










Servicios Personalizados
Articulo
 texto en
texto en  Portugués (pdf)
Portugués (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkRevista Brasileira de Terapia Comportamental e Cognitiva
versión impresa ISSN 1517-5545
Rev. bras. ter. comport. cogn. vol.15 no.1 São Paulo abr. 2013
REVISÃO
Effectiveness of group cognitive behavior therapies for panic disorder: systematic review and meta-analysis
Tárcio SoaresI,*; Jéssica CamargoII; Adolfo PizzinatoIII
IMSc in Social Psychology - Instituto da Família de Porto Alegre (INFAPA)
IIUndergraduate in Psychology - Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS)
IIIPhD in Psychology - Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS)
ABSTRACT
Although cognitive behavior therapies are vastly studied treatments for panic disorder, reviews on the subject usually don't discriminate between individual and group settings. This article aims to evaluate, through meta-analytical techniques, the effectiveness of group cognitive behavior therapy for panic disorder. A literature search on LILACS, PsycINFO, ISI Web of Knowledge and Pubmed was conducted. Intra-group Hedges (g) effect size calculations were made for symptoms of panic and anxiety, agoraphobia, and depression. A random effects model was used to estimate the summary effect sizes and the publication bias was calculated. The search identified 22 articles from 14 different studies. Summary effect sizes were large for symptoms of panic and anxiety (g=1,39), moderate for symptoms of depression (g=0,79) and large for agoraphobic symptoms (g=0,92). These results suggest that these therapies in group are effective for panic disorder and constitute an interesting alternative of treatment.
Keywords: panic disorder; group therapy; group cognitive behavior therapy; meta-analysis; effectiveness.
INTRODUCTION
Panic disorder (PD) is an anxiety disorder characterized by the recurring and unexpected occurrence of panic attacks. A panic attack may be defined as a sudden episode of anxiety associated with a series of symptons such as palpitations, sweating, sensation of choking, trembling, and fear of losing control, going crazy and dying. Panic attacks do not occur exclusively as part of PD, and may be present in other mental disorders (particularly other anxiety disorders) (American Psychiatric Association [APA], 2002).
The lifetime prevalence of PD was estimated at 4.7% (Kessler et al., 2005) in the U. S., and the disorder is most common in women (APA, 2002). In Brasil, there is still no representative data of the population (Salum, Blaya, & Manfro, 2009). Surveys conducted in São Paulo Metropolitan Area found prevalence rates of 1,1% for 12-month period (Andrade et al., 2012; Viana, Teixeira, Beraldi, Bassani, & Andrade, 2009) and 1,6% for lifetime occurrence (Andrade, Walters, Gentil, & Laurenti, 2002). Age at onset is highly variable; PD tends to arise during adolescence or the fourth decade of life. PD is a chronic disorder, but follows a fluctuating course. Longterm spontaneous remission with no recurrence is extremely rare (Sanchez-Meca, Rosa-Alcazar, Marin-Martinez, & Gomez-Conesa, 2010).
PD is considered a major risk factor for other psychiatric disorders, particularly depressive episodes and substance abuse (Angst, 1998), and is one of the anxiety disorders associated with the greatest suffering and professional and social impairment (Manfro, Heldt, & Shinohara, 2004). Furthermore, when compared with healthy individuals, those with PD experience worse quality of life (Rangé, Bernik, Borba, & Melo, 2011) and use nonpsychiatric health services more often (Klerman, Weissman, Ouellette, Johnson, & Greenwald, 1991).
All of these factors contribute to a massive social burden, which includes the direct costs of PD treatment, the indirect costs associated with greater use of nonspecific health services, and the losses associated with work-related difficulties, such as absenteeism, unemployment benefits, and fewer taxes paid (Greenberg et al., 1999).
Among the several treatment modalities available for PD, there is good evidence for the effectiveness of pharmacological treatment and cognitive-behavioral therapy (CBT) protocols (Barlow, Gorman, Shear, & Woods, 2000). The pharmacological approach is the most common in the Brazilian public health system. However, CBTs provide some advantages, such as: (1) no negative side effects, which are common with the medications used to treat PD; (2) can be provided by non-physicians (e.g. trained psychologists or nurses); (3) are associated with lower relapse rates; and (4) appear to be more cost -effective in the long run (Heldt et al., 2010).
Although effective treatment options for PD are currently available, there remains a need for affordable and cost-effective treatment protocols. Cost-related considerations have become a key issue in the field of health (Morrison, 2001). Approximately two-thirds of those affected by some anxiety disorder (including PD) remain untreated for a variety of reasons, with treatment cost being one of the most common (Anxiety Disorders Association of America, 2009). Overall, group-based treatments have been regarded by the academic community as a good answer to these issues (Tucker & Oei, 2007).
Group cognitive-behavioral therapies (GCBTs) derive directly from individual CBTs and appear to be a promising alternative for the treatment of a wide variety of psychiatric disorders (Bieling, McCabe, & Antony, 2008). However, the vast majority of treatment protocols based on the cognitive-behavioral framework are focused on individual rather than group therapy (Bieling et al., 2008).
Although GCBTs are adaptations of individual treatment protocols, the indications, approaches, dynamics, and outcomes of group treatment are different from those of individual therapy (Yalom & Leszcz, 2006). This means that distinct training approaches and research are required for this modality, which is often ignored. Our search yielded 13 meta-analyses on the effects of CBTs for PD. All studies but one (Sanchez-Meca et al., 2010) pooled individual and group CBTs for analysis. Sanchez-Meca et al. (2010) tested whether the mode of exposure to CBT (group, individual, or mixed) was a moderator variable of observed effect sizes and found a trend toward significance in the difference between modalities (p=0.083), with an apparent advantage of individual and group treatment over mixed approaches. To the best of our knowledge, there have been no in-depth systematic reviews or meta-analyses of the effectiveness of GCBTs for PD.
Another issue involving the reviewed meta-analyses was that only three studies used random effects models for their analyses. As noted by Borenstein, Hedges, Higgins and Rothstein (2009), fixed-effects models are based on the assumption that the actual effect size is exactly the same in all studies. Random-effects models, in turn, admit that individual studies can have different effect sizes due to differences such as sample and therapist characteristics, even if they are normally distributed. This enables greater generalization of results and is thus preferred for studies of treatment effectiveness.
Therefore, the objective of this study was to assess, by means of a systematic review and meta-analysis, the effectiveness of GCBTs for PD.
METHOD
Search strategy
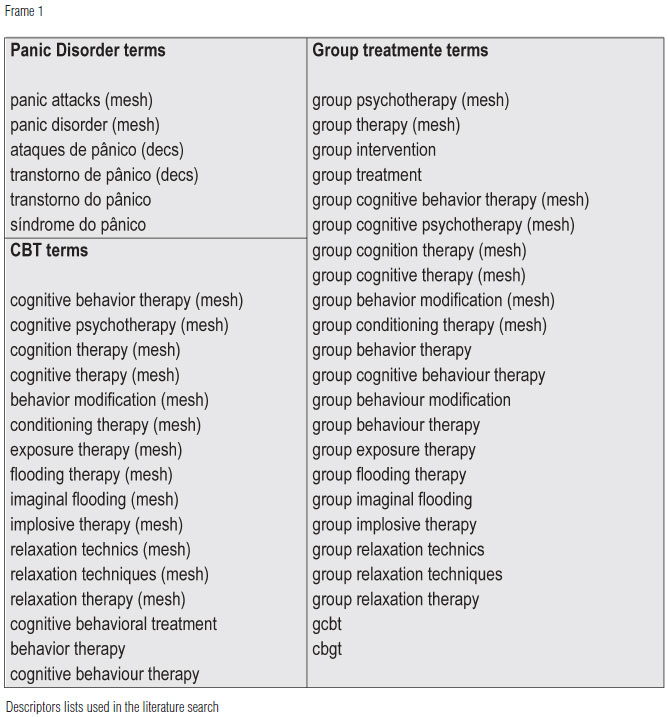
Studies were identified through searches on LILACS, PsycINFO, ISI Web of Knowledge, and PubMed. Three lists of descriptors were created on the basis of the terms "group therapy", "cognitive-behavioral therapy" and "panic disorder". LILACS was searched in Portuguese and all other data bases in English. Descriptor lists are shown in Frame 1.
Due to the limitations of LILACS, only the search terms in the "panic disorder" list could be used, which yielded a wide-ranging search. For the other databases, the intersect of the three lists was used. A handsearch of the references of the most recent meta-analysis on the effectiveness of CBTs for PD (Sanchez-Meca et al., 2010) was also conducted. All database searches were carried out on 13 April 2011.
Study selection
The abstracts of all articles identified by the aforementioned search strategy were read by two independent investigators, who gave their opinions on whether each article should be included in the review. Any divergences were addressed in a meeting between the investigators. When the abstract did not yield enough information to enable an opinion, the full text was read.
The criteria for inclusion were: (1) articles published in English and Portuguese; (2) randomized clinical trial design; (3) all subjects with a diagnosis of PD, regardless of how the diagnosis was established; (4) at least one group treated with a cognitive, behavioral, or cognitive -behavioral approach, as defined within the study itself; (5) the treatment group meeting criterion 4 was treated predominantly by means of group sessions (>50% of sessions or more); and (6) PD was required to be the main focus of treatment. To ensure homogeneity articles on the effects of GCBTs during withdrawal of PD medications were not included.
To prevent duplication of data, when different publications authored by the same investigators or research group (with no clear indication of the difference in samples) were identified, only the most recent or most comprehensive article was taken into account for analysis.
Data extraction
After defining which articles were to be included, two independent investigators read each of the chosen studies and filled out a structured form with information on study characteristics (e.g. use of intention-to-treat analysis, type of control group) and results reported (e.g. means and standard deviations of dependent variables at baseline and after treatment). Again, any divergences were addressed in a meeting between the investigators.
The methodological quality of studies was assessed by means of a series of criteria suggested by Foa and Meadows (1997), Jadad et al. (1996) and Verhagen et al. (1998) . Each study was assigned a score (that of the highest-scoring article). The study was assigned 1 point for each of the following questions, for a maximum of 5 points: (1) Were the participants adequately randomized? (2) Were the investigators blind to allocation? (3) Was there an adequate description of withdrawals and dropouts? (Despite the recommendation of Jadad (1996), we did not deduct points when the reasons for withdrawals and dropouts were not specified.) (4) Did the study use intentionto-treat analysis or any other similar method that includes withdrawals and dropouts? (5) Did the study assess (and describe the results of) treatment integrity or correct adherence to the treatment protocol?
Quantitative analysis
In view of the small number of studies in the heterogeneity of control group types, we chose to analyze withingroup effect sizes only.
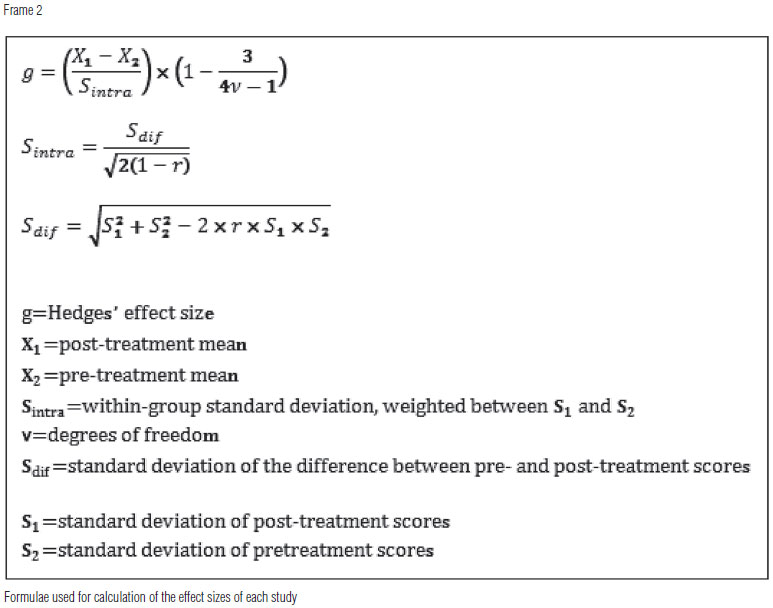
The first step was to calculate the effect size observed for each continuous dependent variable of each study between the pretreatment and post-treatment condition. When data were reported both for completers and intention-to-treat sample, only the latter were taken into account. As the vast majority of studies used measurement instruments with continuous measures, Hedges' g effect sizes were calculated (Hedges & Olkin, 1985). The direction of the effect size was standardized so that a positive effect always represented a better result for the post-treatment group. The formulas used for calculation of effect sizes are shown in Frame 2.
A common issue encountered during meta-analyses of within-group effect sizes is the fact that practically no studies report the coefficient of correlation (r) between pre- and post-treatment scores. Therefore, we used a conservative estimate of r=0.7, as recommended by Rosenthal (1993).
As expected, each of the studies included is a wide variety of instruments for assessment of results. We chose to stratify analysis by symptom domain. On the basis of Morrissette, Bitran and Barlow (2010) and of Shear and Maser (1994), we divided symptoms into a) PD-specific (e.g. number of panic attacks, fear of bodily sensations) and anxiety-specific (no instruments of trait anxiety were included); b) agoraphobia and avoidance behaviors; and c) mood symptons (e.g. depressive symptoms). The definition of which instrument was used for each domain was made by an investigator blinded to study results. When a study reported more than one instrument for assessment of the same domain, effect sizes were averaged. Therefore, three effect sizes were calculated for each study at most.
The summary effect sizes for each of the previously established domains were then calculated, using a random-effects model according to Borenstein et al. (2009). Confidence intervals were set at 95%. Two-tailed hypothesis testing was conducted on the z scores of calculated summary effect sizes.
Publication bias, which may arise because studies with positive results are easier to publish than those with null or negative results, was calculated by means of the Fail-Safe N (Rosenthal, 1979).
The Q test for homogeneity was used to assess the consistency of calculated effect sizes (Borenstein et al., 2009), with the significance level set at p<0.05. The standard deviation of the distribution of the true effects across studies (τ) was also reported.
RESULTS
Selected studies
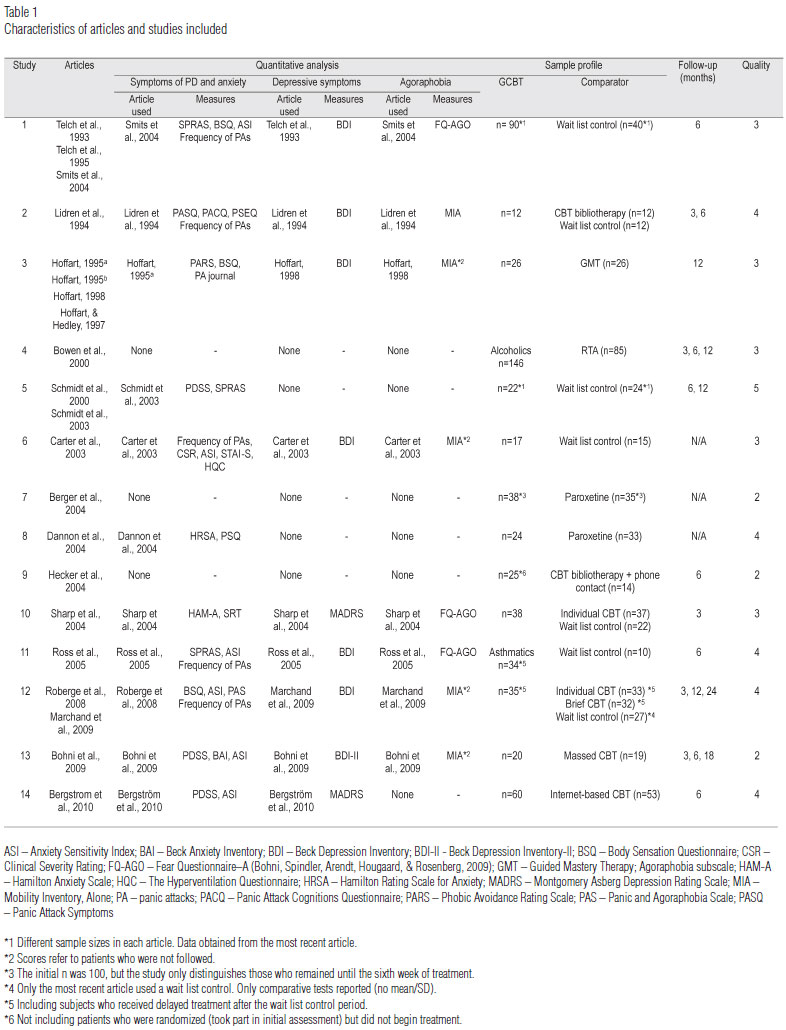
Overall, 22 articles from 14 different studies met the inclusion criteria. Of these, 11 reported enough data for calculation of effect sizes. Table 1 shows the basic characteristics of the included articles and studies.
Study 13 compared two forms of GCBT: intensive GCBT (daily 4-hour sessions during week one, two 2-hour sessions during week two, and one 2-hour session on week three) and a more usual form (13 weekly 2-hour sessions). Only the usual form of GCBT was included in our quantitative analyses.
Considering the data from the most recent articles, a total of 1139 patients with PD were randomized. Of these, 606 were treated with GCBT and 323 were included in our meta-analyses.
In terms of methodological quality, only study 5 had a maximum score. The most common methodological shortcoming of the included studies was lack of information on treatment integrity and proper adherence to the treatment protocol, which was only reported in three studies. On subjective assessment, study 7 had the greatest methodological shortcomings, probably due to publication type - a brief, four-page report that provided only a short description of methods and results.
Characteristics of GCBT protocols and treatment satisfaction
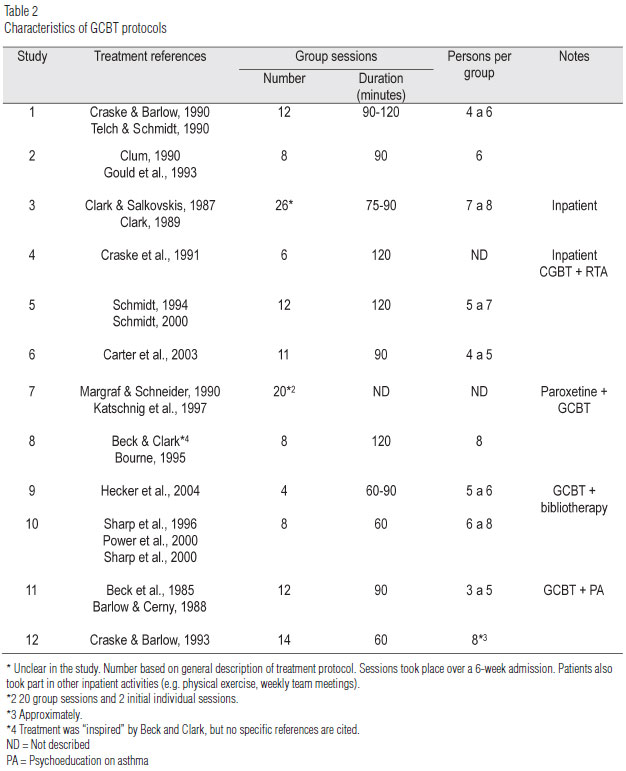
Table 2 provides information on the GCBT protocols used in each study. Of the 14 studies included, 10 used GCBT-only protocols and four included complementary treatment strategies as well. Berger et al. (2004) compared GCBT plus paroxetine versus paroxetine alone. Bowen, South, Fischer and Looman (1994) used panic-focused GCBT as a complementary therapy for alcohol-dependent inpatients with a diagnosis of PD. Ross, Davis, and Macdonald (2005) treat a sample of women with asthma and, thus, included some asthma-targeted psychoeducational interventions as part of the treatment protocol. Finally, Hecker, Losee, Roberson-Nay and Maki (2004) used a combined treatment strategy of bibliotherapy plus four GCBT sessions.
Group sizes were similar across all treatments, ranging from three to eight patients. With the exception of studies 3, 9, and 10, the total duration of treatment was 12-26 hours.
Three studies (2, 11, and 13) assessed patient satisfaction with treatment. Studies 11 and 13 used questionnaire developed by the authors and reported good levels of satisfaction. The only question common to both studies was whether the patient would recommend the treatment to other people with the same condition. On a scale of 0 to 4, patients in study 11 reported a mean score of 3.9. In study 12, on a scale of 1 to 5, the mean score was 4.67. Finally, study 2 used a structured instrument, the Client Satisfaction Questionnaire (Larsen, Atkisson, Hargreaves, & Nguyen, 1979), and also reported high rates of satisfaction with GCBT.
Effectiveness of GCBTs for panic disorder
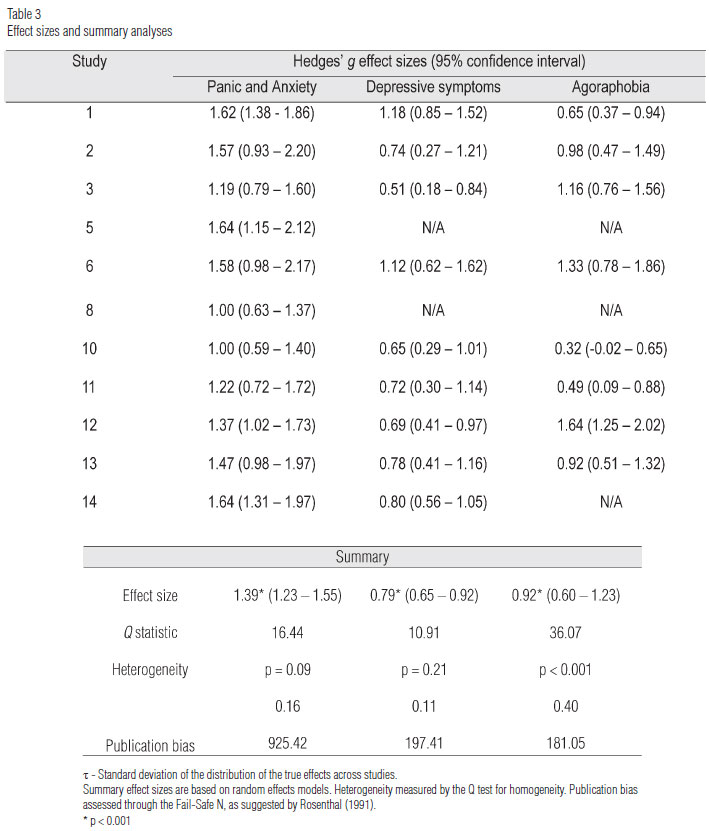
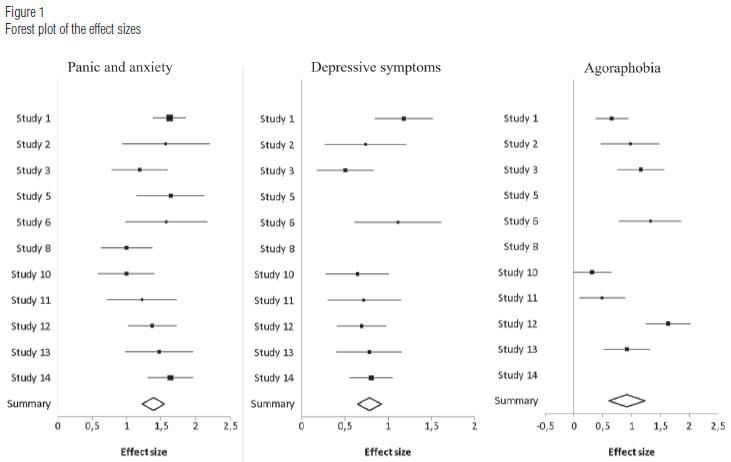
As shown in Table 3, the pre-post summary effect sizes were 1.39 (95%CI, 1.23-1.55) for panic symptoms, 0.79 (95%CI 0.65-0.92) for depressive symptoms, and 0.92 (95%CI 0.60-1.23) for agoraphobic symptoms. According to the Cohen (1988) criteria, effect sizes were moderate-to-large for symptoms of depression and agoraphobia and large for symptoms of panic disorder. All three effect sizes were significant (p<0.0001).
The distribution of effect sizes was heterogeneous for symptoms of agoraphobia (p<0.0001, Q test for homogeneity) and tended toward heterogeneity for symptoms of panic disorder (p=0.09), which evinces an inconsistency between effect sizes. Consequently, the standard deviation of the distribution of the true effects across studies (τ) was particularly high for symptoms of agoraphobia. In other words, 95% of actual effect sizes for the panic symptoms domain were in the 1.06-1.72, range, which is still considered large. However, the same calculation showed that effect sizes for the agoraphobic symptoms domain ranged from 0.11 (null effect) to 1.73 (large effect), thus limiting the findings.
For the depressive symptoms domain, the distribution of effect sizes was not heterogeneous (p=0.21), which led to a small τ. Thus, 95% of the actual effect sizes of each study were estimated to be in the range of 0.57 (moderate) to 1.01 (large).
Calculation of the Fail-Safe N, Rosenthal (1991) indicates that the observed effects probably cannot be explained by publication bias: (922.42 > 60) for the panic and anxiety domain; (197.41 > 50) for the depression domain; and (181.05 > 45) for the agoraphobia domain. Finally, 11 of the 14 studies included had some form of follow-up assessment. On within-group analyses of GCBTs, only study 11 found some difference between the post-treatment and follow-up periods, namely, that improvement in asthma-specific symptoms was no longer significant at 6-month follow-up.
DISCUSSION
The main objective of this study was to assess the effectiveness of GCBTs for PD. Within-group summary effect sizes were moderate to large for symptoms of depression, moderate to large for symptoms of agoraphobia and large for symptoms of panic and anxiety, which shows that GCBTs produce clinically relevant improvements in the assessed symptoms. The original studies used follow-up periods of 3, 6, 12, 18, and 24 months, with sustained improvement of practically all symptoms.
Another issue we investigated was the variability in observed effect sizes. The variation of effect sizes within each study was particularly large for symptoms of agoraphobia. Even if summary effect sizes are moderate to large, between-study variability makes the data inconsistent and decreases its utility. In addition to actual wide variability, the instrument used for measurement of change in agoraphobic symptoms may have been partially responsible for this range. In our review, the three smallest effect sizes were obtained in studies which used FQ-AGO (Fear Questionnaire - A) (Bohni, Spindler, Arendt, Hougaard, & Rosenberg, 2009), and the four largest effect sizes, in studies that used the MIA (Modality Inventory). The small number of studies precluded meta-regression to test this hypothesis.
Of the various meta-analyses of CBTs for PD, only San-chez-Meca et al. (2010) distinguished between scales used for measurement of agoraphobic symptoms. The authors concluded that studies using self-report instruments had smaller effect sizes than studies using clinician-completed instruments. However, both scales used in our analyses were self-report instruments.
Another factor that we didn't control was the proportion of agoraphobic subjects in each study. Agoraphobic patients probably experience greater improvement in these symptoms, which can lead to larger effect sizes and partially explain the heterogeneity in the effect sizes. We suggest that future studies, particularly meta-analyses, address these issues before summarizing data.
Regarding panic and anxiety symptoms, there was a trend toward significance to confirm the hypothesis of heterogeneity between the data reported by different studies. This finding may be explained at least partly by differences in GCBT protocols and differences in the instruments used to measure improvement of these symptoms.
The small number of studies identified precluded any comparative analyses between GCBTs and other treatment approaches. Further studies are required to clarify the relative effectiveness of different treatments.
An in-depth discussion on which treatment modality for PD is most appropriate in a publicly funded health setting would fall outside the scope of this article. We are well aware that issues such as infrastructure, demand profile, and the characteristics of the providers themselves can be determinants in these settings. We can, however, state that GCBTs are an interesting and empirically supported alternative. Furthermore, other studies have shown that GCBTs may be highly beneficial for patients with PD that is refractory to pharmacological therapy (e.g. Heldt et al., 2006; Pollack, Otto, Kaspi, Hammerness, & Rosenbaum, 1994), which is the most common treatment modality in public health settings.
This study has a series of limitations common to meta -analysis. Even though the inclusion criteria were strict, differences in the methodological quality of the chosen studies cannot be bypassed completely. Therefore, in an attempt to minimize discrepancies, we chose to include only randomized clinical trials. A disadvantage of this decision was the exclusion of many uncontrolled and non-randomized studies.
Our choice to include only articles published in English or Portuguese may have led to failure to include important unpublished studies or major studies published in other languages. Furthermore, despite our best efforts to conduct a comprehensive and unbiased search, the possibility that relevant articles may have been excluded remains. Despite that, our analyses show that the significance of the calculated effect sizes was probably not due to publication bias.
Another issue was the small number of studies identified and the heterogeneity of comparator groups, which restricted our meta-analysis to within-subject effect sizes. Although comparisons of this type provide an index of the extent of patient improvement, they do not control for threats to internal validity, such as regression to the mean, spontaneous improvement, and nonspecific treatment factors.
Finally, we intend to update this review in future to include data from new studies and address potential criticism. As noted by Higgins and Green (2011), updating a systematic review after its publication is one way of reducing researcher bias.
REFERENCES
American Psychiatric Association [APA] (2002). Manual diagnóstico e estatístico dos transtornos mentais (DSM-IV-TR). Porto Alegre: Artmed. [ Links ]
Andrade, L., Walters, E. E., Gentil, V., & Laurenti, R. (2002). Prevalence of ICD-10 mental disorders in a catchment area in the city of São Paulo, Brazil. Social Psychiatry and Psychiatry Epidemiology,37, 316-325. [ Links ]
Andrade, L. H., Wang, Y., Andreoni, S., Silveira, C. M., Alexan-drino-Silva, C., Siu, E. R., & Nishimura, R. (2012). Mental Disorders in Megacities: Findings from the São Paulo Megacity Mental Health Survey, Brazil. PLoS ONE,7(2), e31879. [ Links ]
Angst, J. (1998). Panic disorder: history and epidemiology. European Psychiatry,13,51-55. [ Links ]
Anxiety Disorders Association of America (2009). Low-Cost Treatment. [On line]. Disponível: http://www.adaa.org/finding-help/treatment/low-cost-treatment. Recuperado em 04 de Outubro de 2011. [ Links ]
Barlow, D. H., & Cerny, J. (1988). Psychological treatment of panic. New York: Guilford. [ Links ]
Barlow, D. H., & Craske, M. G. (2000). Mastery of your anxiety and panic (MAP-3.). San Antonio: The Psychological Corporation. [ Links ]
Barlow, D. H., Gorman, J. M., Shear, M. K., & Woods, S. W. (2000). Cognitive-behavioral therapy, imipramine, or their combination for panic disorder: a randomized controlled trial. Journal of the American Medical Association,283(19),2529-2536. [ Links ]
Beck, A., Emery, G., & Greenberg, R. (1985). Anxiety disorders and phobias: a cognitive perspective. New York: Basic Books. [ Links ]
*Berger, P., Sachs, G., Amering, M., Holzinger, A., Bankier, B., & Katschnig, H. (2004). Personality disorder and social anxiety predict delayed response in drug and behavioral treatment of panic disorder. Journal of Affective Disorders,80(1),75-78. [ Links ]
*Bergstrom, J., Andersson, G., Ljotsson, B., Ruck, C., Andreewitch, S., Karlsson, A., et al. (2010). Internet-versus group-administered cognitive behaviour therapy for panic disorder in a psychiatric setting: a randomised trial. Bmc Psychiatry,10. [ Links ]
Bieling, P. J., McCabe, R. E., & Antony, M. M. (2008). Terapia cognitivo-comportamental em grupos. Porto Alegre: Artmed. [ Links ]
*Bohni, M. K., Spindler, H., Arendt, M., Hougaard, E., & Rosenberg, N. K. (2009). A randomized study of massed threeweek cognitive behavioural therapy schedule for panic disorder. Acta Psychiatrica Scandinavica,120(3),187-195. [ Links ]
Borenstein, M., Hedges, L. V., Higgins, J. P. T., & Rothstein, H. R. (2009). Introduction to meta-analysis. Chichester: John Wiley Profession. [ Links ]
Bourne E. J. (1995). The anxiety and phobia workbook. Oakland, CA: New Harbinger, [ Links ].
*Bowen, R. C., D'Arcy, C., Keegan, D., & Senthilselvan, A. (2000). A controlled trial of cognitive behavioral treatment of panic in alcoholic inpatients with comorbid panic disorder. Addictive Behaviors,25(4),593-597. [ Links ]
Bowen, R. C., South, M., Fischer, D., & Looman, T. (1994). Depression, mastery and number of group sessions attended predict outcome of patients with panic and agoraphobia in a behavioral medication program. Canadian Journal of Psychiatry-Revue Canadienne De Psychiatrie,39(5),283-288. [ Links ]
*Carter, M. M., Sbrocco, T., Gore, K. L., Marin, N. W., & Lewis, E. L. (2003). Cognitive-behavioral group therapy versus a wait-list control in the treatment of African American women with panic disorder. Cognitive Therapy and Research,27(5),505-518. [ Links ]
Clark, D. M. (1989). Anxiety states: panic and generalized anxiety. In K. Hawton, P.M. Salkovskis, J. Kirk & D.M. Clark (Eds), Cognitive behaviour therapy for psychiatric problems: a practical guide (pp. 52-96). Oxford: Oxford University Press. [ Links ]
Clark, D. M. (1997). Panic disorder and social phobia. New York: Oxford University Press. [ Links ]
Clark, D. M. & Salkovskis, P. M. (1987). Cognitive treatments for panic attacks: therapists's manual. Unpublished manuscript. University of Oxford. [ Links ]
Clum, G. A. (1990). Coping with panic: a drug-free approach to dealing with anxiety attacks. Pacific Grove, CA: Brooks/Cole. [ Links ]
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale: Erlbaum. [ Links ]
Craske, M. G. & Barlow, D. H. (1990). Therapist's guide for the mastery of anxiety and panic. University of Albany, State University of New York: Center for Stress and Anxiety Disorders. [ Links ]
Craske, M. G. & Barlow, D. H. (1993). Panic disorder and agoraphobia. In D.H. Barlow, (Ed.), Clinical handbook of psychological disorders (pp. 1-47). New York: Guilford. [ Links ]
Craske, M. G., Barlow, D. H. (2001). Panic disorder and agoraphobia. In D.H. Barlow, (Ed.), Clinical handbook of psychological disorders: a step-by-step treatment manual (3th ed, pp.1-59). New York: Guilford Press. [ Links ]
Craske, M. G., Bunt, R., & Rapee, R. M. (1991). Perceived control and controllability during in vivo exposure: spider phobics. Journal of Anxiety Disorder, 5,285-292 [ Links ]
*Dannon, P. N., Gon-usishkin, M., Gelbertrn, A., Lowengrub, K., & Grunhaus, L. (2004). Cognitive behavioral group therapy in panic disorder patients:the efficacy of CBGT versus drug treatment. Annals of Clinical Psyciatry, 16,41-46. [ Links ]
Foa, E. B. & Meadows, E. A. (1997). Psychosocial treatments for posttraumatic stress disorder: a critical review. Annual Review of Psychology, 48,449-480. [ Links ]
Gould, R. A., Clum, G. A., & Shapiro, D. (1993). The use of bibliotherapy in the treatment of panic: a preliminary report. Behavior Therapy, 24,241-253. [ Links ]
Greenberg, P. E., Sisitsky, T., Kessler, R. C., Finkelstein, S. N., Berndt, E. R., Davidson, J. R. T., et al. (1999). The economic burden of anxiety disorders in the 1990s. Journal of Clinical Psychiatry, 60(7),427-435. [ Links ]
*Hecker, J. E., Losee, M. C., Roberson-Nay, R., & Maki, K. (2004). Mastery of your anxiety and panic and brief therapist contact in the treatment of panic disorder. Journal of Anxiety Disorders, 18(2),111-126. [ Links ]
Hedges, L. V. & Olkin, I. (1985). Statistical methods for meta-analysis. Orlando: Academic Press. [ Links ]
Heldt, E., Kipper, L., Blaya, C., Salum, G. A., Hirakata, V. N., Otto, M. W., et al. (2010). Predictors of relapse in the second follow-up year post cognitive-behavior therapy for panic disorder. Revista Brasileira de Psiquiatria, 33(1),23-29. [ Links ]
Heldt, E., Manfro, G. G., Kipper, L., Blaya, C., Isolan, L., & Otto, M.W. (2006). One-year follow-up of pharmacotherapy-resistant patients with panic disorder treated with cognitive-behavior therapy: outcome and predictors of remission. Behaviour Research and Therapy, 44(5),657-665. [ Links ]
Higgins, J. P. T., Green, S.(2011). Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0). Disponível: www.cochrane-handbook.org. Recuperado em 04 de Outubro de 2011 [ Links ]
*Hoffart, A. (1995a). A comparison of cognitive and guided mastery therapy of agoraphobia. Behaviour research and therapy, 33(4),423-434. [ Links ]
*Hoffart, A. (1995b). Cognitive mediators of situational fear in agoraphobia. Journal of Behavior Therapy and Experimental Psychiatry, 26(4),313-320. [ Links ]
*Hoffart, A. (1998). Cognitive and guided mastery therapy of agoraphobia: long-term outcome and mechanisms of change. Cognitive Therapy and Research, 22(3), 195-207. [ Links ]
*Hoffart, A. & Hedley, L. M. (1997). Personality traits among panic disorder with agoraphobia patients before and after symptom-focused treatment. Journal of Anxiety Disorders, 11(1),77-87. [ Links ]
Jadad, A. R., Moore, R. A., Carroll, D., Jenkinson, C., Reynolds, D. J. M., Gavaghan, D. J., et al. (1996). Assessing the quality of reports of randomized clinical trials: is blinding necessary? Controlled Clinical Trials, 17(1),1-12. [ Links ]
Katschnig, H., Berger, P., Sachs, G., Holzinger, A., Amering, M., Mayerhofer, D., Baischer, W., Windhaber, J., & Dantendorfer, K. (1997). Gruppenpsychotherapie bei Paniksto rung. Ein Slow-Open-Konzept mit kognitiven und interpersonellen Elementen. In C. Mundt, M.
Linden, W. Barnett (Eds.). Gruppenpsychotherapie in der Psychiatrie (pp. 143-146). Springer, Wien, New York.
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and ageof-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62,593-602. [ Links ]
Klerman, G. L., Weissman, M. M., Ouellette, R., Johnson, J., & Greenwald, S. (1991). Panic attacks in the community - social morbidity and health-care utilization. Journal of the American Medical Association, 265(6),742-746. [ Links ]
Larsen, D., Atkisson, C., Hargreaves, W., & Nguyen, T. (1979). Assessment of client/patient satisfaction: development of a general scale. Evaluation and Program Planning, 2,197-207. [ Links ]
*Lidren, D. M., Watkins, P. L., Gould, R. A., Clum, G. A., Asterino, M., & Tulloch, H. L. (1994). A comparison of bibliotherapy and group-therapy in the treatment of panic disorder. Journal of consulting and clinical psychology, 62(4),865-869. [ Links ]
Manfro, G. G., Heldt, E., & Shinohara, H. (2004). Transtorno de pânico terapia cognitivo-comportamental na prática psiquiátrica. Porto Alegre: Artmed. [ Links ]
*Marchand, A., Roberge, P., Primiano, S., & Germain, V. (2009). A randomized, controlled clinical trial of standard, group and brief cognitive-behavioral therapy for panic disorder with agoraphobia: a two-year follow-up. Journal of Anxiety Disorders, 23(8),1139-1147. [ Links ]
Margraf, J., Schneider, S. (1990). Panik, Angstanfa¨lle und ihre Behandlung Springer, Berlin, Heidelberg. New York. [ Links ]
Morrison, N. (2001). Group cognitive therapy: treatment of choice or sub-optimal option? Behavioural and Cognitive Psychotherapy, 29(3),311-332. [ Links ]
Morrissette, S. B., Bitran, S., & Barlow, D. H. (2010). Panic disorder and agoraphobia Handbook of assessment and treatment planning for psychological disorders. London: The Guilford Press. [ Links ]
Pollack, M. H., Otto, M. W., Kaspi, S. P., Hammerness, P.G., & Rosenbaum, J. F. (1994). Cognitive-behavior therapy for treatment-refractory panic disorder. Journal of clinical psychiatry, 55(5),200-205. [ Links ]
Power, K. G., Sharp, D. M., Swanson, V., & Simpson, R. J. (2000). Therapist contact in cognitive behavior therapy for panic disorder and agoraphobia in primary care. Clinical Psychology and Psychotherapy, 7,37-46. [ Links ]
Rangé, B. P., Bernik, M., Borba, A. G., & Melo, N. M. M. D. (2011). Transtorno de pânico e agorafobia. Em B.P. Rangé (Org.). Psicoterapias cognitivo-comportamentais: um diálogo com a psiquiatria (2nd ed, pp. 238-268). Porto Alegre: Artmed. [ Links ]
*Roberge, P., Marchand, A., Reinharz, D., & Savard, P. (2008). Cognitive-behavioral treatment for panic disorder with agoraphobia: a randomized, controlled trial and cost-effectiveness analysis. Behavior Modification, 32(3),333-351. [ Links ]
Rosenthal, R. (1979). The file drawer problem and tolerance for null results. Psychological Bulletin, 86(3),638-641. [ Links ]
Rosenthal, R. (1991). Meta-analytic procedures for social research. Thousand Oaks: Sage Publications. [ Links ] Rosenthal, R. (1993). Meta-analytic procedures for social research. Newbury Park: Sage Publications. [ Links ]
*Ross, C. J. M., Davis, T. M. A., & Macdonald, G. F. (2005). Cognitive-behavioral treatment combined with asthma education for adults with asthma and coexisting panic disorder. Clinical Nursing Research, 14(2),131-157. [ Links ]
Salum, G. A., Blaya, C., & Manfro, G. G. (2009). Transtorno do pânico. Revista de Psiquiatria do Rio Grande do Sul, 31(2),86-94 [ Links ]
Sanchez-Meca, J., Rosa-Alcazar, A. I., Marin-Martinez, F., & Gomez-Conesa, A. (2010). Psychological treatment of panic disorder with or without agoraphobia: a meta-analysis. Clinical Psychology Review, 30(1),37-50. [ Links ]
Schmidt, N. B. (1994). Safety maneuver elimination for panic disorder. Unpublished treatment manual. [ Links ]
*Schmidt, N. B., McCreary, B. T., Trakowski, J. J., Santiago, H. T., Woolaway-Bickel, K., & Ialongo, N. (2003). Effects of cognitive behavioral treatment on physical health status in patients with panic disorder. Behavior Therapy, 34(1),49-63. [ Links ]
*Schmidt, N. B., Woolaway-Bickel, K., Trakowski, J., Santiago, H., Storey, J., Koselka, M., & Cook, J. (2000). Dismantling cognitive-behavioral treatment for panic disorder: Questioning the utility of breathing retraining. Journal of Consulting and Clinical Psychology, 68(3),417-424. [ Links ]
Sharp, D. M., Power, K. G., Simpson, R. J., Swanson, V., Moodie, E., Anstee, J., & Ashford, J. J. (1996). Fluvoxamine, placebo and cognitive behaviour therapy, usedalone and in combination in the treatment of panic disorder and agoraphobia. Journal of Anxiety Disorders, 10,219-242. [ Links ]
Sharp, D. M., Power, K. G., & Swanson, V. (2000). Reducing therapist contact in cognitive behaviour therapy for panic disorder and agoraphobia in primary care: global measures of outcome in a randomised controlled trial. British Journal of General Practice, 50,963-968. [ Links ]
*Sharp, D. M., Power, K. G., & Swanson, V. (2004). A comparison of the efficacy and acceptability of group versus individual cognitive behaviour therapy in the treatment of panic disorder and agoraphobia in primary care. Clinical Psychology & Psychotherapy, 11(2), 73-82. [ Links ]
Shear, M. K. & Maser, J. D. (1994). Standardized assessment for panic disorder research - a conference report. Archives of general Psychiatry, 51(5),346-354. [ Links ]
*Smits, J. A. J., Powers, M. B., Cho, Y. R., & Telch, M. J. (2004). Mechanism of change in cognitive-behavioral treatment of panic disorder: evidence for the fear of fear mediational hypothesis. Journal of Consulting and Clinical Psychology, 72(4),646-652. [ Links ]
*Telch, M. J., Lucas, J. A., Schmidt, N. B., Hanna, H. H., Jaimez, T. L., & Lucas, R. A. (1993). Group cognitive-behavioral treatment of panic disorder. Behaviour Research and Therapy, 31(3),279-287. [ Links ]
Telch, M. J. & Schmidt, N. B. (1990). Cognitive-behavioral treatment for panic disorder and agoraphobia: panic inoculation treatment manual. (Unpublished manuscript) [ Links ]
*Telch, M. J., Schmidt, N. B., Jaimez, T. L. N., Jacquin, K. M., & Harrington, P.J. (1995). Impact of cognitive-behavioral treatment on quality-of-life in panic disorder patients. Journal of consulting and clinical psychology, 63(5),823-830. [ Links ]
Tucker, M. & Oei, T. P. S. (2007). Is group more cost effective than individual cognitive behaviour therapy? The evidence is not solid yet. Behavioural and Cognitive Psychotherapy, 35(1),77-91. [ Links ]
Verhagen, A. P., de Vet, H. C. W., de Bie, R. A., Kessels, A. G. H., Boers, M., Bouter, L. M., et al. (1998). The delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. Journal of Clinical Epidemiology, 51(12),1235-1241. [ Links ]
Viana, M. C., Teixeira, M. G., Beraldi, F., Bassani, I. S., Andrade, L. H. (2009). São Paulo megacity mental health survey - a population-based epidemiological study of psychiatric morbidity in the São Paulo Metropolitan Area: aims, design and field implementation. Revista Brasileira de Psiquiatria, 31(4),375-386. [ Links ]
Yalom, I. D. & Leszcz, M. (2006). Psicoterapia de grupo: teoria e prática. Porto Alegre: Artmed.Quadro 1Tabela 1 [ Links ]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}