










Serviços Personalizados
artigo
 texto em
texto em  Português (pdf)
Português (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkRevista Brasileira de Terapia Comportamental e Cognitiva
versão impressa ISSN 1517-5545
Rev. bras. ter. comport. cogn. vol.14 no.3 São Paulo dez. 2012
ARTIGOS
Therapeutic companions: characterization of professional practice in the perspective of behavior analysis
Mariana Nunes da Costa MarcoI,*; Sandra Leal CalaisII,**
INúcleo Paradigma de Análise do Comportamento - Mestre em Psicologia (UNESP)
IIUniversidade Estadual Paulista Júlio de Mesquita Filho - Programa de Pós-Graduação em Psicologia do Desenvolvimento e Aprendizagem - Doutora em Psicologia (PUC-Campinas)
ABSTRACT
Therapeutic Accompaniment as a clinical practice was born in the antipsychiatry political-ideological movement. Most research papers try to build a Therapeutic Accompaniment profile from the beginning of this historical context, but the concept has not yet reached a scientific consensus. Although there are some common characteristics, the Therapeutic Accompaniment's diverse practice makes it difficult to identify the variables and consequently to built a final concept. The main purpose of this study was to characterize therapeutic companions under the behavior analysis perspective. Thirteen Therapeutic Companions, of both sexes, participated of this research. They were from the city of São Paulo and submitted to a semi-structured interview. The results were analyzed in four analysis dimensions and unfolded in categories. It is possible to observe that the Therapeutic Accompaniment's profiles are constantly changing and to characterize them imply the observation of many variables that will be discussed here.
Keywords: therapeutic companions; behavior analysis; clinical psychology
INTRODUCTION
In 1970, Kanfer and Phillips commented on the relevance and importance of planning the environment for behavior change, highlighting the care in the natural environment. Since behavior takes place in the interaction between organism and environment, the design of this environment could cause changes in behavior. They offered training to people who are not directly related to psychology, but who would be close to the client by the time that the problem behavior would naturally happen. They emphasized that the maintenance of desirable behavior and its generalization were intensified when the intervention occurred at home, at school and in institutions where the client resides. These proposals are similar to those currently developed by therapeutic companions (TC), however the proposal called Therapeutic Accompaniment (TA) is rather new and has been subject of scientific research, which has grown significantly with many professionals involved since this extensive work regards several areas of health.
The name Therapeutic Accompaniment is derived from psychoanalytic proposals. The Therapeutic Accompaniment has as precursors the anti-psychiatry movement and institutional psychotherapy that occurred on the 50';s in Europe and the United States. While in Latin America, TA seems to have emerged in the late 60';s in Buenos Aires, Argentina, where many psychoanalysts were affiliated to psychiatric hospitals. Nevertheless the practice of the TC not only transcends the therapy done in workroom (the one limited to the office), as it was conceptualized in its advent, but also is willing to intervene in the individual';s environment - where the reinforcers necessary to learn new skills are offered - arranging contingencies of reinforcement (Guedes, 1993). The problem with presenting the TA as a field of activity is disclosed by the lack of harmony between theories and besides its concept has not yet achieved a scientific consensus. Researchers in a variety of theoretical approaches, especially since the 1980s, became interested in the subject even though there are publications dating from the 60';s. There are some elements to establish the concept of the TA, but the diversity found in practice questions the identification of common aspects of the different forms of this named practice and thus building a more solid concept. Hence, controversies are still present and the concept of the TA has been based on aspects such as training, role in the multidisciplinary team, theoretical framework and the work performed (Simões, 2005; Zamignani, Kovac & Vermes, 2007).
Historical considerations on the advent of Therapeutic Accompaniment are relevant because in some way they assist in the description of current practices. Therapeutic Accompaniment is a form of therapy practice developed within political-ideological movements such as the anti-psychiatry reform, institutional psychotherapy and anti-asylum campaign. At the heart of these political movements, new functions were created for mental health professionals, which became known as psychiatric aides, and in other places, therapeutic companions (Baker, 1998; Benevides, 2007).
Later, the term therapeutic companion was renamed after the professionals who were involved in clinical practice outside the traditional office setting and psychiatric clinics, which according to authors (Estellita-Lins, Coutinho & Oliveira, 2009; Reis Neto, 1995) could be established in the context of psychiatric reform as a form of mental health inter vention based on home care, although some include it among psychotherapeutic modalities.
The therapeutic companion has become an important ally in the maintenance of social ties and active participation in the quality of life of individuals, who had been affected by health problems which hampered their ability to continue working, studying or even to take part in family and take care of oneself (Pitia & Santos, 2005).
In an attempt to conceptualize TA, researchers have been focusing their efforts in contextualizing practices and features from its historical emergence and have found trouble in this task (Rossi, 2006). As from the beginning this practice was responding to different clinical needs and guiding itself conceptually in diverse manners, therefore the reconstruction of its history and the theoretical and clinical discussion are tricky tasks.
It is observed that while Behavior Analysis describes the TA as a proposal integrated to Psychology, one could see that the practice is configured differently in other approaches and other countries. Mauer and Resnizky (2008), for instance, propose a characterization of the Therapeutic Accompaniment in the psychoanalytic perspective, defending the idea of service in "multiple approach" - which in this context means to meet all the client';s family network through a multidisciplinary team - in which the therapeutic companion could be any professional who conduct outdoor activities and / or proposals for social reintegration. In Argentina, a country with predominantly psychoanalytic practice, for example, a code of ethics for therapeutic companions (Lic & Bustos, 2010) was published in August 2010. In that country, therapeutic companion is characterized as a regulated profession.
The features of the practice are not tied up and / or restricted to the physical space of a particular institution - hospital, office or school, for instance - that expands the possibilities of intervention, which are as diverse as their definitions and stories regarding its dawn. Basically its activities are supported on the tripod (a) service outside the office, (b) dialogue with the family and (c) teamwork (Simões, 2005; Zamignani et al., 2007).
Several names were given for this practice, such as: qualified friend, psychiatric caregiver, psychiatric auxiliary, home escort and therapeutic companion. The time sequence for the names and functions of what we now call TC is inaccurate (Ayub, 1996). To Yagiu (2007), the purpose of the attendant is to establish ties with psychiatric patients and have a "differentiated listening of madness" (p.2), in order to develop and strengthen healthy social relationships and offer a new dynamics to psychiatric institutions. The description of these goals made by Yagiu (2007) are based on the psychoanalytic theory, and although the term psychiatric attendant has fallen into disuse, the practice of TA arising from this context and form this theoretical approach remains quite similar. The work that begins with "psychiatric attendant" or "psychiatric auxiliary" continues to follow its path of keeping psychotics patients company while seeking recreation, relaxation and socialization.
The "qualified friend" came to transform the ways in intensive care in mental health, which were integrated into the purpose of the practice of the TC. It can be argued that the TA has evolved from an antipsychiatric background with origin in the 60';s, to another model on the psychiatric reform and anti- asylums, eventually coming to the incorporation of a clinical instrument that dispenses with the conventional setting (Simões, 2005). According to Zamignani et al. (2007), the conceptual discussion in the behavior-analytic approach has been poorly defined because the setting does not define the practice of AT, and the name of the individual who leaves the traditional environment to work in the environment outside the office is under the control of other variables, such as the role it occupies in the multidisciplinary team.
Regardless of theoretical approach, to Ribeiro (2002), the TA presents itself ranging from a parallel practice of caring for people who are in psychological distress across situations that require more intensive care than what is offered in the regular treatment - the clients are in treatment and there is the possibility of adding a number of other accompaniments within the existing demands - to the possibility of building a whole new practice, in which all knowledge is in dialogue on these interventions (Reis, 2006).
Multiplicity also appears in the way the Therapeutic Accompaniment characterized as a practice in the health field, which can be either taken as a program and as an intervention strategy (Silva & Silva, 2006). In this sense, the authors point out the need to distinguish between program and strategy, when regarding the TC';s practice. This distinction shows that the TC';s behavior would be under the control of different contingencies, because it conveys differences that mark not only the theoretical assumptions but that also have influence in decision-making. Morin (1996) defines program as a sequence of predetermined actions that must start and run one after another, without changing. "Certainly, one program works very well when the surrounding conditions do not change, and especially when left undisturbed" (p.284). While strategy, although planned, can be modified in light of information, events, unforeseen events that befall in the course of action. It unavoidably deals with uncertainties.
As pointed out in Zamignani, Banaco and Wielesnka (2007) therapy based on the principles of behavior analysis has been a consistent and effective alternative to deal with problems related to human behavior and much of what is assumed today is the product of changes occurred in behavior modification and in applied behavior analysis. The authors then point out that in the beginning, both applied their knowledge in environments considered to be closed, because in these places researchers / therapists had, besides easy access, greater control of environmental variables that produced the behaviors of subjects who took part in the intervention. Hence, under similar situations resembling those at the basic research laboratory.
Although the controlled environments provide a higher efficacy for interventions to ensure the generalization of these clinical breakthroughs in the natural environment was unlikely. After the very criticized practices of behavior modifiers, it sought to implement procedures in natural environments in order to change these environments and produce as a consequence the modification of subject';s actions. This transition between behavior modifiers and behavioral therapists, demanded a huge effort from these professionals because the intervention';s target was no longer only one, or a homogeneous group it has also become their parents, children, teachers, spouses, depending on the goal (Zamignani et al., 2007a).
It is necessary to point out that the entire modifying behavior movement had great influence on the practice of behavioral therapists who began to work within the offices. Much of the literature produced in this first movement, describes what has currently been seen as the current practice of the therapeutic companions. Kazdin (1984) points out that the applied analyst does not seek to identify foregone processes, but works with the contingencies in which the behavior fits, i.e., treating the case where problem behaviors occur. The therapist goes to these places to observe the contingencies and restructure them. Alternatively, he develops programs to be run in these places with the client or their guardians. Contingencies applied by others as the client';s nurse, wife, teacher or parents, under the supervision of a applied analyst, is characterized as treatment by a mediator. What the author classify as treatment by a mediator resembles the current practice of the therapeutic companions.
Baumgarth, Guerrelhas, Kovac, Mazer and Zamignani (1999) and Londero et al. (2010), are reference authors to the current practice of behavior therapy, they emphasize that TA also has as a main characteristic the intervention in the client';s natural environment and one';s daily life. The environment outside the office, where the maintaining contingencies of behaviors to be altered occur, is very rich for the behavior analyst';s practice. As a helper the therapeutic companion is required to collect data, uses techniques and also handles contingencies, which require change and were previously determined by those responsible for care (Guerrelhas, 2007).
The therapeutic companion can then be seen as "an arranger of contingencies of reinforcement and positive reinforcement provider" (Savoia & Sampaio, 2010, p. 39). The term used by the authors illustrates the important role of the therapeutic relationship shaping a new behavioral repertoire in the client. An "arranger of contingencies" aims to promote conditions in which the likelihood of garnering positive reinforcers to behaviors to be shaped is enhanced. In an account for that, Zamignani (1997) reported a case, suggesting that the establishment of a therapeutic relationship is the key in adherence to therapy.
Thus, this research aimed to characterize the practice of therapeutic companion in the outlook of Behavior Analysis. For this, an interview was applied to participants in order to describe the work of a sample of therapeutic companions, considering their work experience, basic and specific training, type of complaint served and place of work, besides their difficulties and advantages.
METHOD
Participants
16 participants were interviewed. However, by the end, only 13 were taken into consideration. The disposal of three participants was necessary because during the interview it was observed that they did not meet the inclusion criteria. Thereby all participants in this study were therapeutic companions active in the city of São Paulo according to the following inclusion criteria: (a) be assisting at least one case during the interview or to have concluded the service to the utmost of two months preceding the date of the interview, (b) have attended at least three cases since their inception, (c) be a trained psychologist or in training and (d) act in accordance with the theoretical approach of Behavior Analysis. Data collection in this research was performed by a non-probabilistic sample of convenience, subject to semi-structured interviews. The participants were selected in research and training Therapeutic Accompaniment centers, they were psychotherapists who do Therapeutic Accompaniment like interventions and were also indicated by the clients themselves. All ethical procedures in research with humans have been complied with, according to the Ethics in Research Committee of the Faculty of Sciences of the São Paulo State University - UNESP (Case #2138/46/01/09).
Data Analysis
The answers of the interview participants were treated with categorical analysis of speech (Bardin, 1977). For the quantitative and qualitative study were established four dimensions of analysis: a) inception and permanence in the area of Therapeutic Accompaniment, b) description of the practice of Therapeutic Accompaniment; c) questions about the training and d) conditions they like and dislike about the practice.
Inception and permanence in the area of Therapeutic Accompaniment: This first dimension was separated in the categories: presentation to the subject, presentation to the practice and reasons for continuing practicing. The passages that reported how the participant had his first contact with the therapeutic companion and when he made his first visit were considered under the categories of "presentation". They were asked to tell "... how and when did you start working with Therapeutic Accompaniment ..."
Description about the practice of Therapeutic Accompaniment: this dimension of analysis is broad and encompasses multiple categories. The thoroughly analyzed description made by the participants about the way they proceed during the Therapeutic Accompaniment session, from the moment they start working with the case until the time of discharge or withdrawal, including supervision and theoretical considerations.
Questions about the training: the constitution of this third dimension involves the aspects that, according to participants, must be observed and changed about the training. Pieces of personal opinion on the general training of the therapeutic companion and about the very formation of the participant were considered here.
Conditions they like and dislike about the practice: here are excerpts of speech that indicate variables that kept them either close or away from the practice of Therapeutic Accompaniment.
Registration categories were built from the data which facilitated the analysis of the data because they were grouped into less comprehensive classes the recurring themes in the interviews, since the verbal report hinders the establishment of mutually exclusive categories. Thus, the totals do not necessarily correspond to the total number of events categorized. The analysis was initially performed by observing the absolute and relative frequency of the data collected and, after this first phase, important relations between the four dimensions mentioned above were processed.
RESULTS AND DISCUSSION
Inception and permanence in the area of Therapeutic Accompaniment
As previously described, this first analyzed dimension of the speech was broken into the categories: presentation to the subject, presentation to the practice and reasons for continuing practicing. It is noted then that the presentation to Therapeutic Accompaniment occurs predominantly in the undergraduate level, either as knowledge of the subject or presented with the practice. The literature does not address how the presentation occurs, as when authors discuss the presentation they endeavor searching about the proposal for Therapeutic Accompaniment. Data regarding presentation, as displays in Table 1, demonstrate that it occurs predominantly in the undergraduate level and, although not directly observed in other publications, there is evidence it is consistent with what was produced in TA. When researching the characteristics of TA, we read that it is often a student (Londero et al., 2010; Zamignani & Wielenska, 1999; Zamignani, et al., 2007b), so their first contact with the subject and its practice are as an undergraduate student.
Regarding the reasons for continuing practicing, participants reported that the clinical practice outside the office environment is consistent with behavior analysis and provides direct observation of the contingencies in action, which in turn generates faster and more effective results. Furthermore, there were personnel aspect that were considered by all participants, for instance, preference for the absence of routine and the somewhat restricted environment.
Description of the practice of Therapeutic Accompaniment
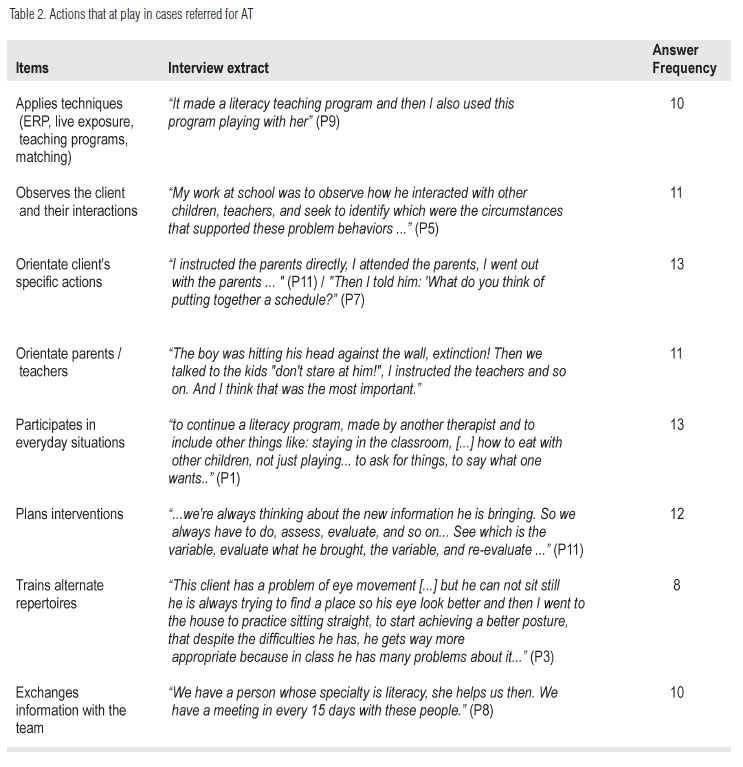
Some passages calls attention to the customer and / or therapist needs that could be supplied with the practice of TA. In addition to that, the participant was asked to describe what they did in the attended cases. Each case has its particularity and its unique needs, but the choice of attending outside of the traditional clinic has its similarities and practice of therapeutic companion, according to the participants, it concerns the observation of contingencies in action, planning and intervention of the control variables at the time they happen. Nevertheless it has been relevant for cases of re-establishing social contacts and repertoire (Caballo, Irutia & Arias, 2010), maintenance of a more adaptive daily routine or the creation of new productive spaces for the individual with physical illness / biological limitations, psychiatric, addiction and geriatric complications (Londero et al., 2010). The actions of therapeutic companions in the environment outside the office differ little from the practice of behavioral therapist at the clinic. At the technological level, there is a set of techniques derived from performed researches and generally are direct manipulations of antecedents and consequences, such as Exposure and Response Prevention (ERP), point system, time out procedure, reinforcement and extinction of sensory or social skills, programs for training specific skills as shown in Table 2. This table exemplifies the items designed to analyze what the participant does when it acts as a therapeutic companion. The therapeutic companion must use the techniques as tools of their work and recognize that the therapist';s role is not limited to technique implementation. Thus, it appears another possible unique feature of therapeutic companion, as the psychologist who attends at the traditional office environment does not receive instructions for their care, even as part of a multidisciplinary team. Londero and Pacheco (2006) presented a study on the referrals to the therapeutic companion and observed that the referrals are influenced by the "functional disabilities" of the client which includes the most basic skills like hygiene, self management, self-control and activities of daily living and even the planning necessary for adherence to treatment. It has also been indicated to those with social relationship abilities compromised, for syndromic reasons or not.
Being in the client';s environment also facilitates the generalization of behaviors. "The maintenance of desired behaviors and its generalization to other situations is enhanced when the treatment is done at home, at school or institution where the patient lives" (Kanfer & Phillips, 1970, p.75). Accordingly, there are no publications on the therapeutic companion as a facilitator of generalization, however, is the role of behavioral therapy to promote generalization and autonomy of the individual and the natural environment has been considered to be the best to promote it. The exposure in the natural environment has the consequence that the acquired and reinforced responses during the interaction with the therapeutic companion often generalize to other environments, being under the control of natural contingencies. The therapeutic companion plans and arranges contingencies closer to the natural environment of the client, enhancing access to reinforcers and the emission of new behavior. The observation of the natural environment is essential to the therapeutic companion, however this research did not emerge as a major goal for the introduction of the therapeutic companion for this case but as part of the analysis and intervention planning.
Questions about training
Seven participants indicated the need to train the practice of Therapeutic Accompaniment and better qualify the professional, which is understood as the teaching of theory, technique and methodologies that aim to achieving a therapeutic result. The therapeutic companions - in general - see the importance to strengthen the theoretical base and expand the discussion of literature about TA which is still incipient. "The conceptual training, the theoretical framework is important [...] and there is a lack of publications in the area to give clearer guidelines" (Participant 5).
Although the participants in this study do not argue that one must necessarily have done a TA course, it was appointed that the formation of a professional is incoherent - because therapeutic companions are much more exposed to the contingencies and the multiple control variables - but their training is shorter than for those who intend to attend in a more controlled environment such as the office. The therapeutic companions also commented on the lack of knowledge about their job by the population and of health professionals and that there is a need for dissemination and clarification of the practice. Unawareness of what therapeutic companions do also hinders recognition of their work. When asked to evaluate the work of a therapeutic companion, the participants mentioned that the key criterion is related to academic activities and length of experience.
Conditions they like and dislike about the practice
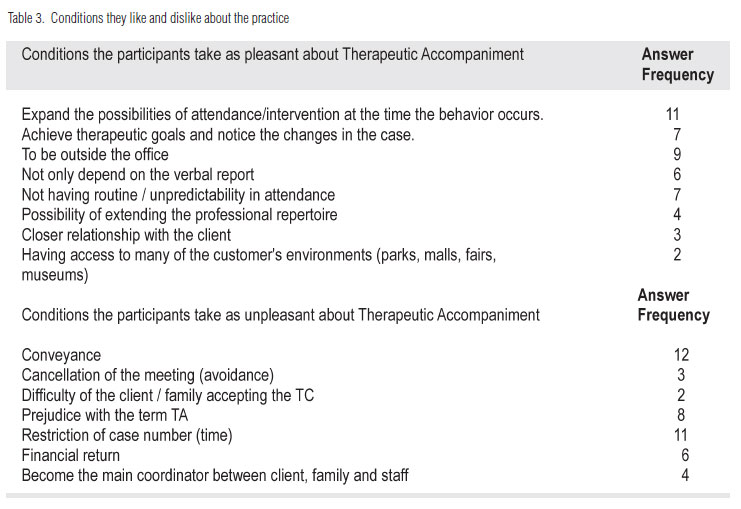
The controversy over the appropriate term to describe the work outside the office expands on this latter dimension of analysis, participants indicate that the therapeutic companions are commonly underestimated among the team. This devaluation is an item that takes part in the information about the conditions they dislike about the practice, as shown in Table 3.
Besides the prejudice against the term, some other aspects were mentioned such as conveyance, number of cases restriction - due to time spent on transport with each attendance (about 2:30 to 3 hours), the difficulty that some families have to accept the Therapeutic Accompaniment';s proposal, to become the main coordinator of information between client, family and staff; and the financial return. Concerning the pleasant conditions, there is the item "closer relationship with the customer," which confirms the interest of these therapists to establish a positive therapeutic relationship with the client. The lack of routine and unpredictability in attendance was also regarded as pleasant. The possibility to improvise and to test alternatives at the moment the behavior occurs was considered to be satisfying aspects as well.
At this point, we emphasize some professional aspects concerning the generation of participants. One has to consider that the therapeutic companions are aged between 20 and 30 years, the Generation Y (or the millennial), that according to administration researches, they need for flexibility and have little work routines, common conditions outside the traditional clinic (Cortoni & Cortoni, s.d). Furthermore, according to the participants the fact of not depending solely on verbal declarations helps achieve much effective changes, and somewhat faster. All participants reported at some point in the interview that Therapeutic Accompaniment has an important role in the clinic psychology and that they identify themselves with this kind of care for the setting, the theoretical proposal and / or the observed therapeutic results. The professional practice of the therapeutic companion is largely autonomous although there are cases of employed professionals (hired or interns) and according to participants the access to cases is given by referral (institutional, by coworkers, other health professionals or clients themselves).
The interview results show that the therapeutic companion';s profile is constantly changing and that its description implies the consideration of many variables. By questioning the professionals who are involved with the therapeutic companions'; training, there was a series of basic conditions for carrying out their work, such as: solid theoretical knowledge, social skills and available time. However, it is not possible to define who the therapeutic accompaniment happens as each professional, considering theoretical and philosophical ideals, propose a different kind of intervention. Most likely, the only common characteristic is without exception the outside the office care.
FINAL THOUGHTS
Preparing a review of the results, it was considered that the participants represent a portion of the behavior analysis therapeutic companion community which provided information that allowed us to revisit the issues raised in the literature. Propose the definition of a professional and its practices based on their self-report is not a simple task. First of all because the therapeutic companion has not been well theoretically defined owing to the fact that of all the implications described and discussed in this research, and secondly because even though verbal behavior is subject to the same principles of nonverbal behavior there is a feature that differs significantly and requires a separate analysis: the nature of the reinforcement that establishes and maintains it - which requires the mediation of another person. Therefore, reporting to someone about one';s role in therapeutic accompaniment brings up one';s personal story, either in theoretical or practical levels and the report is also influenced by the presence of the listener. Thereby, what';s been reported does not necessarily reflect what is done publicly but what one says it does.
Therapeutic companions in Behavior Analysis were influenced by two distinct movements: the anti-asylums and psychiatric reform, along with the first attempts of clinical practice derived from Experimental Behavior Analysis. The influences of anti-asylums reflects the therapeutic companion';s function to stop or prevent psychiatric or chronic clients from being interned and excluded from the community, while the influence of the clinical practice derived from the Experimental Behavior Analysis places the Therapeutic Accompaniment as an intervention consistent with the theoretical assumptions of direct arrangement of contingencies.
It can be asserted that for Behavior Analysis, Therapeutic Accompaniment is characterized by a service in the customer';s environment, outside the office, aimed at the client';s social rehabilitation and the development of alternative repertoires, as well as performs the analysis and intervention to solve a problem without restricting oneself to contingencies artificially arranged in the clinical environment. The features of Therapeutic Accompaniment are similar to the clinical practice, since the understanding of the human phenomenon uses the same philosophical assumption which is Radical Behaviorism.
So, the intervention that is based on these assumptions makes use of analysis and manipulation of contingencies that govern any behavior pattern.
The therapeutic companion seems to be the professional that attends in the customer';s environment, inserted in this context by the referral of another professional (more experienced or who don';t practice outside the office). Their education level has been either complete college degree or attending, since they need a basic therapeutic skill. It is a practice that occurs in a multidisciplinary team and the professional can assume both the function of assisting the process, or as the responsible and coordinator of the case.
It was observed that they perform the same functions as therapists who only assist in the office such as making the initial contract, observation, assessment, treatment planning and applying techniques. The main differences are the setting, the type of variable to which one has access and the therapeutic goals. This type of intervention is recommended for those who need to develop and improve social repertoires, with moderate and severe difficulties that limit the client in situations where she or he has functional impairments, difficulties ascribed to aging, pervasive developmental disorders, anxiety disorders and other psychiatric diagnoses. The Therapeutic Accompaniment was intended to prevent relapses and hospitalization, but the focus has changed and now it does not necessarily has been characterized as a subordinate intervention.
The personal characteristics these professionals show are social skills, agility and improvisation, which is valued by professionals that do and / or indicate clients to therapeutic companions, they also prefer activities without the office';s restrictions - either as an activity complementary to a psychotherapeutic process or as an intervention proposal that happens entirely outside the office. The concept of Therapeutic Accompaniment as an auxiliary component of psychotherapy has weaken with the expansion of research in the area and the training of behavior analysts.
Other noteworthy condition of these participants is that they are organized into groups of students and professionals from institutions and / or clinics. This seems like a good alternative, because it allows clients to access their services and promotes continuous theoretical and technical training through supervision and study groups.
It is then observed that Therapeutic Accompaniment has been considered to be a form of therapeutic intervention that takes place in the client';s context, which did not reach a scientific consensus and that it is a changing concept. With respect to the name for this type of intervention, scientific conceptualization is not clear yet. The term itself does not define the practice. In any case, there are professionals who argue that in Behavior Analysis the term itself does not determine the therapeutic companion';s role and what one does. Moreover, it has become a significant type of service to the user community, and for other approaches within psychology.
It is worth mentioning here that the lack of regulation in this professional practice brings another problem to the definition of a therapeutic companion as to any other professional attending outside the office. Both psychologists and other health professional are subjects to their own council because it is important to consider the risks to client and professionals to make a proposal without support laws and code of ethics. These councils consider students as trainees.
As stated, it seems clear that behavior analyst performing outside the office is consistent with their theoretical assumptions. It points out the need to observe which control variables this decision is based on: the client';s demand, the prognostic hypothesis and effectiveness of the intervention, or if by the comfort of not having to be in transit or the financial return.
Although behavior analysts are careful in researching and publishing about Therapeutic Accompaniment, there is still a lack of scientific literature. Questions about ethics and the limits of practice need to be further explored and further research addressing the client ought to be developed.
REFERENCES
Ayub, P. (1996). Do amigo qualificado ao Acompanhante Terapêutico. Infanto: Revista Neuropsiquiátrica da Infância e Adolescência, ano II, n. 4. p. 37-40. [ Links ]
Bardin, L. (1977). Análise de conteúdo. Lisboa: Edições 70. [ Links ]
Barreto, K. D. (1998). Ética e técnica no acompanhamento terapêutico: andanças com Dom Quixote e Sancho Pança. São Paulo: Unimarco Editora. [ Links ]
Baumgarth, G. C. C., Guerrelhas F. F., Kovac, R., Mazer, M. & Zamignani, D. R.. (1999). A Intervenção em Equipe de Terapeutas no Ambiente Natural do Cliente e a Interação com Outros Profissionais. Em: R.R, Kerbauy, & R. C. Wielenska (Orgs.) Sobre Comportamento e Cognição. Santo André: ESETec, 1999, v. IV p. 164-171 [ Links ]
Benevides, L. L. M. G. (2007). A Função de publicização do Acompanhamento Terapêutico na clínica: O contexto, o texto e o foratexto do AT. 2007. 184 f. Dissertação (Mestrado Psicologia) - Universidade Federal Fluminense - Instituto de Ciências Humanas e Filosofia. Rio de Janeiro. [ Links ]
Caballo, V. E., Irutia, M. J., & Arias, V. (2010). Treino de Habilidades Sociais em situação natural. Em: I., Londero et al. (Org.) Acompanhamento Terapêutico: Teoria e Técnica na Terapia Comportamental e Cognitivo-Comportamental. São Paulo: Ed. Gen/Santos. 2010. p. 51-66. [ Links ]
Cortoni, L. F., & Cortoni, S. Z. (s.d). Duas gerações convivendo na mesma empresa: adversárias ou aliadas? A visão dos líderes sobre a geração Y. s.d. Disponível: <http://www.ateliedepesquisa.com.br/AF_resultados-geracaoXY2.pdf> Recuperado em 17 de dezembro de 2010 [ Links ]
Estellita-Lins, C., Oliveira, V. M., & Coutinho, M. F. (2009). Clínica ampliada em saúde mental: cuidar e suposição de saber no acompanhamento terapêutico. Ciência saúde coletiva. Rio de Janeiro, v. 14, n. 1, p. 195-204, fev. [ Links ]
Guedes, M. L. (1993). Equívocos da terapia comportamental. Temas em Psicologia, Ribeirão Preto v. 1, n. 2, ago. Disponível: <http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1413-389X1993000200011&lng=pt&nrm=iso>. Recuperado em 19 de dezembro 2010 [ Links ]
Guerrelhas, F. F. (2007). Quem é o acompanhante terapêutico: história e caracterização. Em: D. R. Zamignani, R. Kovac, & J. S. Vermes (Orgs.) A Clínica de Portas Abertas: experiências e fundamentação do acompanhamento terapêutico e da prática clínica em ambiente extraconsultório. Santo André: ESETec, 2007. cap 1. [ Links ]
Kanfer, F. H., & Phillips, J. S. (1970). Os princípios da Aprendizagem na terapia comportamental. São Paulo: E.P.U, v. III. [ Links ]
Kazdin, A. (1984). Behavior modification in applied settings. Pacific Grove, CA: Brooks/Cole, Ed. 3. [ Links ]
Lic, M. L. F., & Bustos, N. G. (2010). Código de ética. Asociación acompañantes terapêuticos de La república Argentina (AATRA). Buenos Aires. Disponível <http://www.aatra.org.ar/cod_etica.html> Recuperado em 22 out 2010 [ Links ]
Londero, I. et al. (2010). Acompanhamento Terapêutico: Teoria e Técnica na Terapia Comportamental e Cognitivo-Comportamental. São Paulo: Ed. Gen/Santos. 2010. [ Links ]
Londero, I., & Pacheco, J. T. B. (2010). Por que encaminhar ao acompanhante terapêutico? Uma discussão considerando a perspectiva de psicólogos e psiquiatras. Psicologia em Estudo, Maringá v. 11, n. 2, p. 259-267, maio/ago. 2006. Disponível: <http://www.scielo.br/pdf/pe/v11n2/ v11n2a03.pdf>. Recuperado em 25 de outubro de 2010 [ Links ]
Mauer, S. K., & Resnizky, S. (2008). Acompanhantes Terapêuticos: atualização teórico- clínica. Buenos Aires: Letra viva. [ Links ]
Morin, E. (1996). A epistemologia da complexidade. Em: D. F. Schnitman (Org.) Novos paradigmas, cultura e subjetividade. Porto Alegre: Artes Médicas, p. 274-289. [ Links ]
Pitia, A. C. A., & Santos, M. A. (2005). Acompanhamento terapêutico: a construção de uma estratégia clínica. São Paulo: Vetor. [ Links ]
Reis Neto, R. O. (1995). Acompanhamento terapêutico: emergência e trajetória histórica de uma prática em saúde mental no Rio de Janeiro. Dissertação (Mestrado Psicologia Clínica) - Pontifícia Universidade Católica do Rio de Janeiro, Rio de Janeiro, 1995. [ Links ]
Reis, R. L. A (2006). Construção de uma rede de entendimento do sujeito em sofrimento psíquico: Clínica Ampliada? 2006. 42 f. Trabalho de Conclusão de Curso (Graduação Psicologia). Universidade do Vale do Rio dos Sinos, São Leopoldo. [ Links ]
Ribeiro, T. C. C. (2002). Acompanhar é uma barra: Considerações Teóricas e Clínicas sobre o Acompanhamento Psicoterapêutico. Revista Psicologia Ciência e Profissão. São Paulo, v. 22, n. 2, p. 78-87. [ Links ]
Rossi, G. (s.d) História do AT na Argentina. Disponível <http://siteat.cjb.net/> Recuperado em 16 novembro de 2009. [ Links ]
Savoia, M. G., & Sampaio, T. P. A. (2010). Técnicas cognitivocomportamentais: considerações sobre o repertório do AT. Em: I. Londero et al. (Org.) Acompanhamento Terapêutico: Teoria e Técnica na Terapia Comportamental e Cognitivo-Comportamental. São Paulo: Santos, 2010, p. 37-49. [ Links ]
Silva, A. T.; Silva, R. N. (2006). A emergência do acompanhamento terapêutico e as políticas de saúde mental. Psicologia ciência e profissão. Brasília, v. 26, n. 2, jun. Disponível <http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1414-98932006000200005&lng=es&nrm=iso> Recuperado em 15 de setembro de 2009. [ Links ]
Simões, C. H. (2005). A produção científica sobre o acompanhamento terapêutico no Brasil de 1960 a 2003: Uma análise Crítica. 157 f. Dissertação (Mestrado Enfermagem e Trabalho) - Universidade Estadual de Campinas - Faculdade de Ciências Médicas, Campinas, 2005. [ Links ]
Yagiu, H. (2007). Projetos no Acompanhamento Terapêutico: apontamentos para elaboração. Em: R. G. Santos (Org.) Textos, texturas e tessituras no acompanhamento terapêutico. São Paulo: Instituto A Casa/Editora Hucitec. p. 157-172. [ Links ]
Zamignani, D. R. (1997). O Trabalho do Acompanhante Terapêutico: A prática de um analista do Comportamento. Revista Biociências. Taubaté, v.1, n.3, p. 77-90. [ Links ]
Zamignani, D. R., Banaco, R. A., & Wielenska, R. C. (2007a). O mundo como setting clínico do analista do comportamento. Em: D. R. Zamignani, R. Kovac, & J. S. Vermes (Orgs.) A Clínica de Portas Abertas: experiências e fundamentação do acompanhamento terapêutico e da prática clínica em ambiente extraconsultório. Santo André: ES-ETec, 2007, p. 21-29. [ Links ]
Zamignani, D. R., Kovac, R., & Vermes, J. S. (2007b). A Clínica de Portas Abertas: experiências e fundamentação do acompanhamento terapêutico e da prática clínica em ambiente extraconsultório. Santo André: ESETec. [ Links ]
Zamignani, D. R., & Wielenska, R. C. (1999). Redefinindo o papel do acompanhamento terapêutico. Em: R. R. Kerbauy & R. C. Wielenska (Orgs.) Sobre comportamento e cognição. Santo André: ARBytes Editora, 1999, p. 157-165. [ Links ]

{kind=link}
{kind=link}
{kind=link}