian sample in each category of the instrument (Table 3.3B).
In Table 3.3A, it is possible to observe that, although the mean scores of the Brazilian sample have statistically differed from the American normative sample, with medium to large effect size, in most categories, and at all ages, these scores are within the typical sensory performance range in all the categories of the instrument and for all the age groups.
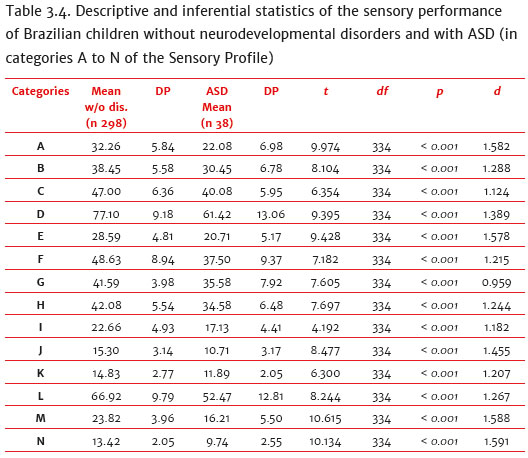
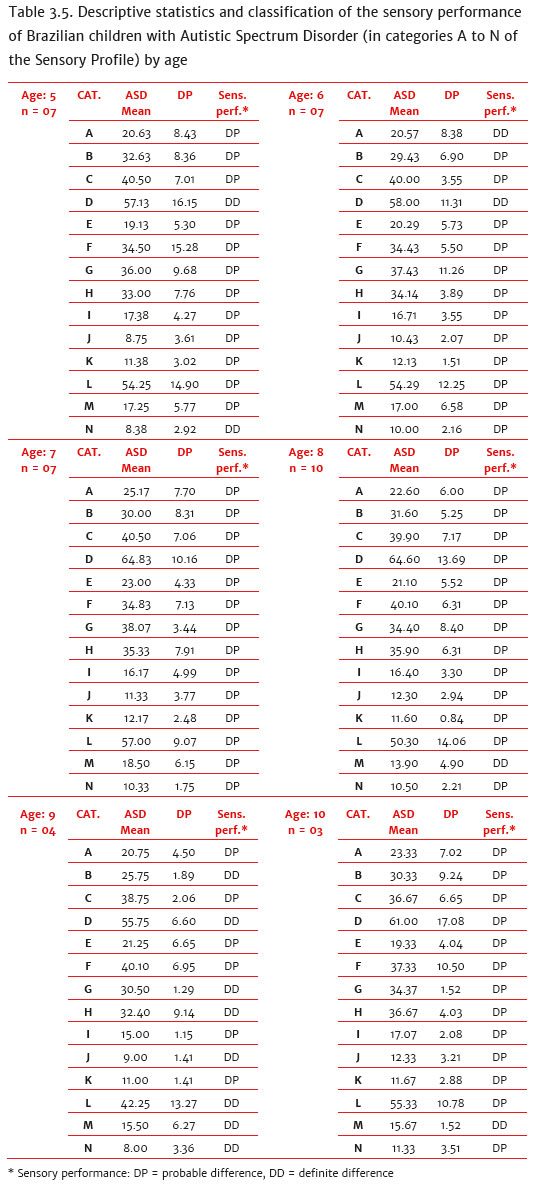
Then, it was evaluated whether the instrument discriminates the children without neurodevelopmental disorders from the children with ASD. In the 14 categories of the instrument, the mean scores of the children without disorders and with ASD were statistically different. In addition, the mean scores of the ASD group were significantly lower than those of children without neurodevelopmental disorders (Table 3.4) and, corroborating these results, the classification of the sensory performance of children with ASD was in the probable difference and/or definite difference ranges in all the categories of the instrument and in the six age groups investigated in this study (Table 3.5). The results of these analyses demonstrate evidence that the instrument differentiates the sensory performance of children without neurodevelopmental disorders and of children with ASD.
4. Discussion
The previous study conducted by Mattos, D'Antino, & Cysneiros (2015) showed that the Sensory Profile as translated and culturally adapted from English into Brazilian Portuguese presented satisfactory internal consistency and that it could be investigated to verify its reliability and validity. In the present study, the caseload was expanded and involved 336 children, 298 of them without neurodevelopmental disorders, and 38 with ASD. It must be pointed out that, in this study, the Brazilian sample of children with ASD was larger and more homogeneous in relation to the age group (5 to 10 years old) compared to the American sample, which involved 32 children aged from 3 to 13 years old (Dunn, 1999b).
The research conducted for the development of the instrument pointed to the fact that sensory processing skills did not change substantially from the age of five (Dunn, 1999b), which was also verified in this study. Although the scores of eight and nine-year-old children of this sample of Brazilian children without neurodevelopmental disorders were statistically lower than the scores of ten-year-old children in only one category of the instrument, they were still within the typical performance range.
Concerning the reliability of the instrument, Cronbach's Alpha was calculated for the 14 categories and the nine factors of the instrument in relation to the performance of the Brazilian children without neurodevelopmental disorders. The alpha values higher than 0.60 were observed in 12 of the 14 categories and in seven of the nine factors of the instrument, located between the satisfactory and the ideal, and were similar to those reported in the American normative sample. Corroborating our results, Neuman et al. (2004) and Kayihan et al. (2015) also reported, in a minority of the categories, alpha values below 0.60, but they considered the Sensory Profile as a reliable instrument, as they argued that alpha values above 0.60, in most categories, are indicative of an acceptable internal consistency. Although the internal consistency of the instrument is between satisfactory and ideal, the sensory performance of the Brazilian children without neurodevelopmental disorders, in the great majority of the categories and age groups, was lower than the performance reported in the American normative sample (Dunn, 1999b), as observed by Neuman (2006) for Israeli children. Thus, the new score ranges for the classification of sensory performance (typical performance, probable difference, and definite difference) were established in each category of the instrument and according to the instructions of its manual. Utilizing the new score ranges, it was observed that the sensory performance of the children with ASD, in all the ages and categories, was in probable difference and/or definite difference, and in no category or age group, it was found in a typical performance. Not surprisingly, it was observed that the means of the children with ASD were notably lower in all the categories of the instrument when compared to the means of the children without neurodevelopmental disorders.
The results showed that the Sensory Profile as translated and culturally adapted to Brazilian Portuguese pointed to the presence of sensory impairments in the children with ASD investigated in this study, reiterating the presence of sensory processing difficulties in ASD conditions widely described in the literature (Pfeiffer et al., 2011, Ganapathy & Priyadarshini, 2014 and Kayihan et al., 2015) and in the American Psychiatric Association/Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (American Psychiatric Association, 2014).
5. Conclusion
The results of the present study showed that the Sensory Profile as translated and culturally adapted to the Brazilian Portuguese presents an internal consistency similar to that observed in the original instrument in the English language, located between satisfactory and ideal. The Brazilian children without neurodevelopmental disorders - all resident in the southeastern region of Brazil, more specifically in the metropolitan region of São Paulo - in general, presented lower mean values than the children of the American normative sample. Through the new score ranges established for the Brazilian children regarding the classification of sensory performance in all the categories of the instrument, it was possible to observe that all the children with ASD investigated in this caseload fit within the probable difference and/or definite difference ranges and that their sensory performances were lower than those observed in children without neurodevelopmental disorders.
Future studies with a representative national sample and other clinical groups are required to ensure the reliability and validity of the instrument, including the expansion of the age range which, in this study, was restricted to the ages of 5 to 10 years old. In addition, it would be appropriate to include the confirmatory factor analysis to investigate whether the factor structure of the original instrument remains in the translated and adapted version. Despite the above mentioned limitations, the results of the present study showed that the Sensory Profile as translated and culturally adapted to Brazilian Portuguese pointed to the presence of sensory processing impairments in the children with ASD investigated in this research.
References
Almomani, F. M., Brown, C., Dahab, S. A., Almomani, M., & Nadar, M. (2014). Cross-cultural adaptation of the Adolescent/Adult Sensory Profile: Establishing linguistic equivalency and psychometric properties of the Arabic version. Disability and Rehabilitation, 36,765-770. doi:10.3109/09638288.2013.819386 [ Links ]
American Psychiatric Association. (2014). Manual diagnóstico e estatístico de transtornos mentais: DSM-5. (5ª Ed.) Porto Alegre: Artmed. [ Links ]
Ashburner, J., Ziviani, J., & Rodger, S. (2008). Sensory processing and classroom emotional, behavioral and educational outcomes in children with Autism Spectrum Disorder. American Journal of Occupational Therapy, 62(5),564-573. doi:10.5014/ajot.62.5.564 [ Links ]
Ayres, A.J. (1972). Sensory integration and learning disorders. Los Angeles: Western Psychological Services. [ Links ]
Baranek, G. T., Chin, Y. H., Hess, L. M., Yankee, J. G., Hatton, D. D., & Hooper, S. R. (2002). Sensory Processing correlates of occupational performance in children with fragile X syndrome: Preliminary findings. American Journal of Occupational Therapy, 56(5),538-546. doi:10.5014/ajot.56.5.538 [ Links ]
Cabrera, S. J., Ayuso, D. R., Gil, G. R., & Juárez, J. M. T. (2017). Assessment of sensory processing characteristics in children between 3 and 11 years old: A systematic review. Frontiers in Pediatrics, 12(5),266. doi:10.3389/fped.2017.00057 [ Links ]
Cervera, P. S., Cerezuela, G. P., Sala, F. G., Minguez, R. T., & Andrés, M. I. F. (2017). Sensory processing in children with Autism Spectrum Disorder and/or Attention Deficit Hyperactivity Disorder in the home and classroom contexts. Frontiers in Psychology, 11(8),1772. doi:10.3389/fpsyg.2017.01772 [ Links ]
Chung, J. C. (2006). Measuring sensory processing patterns of older Chinese people: psychometric validation of the Adult Sensory Profile. Aging & Mental Health, 10, 648-655. doi:10.1080/13607860600648080 [ Links ]
Conboy, J. E. (2003). Algumas medidas típicas univariadas de magnitude de efeito. Análise Psicológica, 2(XXI),145-158. doi:10.14417/ap.29 [ Links ]
Dubois, D., Lymer, E., Gibson, B. E., Desarkar, P., & Nalder, E. (2017). Assessing sensory processing disfunction in adults and adolescents with Autism Spectrum Disorder: A scoping review. Brain Sciences, 7(8),1-24. doi:10.3390/brainsci7080108 [ Links ]
Dunn, W. (1999a). Caregiver Questionnaire - Sensory Profile. United States: Pearson. [ Links ]
Dunn, W. (1999b). User's Manual - Sensory Profile. United States: Pearson. [ Links ]
Ee, S., Loh, S., Chinna, K., & Marret, M. J. (2016). Cross-cultural adaptation and psychometric properties of the Malay version of the short sensory profile. Physical & Occupational Therapy in Pediatrics, 36(2),117-130. doi:10.3109/0194638.2015.1040574 [ Links ]
Engel-Yeger, B. (2012). Validating the Adolescent/Adult Sensory Profile and examining its ability to screen sensory processing difficulties among Israeli people. British Journal of Occupational Therapy, 75,321-329. [ Links ]
Ganapathy, S. U., & Priyadarshini, S. (2014). Standardization of Tamil version of Short Sensory Profile. International Journal of Pharma and Bio Sciences, 5,260-266. [ Links ]
Kayihan, H., Akel, B. S., Salar, S., Huri, M., Karahan, S., Turker, D., & Korkem, D. (2015). Development of a turkish version of the Sensory Profile: Translation, cross-cultural adaptation, and psychometric validation. Perceptual and Motor Skills, 120(3),971-976. doi:10.2466/08.27.PMS.120v17x8 [ Links ]
Mattos, J. C., D'Antino, M. E. F., & Cysneiros, R.M. (2015). Tradução para o português do Brasil e adaptação cultural do Sensory Profile. Psicologia: Teoria e Prática, 17(3),104-120. doi:10.15348/1980-6906/psicologia.v17n3p104-120 [ Links ]
Neuman, A., Greenberg, D. F., Labovitz, D. R., & Suzuki, L. A. (2004). Crosscultural adaptation of the Sensory Profile: Establishing linguistic equivalency of the Hebrew version. Occupational Therapy International, 11(2),112-130. doi:10.1002/oti.201 [ Links ]
Neuman, A. (2006). Patterns of response to sensory stimuli encountered in daily activities: a comparison between 3-10-year-old Israeli and American children without disabilities. Occupational Therapy International, 13(2),79-99. doi:org/10.1002/oti.9 [ Links ]
Pfeiffer, B. A., Koening, K., Kinnealey, M., Sheppard, M., & Henderson, L. (2011). Effectiveness of Sensory Integration Interventions in Children with Autism Spectrum Disorders: A pilot study. American Journal of Occupational Therapy, 65(1),76-85. [ Links ]
Souza, A. C., Alexandre, N. M. C., & Guirardello, E. B. (2017). Propriedades psicométricas na avaliação de instrumentos: avaliação da confiabilidade e da validade. Epidemiologia e Serviços de Saúde, 26(3),649-659. doi:10.5123/s1679-49742017000300 [ Links ]
 Mailling address:
Mailling address:
Jací Carnicelli Mattos
Programa de Pós-Graduação em Distúrbios do Desenvolvimento, Universidade Presbiteriana Mackenzie
Rua da Consolação, 930, Prédio 28
São Paulo, SP, Brazil. CEP: 01302-907
E-mail: jcarnicellimattos@gmail.com
Submission: 10/05/2018
Acceptance: 28/02/2019
The present work was supported by the Mackenzie Research Fund MACKPESQUISA and the Coordination for the Improvement of Higher Education Personnel – Brazil (CAPES) – Funding Code 001.


{kind=link}