










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
On-line version ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.9 no.1 Ribeirão Preto Apr. 2013
ORIGINAL ARTICLE
Analysis of evolution of mental and behavioral disorders through International Classification of Diseases review
Análisis de la evolución de los trastornos mentales y comportamentales a lo largo de las revisiones de la Clasificación Internacional de Enfermedades
Rubia Paixão BenedictoI; Mey Fan Porfírio WaiII; Renata Marques de OliveiraII; Cecília GodoyIII; Moacyr Lobo da Costa JrIV
IMSc, RN, Hospital Santa Tereza de Ribeirão Preto, Secretaria do Estado de São Paulo, Ribeirão Preto, SP, Brazil
IIDoctoral student, Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, WHO Collaborating Centre for Nursing Research Development, Ribeirão Preto, SP, Brazil
IIIMSc
IVPhD, Associate Professor, Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, WHO Collaborating Centre for Nursing Research Development, Ribeirão Preto, SP, Brazil
ABSTRACT
This study aimed to describe the creation and evolution of three diagnostic categories of the chapter V of the International Classification of Diseases ICD, denominated in ICD-10: 1) Mood disorders, 2) Schizophrenia and 3) Mental and behavioral disorders due to psychoactive substance use, since the sixth to the tenth review (current). The changes of these categories within the ICDs were described, along with the code changes and it was quantified the grouping, categories and subcategories numbers. We observed significant changes, incorporations of new definitions and redefinitions. It was concluded that the changes followed the course of the diseases and psychiatric disorders that were full with prejudice and exclusion expressions, especially in addition to expanding the number of categories, the improvement in the content of Chapter V.
Descriptors: International Classification of Diseases; Mood disorders; Schizophrenia; Substance-Related Disorders.
RESUMEN
Este estudio tuvo por objetivo describir la creación y la evolución de tres categorías diagnósticas del capítulo V de la Clasificación Internacional de Enfermedades-CID, denominadas en CID-10: 1) Trastornos de humor, 2) Esquizofrenia y 3) Trastornos mentales y comportamentales debido al uso de substancias psicoactivas, desde la sexta revisión a la décima (actual). Fueron descritos los cambios de esas categorías entre CID, los cambios de códigos y cuantificado el número de agrupamientos, categorías y subcategorías. Se observaron cambios significativos, incorporaciones de nuevas definiciones y redefiniciones. Se concluyó que las alteraciones ocurridas acompañaron la trayectoria de las enfermedades y trastornos psiquiátricos que fueron cargados de expresiones que remeten preconcepto y exclusión, destacándose además de la expansión del número de categorías, el mejoramiento en el contenido del capítulo V.
Descriptores: Clasificación Internacional de Enfermedades; Trastornos del humor; Esquizofrenia; Trastornos Relacionados con Sustancias.
Introduction
The International Statistical Classification of Diseases and Related Health Problems (ICD) is currently the most frequently diagnosis system used in coding health problems, including in psychiatry, and aims to search for an international diagnoses standardization(1)
ICD knowledge is of fundamental importance for professionals, considering that information relating to health are properly understood and compared, it is need an organization in its presentation. This occur in ICD through a rating system that has evolved over the years, with its conceptual beginnings in the nineteenth century(2-3).
It is necessary to know the ICD historical evolution, since its appearance to how it is presented today, in order to allow a better diagnoses understanding in assisted patients over the past few years, as well as higher research reliability on the historical subject series.
The ICD creation process as it stands out nowadays is old and complex. When we conducted an epitome history we found that for many years the major concern of the statistical scholars was in relation to diseases that caused of death and not diseases that cause disability and distress for its sufferers.
In the seventeenth century, John Graunt held the first statistical study of disease, in which, in order to estimate the proportion of deaths in children, created a classification of diseases based on the causes. It is important to consider that at that period there was no record of the correlation between mortality and age, which certainly made it difficult to study.
In the years following that first study, important researchers as William Cullen (1710-1790) and William Farr (1807-1883) dedicated themselves to the creation of a diseases classification for causes of death, being implemented in some countries. The big challenge of that period was the inability of international death comparison occurrence of certain causes, since there was no classifications standardization between different countries.
Several discussions on the classification standardization of death causes were performed. In 1853, in Brussels, there was the First International Statistical Congress; in 1855, in Paris, the Second International Statistical Congress; in 1891 a committee was created and chaired by Jacques Bertillon for the development of a death classification that could be adopted worldwide. In the following years there were performed international conferences to review the Classification created by Bertillon(2).
From the sixth review, created in 1948 and started to be used in 1950, the responsibility for works review, publication and dissemination of the International Classification of Diseases was passed to the World Health Organization (WHO). The sixth review conference was the beginning of a new era in the international field of vital and health statistics, especially in relation to mental disorders, because once standardized, the terminologies related to these disorders, these statistics started to be realized with higher property(3-4).
There was an evolution from the sixth to the tenth ICD review, which was the expanding number of categories to classify both morbidity and mortality. ICD is composed of chapters, each chapter is divided into groupings, each grouping is subdivided into categories and, finally, the categories are subdivided into subcategories.
Considering current expectations regarding the development of the 11th ICD review, it is important that discussions are conducted on the changes that occurred over the previous reviews. Thus, this study aimed to describe the creation and evolution of four diagnostic categories of the Chapter V of the International Statistical Classification of Diseases and Related Health Problems, as it is called in its most current review (ICD-10): 1) Mood disorders (affective); 2) Schizophrenia, schizotypal and delusional disorders; 3) Mental and behavioral disorders due to alcohol use; 4) Mental and behavioral disorders due to use of other psychoactive substances.
Material and Method
Interested in psychiatry, the evolution from the sixth to the tenth ICD review is not simple and trivial, but complex by the large number of changes. Therefore, there were described the main changes regarding the ICD evolution on the following diagnostic categories: affective disorders, schizophrenia, and mental and behavioral disorders due to use and abuse of substances.
The reason for the choice of these categories happened after surveying the Unified Health System Database - DATASUS, in which are available for free, easily and friendly, through the site www.datasus.gov.br, all information that can be accessed from the Ministry of Health. The following table shows the impact of these disorders within Brazilian mental health for 2009.

As noted, the mental and behavioral disorders were responsible for 274,808 hospitalizations in Brazil in 2009, equivalent to 2.4% of all SUS (Brazilian Unified Health System) hospitalizations in the country in 2009. When distributed by morbidities, schizophrenia, mood disorders and mental and behavioral disorders because of psychoactive substance use (including alcohol) they were responsible for 90% of the psychiatric hospitalizations.
In this context, it was opted by describing only the categories related to schizophrenia, affective disorders and mental and behavioral disorders related to psychoactive substances use because they were the most frequent diagnoses in psychiatric hospitalizations.
Defined the diagnostic categories, we tried to present them in descriptions tables from the sixth to the tenth ICD review, punctuating each review sequence.
Results
ICD - Sixth Review (1948)5 to ICD - Seventh Review (1955)(6)
While the first reviews of the classification concerned only to death causes, from the Sixth Review, in 1948, its purpose expanded by including non-fatal diseases. It was first called "International Classification of Diseases" with unprecedented participation of the Pan American Health Organization and the World Health Organization
Regarding mental health, ICD named, in the sixth review, the Chapter V - "Mental disorders, psychoneuroses and personality changes." In this chapter there were three groupings, 26 categories, 60 subcategories with codes from 300 to 326. In the ICD-7, the chapter V was renamed to "Mental diseases, psychoneuroses and personality disorders" and there was no increase in the groupings numbers, categories or subcategories.
Some disuse definitions were: schizotimic; psychosis mixed with schizophrenic; manic depressive psychosis; hysteria, compensation neurosis and lying.
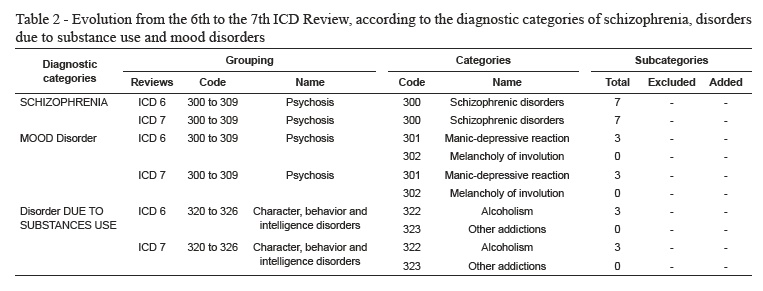
The following table shows the main changes in the diagnostic categories of schizophrenia, disorders due to substance use and mood disorders in the transition from the 6th to the 7th ICD review.
Table 2 shows that schizophrenia is within the psychoses grouping from ICD-6 to ICD-7. Regarding the category, the same code (300) was maintained, name (Schizophrenic disturbances) and subcategories number from ICD-6 to ICD-7.
From ICD-6 to ICD-9, the grouping related to the current affective mood disorders has been named Psychoses, with the same codes 300-309 in the sixth and seventh review. In this grouping there were only two categories: 301 "Manic-depressive reaction" (with three subcategories) and 302 "Involution melancholia" (without subcategories).
It was observed that the Disorders related to alcohol abuse and other psychoactive substances was within the group of Disorders of character, behavior and intelligence in ICD-6 and in ICD-7. In these two ICD versions, the categories and subcategories remained the same, respectively 322 "Alcoholism" and 323 "Other Dependencies", there were three subcategories in the first version. With regard to the categories in ICD-6 and ICD-7, the codes and names remained the same.
ICD - Seventh Review (1955) to ICD - Eighth Review (1965)(7)
The chapter V receives new title "Mental Disorders", which was changed from the previous review. There was a brief explanation that the section was intended for patients with mental disorders, and the chapter was not indicative for mortality classification as primary cause.
There was in the eighth review of Chapter V: three groupings, 26 categories and 131 subcategories. By comparing the seventh to the eighth review, it was found that the groupings and categories number had not changed, while the subcategories obtained an increase from 60 to 131.
For the first time, it appeared in the ICD volumes the term hypomania.
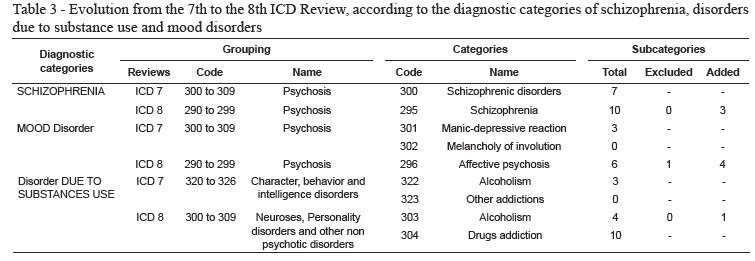
In the ICD-8, in the Schizophrenia grouping, the category code became 295. Three schizophrenia subcategories were added - residual schizophrenia (295.6), schizoaffective type (295.7) and the subcategory Other and Unspecified has been subdivided into two: Other (295.8) and Unspecified type (295.9).
In the CID-8, the category "Affective psychosis" was presented with six subcategories, the categories of past reviews were removed and four new subcategories were added. It is noteworthy that the category "Involution melancholia", found in the 6th and 7th review, was excluded as a category in the ICD-8, but it became a subcategory.
In the ICD-8, the category related to mental disorders due to use of substances was named Neuroses, personality disorders and other nonpsychotic mental disorders. Its code was changed from 322 to 303, but its name was maintained and some subcategories were added: Episodic alcohol excess (303.0); usual alcoholic excess (303.1) and alcohol dependence (303.2). The code 323 was changed to 304, and renamed from "Other drug addiction" to "Drug addiction", with ten more subcategories.
ICD - Eighth Review (1965) to ICD - Ninth Review (1975) (8)
From the ninth review, this classification section differed from the others because it includes a glossary defining the titles meaning, in order to reduce the biases of communication serving as a common reference for professionals in the psychiatry field. This provided a better adjustment in the classification of diagnoses, thus, allowing more reliable statistical analysis.
From the eighth to the ninth review, the groupings number remained the same (3) with the change of a title, in which Mental retardation was renamed to Oligophrenia. The ninth had 30 categories and 180 subcategories.
In the ICD-9 the only modification in the category Schizophrenia was referring to the name that became Schizophrenic Psychoses.
Regarding mood disorders, the codes 290-299 were kept in the 8th and the 9th review. From the 8th revision, made up of two categories and have started to have a category - 296 "Affective Psychosis".
In the ICD-9 the category "Affective psychosis" had 9 subcategories, 5 subcategories were added and 2 subcategories were excluded in relation to previous reviews. In addition, the term "Neuroses" was replaced by "Neurotic disorders" in the grouping name.
In ICD-9 the codes 303 and 304 remained the same from the previous ICD, however, the name of the code 303 was changed from "Alcoholism" to "Alcohol dependence syndrome", without subcategory, and in the code 304 the previous subcategories were excluded, and the following subcategories were added: Opium, opium alkaloid of opium and its derivatives (304.0); synthetic analgesics with effects similar to morphine (304.1); Barbiturates (304.2); Other hypnotics and sedatives or "tranquilizers" (304.3); Cocaine (304.4); Cannabis sativa (marijuana) (304.5); Other psychostimulants (304.6); Hallucinogens (304.7); Other (304.8) and Unspecified drug (304.9).
In that same ICD review, there was the addition of the category whose code is 305 and named "Drug abuse without dependence," with ten subcategories.
ICD- 9th Review (1975) to ICD - 10th Review of 9 ICD (1995)
The tenth review was renamed International Statistical Classification of Diseases and Related Health Problems, differently from what was happening since the sixth review. This title change emphasized the capacity of statistical purposes which, since that moment, has an emphasis on morbidity. Although the name has changed, the acronym remained the same: ICD.
There was a major change in the ICD-10, the codes were changed to alphanumeric to enable better expansion. It is believed that alphanumeric codes have enabled a better balance between the chapters' contents, as well as opened space for future additions and changes without needing to restructure the whole system.
To Chapter V that was named "Mental Disorders" the term Behavioral was added, thus, called "Mental and Behavioral Disorders." It was also found that in ICD-9 there were 3 groups, 30 categories and 180 subcategories. In ICD-10, with substantial expansion, it was from 3 to 11 groupings; from 30 to 78 categories and from 180 to 274 subcategories, with codes ranging from F00 to F99.
For better visualization, they will be presented in a table comparing the changes regarding the categories related to schizophrenia, affective disorders and mental disorders due to use substances.
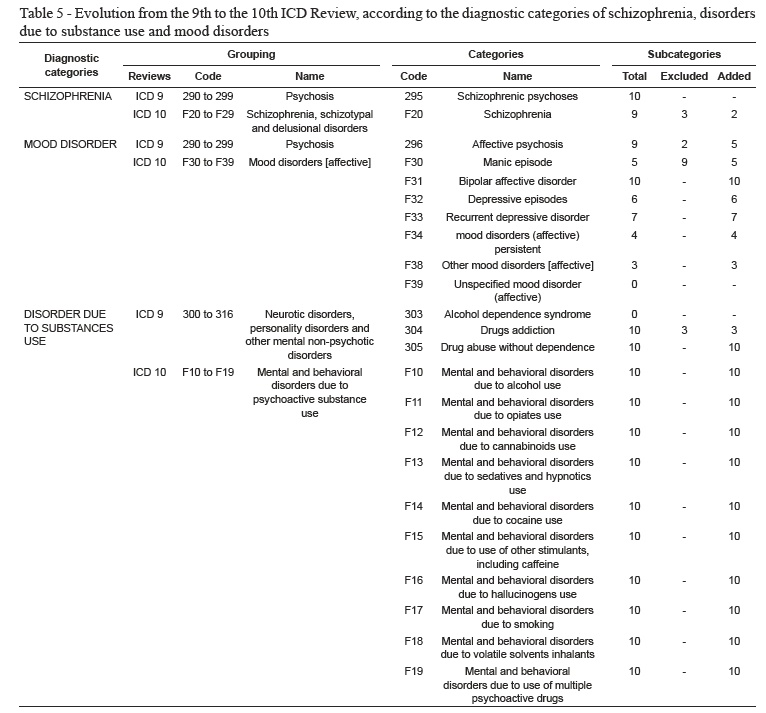
In the ICD-10, the psychoses grouping is called "Schizophrenia, schizotypal and delusional disorders." Regarding the category, Schizophrenia was F-20, in the previous ICD it was 295 Schizophrenic psychosis.
In the ICD-10, the grouping that covers schizophrenia, schizotypal and delusional disorders (F20 - F29) has been expanded by the introduction of new categories such as schizotypal disorder and persistent delusional disorders. The mild psychosis rating was also considerably expanded.
In schizophrenia category (F20) there were also added two new subcategories, undifferentiated schizophrenia (F20.3) and post-schizophrenic depression (F20.4). Furthermore, there were excluded the subcategories acute schizophrenic episodes, latent schizophrenia and schizoaffective type, the first and second were present since the sixth review and the last was present since the eighth.
Mood disorders (affective), named in the ICD-10, underwent abrupt changes along the ICD reviews, and it is current presented in a very different name compared to what was presented in the previous reviews.
With regard to the 10th revision, the changes were quite evident. The grouping came to be called differently from previous reviews. From the 6th to the 9th review, the grouping was called "Psychosis", in the 10th review it was called "Mood disorders (affective)," coded from F30 to F39.
It is clear that the classification of affective disorders in ICD 10 has been presented in order to follow the principle of gathering disorders on common issues. In ICD 10 there were presented 10 subcategories all different from what had been so far presented by previous reviews. Bipolar disorder was included in the ICD for the first time. Terms such as "neurotic depression" and "endogenous depression" are no longer used, but their equivalents can be found in different types and severities of depression now specified. There was also included "dysthymia" diagnosis (F34.1).
In relation to disorders due to substance use, in ICD-10 there were grouping, categories and subcategories changes. The grouping was named Mental and behavioral disorders due to psychoactive substance use and codes from F-10 to F-19. These codes were subdivided into 10 categories according to the different types of psychoactive substances, such as: alcohol, opioids, cannabinoids, sedatives and hypnotics, cocaine, caffeine, hallucinogens, tobacco, volatile solvents, and other psychoactive substances. All these categories were added with 10 subcategories, respectively defined: .0 Acute intoxication; .1 Harmful to health; .2 Dependence Syndrome; .3 Abstinence syndrome [state]; .4 Abstinence syndrome with delirium; .5 Psychotic disorder; .6 Amnesic syndrome; .7 Residual and late-onset psychotic disorder; .8 Other mental or behavioral disorders and .9 Unspecified mental or behavioral disorder.
Final Consideration
From the sixth to the tenth ICD review there were significant changes, incorporations of new definitions and redefinitions, particularly in relation to mental health. Whatever are the studies related to this area, it is essential ICD knowledge for coding, selection of causes and different concepts used over the years.
Regarding the ICD chapter V, it was found that the changes followed the course of the diseases and psychiatric disorders that were named with expressions referring prejudice and exclusion, but also following its own evolution in the international psychiatric classification.
These several changes make difficult to obtain Brazilian statistical data on mental health in a historic series. We observed the lack of mental health indicators in the DATASUS, such as morbidity rate for depression and alcohol use and abuse and other drugs.
We also concluded, with respect to chapter V, that only the retrospective studies from the ICD-9 are viable, because only after this review there was a higher system of codes stabilization and less review discontinuity. Finally, it is not only expanding the number of categories that should be cited rather than the content of chapter V became more logical, i.e., less susceptible to change and with more correlated categories and subcategories.
References
1. Santos-Júnior A, Lima e Silva LFA, Banzato CEM, Pereira MEC. Avaliação qualitativa sobre o que os psiquiatras brasileiros esperam das classificações diagnósticos. Rev Psiquiatr Rio Grande do Sul. 2009;31(2):112-5. [ Links ]
2. Costa-Júnior M L. Estatística de Saúde on-line teoria e prática. [Livre-docência]. Ribeirão Preto: Escola de Enfermagem de Ribeirão Preto da Universidade de São Paulo; 2006. [ Links ]
3. Laurenti R. As manifestações de sofrimento mental mais frequentes na comunidade. SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) [Internet]. 2007;[acesso 13 jan 2013]. 3(2). Disponível em: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1806-69762007000200007&lng=pt&nrm=iso&tlng=pt [ Links ]
4. Grassi PR, Laurenti R. Implicações da introdução da 10ª Revisão da Classificação Internacional de Doenças em análise de tendência da mortalidade por causas. Inf Epidemiol SUS. jul-set 1998;2(3):43-7. [ Links ]
5. Ministério da Educação e Saúde (BR). Manual da classificação internacional de doenças, lesões e causas de óbito. Sexta Revisão. Rio de Janeiro: Ministério da Educação e Saúde; 1952. [ Links ]
6. Organização Panamericana da Saúde. Manual da classificação internacional de doenças, lesões e causas de óbito. Sétima revisão. Washington, DC: OPS; 1964. [Versão em português] [ Links ].
7. Organização Panamericana da Saúde. Manual da classificação internacional de doenças, lesões e causas de óbito. Oitava revisão. Washington, DC: OPS; 1969. [Versão em português] [ Links ].
8. Organização Mundial da Saúde. Manual de classificação internacional de doenças, lesões e morte. Nona revisão, 1975. São Paulo: Centro Colaborador da OMS para a Classificação de Doenças em Português; 1978. [ Links ]
9. Organização Mundial da Saúde. Classificação internacional de doenças e problemas relacionados à saúde. Décima revisão. São Paulo: Centro Colaborador da OMS para a Classificação de Doenças em Português; 1993. [ Links ]
 Correspondence
Correspondence
Mey Fan Porfírio Wai
Av. Bandeirantes, 3900
Bairro: Monte Alegre
CEP: 14040-902, Ribeirão Preto, SP, Brasil
E-mail: meyfan@hotmail.com
Received: Sept. 12th 2011
Accepted: Mar. 20th 2013

{kind=link}
{kind=link}
{kind=link}
{kind=link}