










Serviços Personalizados
artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.21 no.2 São Paulo maio/ago. 2019
http://dx.doi.org/10.5935/1980-6906/psicologia.v21n2p336-358
ARTICLES
CLINICAL PSYCHOLOGY
How I am, how am I: nutritional status and body image in women submitted to aesthetic plastic surgery
Como Sou, como Estou: estado nutricional e imagem corporal em mulheres submetidas à cirurgia plástica estética
Como Soy, como Estoy: estado nutricional e imagen corporal en mujeres sometidas a cirurgia plastica estetica
Alessandra F. E. GarciaI; Sebastião S. AlmeidaII; Telma Maria B. CostaIII
IUniversity of São Paulo, Ribeirão Preto, SP, Brazil
IIUniversity of São Paulo, Ribeirão Preto, SP, Brazil
IIIUniversity of São Paulo, Ribeirão Preto, SP, Brazil
ABSTRACT
Aesthetic Plastic Surgery (APS) has grown dramatically around the world, especially in Brazil. Women were more dissatisfied with their appearance compared to men, and this is the main predictor for the search of APS. We investigated the body image (BI) and nutritional status (NS) of 40 adult women requesting APS - Clinical Group (G1, n = 20) - and 20 not requesting APS - Comparative Group (G2) - with similar age and socio-educational characteristics. We evaluated the biochemistry of blood, the BMI, and the percentage of body fat, with a statistically significant difference between G1 and G2 (p < 0.01). G1 showed a higher prevalence of overweight/obesity, dissatisfaction with the overall appearance (p = 0.04) in the Body-Self-Relationships Questionnaire, concern with BMI (p = 0.04), and major investment in appearance (p = 0.04). Due to these potential indicators of mental health problems, psychological and nutritional monitoring is essential to prevent poor progression in APS.
Keywords: body image; plastic surgery; nutritional evaluation; nutritional status; biochemical exams.
RESUMO
Cirurgia Plástica Estética (CPE) cresceu drasticamente no mundo, especialmente no Brasil. Mulheres mostraram-se mais insatisfeitas com a aparência em relação aos homens, e esse é o principal preditor para a busca da CPE. Investigou-se a Imagem Corporal (IC) e o Estado Nutricional (EN) de 40 mulheres adultas solicitantes de CPE - Grupo Clínico (G1, n = 20) - e 20 não solicitantes de CPE - Grupo de Comparação (G2) - de características etárias e socioeducacionais semelhantes. Avaliaram-se a bioquímica do sangue, o IMC e a porcentagem de gordura corporal com diferenças estatísticas significativas entre G1 e G2 (p < 0, 01). O G1 apresentou maior prevalência de sobrepeso/obesidade, insatisfação com a aparência geral (p = 0,04) no Body-Self-Relationships Questionnaire, grande preocupação com o IMC (p = 0,04) e grande investimento na aparência (p = 0,04). Em função desses potenciais indicadores de problemas de saúde mental, o monitoramento psicológico e nutricional é essencial para prevenir uma evolução negativa em CPE.
Palavras-chave: imagem corporal; cirurgia plástica; avaliação nutricional; estado nutricional; exames bioquímicos.
RESUMEN
Cirugía Plástica Estética (CPE) creció drásticamente en Brasil y en el mundo. Mujeres se mostraron más insatisfechas con la apariencia que los hombres, siendo éste el principal predictor de búsqueda por CPE. Se ha investigado la imagen corporal (IC) y el estado nutricional (EN) de 40 mujeres adultas solicitantes de CPE - Grupo Clínico (G1, n = 20) - y 20 que no solicitó CPE - Grupo de Comparación (G2) - de características de edad e socioeducativa similares. Se evaluó la bioquímica de la sangre, el IMC y el % de grasa con diferencias significativas entre G1 y G2 (p < 0, 01). G1 mostró mayor prevalencia de sobrepeso/obesidad, insatisfacción con la apariencia (p = 0.04) en el Body-Self-Relationships Questionnaire, preocupación por el IMC (p = 0.04) y mayor investidura en apariencia (p = 0.04). Debido a estos indicadores potenciales de problemas de salud mental, el monitoreo psicológico y nutricional es esencial para prevenir la mala progresión en CPE.
Palabras clave: imagen del cuerpo; cirugía plástica; evaluación nutricional; alor nutricional; exámenes bioquímicos.
1. Introduction
According to the Brazilian Society of Plastic Surgery (Sociedade Brasileira de Cirurgia Plástica, 2017), the last census indicated a significant increase in the number of Aesthetic Plastic Surgeries (APS) in Brazil, which is the second country in the number of aesthetic surgical procedures, reaching 1.47 million surgeries by year. Of this total, 839,288 (57%) are APS and 664,809 (43%) are reparative surgeries. The main APS performed were respectively: augmentation mammoplasty (288,597 = 19.6%), liposuction (229,700 = 15.6%), and abdominoplasty (229,512 = 15.6%). The majority of patients performing aesthetic procedures are women, although there is a growth in the demand for these interventions between men. APS is an elective surgical procedure that seeks appearance improvement, changing the original forms of the patient, being a surgery of appearance and self-esteem (Avelar, 2011).
Body Image (BI) involves a complex entanglement of psychological, social, cultural, and biological factors that subjectively determine how individuals see themselves, think they are seen, and see others (Damasceno et al., 2006). Cash (2011) considers that BI includes two simultaneous factors: attitudinal and perceptive. Perceptual dimensions relate to the individual's estimation of the size and shape of his/her own body and how he/she thinks about it, while attitudinal factors include many affective, behavioral, cognitive, and satisfaction or dissatisfaction variables related to one's appearance.
Dissatisfaction with BI reflects the discrepancy between the self-perceived body and the ideal body, and may relate to negative assessments of body size, body weight and shape, and muscle tone. Disorders related to BI have become a global epidemic, and family, peers, media, sociocultural, and biological elements influence the condition. Studies have pointed out that comments and attitudes of parents regarding BI, weight, and appearance are related to the dissatisfaction of BI in children, causing concerns about weight and the use of restrictive diets (Laus, Straatman, Kakeshita, Braga Costa, & Almeida, 2013).
It is common to find studies in Brazil and worldwide that highlight the perceptual component, that is, how much the individual has or does not have an (in)accurate estimate related to their size, shape, and body weight. The attitudinal dimension, in which the cognitive, affective, and behavioral components are present, usually is little accessed. This dimension accesses other components no less relevant than (dis)satisfaction, but rather cognitive components (investment and beliefs), affective (emotions), and behavioral (concerns about one's appearance) (Laus, 2016). Data on the relationship between the excessive preoccupation with physical appearance, low levels of education, and the search for APS, although uncertain, lead to the hypothesis that the search for APS seems to be associated with the desire to solve conflicts in interpersonal relationships (Sante & Pasian, 2011).
Inadequate perception of body weight, regardless of nutritional status, is associated with the presence of mental disorders and unhealthy behaviors of weight control (Saikali, Soubhia, Scalfaro, & Cordás, 2004). Almeida et al. (2018) pointed out that in the female sex there were more significant distortions in the perception of self-image since women tend to suffer more social pressure to achieve the "perfect body" than men. The study revealed that the overestimation of body image was higher in healthy female adolescents and dissatisfaction with appearance was associated with a higher risk of low weight. Also, De Brito et al. (2010, 2014, 2015, 2016) and Van der Lei and Bouman (2016) described that patients seeking plastic surgery present alterations in BI, self-esteem, mental health, as well as body weight concerns and body dysmorphic disorder symptoms.
Obesity and weight excess are among the situations that can make the individual perceive him/herself as different. Such conditions can be associated with the lack or excess of nutrients that generate an overload to the organism, leading to nutritional imbalance. Every surgical procedure is invasive and causes stress to the body. Regardless of whether it is a minor or minimally invasive procedure or a minor surgery, the nutritional state of the patient is involved, as it will require a demand for several nutrients in the healing process (Suzuki, Fernandez Filha, & Peres, 2013). APS is a specialty that should be concerned not only with the body contour but also with the psychosocial, behavioral, and physiological implications. In this sense, nutritional and psychological support can help the patient and the multidisciplinary team, which, in turn, contributes to surgical success (Segal, Cardinal, & Cordás, 2002).
The justification of this study is based on the need for an analysis of the nutritional status (NS) of the applicants of APS to observe their (in)adequacy for the surgical intervention, mainly to evaluate potential risks and complications due to nutritional deficiencies, as well as the presentation of mental disorders and distortion in BI, which can lead to complications and losses to their general health and expenditures for the Brazilian Unified Health System (Sistema Único de Saúde, SUS) and agreements (complementary medicine). Besides, there are likely to be implications and wear and tear for both the patient and the surgeon, which may interfere with the success of APS and result in exclusion.
The objectives of the study was: 1. to evaluate the BI and NS of women requesting APS (Clinical Group, G1) and non-APS applicants (Comparison Group, G2) an to compare those variables in both groups; 2. to investigate the perceptual and attitudinal components (affective, cognitive, (dis)satisfaction and behaviors) related to BI of women requesting APS (G1) and non-seeking (G2) women; 3. to access in both groups the complete blood count, complete coagulogram, total and HDL cholesterol, routine urine, fasting glycemia, creatinine, albumin, and ferritin to evaluate by means of anthropometric measures (weight and height), body composition (% fat) (A, K, C, E) and minerals (Iron, Zinc, Copper, and Magnesium).
2. Method
2.1 Participants
Participants were randomly selected in two groups: Clinical Group (G1, n = 20), and Comparison Group (G2, n = 20). The sample size took into account the flow of patients from the private clinic where data for the G1 was collected, and the time of data collection destined to the present study.
G1 was composed of adult women, aged between 20 and 59 years, from a private APS clinic. For G2, adult women were recruited from the university community, with the same age and socioeconomic characteristics as G1. The inclusion criteria for G1 were: to be within the stipulated age range, to seek to perform aesthetic surgical procedures (augmentation mammoplasty, liposuction, and/or abdominoplasty), and to be female. G2 was composed by women of the population with the same characteristics of G1 and who had no interest in performing APS in the next two years.
Regarding the exclusion criteria for both groups, the following were highlighted: presenting any apparent physical deficiency that made it impossible for the participants to respond to the instruments applied; have undergone a preoperative aesthetic and postoperative surgical procedure for the Clinical Group (G1). The study was approved by the Human Research Ethics Committee of the Faculty of Philosophy, Sciences and Letters of Ribeirão Preto, University of São Paulo, and the data of both groups were collected in a specialized private Clinic of Ribeirão Preto, in the State of São Paulo, with authorization from the person in charge.
Participants who fulfilled the inclusion criteria of the present study were individually scheduled for the data collection. The women invited to participate in the research were oriented about the nature and objectives of the study as well as the confidential nature of the responses and the need to answer all items with attention and responsibility.
By accepting the Informed Consent Form (ICF), one form was delivered to the participant, and the other was filed by the researchers, who differed between the groups (G1 and G2) so that the information was properly addressed to the participants.
2.2 Materials and instruments
2.2.1 Biochemical Measures
The biochemical measures were conducted in a private laboratory and standard procedures were used to evaluate complete blood count, coagulation time, total cholesterol and HDL, routine urine, fasting glycaemia, creatinine, serum albumin, and ferritin, vitamins (A, K, C, E), and minerals (Iron, Zinc, Copper, and Magnesium), following the reference values (RV) of the Brazilian Society of Clinical Pathology adopted by the Private Laboratory of Clinical Analyzes.
2.2.2 Economic Classification Criteria
The economic classification of the participants was obtained by the Brazilian Economic Classification Criteria (BECC) of the Brazilian Association of Research Companies (2014). The classification is made in classes from A to E with a variation of 0 to 46 points based on the average family income.
2.3 Behavioral Measures
For the measure of the behavioral variables were utilized the following instruments:
2.3.1 Multidimensional Body-Self-Relationships Questionnaire (MBSRQ)
The instrument was developed in 1990 by Brown, Cash, and Mikulka with 34 items, all related to appearance. The instrument was later translated and adapted by Laus (2016), and is now known as the "Multidimensional Questionnaire on Relationships with the Body itself - scales of appearance". It consists of two scales of appearance of the original questionnaire (evaluation of the appearance and orientation of the appearance), plus three subscales (Satisfaction with the areas of the body, Concern about being overweight and self-classifying of weight). The instrument evaluates two dimensions: "Evaluation" and "Orientation" cognitive-behavioral, accessing affective, cognitive, behavioral components, and satisfaction with BI. Regarding the Multidimensional Body-Self Relations Questionnaire-Appearance Scales (MBSRQ-AS) scoring method, it is a self-applied Likert scale instrument that ranges from "Strongly Disagree" (1 point) to "Strongly Agree" (5 points), in which the inverted score was withdrawn in the Brazilian version.
The results of each subscale are derived from the average of its items. The MBSRQ appearance orientation (AO) subscale was not evaluated in the present study since it has the same investment extension in appearance as the motivational salience (MS) of the "Revised Appearance Scheme Inventory." Both indicate how much the individual is engaging in appearance-oriented behaviors to feel more attractive. The following are the subscales, according to Laus (2016):
(i) The subscale evaluation of appearance (EA): evaluates feelings about physical (in)attractiveness and (dis)satisfaction with appearance, being that a high score indicates greater positivity and satisfaction, while low score reflects general unhappiness with physical appearance.
(ii) Appearance orientation (AO): accesses the investment extension in appearance. High results point out that the individual gives great importance, pays more attention to appearance and engages in excessive beauty behaviors; low results indicate that the individual is apathetic about appearance, that is, gives little importance to him/ her and that he/she does not strive to “look good.”
(iii) Body Areas Satisfaction Scale (BASS) is similar to the AE subscale, with the difference that it measures the (dis)satisfaction with the other body areas.
(iv) Concern about Overweight Preoccupation (OWP) reflects anxiety and vigilance of exacerbated weight, with restrictive dieting practices indicating a great concern and anxiety related to fat and overweight.
(v) Self-classification Weight (SCW) is a subscale of a perceptual character that determines the (in)accuracy of the weight perception estimate, from “far below” to “far above” weight.
2.3.2 Appearance Schemas Inventory-Revised (ASI-R)
This instrument was translated and adapted by Laus (2016) for the Brazilian population and it is called "Appearance Inventory Schemes - Revised" (ASI-R), which is a self-scale application that assesses the dysfunctional investment an individual may have with their physical appearance, beliefs about their BI, and how much that may influence their life. Its 20 items are divided into two different, but related, investment forms: 1. appearance evaluation (AE), with 12 items reflecting the intensity with which beliefs about appearance influence the social and personal life of the individual; and 2. the MS, with eight items that relate to the intensity of concern about their appearance and the way they adopt behaviors to control it. In the original instrument, the questions are answered on a Likert scale, consisting of five alternative responses, ranging from "Strongly Disagree" (one point) to "Strongly Agree" (five points). In the original instrument prepared by Cash in 2002, six of the scale items were formulated in the opposite direction to the others and should have their scores inverted. The final score results from the average of the scores obtained in the 20 items of the scale, thus oscillating between one and five, and the higher this result, the higher the levels of investment in the individual's appearance. In the Brazilian version (translated and adapted), the questions are answered in the same way. However, items from the scale with inverted scores were removed, as well as it is not necessary to calculate the final average between the two protrusions, between the items of each subscale.
2.2.6 Anthropometric evaluation
This measure was carried out starting with the measurement of weight and height to obtain a BMI according to World Health Organization (2000), in order to perform the nutritional diagnosis of the participants through Welch® anthropometric mechanical platform scale (capacity 150 kg, accuracy 100 g) previously calibrated for weight gauging and fixed stadiometer (200 cm, precision 0.1 cm) for gauging height. Considering that the BMI does not distinguish the weight associated with muscle or body fat, it was necessary to evaluate the body composition of the individuals for a more reliable evaluation of the NS. Thus, to complement the anthropometric evaluation, the bioimpedance was performed to investigate the body composition of the participants, according to Lohman (1992). For its evaluation, the portable electric bioimpedance, brand Inbody 230®, was used to measure the body composition of lean mass and segmented fat, separately, in addition to total body water, basal metabolic rate, nutritional diagnosis, muscle-fat control, expenditure energy intake, and recommended caloric intake per day.
3. Procedure
The application of the instruments for both groups G1 and G2 occurred in fitting rooms, which allowed the privacy of the interviewee, located in the physical space of the medical service. Since G1 participants were evaluated in the preoperative period after the surgeon's request for examination, approximately 30 days before the APS, firstly, the questionnaire was used to characterize the sample created by the researchers, which consisted of three sections related to the Sociodemographic data (age, marital status, schooling, among others); clinical data, with questions directed and similar to the G1 and G2 groups, e.g., in the case of G1, questions prior to the surgical procedure related to the type(s) of surgical procedure(s) and expectations; performance of diets, use of medications for weight loss and /or weight control - with or without nutritional counseling; psychological counseling /use of psychotropic medication.
During the preoperative consultation for the combination of the surgery, the surgeon requested biochemical tests (blood and routine urine) for G1 participants, according to the protocol adopted by the clinic. The objective of these tests was to evaluate the clinical (general condition) and nutritional conditions of the participants, in order to see if they were able to perform APS, comparing them with G2; however, it is emphasized that for the G2 the researchers requested the exams. The patients went to the private laboratory previously stipulated by the researchers, where they underwent the laboratory tests, funded by the private health plan of each participant of the clinical group (G1), and for the group of Comparison no equivalent (G2) was funded by the Laboratory of Nutrition and Behavior, FFCLRP /USP. Complete blood count, coagulation time, total cholesterol and HDL, routine urine, fasting glycemia, creatinine, serum albumin, and ferritin, vitamins (A, K, C, E), and minerals (Iron, Zinc, Copper, and Magnesium) were evaluated.
3.1 Data analysis
Descriptive and comparative statistical tests analyzed the results for the instruments (ASI-R and MBSRQ-AS Scales). The association between the groups in the qualitative variables was based on Fisher's Exact Test. For the comparison of the quantitative cut-off (ASI-R and MBSRQ-AS Scales), the Mann-Whitney Test was used. In both comparisons, a significance level of 5% was established. All analyses were performed using SAS 9.2 software.
4. Results
Regarding the results of the characterization of the sample, the clinical group (G1) consisted of 20 participants (19 autonomous professionals and one from the university), who requested APS to perform the following procedures: augmentation mammoplasty (30%, n = 6), mammoplasty of increase and liposuction (5%, n = 1), abdominoplasty (10%, n = 2); liposuction (10%, n = 5).
Participants in the non-equivalent comparison group (G2) were randomly recruited, consisting of professionals (with full tertiary education), five undergraduates, and a salaried female worker with high school education. They did not seek in the past or had an interest in performing aesthetic surgical procedures in the next two years. The G1 participants had a mean age of 35.85 years (SD ± 10.89), while the G2 participants had a mean age of 34.00 years (SD ± 10.67). Regarding marital status, G1 participants were single (55%), while in G2 there were 50% of single, belonging to class A (50%) and B (50%) in G1, and class A (60%) and B (40%) in G2, according to BECC, and they had completed higher education (95% in both groups). Regarding the use of weight loss drugs and/or supplements, 90% stated that they did not use, with any statistical difference between groups (p = 0.14). Almost half of the participants from G1 (45%) were under psychotherapeutic treatment, while only 5% in G2 had the same condition, which indicated a significant difference between the groups (p < 0.01). As for the use of psychotropic drugs, the prevalence of consumption among G1 participants was 40%, and 5% in G2 with a statistical difference, that is, G1 > G2 (p = 0.02), (Table 4.1).
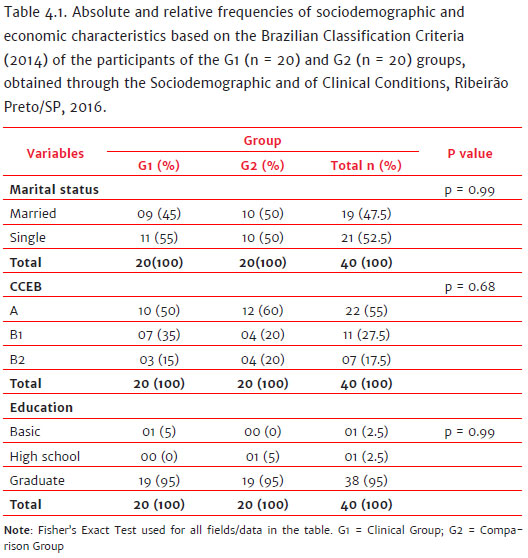
Table 4.2 shows the descriptive statistical results (mean, standard deviation, minimum, median, and maximum) of the variables of the groups G1 and G2 (height, BMI, fat percentage, and desire to lose weight). It was verified that in the G1 group 5% of the women (n = 1) were on the average weight; 15% (n = 3) were above the average weight, and 50% (n = 10) were obese. Concerning the participants of the G2 group, none of them were within the normal range; 50% (n = 10) were above the average weight, and 50% (n = 10) were obese. There was a statistical difference between the groups (p = 0.04). Regarding the classification of body fat composition (Lohman, 1992), it was found that in G1 95% of the women were above average body fat and obese, and in G2 none of them were within the normal range of body fat, since 50% were above average body fat and 50% were obese, with a statistical difference between the groups (p = 0.04).
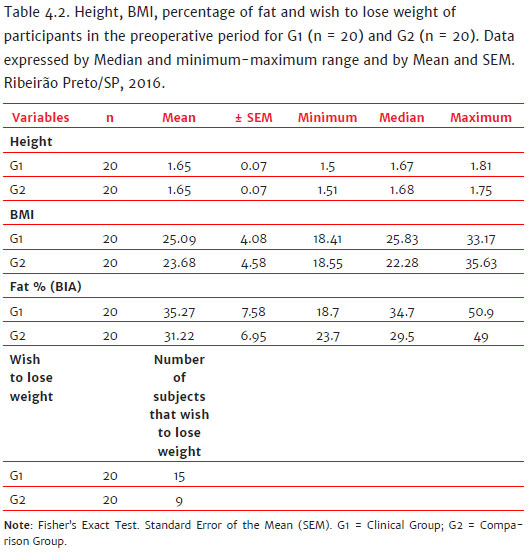
In summary, according to the descriptive statistical results (mean ± standard error of the mean - SEM), the following variables were highlighted: the IMC showed values of 25.09 ± 4.08 in G1 and 23.68 ± 4.58 in G2; the percentage of fat showed values of 35.27 ± 7.58 for G1 and 31,22 ± 6,95 in G2; regarding the MBSRQ-R it was shown in the G1 group 75% (n = 15) would like to lose weight, while 25% (n = 5) did not respond; in G2, 45% (n = 9) would like to lose weight, while 55% (n = 11) did not respond.
Regarding the characterization of the BI, a greater time of dissatisfaction with the appearance was reported by the participants in G1 (n = 15) in relation to G2 (n = 9), since 75% of the participants of G1 and only 45% of the participants of G2 groups had dissatisfactions as early as the childhood/adolescence ages (p = 0,04).
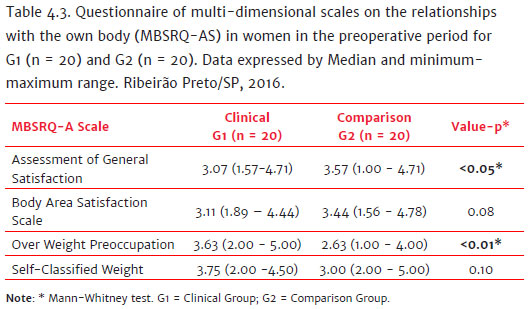
For the MBSRQ-AS Questionnaire divided into four subscales, it was observed significant statistical differences between the two groups in OWP, with G1 showing more preoccupation (p < 0.01), and in Assessment General Satisfaction (AGS), with G2 showing more satisfaction (p < 0.05). There were no differences between groups in the other two subscales (Table 4.3).
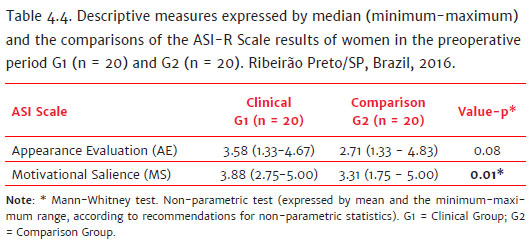
The results of the ASI-R instrument are shown in Table 4.4. Considering self-evaluating and motivational Salience of the ASI-R, a significant statistical difference was found in the motivational salience (p = 0.01). Such a salience measures the degree of investment and cares with its appearance, showing more investment in the G1 group.
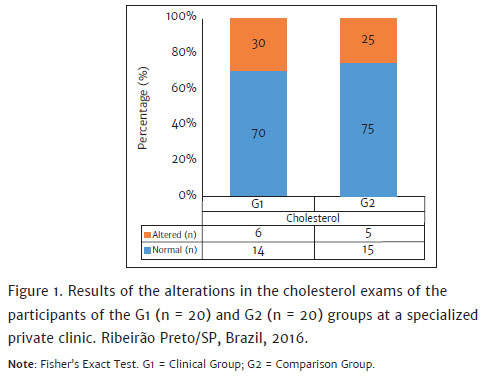
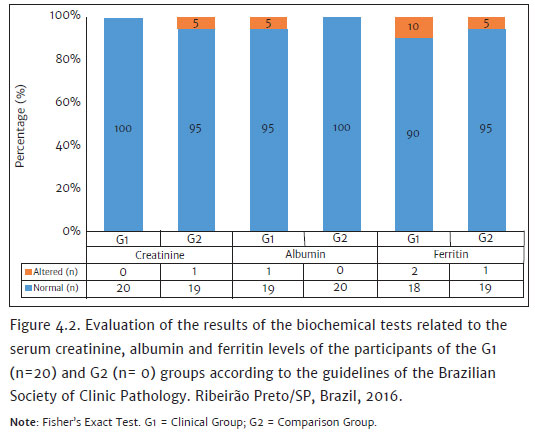
No significant differences were found between groups on the laboratory blood tests (blood count, coagulogram, lipidogram, fasting glucose, albumin, creatine, and circulating ferritin) (Figures 4.1 and 4.2).
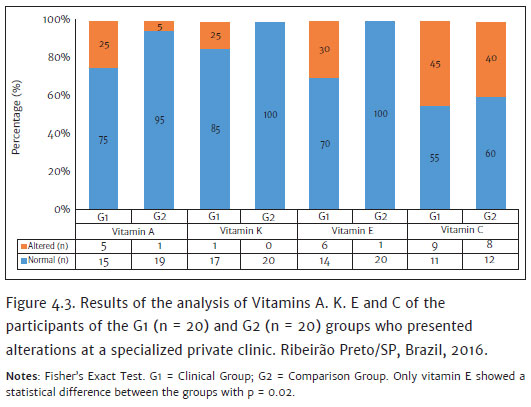
In particular, a significant statistical difference was found between the G1 and G2 groups for vitamin E (p = 0.02) with a deficiency in 30% of the G1 participants, whereas, in G2, 100% were within the normal range. The results of the other vitamins did not show any differences between the groups (Figure 4.3).
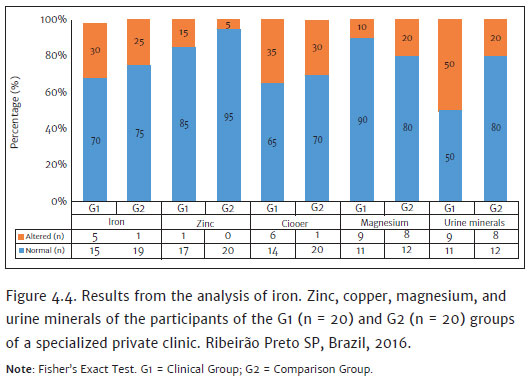
No significant differences were observed in the analysis of iron, zinc, copper, magnesium, and urine minerals (Figure 4.4).
5. Discussion
The objective of the study was to evaluate the BI and NS of women requesting or not APS to investigate the perceptual and attitudinal components (affective, cognitive, and (dis)satisfaction behaviors).
Before discussing the main data, it is important to inform that the socioeconomic and age profiles of the participants of the present study are similar to the profile shown by previously reported studies (Sante & Pasian, 2011; Mota, 2016).
Laus (2016) hypothesizes that single men and women value and invest more in their appearance in order to become more attractive in search of loving relationships. Still, in the sample characterization questionnaire, it was identified that G1 was dissatisfied since childhood and adolescence, which did not occur in the Mota (2016) study, that found 65% of women requesting APS who were dissatisfied with their appearance since early adulthood. Also, the search for aesthetic procedures and dysfunctional behaviors that put health at risk is related to the level and precocity of dissatisfaction with BI (Mota, 2016).
Women are more dissatisfied and jealous than men because they are more concerned with appearance and weight (Kakeshita & Almeida, 2006). In a situation of inadequate BMI, they adopt unhealthy attitudes and behaviors for the control of weight. These strategies are related to sociocultural aspects, being overweight favors inaccurate estimation and dissatisfaction with appearance (Kakeshita & Almeida, 2006).
The global study on the real truth about beauty, conducted by Etcoff, Orbach, Scott, & D'Agostino (2004) at Harvard University with 3200 women from nine countries (USA, Canada, Britain, Italy, France, Portugal, Brazil, Argentina, and Japan) in the age group 18-64 showed the following results: In Brazil, only 6% of women considered themselves beautiful and believed that beauty generates more opportunities for success in life and 54% believe in APS as a strategy to increase attractiveness, 7% have already performed APS, and it was found the highest percentage of APS acceptance among the countries studied, in addition to the per capita consumption of drugs for weight loss. These data corroborate with the results found in this research, regarding the dissatisfaction with BI among women as a global epidemic, regardless of whether they are applicants (or not) for APS.
Regarding the Nutritional status of the clinical group, G1 participants were overweight and obese, similar to what was found in the WHO Global Report (2000), which indicated 52.80% of overweight adult women (over 18 years), according to the BMI (kg/m2), indicating a global public health problem (Pan America Health Organization, 2016). Another Brazilian study (Garcia, Ferreira, Schneider, & Simeão Júnior, 2013) also evaluated the NS through a Questionnaire (with food frequency) and 24-hour reminder application in 26 patients in a specialized private clinic in Ribeirão Preto, in the State of São Paulo, emphasizing the public health problem of obesity. They found that 61.54% of the participants were eutrophic, 27% had grade I obesity, and 11.50% had grade II obesity. They concluded that although the participants were more concerned with the aesthetic standards of the body and were eutrophic, they indicated nutritional deficiencies and caloric intake below their needs. Thus, the results of the study reinforce the importance of an adequate intake of the energy and nutrient needs essential to contribute to the healing process and to avoid future complications in the postoperative period.
Obesity is a pro-inflammatory pathology, due to the excess of adipocyte cells that release inflammatory mediators (Azevedo & Pujol, 2011), so the correlation between APS and obesity can lead to problems in healing and increased susceptibility to inflammation (Chen, Karri, Chung, & Yang, 2010). Therefore, the need for an accurate evaluation of the nutritional status to ensure a good evolution in the perioperative period is emphasized.
Although no significant difference was found between groups in the biochemical analysis except vitamin E, there were biochemical parameters that showed changes in G1. These patients may indicate a greater predisposition to possible future complications that may impair the final surgical result and result in an unsatisfactory result. One hypothesis for this finding is that there may have been a low intake of vitamin E sources or even some malabsorption problem.
In this context, biochemical tests are essential for patients who seek APS to avoid possible future surgery complications. Biochemical evaluation can function as a tool for an assessment of nutritional deficiencies, obesity, and other diseases (Oliveira et al., 2012).
6. Conclusions
Research that encompasses APS and multidimensionality of BI is still limited, if not scarce, in Brazil and the world. The main limitation of the present study was the impossibility to compare the specific biochemical results of the present study with data from other researchers since it was not found published studies in the APS area. In the same way, it was not found published studies comparing biochemical data with body image and nutritional status. The literature had shown that biochemical exams are requested only in studies of bariatric surgery. Thus, future studies in this area are highly needed.
However, the studies are fundamental for the development of strategies that promote global patient care, as well as improving the quality of life, physical and mental well-being and optimizing the final APS result. The first and most important step of the nutritional education with the dietitian, simultaneously with the psychotherapeutic follow-up is the behavioral change, only possible through self-knowledge, changing beliefs and attitudes. It is also need to address the anxiety and suffering that women submit to achieving unrealistic goals. It is also important to point out that individuals with chronic diseases (CDs) seeking APS, however, require more care and evaluation, precisely because of the potential risk of perioperative complications, related to nutritional deficiencies and tissue hypoxemia that hamper recovery and healing of the individual.
In this sense, we highlight the importance of the dietitian to perform a clinical and nutritional evaluation, as well as the request of biochemical tests for a more careful investigation: from previous laboratory tests (and actuals), anamnesis and the patient history that may contribute to the definition of the prognosis.
This scenario also reinforces the importance of primary cares constituted by the surgeon physician, clinical dentist, and psychologist, who holds the knowledge of cognitive-behavioral therapy to detect and minimize dysfunctional behaviors, simultaneously restoring and ensuring satisfactory aesthetic results.
References
Associação Brasileira de Empresas de Pesquisa - ABEP. (2007). O novo critério padrão de classificação econômica Brasil. São Paulo: ABEP. Retrieved from http://www.abep.org/criterio-brasil [ Links ]
Almeida, C. A. N., Garzella, R. C., Natera, C. C., Almeida, A. C. F., Ferraz, I. S., & Del Ciampo, L. A. (2018). Body image self-perception distortion in teenagers. International Journal of Nutrology, 11(2),61-65. doi:10.1055/s-0038-1669407 [ Links ]
Avelar, C. F. P. (2011). Personality and propensity to cosmetic plastic surgery (Unpublished Master's Dissertation). Federal University of Minas Gerais, Belo Horizonte, Brazil. [ Links ]
Azevedo, A. L. G., & Pujol, A. P. (2011). Chronic inflammation and aesthetic disorders. In Pujol, A. P. P. (Org.), Nutrition applied to aesthetics. (pp. 21-34). Rio de Janeiro: Rubio. [ Links ]
Brown, T. A., Cash, T. F., & Mikulka P. J. (1990). Attitudinal body-image assessment: factor analysis of the Body-Self Relations Questionnaire. Journal of Personality Assessment, 55(1-2),135-144. [ Links ]
Cash, T. F. (2002). Cognitive-behavioral perspectives on body image. In T. F. Cash & T. Pruzinsky (Eds.), Body image: a handbook of theory, research, and clinical practice (pp. 38-46). New York: The Guilford Press. [ Links ]
Cash, T. F. (2011). Cognitive-Behavioral Perspectives on Body Image. In Cash T. F. & Smolak L. (Eds.), Body image:A handbook of science, practice and prevention. (pp. 39-47). New York: Guilford Press. [ Links ]
Chen, H. C., Karri, V., Chung, K. P., & Yang, M. C. (2010). Psychological profile of Taiwanese female cosmetic surgery candidates: Understanding their motivation for cosmetic surgery. Aesthetic Plastic Surgery, 34(3),340-349. doi:10.1007/s00266-009-9461-6 [ Links ]
Damasceno, V. O., Vianna, V. R. A., Vianna, J. M., Lacio, M., Lima, J. R. P., & Novaes, J. S. (2006). Body image and ideal body. Revista Brasileira de Ciência e Movimento, 14(2)87-96. [ Links ]
De Brito, M. J. A., Nahas, F. X., Barbosa, M. V., Dini, G. M., Kimura, A. K., Farah, A. B., & Ferreira, L. M. (2010). Abdominoplasty and its effect on body image, self-esteem, and mental health. Annals of Plastic Surgery, 65(1),5-10. doi:10.1097/SAP.0b013e3181bc30f7 [ Links ]
De Brito, M. J. A., Nahas, F. X., Córdas, T. A., Felix, G. A. A, Sabino Neto, M., & Ferreira, L. M. (2014). Compreendendo a psicopatologia do transtorno dismórfico corporal de pacientes de cirurgia plástica: Resumo da literatura. Revista Brasileira de Cirurgia Plástica, 29(4),599-608. doi:10.5935/2177-1235.2014RBCP0106 [ Links ]
De Brito, M. J. A., Felix, G. A. A., Nahas, F. X., Tavares, H., Cordás, T. A., Dini, G. M., & Ferreira, L. M. (2015). Body dysmorphic disorder should not be considered an exclusion criterion for cosmetic surgery. Journal of Plastic, Reconstructive & Aesthetic Surgery, 68(2),270-272. doi:10.1016/j.bjps.2014.09.046 [ Links ]
De Brito, M. J. A., Nahas, F. X., Cordás, T. A., Gasma, M. G., Sucupira, E. R., Ramos, T. D. ... Ferreira, L. M. (2016). Prevalence of body dysmorphic disorder symptoms and body weight concerns in patients seeking abdominoplasty. Aesthetic Surgery Journal, 36(3),324-332. doi:10.1093/asj/sjv213 [ Links ]
Etcoff, N., Orbach, S., Scott, J., & D'Agostino, H. (2004). The real truth about beauty: A global report: Findings of the global study on women, beauty and well-being. Retrieved from http://www.clubofamsterdam.com/contentarticles/52%20Beauty/dove_white_paper_final.pdf [ Links ]
Garcia, A. F. E., Ferreira, L.G.M., Schneider, A.P., & Simeão Júnior, C.A. (2013). A inadequação de macro e micronutrientes da dieta de pacientes no pós-operatório submetidos às cirurgias plásticas. Revista Médica Electrónica de Portales Medicos.com, 8(8),1-6. [ Links ]
Kakeshita, I. S., & Almeida, S. S. (2006). Relationship between body mass index and the perception of self-image in university students. Revista de Saúde Pública, 40(3),497-504. doi:10.1590/S0034-89102006000300019 [ Links ]
Laus, M. F. (2016). Dysfunctional psychological investment in appearance: Would love relationships be protective factors? (Unpublished Postdoctoral Report). University of São Paulo, Ribeirão Preto, Brazil. [ Links ]
Laus, M. F., Straatman, G., Kakeshita, I. S., Braga Costa, T. M., & Almeida, S. S. (2013). The influence of body image on eating behavior. In Almeida S. S., Braga Costa T. M., Straatman G. & Laus M. F. (Orgs.), Psychobiology of Eating Behavior (pp. 103-118). Rio de Janeiro: Rubio. [ Links ]
Lohman, T. G. (1992). Assessing fat distribution. In Lohman T. G. Advances in body composition assessment. Current issues in exercise science series. (pp. 57-63). Illinois: Human Kinetics Champaign. [ Links ]
Mota, D. C. L. (2016). Body image, food attitudes and nutritional status of women submitted to aesthetic plastic surgery. (Unpublished Thesis). University of São Paulo, Ribeirão Preto, Brazil. [ Links ]
Oliveira, M. R., Fontes, G. G., Lima, L. M., Gomes, A. P., Vieira, P. A. F., & Siqueira-Baptista, R. (2012). Avaliação Bioquímica do Sangue. Interpretação de exames laboratoriais aplicados à nutrição clínica. In L. Calixto-Lima & N. T. Reis (Orgs.), Interpretação de testes laboratoriais aplicados a nutrição clínica (pp. 19-37). Rio de Janeiro: Rubio. [ Links ]
Pan America Health Organization. (2016). Overweight in adults by sex in countries of the Americas. Retrieved from http://www.paho.org/hq/index.php?option=com_content&view=article&id=12695&Itemid=41164&lang=en [ Links ]
Saikali, C. J., Soubhia, C. S., Scalfaro, B. M., & Cordás, T. A. (2004). Body image in eating disorders. Journal of Clinical Psychiatry, 31(4),164-166. [ Links ]
Sante, A. B., & Pasian, S. R. (2011). Body Image and personality characteristics of women applying for aesthetic plastic surgery. Psicologia: Reflexão e Crítica, 24(3),421-429. doi:10.1590/S0102-79722011000300003 [ Links ]
Segal, A., Cardinal, M.V., & Cordás, T.A. (2002). Psychosocial and psychotherapeutic aspects of obesity. Journal of Clinical Psychiatry, 29(2)81-89. [ Links ]
Sociedade Brasileira de Cirurgia Plástica (2017). Censo 2016: Situação da cirurgia plástica no Brasil: Análise comparativa das pesquisas 2014 e 2016. Retrieved from http://www2.cirurgiaplastica.org.br/wp-content/uploads/2017/12/CENSO-2017.pdf [ Links ]
Suzuki, V. Y., Fernandez Filha, I. C. A. A. H., & Peres, I. S. (2013). Performance of the Dietist in Plastic Surgery. In V.Y. Suzuki & A. P. Schneider (Orgs.), Nutritional care in plastic surgery, a multidisciplinary approach. (pp. 1-10). Rio de Janeiro: Rubio. [ Links ]
Van der Lei, B., & Bouman, T. K. (2016). Body dysmorphic disorder in patients seeking abdominoplasty, rhinoplasty, and rhytidectomy. Plastic and Reconstructive Surgery, 138(3),553e-554e. [ Links ]
World Health Organization. (2000). Obesity-Preventing and Managing the Global Epidemic. Report of a WHO consultation on obesity. Geneva: WHO. (Technical Report Series, No. 894). [ Links ]
 Mailling address:
Mailling address:
Sebastião Sousa Almeida
Faculdade de Filosofia, Ciências e Letras de Ribeirão Preto (FFCLRP-USP)
Avenida dos Bandeirantes, 3900, Campus USP
Ribeirão Preto, SP, Brazil. CEP 14040-901
E-mail: sebasalm@usp.br
Submission: 06/09/2018
Acceptance: 15/04/2019

