










Servicios Personalizados
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versión On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.8 no.1 Ribeirão Preto abr. 2012
ORIGINAL ARTICLE
Overload generated by the interaction with schizophrenia patients: nursing building family care
Recargo generado por el convivio con el portador de esquizofrenia: la enfermería construyendo el cuidado a la familia
Mariana Silva GomesI; Rosâne MelloII
IUndergraduate
student in Nursing, Escola de Enfermagem Alfredo Pinto, Universidade Federal
do Estado do Rio de Janeiro, RJ, Brazil. E-mail: mariana-sgomes@hotmail.com
IIRN, Ph.D. in Nursing, Adjunct Professor, Escola de Enfermagem Alfredo
Pinto, Universidade Federal do Estado do Rio de Janeiro, RJ, Brazil. E-mail:
rosane.dv@gmail.com
ABSTRACT
Schizophrenia is a chronic degenerative mental disease, in which the patient has difficulty in self care. Due to deinstitutionalization, the daily life brings burden to family. The goal here was to analyze the degree of overload of the primary caregiver living with the holder of schizophrenia in a psychiatric emergency hospital in the State of Rio de Janeiro. This is a descriptive research with quantitative approach. The participants were ten families in a period of fifteen days for data collection. We used the scale of burden of psychiatric patients' relatives, analyzed by the Likert scale. Overloads were found high in the familiar daily routine and intense shock of their mental health, being fundamental that nursing include families in treatment, reducing the overload.
Descriptors: Schizophrenia; Psychiatric Nursing; Family Health.
RESUMEN
La esquizofrenia es enfermedad mental crónico-degenerativa, en que el portador presenta dificultades para el autocuidado. En razón de la desinstitucionalización, la vivencia cotidiana acarrea recargo a los familiares. El objetivo, aquí, fue analizar el grado de recargo del principal cuidador que convive con el portador de esquizofrenia, en un hospital de emergencia psiquiátrica de la Provincia de Rio de Janeiro. Se trata de pesquisa descriptiva, con abordaje cuantitativo. Participaron diez familiares, en un período de quince días para recogida de datos. Se utilizó la escala de recargo de los familiares de pacientes psiquiátricos, analizados por la escala Likert. Fueron encontrados recargos elevados en la rutina diaria del familiar e intenso estremezco de su salud mental, siendo fundamental que la enfermería incluya las familias en el tratamiento, apocando los recargos.
Descriptores: Esquizofrenia; Enfermería Psiquiátrica; Salud de la Família.
Introduction
Schizophrenia is a chronic degenerative mental disease, in which sick people have difficulty recognizing reality, behaving within the social parameters of normality and even performing self-care tasks and personal hygiene. It is the most serious of mental illnesses, affecting around two million Brazilians and it is surrounded by taboos and prejudices due to ignorance of the majority of the population about this disease (1).
Considering the family unit as a provider of care in situations of health and illness of its members, the place for recognition of differences and the source of the first affective exchanges, the latter is in constant and daily contact with patients with schizophrenia (2).
Therefore, the family suffers intensely with the situation of the ill person, experiencing feelings of distress, depression, isolation, chronic sadness, guilt and anxiety. The presence of disorder causes disruption of the family's existential routine, in which the primary caregiver puts its own needs and wants in the background, becoming overwhelmed for bearing the expenses generated by the disease (3).
On the other hand, there are families who cultivate feelings of denial, anger and critical attitude to people with psychological distress. However, the daily life makes these families also suffer from the damage caused by the disorder, because the emotional impact that mental disorders brings to families is often as intense as the one that reaches the patient (1).
The term "family burden" is based on the impact caused by the presence of psychiatric patients with the family and may involve economic, practical and emotional responses to those who are submitted to family entrusted with the care necessary and required by the patient (4).
The burden felt by the family is characterized by objective and subjective dimensions. The objective burden refers to the negative, concrete and observable consequences resulting from the presence of the mentally ill in the family. When discussing the objective burden, we consider the extra daily tasks that they need to perform to meet the needs of the mentally ill, the financial losses, the radical changes in social, family and professional routine of the family and the support that schizophrenics receive from their families (5-6).
In contrast, the subjective aspect of burden is defined by the perception of the family about the situation, its emotional reaction; its feeling is suffering an overload, and the shock of its mental health (5).
Given the above, it is important to study the family burden resulting from the coexistence of the patient with schizophrenia, since the current mental health policy in Brazil is based on the return and the permanence of people with mental disorders in their family and social core, encompassing leisure, community and work (7).
As a result, it is necessary that nursing professionals including the family in caring for people with mental disorder knows and values the potential overload on existing family and establishes strategies to reduce in order to reduce it.
We outlined here, the objective of the study: to analyze the degree of overloading the primary caregiver living with the person with schizophrenia in a psychiatric emergency hospital in the State of Rio de Janeiro.
Material and Methods
We opted for descriptive research with quantitative approach.
The setting for data collection was a municipal psychiatric emergency hospital located in the State of Rio de Janeiro. The research was conducted at meetings of families, where patients did not participate, only health professionals and family members, and the data collection period was fifteen days.
The subjects were ten families - primary caregivers - who lived with the person diagnosed with schizophrenia. Among them were included relatives of both genders, ages ranged between 27 and 78 years, and the predominant age group 41-50 years. The total of participants is justified by the regular attendance to family meetings.
Data were collected through two instruments: the instrument of family contextualizing and scale of burden of psychiatric patients' relatives.
The first instrument consisted of a structured interview covering issues such as identification data of the family, the family's relationship with the carrier of psychological distress and relationship with the family service.
The second instrument consists of an adapted and validated scale for Brazil, in order to evaluate the overload of the psychiatric patient's primary caregiver (8).
This quantitative scale has 41 items and evaluated various dimensions of family life, organized into subscales. They are: A) assistance in daily life, B) supervision for problem behaviors, C) financial expenditure, D) impact on the daily routine and E) concern for the patient.
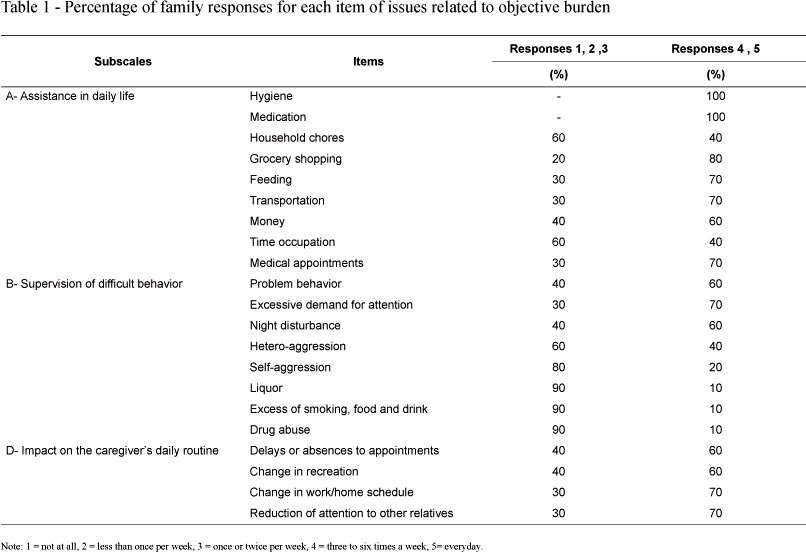
For the schedule of responses related to overload, the Likert scale was adopted. Since the issues of objective burden and assessment of family concerns with the patient the answer choices contain five points. Of these, 1 = not at all, 2 = less than once per week, 3 = once or twice a week, 4= four to six times per week and 5 = every day.
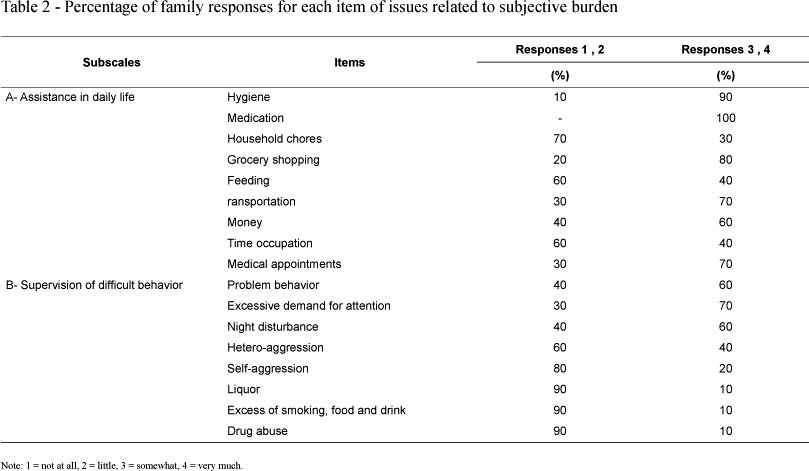
For questions regarding the subjective burden in relation to the degree of discomfort, the response options contain four points, where 1 = not at all, 2 = a little, 3 = somewhat, 4 = very much.
The study was approved by the unit as well as submitted to and approved by the Ethics Committee of the hospital.
Prior to the beginning of the interview, all family members expressed their acceptance to participate in writing by signing the consent form (9).
For data analysis of the instrument family contextualizing it was carried out a descriptive analysis of results. As for the verification of the family burden, the burden scale of the psychiatric patients' relatives, we analyzed the percentage of responses for each item of the subscales, whereas, on issues related to objective burden and assessment of family concerns with the patient, the answers above 4 indicate high overload. On the other hand, the issues related to subjective burden, the answers above 3 indicate high burden of primary caregivers (10).
The subscale C does not apply to the calculations of percentage, it refers to values in spending money with the patient and assesses the economic issues of the family group (8).
Results and Discussion
Characterization of the subject
The entire family living with the patient and being the primary caregivers contributes to increase the frequency of task assistance provided to the patient, as it is on the main caregivers who fall the hardest tasks of care for schizophrenia patients, which are weakened to perform their own personal care (10).
Concerning the degree of kinship of the family member to the patient with schizophrenia, the mothers were identified as the primary caregivers of patients (60%), with predominance of females among the subjects.
The task of caring for the mentally ill has been attributed to women, and searching for the role of women who care for mentally ill, it was found that they are subject to various consequences arising from this responsibility, and express difficulty coping with the person diseased in the family, especially in crisis, when the schizophrenics express delusions and hallucinations, generating intense conflict in the family (11-12).
The predominant educational level of the family was incomplete basic education (80%), with average monthly income of R$ 495.00. All respondents supported the home.
Some characteristics of caregivers indicate increased family weariness, among them, poor education and low socioeconomic status (13).
In addition, all participant subjects were assisted at the service, partaking family meetings. And most of them (70%) were undergoing medical treatment with antidepressants.
Some studies support this search result, to emphasize that families suffer intense exhaustion with mental illness of a loved one, experiencing feelings of distress and sadness, manifesting them through psychopathological stress where depression is the most common among them (14).
Objective burden
The results related to objective burden are shown in Table 1.
According to the subscale, most caregivers replied that they assist in the daily life of the bearer of psychological distress with high frequency, showing high objective burden to the family member.
In this sense, the strict administration of medications, difficulties in the hygiene tasks of the schizophrenic and their limitations in managing their own life situations are stressful to the caregiver, so that he has to supervise and assist the patient with intense frequency in these activities, causing increased overload to the family (15).
Looking at the B subscale, it was observed that most families did not perform supervision with difficult behavior with intense frequency, thus, low overload prevailing in this subscale.
One explanation for this result would be that, during the family meetings, it was found that the vast majority of schizophrenics did not show aggressive behavior toward others or to themselves, nor did they abuse of alcohol and drugs.
By analyzing the D subscale it was found that most families suffer the impact on daily routines, since respondents who are harmed in their routines with high frequency, causing them high overload.
Confirming this result, families living with this type of mental disorder sufferers, present overload in their daily routines, in the sense that they need to attend the household needs of the patient, which are impaired due to the complex symptomatology of the disease, which encompasses the activities of daily disorientation, causing the family members to be absent from work, their social commitments and direct their attention to the care of the mentally disabled (16).
Furthermore, changing the family's leisure is explained by the large stigma and prejudice surrounding the disease, in which the schizophrenic is excluded by society and therefore their main caregivers also suffer this prejudice, causing removal from leisure activities (16).
Subjective burden
The results related to subjective burden are shown in Table 2.
The subscale demonstrated that the majority of families felt extremely uncomfortable to assist in the daily life of the patient, indicating a high subjective burden for them, or disturbances to their mental health.
Consequently, the family feels quite the impact of having to meet the needs of the mentally ill, abdicating their own lives and their desires to take care of schizophrenia patients, which requires intense attention due to their limited condition to manage their own assets and personal life (16).
In examining the subscale B, on issues dealing with aggression, smoking, alcohol and drugs, it was observed that the reduced presence of these behaviors in schizophrenia study, leads to the familiar low overload, i.e., reduction of its impact when considered in set (10).
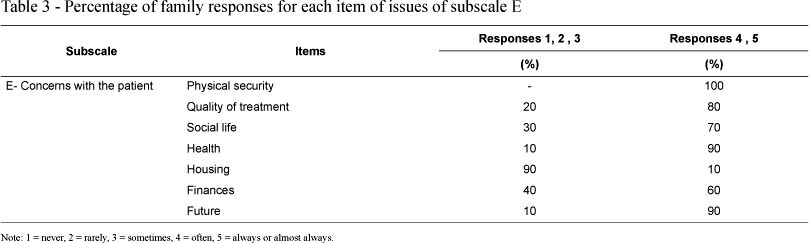
The results of the subscale E are distributed in Table 3.
According to the analysis of the subscale E, it was found that the vast majority of families are intensely concerned with the patient, causing them high overload.
The families of schizophrenia patients feel insecure about the quality of treatment being given to the patient, fear for the safety of the patient, because in times of crisis, there is exacerbation of body movements, intense preoccupation with health and the future of the sick member, especially concerning how their financial situation would be, were it not for the caregiver's assistance (1).
Regarding the results of the subscale C, the average monthly expenses of the family and the patient was R$ 325.00. Considering the average household monthly income (R$ 495.00), and that most patients did not contribute to the monthly expenses, it was possible to detect the presence of financial burden on caregivers. Thus, families living with schizophrenia, often feel financial burden, considering the inability productive as a symptom of the disease, i.e., the ill person stops working, there was an increase in spending for the primary caregiver, resulting from the purchase of medicines, food and other expenses that generate change in the family budget (16).
The nursing care to families
Due to the deinstitutionalization process, the family was included in the care of mental patients, aiming at better recovery of the patient, and appropriate participation of society and the family in treatment, redirecting the mental health care model (17).
The decrease of the burdens felt by the family are considered significant when the primary caregiver participates in programs of family support, expressing their anxieties, doubts about the disease and exchanging relevant information about the difficult situations created by the coexistence of the patient with schizophrenia (13).
In this context, it is essential that nursing professionals develop actions to assist families through individual care, attention to core families, psychoeducational groups, so they can promote counseling, questions about the disease, aid in the management of everyday life and establishment of strategies to cope with their own psychological distress of the family and patient (18). Therefore, the empowerment of the family in times of crisis, the fall of overload and harmonious family life are consequences of adequate support to families.
Furthermore, it is necessary to stimulate the adhesion of the relative processing, as a family cooperative reduces the risk of relapse, and consequently, the instabilities in the family (1).
Reinforcing these observations, the raising of families, called "psychoeducational groups" for families, have contributed to the less confrontational interaction between the caregiver and the patient's psychological distress, as it assists families in understanding the disease, creating more security and optimism to the family (19).
Conclusions
Considering the family core the primary means of interaction of schizophrenia patients, the family takes on greater responsibilities, which undoubtedly leads to changes in daily activities, the family budget and major concerns, generating overloads the primary caregiver.
Therefore, it is certain that the family needs to feel prepared to receive and care for the mentally ill in the family, guided by mental health professionals, so that they can expose all their problems freely and safely to face difficult situations, arising from the interaction with the bearer of psychic distress.
Confirming, therefore, that psychosocial interventions care to family members of individuals with schizophrenia needs to be increasingly adopted in mental health services. For these interventions are effective for the family, it is necessary to obtain the collaborative participation of the family and recognize the difficulties which it is replaced with the presence of a member with severe mental disability.
Based on what was discussed herein, it is believed that the mental health professional, to work together with families, patients and services, needs to know how to detect the degree of overloading of the main caretakers of the ill person, develop proposals for care families, minimizing family burdens and increasing the quality of life of patients with schizophrenia, as well as their family.
References
1. Palmeira L, Geraldes MT, Bezerra AB. Entendendo a Esquizofrenia: como a família pode ajudar no tratamento? Rio de Janeiro: Interciência; 2009. [ Links ]
2. Castilho T. Família e relacionamento de gerações. In: Congresso Internacional Co-Educação de Gerações. 2003; São Paulo: SESC. [acesso 03 fev 2010]. Disponível em: http://www.sescsp.org.br/sesc/images/upload/conferencias/94.rtf [ Links ]
3. Zanetti AC, Galera S. O impacto da esquizofrenia para a família. Rev Gaúch Enferm. 2007;28(3):385-92. [ Links ]
4. Pegoraro RF, Caldana, RH. Sobrecarga de familiares de usuários de um Centro de Atenção Psicossocial. Psicol Estudo. 2006;11(3):569-77. [ Links ]
5. Maurin JT, Boyd CB. Burden of mental illness on the family: a critical review. Arch Psychiatr Nurs. 1990;4(2):99-107. [ Links ]
6. Tessler RC, Gamache GM. Family experiences with mental illness. Auburn House: Westport; 2000. [ Links ]
7. Mello R. A construção do cuidado à família e a consolidação da reforma psiquiátrica. Rev Enferm UERJ. 2005;13(3):390-6. [ Links ]
8. Bandeira M, Calzavara MG, Varella AA. Escala de sobrecarga dos familiares de pacientes psiquiátricos: adaptação transcultural para o Brasil (FBIS-BR). J Bras Psiquiatr. [periódico na Internet]. 2005. [acesso 04 nov 2009]; 54(3):206-14. Disponível em: http://www.ufsj.edu.br/lapsam/sobrecarga_familiar.php [ Links ]
9. Hardy E, Bento SF, Osis MJ. Consentimento Informado Normatizado pela Resolução 196/96: Conhecimento e Opinião de Pesquisadores Brasileiros. RBGO. 2002;24(1):59-65. [ Links ]
10. Barroso SM, Bandeira M, Nascimento E. Sobrecarga de familiares de pacientes psiquiátricos atendidos na rede pública. Rev Psiquiatr Clín. 2007;34(6):270-7. [ Links ]
11. Ornellas CP. O paciente excluído: história e críticas das práticas médicas de confinamento. Rio de Janeiro: Universidade Federal de Santa Catarina; 1997. p. 150-231. [acesso 17 mar 2010]. Disponível em: http://www.cfh.ufsc.br/~labhiss/exclud2.html [ Links ]
12. Gonçalves AM, Sena RR. A reforma psiquiátrica no Brasil: Contextualização e reflexos sobre o cuidado com o doente mental na família. Rev. Latino-Am. Enfermagem. 2001;9:48-55. [ Links ]
13. Loukissa D. Family burden in chronic mental illness: a review of research studies. J Adv Nurs. 1995;21(2):248-55. [ Links ]
14. Scherer ZP, Scherer EA. O doente mental crônico internado: uma revisão da literatura. Rev. Latino-Am. Enfermagem. 2001;9(4):56-61. [ Links ]
15. Spaniol L, Zipple AM, Lockwood D. The role of the family in psychiatric rehabilitation. Schizophrenia Bull Rockville. 1992;18:341-8. [ Links ]
16. Koga M. Convivência com a pessoa portadora de esquizofrenia: Sobrecarga familiar [dissertação de mestrado]. Ribeirão Preto (SP): Escola de Enfermagem de Ribeirão Preto da Universidade de São Paulo; 1997. [ Links ]
17. Ministério da Saúde (BR). Lei Nº 10.216, de 6 de abril de 2001. Dispõe sobre a proteção e os direitos das pessoas portadoras de transtornos mentais e redireciona o modelo assistencial em saúde mental. Brasília (DF): Ministério da Saúde; 2001. [ Links ]
18. Scazufca M. Abordagem familiar em esquizofrenia. Rev Bras Psiquiatr. 2000;22, Suppl 1:50-2. [ Links ]
19. Yacubian J. Grupos psicoeducacionais para familiares. São Paulo: Associação Brasileira de familiares, amigos e portadores de transtornos afetivos; 2009 [acesso 01 de jun 2010]. Disponível em: http://www.abrata.org.br/site/artigos/artigos.asp?vLink=artigos&artigoId=12 [ Links ]
Received: July
20th 2010
Accepted: Aug. 3rd 2011

{kind=link}
{kind=link}
{kind=link}