










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkPsicologia: teoria e prática
Print version ISSN 1516-3687
Psicol. teor. prat. vol.22 no.2 São Paulo May/Aug. 2020
http://dx.doi.org/10.5935/1980-6906/psicologia.v22n2p83-104
ARTICLES
SOCIAL PSYCHOLOGY
Social representations of a former Colony Hospital: a study of its residents
Representaciones sociales sobre un antiguo hospital colonia: un estudio con sus residentes
Ádilo L. V. Passos ; Ludgleydson F. de Araújo
; Ludgleydson F. de Araújo
Federal University of Delta do Parnaíba, PI, Brazil
ABSTRACT
This study aimed to analyze the social representations of residents of a colony hospital (CH), in the northeast of Brazil, about the institution itself. Participants were 16 residents, aged between 48 and 85 years (M = 67.0 years, SD = 9.7). Data were collected using a sociodemographic questionnaire and semi-structured interviews. The interviews were analyzed using the Descending Hierarchical Classification method. The results indicated the centrality of justifying function of social representations, showing explanations for staying in the Colony, even after being cured. Thus, for some residents, living at the CH is due to the lack of resources. For others, remaining at the place arises from attachment to the institution. Therefore, although the CH was a shelter for patients and enabled them to be "cared for," this institution has also contributed to the construction of negative representations about these people and has not provided sufficient subsidies to reinsert them into the society.
Keywords: social representations; Hansen's disease; leprosy; colony hospital; isolation.
RESUMEN
Se objetivó analizar las representaciones sociales de los residentes de un hospital colonia (HC), de noreste brasileño, sobre esta institución. Participaron 16 residentes, con edades entre 48 y 85 años (M = 67,0 años, SD = 9,7). Para los datos utilizó un cuestionario sociodemográfico y entrevistas semiestructuradas. Analizó las entrevistas utilizando el método de Clasificación Jerárquica Descendente. Los resultados indicaron la centralidad de la función justificadora de las representaciones sociales, evidenciando explicaciones de la permanencia en la colonia, ya que están curados. Asimismo, para algunos residentes, vivir en HC viene de la falta de recursos. Para otros, permanecer en el lugar se deriva del apego a la institución. Finalmente, aunque el HC ha servido de refugio para los enfermos y les ha permitido ser "atendidos", esta institución también ha contribuido a la construcción de representaciones negativas sobre estas personas y no ha proporcionado suficientes subsidios para reintegrarlos socialmente.
Palabras clave: representaciones sociales; hanseníase; lepra; hospital colonia; aislamiento.
1. Introduction
Hansen's disease is a chronic contagious infectious disease that manifests through skin lesions, with a significant decrease in pain, tactile, and thermal sensitivity (Ministério da Saúde, 2014). Note that it is a curable disease, and its treatment follows a standard protocol proposed in 1982 by the World Health Organization (WHO) (Awofeso, 2011; Santos et al., 2015).
The treatment that cures Hansen's disease is recent, however. For most of human history, people referred to as "lepers" were considered a threat to healthy individuals and, therefore, were segregated and isolated from life in society (Botero-Jaramillo, Padilla-Pinzón, Beltrán-Serrano, & Ossa-Trujillo, 2017). It is from this context that the so-called colony hospitals emerged. These were facilities intended to control ill individuals socially and were equipped to meet all the basic needs of residents to avoid any type of external interference (Palmeira, Queiroz, & Ferreira, 2012).
It is noteworthy that compulsory isolation measures reached their apex in the Vargas Era (1931-1945). These measures were based on three pillars: dispensary, leprosarium, and preventorium (Castro & Watanabe, 2009). A dispensary facility was responsible for monitoring families and people who had had contact with the sick; a leprosarium facility was responsible for isolating and treating patients; and a preventorium provided care for the non-contaminated children of individuals with Hansen's disease (Palmeira et al., 2012).
The focus at the time was to build leprosarium facilities (colony hospitals). Among the various demands, this measure was a response on the part of the state to the Brazilian elite who, due to the constant scientific dissemination of the disease's contagious nature, demanded more severe actions to protect healthy individuals (Leandro, 2013). For this reason, most of the internees living in these colonies had been taken to isolation against their will, often through the use of police force.
The colony hospital (CH) addressed in this study, located in the northeast of Brazil, was built in a remote area of the city to isolate and treat patients. It was designed to house approximately 50 people, with many pavilions and institutions, including a city hall, police station, and accommodations (Lima & Santos, 2014). Note that the facility's geographical location and the way it was organized translated into effective isolation, which led the local population to hold negative representations of it and its residents.
Because of effective segregation and, consequently, breaking up and/or weakening of family and community ties, many of those who had been confined in colony hospitals, though discharged after being cured, remained isolated (Castro & Watanabe, 2009; Souza & Sena, 2014), a situation experienced by those who took part in this study.
A previous study, the objective of which was to identify the socio-economic profile of the remaining residents of the CH addressed here, 30 people at the time (Vilela & Rocha, 2011), verified that 70% were aged between 51 and 70 years old, 60% were men, 50% presented sequelae from the disease, 60% were unable to read or write, and 45% of the residents were husbandman before being isolated.
These data facilitate understanding the difficulties these individuals might have faced being socially reinserted after they were healed from Hansen's disease. These residents presented significant vulnerability, such as from old age, low educational level, and having an occupation associated with manual labor. The latter appears as a vulnerability considering that, until recently, the disease caused serious damage to one's physical condition.
On the other hand, even though individual factors that hinder an individual's social reinsertion process are important, the state played an important role in this process, as it allowed this population, who needed resources, public policies, government infrastructure, and support in order to leave the hospital, to remain invisible and forgotten. Currently, 22 residents still live in their respective accommodations, while no re-socialization strategy has been devised so far.
Considering that, in the past, Hansen's disease was associated with leprosy, mutilation, suffering, and social isolation, it is not uncommon to find in the literature studies addressing the residents of former colony hospitals, especially reminiscences (Carvalho, 2009; Botero-Jaramillo et al., 2017; Castro & Watanabe, 2009). In these studies, contrary to what one might suppose, former residents tend to represent the Colony as a place where they could rebuild their lives, stating that the "resentment" they experience is not directed to the Colony, but to the "healthy" society that excluded them (Carvalho, 2009; Maciel, 2017; Rocha, Landim, Caprara, Lefèvre, & Lefèvre, 2011).
Despite the relevance of these studies, they were more centered on individual representations and/or historical aspects. Thus, in order to expand the scope of analysis in this type of research, as well as to understand the conceptions held by the residents of a colony hospital, a hospital has been selected that has not been investigated from the psychosocial perspective that this paper adopts, the Theory of Social Representations (TSR).
Social representations (SR) are dynamically and socially built structures that are manifested in the speech and practices guiding the routine decision-making of individuals and groups in the most diverse moments of life (Moscovici, 2007). In the process in which practical knowledge is developed, social actors link information with their experiences and with the knowledge rooted in culture (Belfort, Barros, Gouveia, & Santos, 2015).
Hence, investigating SR means not only identifying cognitions, but mainly revealing the functions of practical knowledge, as well as clarifying the context in which these are developed (Jodelet, 2001). Four functions of SR stand out: the function of knowledge, which makes the world intelligible to individuals and facilitates social communication; the identity function, in which social comparison is used for identity to emerge and to protect particular aspects of a group; the guidance function uses SR as a guide for action; and finally, the justification function, which serves to explain behaviors toward other groups (Chaves & Silva, 2011).
Regarding the process in which SR is created, note the importance of two socio-cognitive mechanisms: anchoring and objectification (Jodelet, 2001). The first refers to an effort to make the unknown familiar using concepts and ideas, which constitute common sense theories. In contrast, the second mechanism attributes substance to ideas, giving them concreteness or iconic structure (Chaves & Silva, 2011).
Due to the SRT's potential to understand common sense, that is, the social context that is shared daily, this study sought to analyze the social representations held by the residents of a colony hospital located in the northeast of Brazil, concerning the facility itself.
2. Method
2.1 Study design
This is an exploratory and descriptive study with a qualitative approach, using cross-sectional data.
2.2 Participants
This study included 16 residents of a colony hospital located in the northeast of Brazil. The hospital facility was inaugurated in July 1931 by a charitable society and was taken over by the government on January 3rd, 1940.
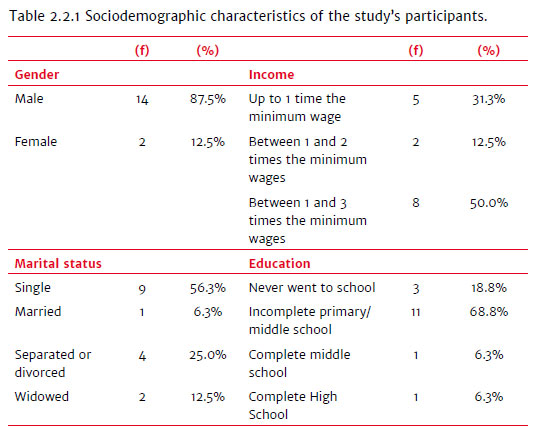
The participants were aged between 48 and 85 years old (M = 67.0 years old; SD = 9.7), and all had been cured of Hansen's disease. The participants' time since diagnosis ranged from 4 and 63 years (M = 36.42; SD = 17.1), and age at the time of hospitalization in the CH ranged from 13 to 66 years (M = 37.56 years and SD = 16.20). Note that the most recent resident has lived at the institution for two years, and the one that has lived there the longest has resided there for 56 years (M = 28.9 years; SD = 17.8). Sociodemographic data are presented in Table 2.2.1.
2.3 Instruments
Data were collected using two instruments. The first was a sociodemographic questionnaire used to characterize the participants, intending to collect information on age, sex, marital status, schooling, income, when they were diagnosed, when they were admitted to the CH, and when they were cured.
The second instrument was a semi-structured interview intended to aid understanding the perceptions participants held about the CH, which included the following guiding question: "What do you think about the CH?"
2.4 Ethical procedures and data collection
This study was submitted to and approved by the Institutional Review Board at the Federal University of Piauí (CAAE: 69177017.3.0000.5669 and opinion report No. 2.311.177), after which the author contacted the CH and asked permission to conduct the study in the institution. Data collection was initiated after providing clarification to potential participants about the study's objectives and informing them that their participation was voluntary and that their identities would remain confidential. Those who agreed to participate signed free and informed consent forms under Resolutions 466/12 and 510/16, Brazilian Council of Health. Data collection took 20 minutes on average.
Inclusion criteria were having or having had a diagnosis of Hansen's disease, living in the CH for at least one year, being older than 18 years old, presenting coherent speech oriented in time and space.
At the time of the interview, the CH had 22 residents, three of whom refused to participate, and another three did not meet the inclusion criteria. One of them presented cognitive deficit, one was temporarily living in the facility, and one resident, though living at the CH, was never diagnosed with Hansen's disease.
2.5 Data analysis
Sociodemographic data were analyzed using descriptive statistics to characterize the participants. Statistics were performed using SPSS for Windows version 21.
Semi-structured interviews were analyzed using Iramuteq software. Data were organized according to a Descending Hierarchical Classification, which enables obtaining lexical classes, characterized by specific words and text segments (TS) with words in common (Camargo & Justo, 2016).
3. Results
The general corpus was composed of 16 texts, separated into 177 TS, 151 (85.31%) of which were used (85.31%), satisfying the minimum criteria reported in the literature, that is, utilizing 75% of the corpus (Camargo & Justo, 2016). A total of 5,902 occurrences (words) emerged; 993 were different words, and 504 were hapax (words that appeared only once). Six classes of semantic approximation were formed; however, given the number of interviewees, we could not establish the profile of people in each class.
The first partition of the dendrogram gave origin to two subcorpora, separating classes 2 and 1 from the others. In the second division, the larger subcorpus was fragmented, generating classes 6 and 5 on the one hand, and Classes 4 and 3 on the other hand. The partition of the corpus into six classes is presented in Figure 3.1.
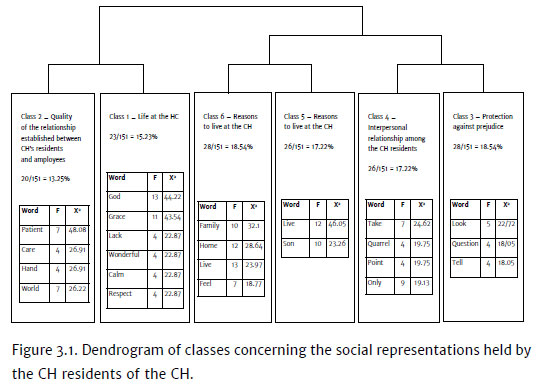
Class 2, "Quality of the relationship between the hospital's residents and employees," is composed of 20 TS (13.25% of the total) and is the smallest class in the dendrogram. In this class, the concept prevails that interpersonal relationships between the hospital's residents and employees are based on mutual respect and consideration, as the following excerpt shows: "The relationship with the Colony's employees, for me it's alright. They are good people, you know? They are good to the patients, treat everybody well, and we also treat them well. Consideration and respect and they respect us".
Class 1, "Life at the CH," comprises 15.23% (f = 23 TS). The words that better relate to this class describe the CH as a wonderful place that meets all the residents' needs and inspires a sense of gratitude. The following excerpts illustrate this class: "My life is wonderful, my life is peaceful, a bed of roses. The Colony is very good"; "I have nothing to complain about. I thank God that I have everything, nothing is missing, thank God."
Classes 6 (f = 28 ST - 18.54%) and 5 (f = 26 ST - 17.22%), called "Reasons to live at the CH," show that the reasons why individuals remain at the CH, even after having being cured of Hansen's disease, are either because they need it, considering they have nowhere else to live, or because they choose to. Note that, even though some report having a family, living with relatives does not seem to be an option.
The statements that best characterize this class include: "The reason I live here is that I feel good here. I have no home, I'm not married, though my entire family regards me well, thank God"; "I can't live by myself"; "Because we don't have another place to go, son. If I could leave here and live somewhere else, I would, but I can't. I have to stay here"; "Son, I'm sorry, but my desire is to stay for as long as I can... I'll only leave if it closes or I die".
Class 4 is composed of 26 ST (17.22% of the total) and is called "Interpersonal relationship among CH residents." It shows that quarrels and the habit of speaking ill of others are the main threats to good coexistence. The following excerpts confirm it: "There is no point in fomenting disunity, fights, because fights take you nowhere, only backward."; "I don't talk about peoples' lives. I take care of my own business. I take care of my life and let others live their lives. I won't meddle. I'll help if I can".
Class 3, "Protection against prejudice," consists of 28 ST (18.54% of the total). In this class, the conception that predominates is that living at the CH protects the individual from prejudice because social relationships are established with those who were also affected by Hansen's disease. The statements that are most representative of this class were: "I'd isolate myself. I wouldn't talk to anyone, but now living here is wonderful. Look at the nature we have here!"; "Listen, considering everything that is bad, here is a piece of heaven. Here you are free of prejudice because everyone is sick, so nobody can speak ill of each other".
This study's results show that, in general, the SR concerning the CH presents meanings in agreement with those presented in the literature. Thus, the lexical content that structured the dendrogram classes (Figure 3.1) are discussed to better understand the SR of the CH presented by its residents.
4. Discussion
As reported by other studies addressing residents of former colony hospitals (Maciel, 2017; Rocha et al., 2011), this study's results also show that life in this type of facility is positively represented. The reasons the participants listed and which explain this representation include the quality of the relationships established between residents and employees, as well as the ability of the CH to meet all the residents' needs.
The friendly relationship established between the facility's employees and residents is perhaps a recent experience. One study showed that isolation in these facilities was marked by prejudice and discrimination, manifested in simple daily activities, such as not sharing household utensils, especially between patients and employees (Palmeira et al., 2012).
Thus, the improvement in the quality of this relationship may be due both to the opening of the colonies to the public and an awakening of a critical awareness regarding the role of employees and how they should treat former internee patients. Indeed, since the Movement for the Reintegration of People Affected by Hansen's Disease (Morhan) in 1981, people with Hansen's disease and those with sequelae were greatly empowered, favoring their autonomy and the exercise of their civil rights (Santos et al., 2015).
Note that Morhan was established as a result of a massive and imposing presence of the state. The social aversion caused by so-called "leprosy" was legitimated and intensified during a long period by the Mandatory Isolation Policy implemented by the now extinct Department of Leprosy Prophylaxis (Vieira, 2008).
It is also interesting to note that the satisfaction of residents with the CH structure contrasts with the experience of most of the 33 colony hospitals remaining from the period of compulsory isolation (Vieira, 2008). In general, these institutions have experienced many problems, among which the following stand out: lack of assistance to its residents; buildings that are depredated; and lack of equipment and medication for those who require health care assistance (Movimento de Reintegração das Pessoas Atingidas pela Hanseníase, 2004).
The CH currently has an organizational structure composed of 55 employees distributed through health services, administration, and psychosocial follow-up. Even though the CH no longer adopts the asylum system, because Hansen's disease is curable, this facility has performed its hospital role for the neighborhood community. It mainly provides a "shelter" for those residents who became aged during their isolation, similar to what happened in other colony hospitals (Souza & Sena, 2014).
The current non-isolationist nature presents a contradiction, as there is a resident who has lived in the CH for only two years (Table 2.2.1). This situation should be seen as a warning not to use the fact that residents remaining from the asylum system are used to legitimate the entry of new residents, considering that the segregationist model was overcome and incongruent with society's principles, that intents to be democratic.
Another significant piece of information in the representational field of CH is the centrality of the explanatory role of SR (Chaves & Silva, 2011), showing an attempt to explain why residents remain in the Colony, considering all patients there have been cured of Hansen's disease. In this context, the interviewees' concepts are anchored, on the one hand, on a need, the fact they do not have a home, a spouse, or even the health condition to be able to live by themselves; and on the other hand, there is the wellbeing they experience in the Colony, a result of the relationships established with other residents, in addition to the fact that they are protected from prejudice.
Lack of resources and of a family social network enabling former patients to rebuild their lives away from the Colony is the context of a large number of those who remain from the compulsory isolation period. This situation is explained by the fact that, when the ill were admitted to the Colony, they were prevented from living with their families and friends and could no longer study or work outside the colony's boundaries (Rocha et al., 2011).
One study conducted with people who spent their lives institutionalized because of Hansen's disease shows that the life in the Colony required these individuals to reconstruct their relationships from a new perspective because their prior values, opportunities, and prospects no longer held truth in the new context of restriction and reclusion they were experiencing (Souza & Sena, 2014).
Another facet of this restrictive and isolationist model of care is that many formerly-confined patients do not want to leave colony hospitals. The main subjective reasons to remain in these facilities include a notion that they belong to the facility; unwillingness to undo the social ties built on isolation; and a sense they are protected against the prejudice experienced outside the colony boundaries (Maciel, 2017).
One of the main factors hindering social reinsertion, and it is a very familiar reason, is prejudice. In this sense, the CH residents tend to represent this facility as being free of prejudice, considering that all residents are in similar conditions, that is, they were all affected and isolated because of Hansen's disease.
Nonetheless, there is no denying the ambiguity of the Colony's role. It sheltered the ill and provided them "care," it also played an important role in influencing negative representations of these people, which became a serious obstacle to social reinsertion.
The fact that prejudice is represented as something that happens outside the Colony corroborates the results of other studies (Carvalho, 2009; Maciel, 2017; Rocha et al., 2011). There is a very interesting finding reported in one study addressing the residents of a former colony hospital (Carvalho, 2009), showing that the identity of these people, at least in part, was based on a dichotomy expressed by the binomial Colony versus society. Thus, the Colony represented a space where they were welcomed, of identifying with the group. In contrast, society represented a place where those with Hansen's disease were banned, a place where they were not wanted.
Thus, it appears that SR directly influences the construction of identity. It occurs because social groups hold representations of themselves, as well as representations of the position they occupy in relation to other groups, contributing to representations that play an important role in one's identity, considering that it is through SR that individuals identify their differences and similarities when compared to others (Deschamps & Moliner, 2014).
For this reason, having a life marked by illness, isolation, and prejudice accruing from Hansen's disease led the residents of the CH to build their identities based on the representations that oppose the ill (residents) and the healthy (society), even if this representation is no longer aligned with the current context; all residents are cured of Hansen's disease, thus, they are no longer the ill.
Therefore, the SR of the CH held by its residents is mainly anchored on positive aspects, highlighting the high level of satisfaction from being able to live in the facility. Nevertheless, it is also well known that this representation is not homogeneous, especially in regard to the reasons why these people remained in the Colony.
Using the explanatory role of SR, the participants list the reasons why they still live in the CH, despite being cured of Hansen's disease, which is divided between objective and subjective reasons. Objective reasons include the fact that formerly ill individuals do not have the material resources and/or physical condition to leave the CH, and, for this reason, they need to remain in the facility.
From an opposing perspective, the residents present subjective explanations for remaining in the CH. Thus, the facility is represented as the place where they reconstructed their lives after hospitalization and established relationships centered on identification and welcoming, distant from the prejudice and discrimination that take place outside this CH.
According to this representation, the CH no longer plays this social role of segregating and isolating, but rather the role of sheltering people at an advanced age and who are physically impaired, who are neglected by the state. On the other hand, the CH still maintaining these residents cannot justify the entry of new residents or to defend an asylum system, considering that there are consolidated treatment and cure for Hansen's disease.
Finally, this study's results portray the context of a specific group and, for this reason, cannot be generalized. In this sense, further research addressing other colony hospitals located in different regions of Brazil is suggested to identify not only the SR of residents, but also those of employees and of the population living near these facilities.
Despite limitations, the importance of this study lies in the fact that it shows that, even though the residents represented the CH from a positive perspective, it still represents a barrier to the re-socialization of those who experienced the asylum system, because it contributes to negative representations, built by its residents, and does not support them leaving the facility.
References
Awofeso, N. (2011). Leprosy control, public health paradigms and stigma. Australian and New Zealand Journal of Public Health, 35(1),9-11. doi:10.1111/j.1753-6405.2010.00662.x [ Links ]
Belfort, P. B., Barros, S. M. M., Gouveia, M. L. A., & Santos, M. F. S. (2015). Representações sociais de família no contexto do acolhimento institucional. Psicologia: Teoria e Prática, 17(3),42-51. Retrieved from http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1516-36872015000300004&lng=t&tlng=pt [ Links ]
Botero-Jaramillo, N., Padilla-Pinzón L.T., Beltrán-Serrano M. A., & Ossa-Trujillo R. H. (2017). Tratamiento de la enfermedad de Hansen en Colombia: Medicalización y control de la enfermedad a lo largo del siglo XX. Revista Facultad Nacional de Salud Pública, 35(3),358-368. doi:10.17533/udea.rfnsp.v35n3a06 [ Links ]
Camargo, B. V., & Justo, A. M. (2016). Tutorial para uso do software de análise textual IRAMUTEC. Florianópolis: Universidade Federal de Santa Catarina, Laboratório de Psicologia Social da Comunicação e Cognição. [ Links ]
Carvalho, K. A. (2009). Tempo de lembrar: As memórias dos portadores de lepra sobre o isolamento compulsório. Aedos, 2(3),238-255. Retrieved from http://seer.ufrgs.br/index.php/aedos/article/view/10592/6241 [ Links ]
Castro, S. M. S., & Watanabe, H. A. W. (2009). Isolamento compulsório de portadores de hanseníase: Memória de idosos. História, Ciências, Saúde - Manguinhos, 16(2),449-487. doi:10.1590/S0104-59702009000200010 [ Links ]
Chaves, A. M., & Silva, P. L. (2011). Representações sociais. In L. Camino, A. R. R. Torres, M. E. O. Lima, & M. E. Pereira. (Orgs.), Psicologia social: Temas e teorias (pp. 299-350). Brasília: Technopolitik. [ Links ]
Deschamps, J., & Moliner, P. (2014). O aporte das representações à problemática da identidade. In J. Deschamps & P. Moliner (Orgs.), A identidade em psicologia social: Dos processos identitários às representações sociais (pp. 80-85). Petrópolis: Vozes. [ Links ]
Jodelet, D. (2001). Representações sociais: Um domínio em expansão. In D. Jodelet (Org.), As representações sociais (pp. 17-44). Rio de Janeiro: EdUerj. [ Links ]
Leandro, J. A. (2013). Em prol do sacrifício do isolamento: Lepra e filantropia na Argentina e no Brasil, 1930-1946. História, Ciências, Saúde - Manguinhos, 20(3),913-938. Retrieved from http://www.scielo.br/pdf/hcsm/v20n3/0104-5970-hcsm-20-03-0913.pdf [ Links ]
Lima, M. R., & Santos, D. T. (2014). Memórias da Colônia do Carpina: Entre a "lepra" e o cotidiano. Paper presented at the II Encontro internacional história, memória, oralidade e culturas, Fortaleza, CE. Retrieved from de http://uece.br/eventos/2encontrointernacional/anais/trabalhos.html [ Links ]
Maciel, L. R. (2017). Memórias e narrativas da lepra/hanseníase: Uma reflexão sobre histórias de vida, experiências do adoecimento e políticas de saúde pública no Brasil do século XX. História Oral, 20(1),33-54. Retrieved from http://revista.historiaoral.org.br/index.php?journal=rho&page=article&op=view&path%5B%5D=696&path%5B%5D=pdf [ Links ]
Ministério da Saúde (2014). Descrição da doença. Retrieved from http://portalsaude.saude.gov.br/index.php/o-ministerio/principal/leia-mais-o-ministerio/705- secretaria-svs/vigilancia-de-a-a-z/hanseniase/11294-descricao-da-doenca [ Links ]
Moscovici, S. (2007). Representações sociais: Investigações em psicologia social. Petrópolis: Vozes. [ Links ]
Movimento de Reintegração das Pessoas Atingidas pela Hanseníase (2004). Jornal do Morhan, pp. 4-15. [ Links ]
Palmeira, I. P., Queiroz, A. B. A., & Ferreira, M. A. (2012). Quando o preconceito marca mais que a doença. Tempus Actas de Saúde Coletiva, 6(3),187-199. [ Links ]
Rocha, A. C. R. P., Landim, F. L. P., Caprara, A., Lefèvre, A., & Lefèvre, F. (2011). O discurso coletivo de ex-hanseniano morador de um antigo leprosário no Nordeste do Brasil. Interface - Comunicação, Saúde, Educação, 15(36),213-223. doi:10.1590/S1414-32832011000100017 [ Links ]
Santos, K. S., Fortuna, C. M., Santana, F. R., Gonçalves, M. F. C., Marciano, F. M., & Matumoto, S. (2015). Significado da hanseníase para pessoas que viveram o tratamento no período sulfônico e da poliquimioterapia. Revista Latino-Americana de Enfermagem, 23(4),620-627. doi:10.1590/0104-1169.0323.2596 [ Links ]
Souza, J., & Sena, T. (2014). O envelhecer institucionalizado de sujeitos sequelados pela hanseníase da U/E Abrigo João Paulo II. Kairós, 17(1),103-123. Retrieved from https://revistas.pucsp.br//index.php/kairos/article/view/19879/14790 [ Links ]
Vieira, M. L. (2008). Hanseníase X lepra: o passado da morte social. In Movimento de Reintegração das Pessoas Atingidas pela Hanseníase. Cadernos do Morhan: A prática do serviço social no Morhan (pp. 70-92). Rio de Janeiro: Morhan. [ Links ]
Vilela, D. A., & Rocha, J. C. T. (2011). Moradores do Hospital Colônia no Norte do Piauí: Um estudo dos perfis de pacientes de hanseníase. Cadernos de Estudos e Pesquisas, 15(33),55-60. Retrieved from http://revista.universo.edu.br/index.php?journal= 1studospesquisa2&page=article&op=view&path%5B%5D=339&path%5B%5D=220 [ Links ]
 Correspondence:
Correspondence:
Ádilo Lages Vieira Passos
Rua Genésio Lopes Moreira, 345, Campo Velho
Chapadinha, MA, Brazil. CEP 65500-000
E-mail: adilolp@hotmail.com
Submission: 13/07/2018
Acceptance: 18/11/2019
The authors would like to thank the Piauí State Research Support Foundation (FAPEPI) for funding the research.
Authors notes
Ádilo L. V. Passos, Postgraduate Program of Psychology, Federal University of Delta do Parnaíba (UFDPar); Ludgleydson F. de Araújo, Postgraduate Program of Psychology, Federal University of Delta do Parnaíba (UFDPar).

