










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkPsicologia: teoria e prática
versão impressa ISSN 1516-3687
Psicol. teor. prat. vol.22 no.1 São Paulo jan./abr. 2020
https://doi.org/10.5935/1980-6906/psicologia.v22n1p144-160
ARTICLES
HUMAN DEVELOPMENT
Associations between maternal responsiveness due to the number of offspring and motor development
Associações entre responsividade materna em função da prole e desenvolvimento motor
Paula Cristina S. Mesquita ; Daniela D. Siqueira; Marilice F. Garotti; Ivete F. R. Caldas
; Daniela D. Siqueira; Marilice F. Garotti; Ivete F. R. Caldas
Federal University of Pará (UFPA), Belém, PA, Brazil
ABSTRACT
Maternal responsiveness (MR) is a predictor of the acquisition of motor skills by premature infants. This study aimed to verify associations between MR due to the number of offspring and motor development (MD) in preterm infants. Eighteen dyads participated in this study, divided into three groups: primiparous mothers with twin newborns (PMT), primiparous mothers (PM), and multiparous mothers (MM). Medical Records, the Social Interaction Scale (SIS), and a Motor Development Observation Protocol were used. In the Adaptive Fine Motor Development (AFMD), the PMT group presented more frequent "normal" outcomes (5; 83.3%), with a mean score of 13.2 points in the SIS (p < 0.0001). For those that evolved with "risk," in both AFMD and gross motor development (GMD), the MM group stood out (4; 66.7%), presenting a mean SIS score of 12.1 (p < 0.0001). The MR quality as a function of the offspring number is associated with AFMD and GMD of premature infants in the first year of life.
Keywords: development; preterm babies; maternal responsiveness; parity; motor development.
RESUMO
A responsividade materna (RM) é um preditor da aquisição de habilidades motoras de prematuros. O objetivo deste estudo foi verificar associações entre a RM e o desenvolvimento motor (DM) de prematuros em função do tamanho da prole. Participaram 18 díades, distribuídas em três grupos: mães primíparas e neonatos gemelares (MPG), mães primíparas (MP) e mães multíparas (MM). Utilizaram-se ficha clínica, Escala de Interação Social (EIS) e Protocolo de Observação do DM. No desenvolvimento motor fino adaptativo (DMFA), o grupo MPG apresentou desfecho "normal" mais frequente (5; 83,3%), com escore 13,2 pontos na EIS (p < 0,0001). Entre aqueles que evoluíram com "risco" tanto no DMFA quanto no desenvolvimento motor grosseiro (DMG), o grupo de MM se destacou (4; 66,7%), apresentando escore de 12,1 (p < 0,0001). A qualidade da RM mostrou estar associada com o DMFA e DMG de prematuros no primeiro ano de vida, em função do tamanho da prole.
Palavras chave: Desenvolvimento; prematuro; responsividade materna; paridade; desenvolvimento motor.
1. Introduction
According to the World Health Organization, it is estimated that around 30 million premature (< 37 weeks) and/or underweight (< 2,500 grams) babies are born annually worldwide. These are at increased risk of morbidity when compared to full-term infants, including cognitive (Schadl et al., 2018) and motor (Thomas, Lacadie, Vohr, Ment, & Scheinost, 2017) changes. One study showed that between 30 and 50% of premature births present motor, cognitive, and behavioral changes (Caldas, Garotti, Shiramizu, & Pereira, 2018).
From this perspective, the quantity and quality of motor skills provide information on the integrity of organ systems. They are considered important indicators for monitoring the physical and mental health of premature infants. These often present alterations in gross, fine, and perceptual-motor skills due to cerebral and musculoskeletal immaturity (Bos, Braeckel, Hitzert, Tanis, & Roze, 2013). As a result, they are slower to develop motor skills such as rolling, sitting, crawling, standing, and walking (Formiga, Vieira, & Linhares, 2015).
Also, other factors may influence the premature infant's motor development, including the quality of the early mother-infant relationship (Feldman, Rosenthal, & Eidelman, 2014; Caldas et al., 2018). Variations in the quality of the attachment are associated with personality differences identified later in life. A key component of this relationship is maternal responsiveness (MR), or the mother's ability to detect and respond to the baby's behavioral signals. Mothers and babies have a perceptual and behavioral predisposition to engage in interactions that promote the attachment (Feldman et al., 2014).
However, clinical conditions of infants, such as prematurity, may present challenges for interactions between mothers and children (Caldas et al., 2018). Maternal interactions with premature babies are less effective than interactions with full-term infants (Zuccarini et al., 2016). Long periods of hospitalization directly influence this relationship, and the development of these preterm infants may become compromised due to the restricted mother-infant interactions (Shah, Robbins, Coelho, & Poehlmann, 2013). The presence of maternal anxiety during prolonged hospitalizations results in less effective maternal behavior during interactions with their children in the first months of life (Feldman et al., 2014).
Because MR also depends on maternal cognitive resources, attention, and care become limited when the demand is extensive and should be given to one person at a time to be considered ideal. This challenge to MR may be present in other contexts associated with the mother's reproductive experience, or parity (Fish & Stifter, 1993), such as mothers of twins and multiparous mothers. The environment of a twin (or triplet) baby differs in many ways from that of a single baby. From the beginning, the twins share maternal attention and communicate in a trio. This can be difficult for both the babies and the mother. Lack of time and factors, such as security, also tend to deprive them of many stimulating opportunities (Bryan, 2003; Lucion & Escosteguy, 2011). One study showed that mothers of premature twins presented fewer initiatives and responses to their children, and were less sensitive to their positive signs and crying (Ostfeld, Smith, Hiatt, & Hegyi, 2000). In the case of multiparous mothers, maternal behavior starts to be influenced by the arrival of another child. Accordingly, those children who already had the mother-child interaction routine adjusted, whether or not they were the only child, suddenly have to divide the mother's attention with the new family member (Fish & Stifter, 1993).
Accordingly, the severe breakdown of the mother-infant interaction is a catastrophic event for the baby and its family members, especially for those infants born prematurely, and it may lead to delays in brain development and increased risk for motor and cognitive impairment (Schadl et al., 2018). Therefore, motor development deserves special attention, since changes in motor skills can be identified earlier, allowing early intervention (Bos et al., 2013). These changes can also impact the social and emotional development of premature infants (Formiga et al., 2015).
Babies may, however, develop adaptive behavioral strategies to deal with potential impairments during interactions with the caregiver. They can learn to develop new ways of interacting with their mother, increasing their skills-coping repertoire, allowing them to recover from disappointment and gain confidence in their problem-solving skills (Morton, 2016). Although this behavior has a high cost in terms of increasing the risk of future behavioral changes, it is a striking example of self-preservation at such a vulnerable stage of human development (Caldas et al., 2018). Accordingly, in order to contribute to a better understanding of the impact of maternal behavior on the motor development of preterm infants, the present study aimed to verify associations between MR as a function of the number of offspring and the motor development (MD) of preterm infants.
2. Method
2.1 Participants
This was a cross-sectional study with a convenience sample. The newborns were born and hospitalized in the Neonatal Intensive Care Unit (NICU) of a private hospital, located in the city of Belém, in the state of Pará. Of the 17 mothers with premature neonates born between August and November 2012, two were excluded: one of them because she did not attend more than one session and the other due to the death of the infant. Thus, 15 mothers participated in the study, three being mothers of twins, and 18 premature newborns, with gestational age (GA) <36 6/7 weeks and birth weight (BW) <2,500 grams. Mothers diagnosed with psychiatric disorders, who lived outside the municipality of Belém, Pará, and those that refused to sign the consent form were excluded, as they were the neonates with congenital malformations, genetic syndromes detected in the neonatal period and those born in or transferred from other institutions. The study was approved by the Research Ethics Committee (Authorization No. 176.898).
The 18 dyads were divided into three groups with six dyads each, delimited according to the gestational characteristics and order of birth of the newborn into the family. The first group (three mothers and six neonates) was composed of primiparous mothers with twin newborns (PMT), the second by primiparous mothers (PM), and the third by multiparous mothers (MM), in this group, all the participants were the third and latest offspring.
2.2 Instruments
The following were used to collect the data:
Medical Records for obtaining gestational information related to the mothers (obstetric diseases, complications during the birth, number of pregnancies, type of delivery and prenatal care), the newborns (birth weight, gestational age, Apgar score, and gender) and postnatal data (need for ventilatory support, phototherapy, and presence of neonatal complications).
Social Interaction Scale (SIS) to assess caregiver responsiveness in six dimensions (level of affection, maintenance of interaction, directivity, contingency, initiation, level of movement/participation). Each dimension was scored by the researcher according to a Likert-type scale (1, 1.5, 2, 2.5, 3 points). According to the final score, which corresponded to the sum of the scores assigned to each dimension, the interactions could be classified as "Poor" (6-10 points), "Good" (10.5-14.5 points) and "Excellent" (15-18 points), published in full by Ruble, McDuffie, King, and Lorenz (2008).
Motor Development Observation Protocol (MDOP): this was based on the Denver Developmental Screening Test II (DDST-II) manual, which covers ages from zero to six years. The Test is made up of 125 tasks, subdivided into four areas: social-personal, language, fine, and gross motor (Frankenburg, Dodds, Acher, Shapiro, & Bresnick, 1992). For the present study, only the results regarding the motor areas were analyzed and discussed, due to the high prevalence of motor skill changes in premature infants with suspected developmental delay (Thomas et al., 2017).
In the area of Adaptive Fine Motor Development (AFMD) the motor skills evaluated were: follows to midline, follows past midline, grasps a rattle, hands together, follows 180°, regards for small object, reaches for small object, searches for the object, picks up the small object, passes an object, picks up two objects, thumb-finger grasp, beats two objects together in the hands, and places object in deep container. In the area of Gross Motor Development (GMD) the skills evaluated were: symmetrical movements, lifts head, head up 45°, head up 90°, sits head steady, bears weight on legs, chest up arm support, changes position, pull to sit holding head steady, sits without support, stands holding on, pulls to stand, sits, stands.
After the evaluation, the children were classified according to their performance: "Normal" when there was no delay or at most one caution in at least one area; "Risk" for two or more cautions and/or a delay in at least one area and "Delay" when two or more delay items were obtained, indicating that the child is highly suspected of developmental impairment (Frankenburg et al., 1992).
2.3 Procedures
After clarifying the purpose of the research and signing the consent form, a schedule of sessions was established throughout the first year of life. The sessions occurred quarterly at three, six, nine, and twelve months of age (Chronological Age). However, because the sample consisted of premature infants, it was necessary to calculate the Gestationally Corrected Age (GCA), which aimed to adjust the development of children for each age recorded. Thus, the GCA corresponded, on average, to one, four, seven, and ten months, respectively.
The sessions developed were semi-structured, performed during the daytime, and recorded on video by a trained scientific initiation student. The sessions were held in an office at the same hospital where the preterm infants were born during the preterm follow-up consultation, and, depending on the child's age, different toys were selected.
Each session lasted thirty minutes, divided into three stages of 10 minutes each. In the first one, the dyad was welcomed, and the information and clinical events that had occurred in the previous quarter were registered; in the second one, the mothers were asked to interact freely with their children; and in the last session, it was the experimenter that interacted. In this study, the final six minutes of the video referring to the mother-baby free interaction period were analyzed, in order to assess the maternal responsiveness, and also the ten minutes of the baby-experimenter interaction period, to assess the children's motor development. A pilot project was conducted with three applications of each instrument, which allowed the conditions of the study to be reproduced and the research team to be trained. Two trained evaluators analyzed the videos to calculate the concordance index regarding the mother and child behaviors.
2.4 Data Analysis
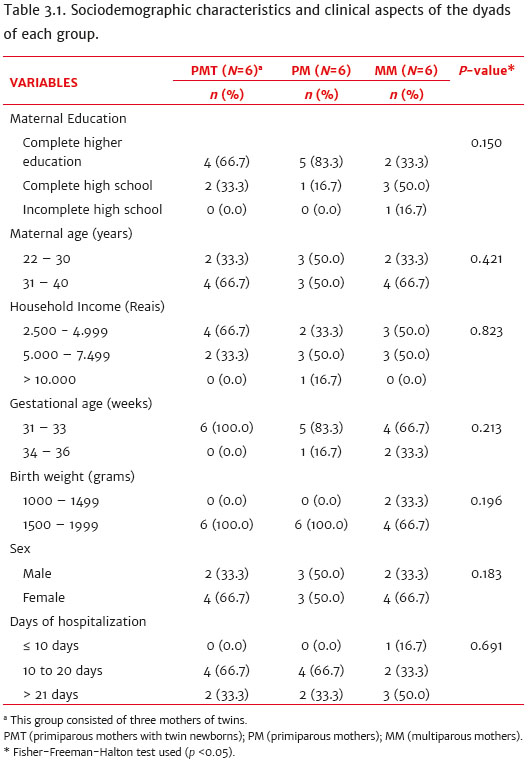
For the statistical analysis, the Statistical Package for the Social Sciences (SPSS) version 22.0 was used. Maternal and neonatal variables were described by frequency and percentage (Table 3.1). These variables were compared between groups using the Fisher-Freeman-Halton test. Pearson's chi-square nonparametric test was also applied to verify the possible relationship between the results of the Social Interaction Scale (SIS) and the Motor Development Observation Protocol (MDOP). A significance level of p <0.05 was considered.
The concordance index between two previously trained independent observers was calculated based on 35% of the total sessions. This concordance was calculated for the categories analyzed by dividing the concordances (C) by the total of possibilities (agreements plus disagreements) in all sessions and multiplying them by 100 (C/A+Dx100). The concordance index was 85% for the maternal responsiveness score results, 83% for the adaptive fine motor development, and 87% for the gross motor development.
3. Results
Table 3.1 presents the sociodemographic characteristics and clinical aspects of the dyads of each group. Concerning maternal education, 5 (83.3%) of the primiparous mothers (PM) group had completed a higher education course, and 4 (66.7%) of the primiparous mothers with twin newborns (PMT) group had a family income between 2,500.00 BRL and 4,999.00 BRL. Regarding gestational age, 6 (100%) of the mothers of the PMT group had their children between 31-33 weeks, 2 (33.3%) of the children of the multiparous mothers (MM) group were born weighing between 1,000 and 1,499 grams, and 3 (50.0%) remained hospitalized for more than 21 days.
The responsiveness level of the mothers was evaluated using the Social Interaction Scale (SIS). Figure 3.2 shows the mothers' scores in the SIS for each group throughout the ages. The PM group stood out in relation to the other groups, maintaining an "excellent" level (15.0-18.0 points) in all sessions, except at one month of corrected age that was rated "good" (10.5-15.5 points). The PMT group showed a reduction in the SIS score at ten months, reaching a "poor" level (6.0 10.0 points). The mean SIS score was 15.9 points for the PM group, 13.2 for the PMT group, and 12.1 for MM.
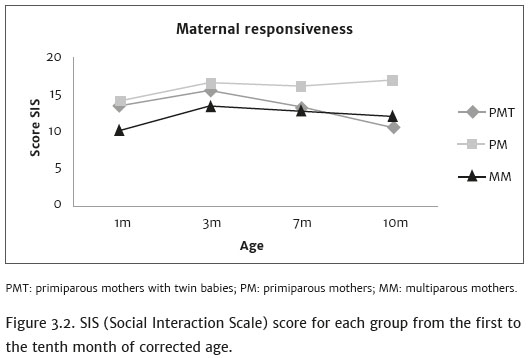
Figure 3.3 shows the mean SIS score, the frequency, and percentage related to the motor development outcome (overall, adaptive fine, and gross) for each group at the end of the first year of life. There was a significant correlation between maternal responsiveness (MR) and the overall motor development of the children (p <0.0001). The PMT group stood out (3; 50.0%) regarding the children that evolved with normal motor development, with the mothers presenting a mean score of 13.2 points in the SIS (p = 0.0002). However, the MM group stood out regarding children with delayed outcomes (4; 66.7%), with the mothers achieving a mean score of only 12.1 points (p <0.0001).
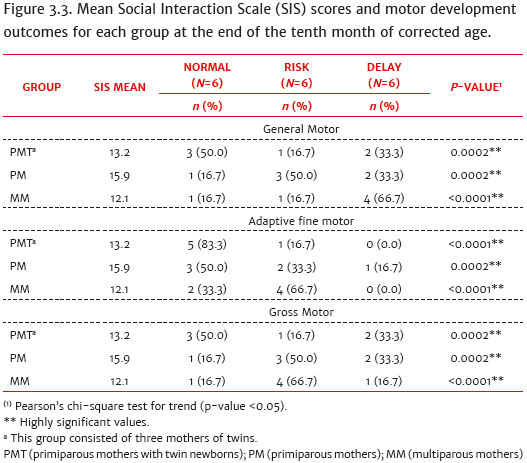
There was also an interaction effect between the MR and adaptive fine motor development (AFMD) (p <0.0001) and gross motor development (GMD) (p <0.0001). The PMT group also presented more children that evolved with normal motor development in both AFMD (5; 83.3%) and GMD (3; 50.0%), with the mothers having a mean score of 13.2 points in the SIS (p <0.0001; p <0.0002). The MM group stood out (4; 66.7%) regarding children with risk outcomes in both AFMD (4; 66.7%) and GMD (4; 66.7%), with the mothers having a mean score of 12.1 points in the SIS (p <0.0001; p <0.0001).
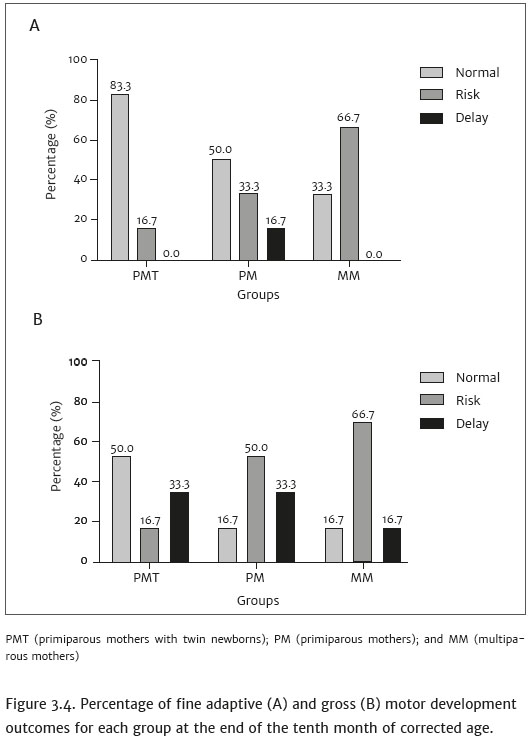
Figure 3.4 shows the percentage of AFMD and GMD outcomes for the children in each group at the end of the first year of life. Regarding AFMD, the majority of the children in the PMT group (83.3%) presented a normal outcome, and only the PM group had a child with a delayed outcome (16.7%). Regarding GMD, all the groups presented children with developmental delay outcomes, with 33.3%, 33.3%, and 16.7% for the PMT, PM, and MM groups, respectively.
4. Discussion
Human beings are slow-growing and have a long period of juvenile dependency that requires a considerable amount of parental investment. Parenting practices, including maternal responsiveness, largely depend on cognitive control and are exercised through executive functions. Cognitive control may be decreased due to executive dysfunction associated with stressful situations (Crandall, Deater-Deckard, & Riley, 2015), such as the presence of a premature baby in the family environment.
From a neurological perspective, the immaturity of the brain makes it difficult for premature newborns to acquire the ability to organize behavioral responses to environmental stimuli and interact with their caregivers (Feldman et al., 2014). Emission of behavioral cues sent to the mother is impaired because they have difficulty remaining alert and are less responsive to signs and sounds. They present significantly less advanced object exploration compared to full-term infants, and they proportionately spend less time manipulating objects and more time organizing an adequate motor response, both when starting the movement of the arm toward the object, as well as reaching for it after the movement (Zuccarini et al., 2016). Accordingly, the pathway may be the other way around, because when faced with a less responsive baby, maternal responses also decrease, causing a negative impact on the MR (Shah et al., 2013).
From this perspective, the attention available to the child also varies according to the focus of maternal attention, whether exclusive or divided with other activities. In the present study, this difference in the quality of maternal responsiveness between the groups can be observed. The group of primiparous mothers stood out during the first year of life by presenting higher scores in the social interaction scale (SIS), which may be justified by the adverse effect of the number of children. The attention available to a single child increases the maternal investment capacity during interactions, unlike mothers with more than one child, who need to divide their focus of attention, reducing this investment (Morton, 2016; Feldman et al., 2014). The presence of several young children at the same time is a source of stress and also a significant challenge to maternal cognitive control skills (Crandall et al., 2015). One study showed that the birth of twins also has a negative impact on maternal responsiveness (Beer et al., 2013).
Furthermore, in the results of the present study, a relationship was found between maternal responsiveness as a function of the reproductive experience and the motor development of preterm infants. Regarding the general motor development, fine adaptive and gross, the group of primiparous mothers with twin newborns presented a higher number of children with a "normal" outcome at ten months of corrected age, even though their mothers had a lower mean SIS score than the group of primiparous mothers. It is suggested that, as a result of maternal cognitive limitations, due to giving attention to the twin children simultaneously, who have practically the same needs because of their age, these infants developed new adaptive interaction strategies with their twin siblings, providing an increase in their motor skills repertoire. This reinforces the idea that one twin functions as a social support system for the other, a kind of "scaffold" for mutual motor development. However, a study showed that twin siblings are more likely to have changes in motor coordination (Chaves, Tani, Souza, Santos, & Maia, 2012), while another one revealed little interaction between the twins, reinforcing the importance of the relationships with caregivers (Lucion & Escosteguy, 2011).
Unlike the groups of primiparous mothers and primiparous mothers with twin newborns, the group of multiparous mothers stood out due to presenting a higher frequency of children with "delayed" general motor development and "risk" of adaptive fine and gross motor outcomes, associated with the low level of maternal responsiveness. It is hypothesized that, since the mothers in this group had more than one child with different ages and needs, the incentive and attention available were much smaller, justifying the higher frequency of children with "risk" and "delays" in the motor development. A study revealed that multiparous mothers are generally less sensitive/responsive and synchronous to their babies' clues compared to primiparous mothers (Ravn et al., 2011).
The present study is the first to investigate the relationship between maternal responsiveness as a function of the reproductive experience and the motor development of preterm infants during the first year of life. The results contribute to the general comprehension of how the social environment, particularly mother-baby interactions, can be related to the motor development of preterm infants with or without siblings. Because multiple birth and prematurity are intertwined, this phenomenon is of great public health importance and requires a comprehensive set of prenatal and postnatal measures to ensure the best outcomes for affected families. There is a need for specific interventions aimed at premature babies to help them improve their chances of appropriate development.
It is considered that this work contributes to the study of mother-infant social interactions, maternal behavior and the motor development of premature children in the first year of life, as it contributes to the comprehension of interactions in a specific context and addresses some of the gaps highlighted in the literature, such as the strictly neurobiological focus in relation to childhood health. Our findings show that the quality of maternal responsiveness as a function of the number of offspring is associated with the fine and gross motor development of preterm infants. However, the present study did not include the participation of full-term infants (Control Group), this being considered a limitation of the research. The relevance of studies that prioritize analyses with larger samples with different cultural contexts and socioeconomic levels is emphasized, aiming to identify other differences in the interactions.
References
Beer, C., Israel, C., Johnson, S., Marlow, N., Whitelaw, A., & Glazebrook, C. (2013). Twin birth: An additional risk factor for poorer quality maternal interactions with very preterm infants? Early Human Development, 89(8),555-559. doi: 10.1016/j.earlhumdev.2013.02.006 [ Links ]
Bos, A. F., Braeckel, K. N. J. A., Hitzert, M. M., Tanis, J. C., & Roze, E. (2013). Development of fine motor skills in preterm infants. Developmental Medicine and Child Neurology, 55(4),1-4. doi: 10.1111/dmcn.12297 [ Links ]
Bryan, E. (2003). The impact of multiple preterm births on the family. BJOG: An International Journal of Obstetrics & Gynaecology, 110, 24-28. doi: 10.12968/hosp.2003.64.11.2344 [ Links ]
Caldas, I. F., Garotti, M. F., Shiramizu, V. K., & Pereira, A. (2018). The socio-communicative development of preterm infants is resistant to the negative effects of parity on maternal responsiveness. Frontiers in Psychology, 9(43), 1-8. doi: 10.3389/fpsyg.2018.00043 [ Links ]
Chaves, R. N. D., Tani, G., Souza, M. C. D., Santos, D., & Maia, J. (2012). Variability in motor coordination: An approach based on the twin design. Revista Brasileira de Educação Física e Esporte, 26(2),301-311. doi: 10.1590/S1807-55092012000200012 [ Links ]
Crandall, A., Deater-Deckard, K., & Riley, A. W. (2015). Maternal emotion and cognitive control capacities and parenting: A conceptual framework. Developmental Review, 36, 105-126. doi: 10.1016/j.dr.2015.01.004 [ Links ]
Feldman, R., Rosenthal, Z., & Eidelman, A. I. (2014). Maternal-preterm skin-to-skin contact enhances child physiologic organization and cognitive control across the first 10 years of life. Biological Psychiatry, 75(1),56-64. doi: 10.1016/j.biopsych.2013.08.012 [ Links ]
Fish, M., & Stifter, C. A. (1993). Mother parity as a main and moderating influence on early mother-infant interaction. Journal of Applied Developmental Psychology, 14(4),557-572. doi: 10.1016/0193-3973(93)90007-IGet [ Links ]
Formiga, C. K. M. R., Vieira, M. E. B., & Linhares, M. B. M. (2015). Avaliação do desenvolvimento de bebês nascidos pré-termo: A comparação entre idades cronológica e corrigida. Journal of Human Growth and Development, 25(2),230--236. doi: 10.7322/JHGD.103020 [ Links ]
Frankenburg, W. K., Dodds, J., Acher, P., Shapiro, H., & Bresnick, B. (1992). Denver II: Training manual. Colorado: Denver Developmental Materials. [ Links ]
Lucion, M., & Escosteguy, N. (2011). Relação mãe-cuidadores de gemelares no primeiro ano após o nascimento. Revista Brasileira de Crescimento e Desenvolvimento Humano, 21(2),307-318. Retrieved from http://pepsic.bvsalud.org/pdf/rbcdh/v21n2/13.pdf. [ Links ]
Morton, M. (2016). We can work it out: the importance of rupture and repair processes in infancy and adult life for flourishing. Health Care Anal, 24(2),119-132. doi: 10.1007/s10728-016-0319-1 [ Links ]
Organização Mundial de Saúde. (2018, dezembro 13). Quase 30 milhões de recém-nascidos prematuros e doentes necessitam de tratamento para sobreviver todos os anos. Retrieved from https://www.paho.org/bra/ [ Links ]
Ostfeld, B. M., Smith, R. H., Hiatt, M., & Hegyi, T. (2000). Maternal behavior toward premature twins: Implications for development. Twin Research and Human Genetics, 3(4),234-241. doi: 10.1375/twin.3.4.234 [ Links ]
Ravn, I. H., Smith, G., Lindemann, R., Smeby, N. A., Kyno, N. M., Grupo, E. H., & Sandvik L. (2011). Effect of early intervention on social interaction between mothers and preterm infants at 12 months of age: A randomized controlled trial. Infant Behavior and Development, 34(2),215-225. doi: 10.1016/j.infbeh.2010.11.004 [ Links ]
Ruble, L., McDuffie, A., King, A., & Lorenz, D. (2008). Caregiver responsiveness and social interaction behaviors of young children with autism. Topics in Early Childhood Special Education, 28(3),158-170. doi: 10.1177/0271121408323009 [ Links ]
Schadl, K., Vassar, R., Cahill-Rowley, K., Yeom, K. W., Stevenson, D. K., & Rose, J. (2018).
Prediction of cognitive and motor development in preterm children using exhaustive feature selection and cross-validation of near-term white matter microstructure. NeuroImage: Clinical, 17, 667-679. doi: 10.1016 /j.nicl.2017.11.023
Shah, P. E., Robbins, N., Coelho, R. B., & Poehlmann, J. (2013). The paradox of prematurity: The behavioral vulnerability of late preterm infants and the cognitive susceptibility of very preterm infants at 36 months post-term. Infant Behavior and Development, 36(1),50-62. doi: 10.1016 /j.infbeh.2012.11.003 [ Links ]
Thomas, A. R., Lacadie, C., Vohr, B., Ment L. R., & Scheinost, D. (2017). Fine motor skill mediates visual memory ability with microstructural neuro-correlates in cerebellar peduncles in prematurely born adolescents. Cerebral Cortex, 27(1),322-329. doi: 10.1093/cercor/bhw415 [ Links ]
Zuccarini, M., Sansavini, A., Iversonb, J., Savini, S., Guarini, A., Alessandroni, R., Faldellac, G., & Aureli, T. (2016). Object engagement and manipulation in extremely preterm and full term infants at 6 months of age. Research in Developmental Disabilities, 55, 173-184. doi: https://doi.org/10.1016/j.ridd.2016.04.001 [ Links ]
 Correspondence:
Correspondence:
Ivete Furtado Ribeiro Caldas
Avenida Pedro Álvares Cabral, 1879, Residencial Lourdes Caldas, bloco B, ap. 202, Marambaia
Belém, PA, Brazil. CEP 66113-190
E-mail: ivbeiro@yahoo.com.br
Submission: 21/09/2018
Acceptance: 26/08/2019
This research was supported, through the granting of a scholarship, by the Coordination for the Improvement of Higher Education Personnel (CAPES).
Authors note
Paula Cristina S. Mesquita, Department of Physiotherapy, Speech Therapy and Occupational Therapy, Faculty of Medicine, University of São Paulo (USP); Daniela D. Siqueira, Physiotherapy Course, University of the Amazon (UNAMA); Marilice F. Garotti, Institute of Health Sciences (IHS), Federal University of Pará (UFPA); Ivete F. R. Caldas, Department of Morphology and Physiological Sciences (DMPS), Child Development Laboratory (CDL), Pará State University (UEPA).

