










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versión On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.9 no.3 Ribeirão Preto dic. 2013
http://dx.doi.org/10.11606/issn.1806-6976.v9i3p136-143
ORIGINAL ARTICLE
Psychosocial characteristics of patients with a history of suicide attempts at a Center for Psychosocial Care (CAPS)
Características psicosociales de usuarios de un caps con historia de tentativa de suicidio
Maria Ivoneide Veríssimo de OliveiraI; José Gomes Bezerra FilhoII; Maria Vilma Neves de LimaII; Caroline Carneiro FerreiraIV; Larissa Uchoa GarciaIV; Leirylane de Souza Pereira GoesV
IMSc, RN, Centro de Ciências da Saúde, Universidade Federal do Ceará, Fortaleza, CE, Brazil
IIPhD, Adjunct Professor, Faculdade de Medicina, Universidade Federal do Ceará, Fortaleza, CE, Brazil
III MSc, RN, Secretaria Municipal de Saúde, Fortaleza, CE, Brazil
IVUndergraduate student in Pharmacy, Universidade Federal do Ceará, Fortaleza, CE, Brazil
VMasters student, Universidade Federal do Ceará, Fortaleza, CE, Brazil
ABSTRACT
Objective - To identify the psychosocial characteristics of patients with a history of suicide attempts at a CAPS Fortaleza, Ceará, Brazil. Of the sample, 64.6% were female, 76% with ages varying from 30-59 and 65.5% were unmarried. The bivariate analysis with outcome (more than one suicide attempt), showed an association of p <0.05 with not working, does not like the work, history of psychiatric confinement, hospital care, referred to the CAPS. In the multivariate analysis, the association with psychiatric confinement was identified as a risk factor, the hospital care as a protective factor, as well as the referral. The significant factors remained the same in the model: psychiatric confinement as a risk factor, referral and hospital care, as a protective factor.
Descriptors: Suicide; Suicide, Attempted; Risk Factors; Personal Protection.
RESUMEN
Objetivo-Identificar características psicosociales de usuarios de un CAPS con historia de tentativa de suicidio. Fortaleza-Ceará-Brasil. De la muestra, 64,6% eran del sexo femenino, 76% entre 30-59 años, 65,5% sin compañero. En el análisis bivariado con final (más de una tentativa de suicidio), hubo asociación p<0,05 con no trabajar, no le gustar el trabajo, historia de internaciones psiquiátricas, servicio hospitalario, encaminamiento a los CAPS. En el análisis multivariado, asociación con internamientos psiquiátricos como factor de riesgo, servicio hospitalario como factor de protección, como también encaminamiento. Permanecieron significativas en el modelo: internaciones psiquiátricas como factor de riesgo, encaminamiento y servicio hospitalario, como factor protector.
Descriptores: Suicídio; Intento de Suicidio; Factores de Riesgo; Protección Personal.
INTRODUCTION
Suicide means the action of taking his own life. In a classic work from the nineteenth century (1898), Emile Durkheim offers this definition: Suicide is applied to all cases of death resulting directly or indirectly from a positive or negative act of the victim himself, which he knows will produce this result(1). He classifies this act as a social phenomenon and divides it into four types: egoistic, altruistic, anomic, and fatalistic. While egoistic is the result of excessive individuation, with emphasis on the autonomy of the individual conscience and the absence of significant family or social interactions; the anomic joins the unruliness, crises, and changes by the weakening of the social fabric, and the altruistic is explained by the subordination of the individual to social purposes, act perceived as a duty, an impersonal gesture. Regarding the fatalistic, though seen as of little contemporary relevance, according to the author that happened when an individual is too-ruled governed. In this scenario, the oppression of the individual resulted in a feeling of helplessness before fate or society(2).
About its etiology, there are some significant risk factors, such as the psychosocial ones, chronic diseases, biology, personality, psychiatric disorders, and the genetic and family histories as particularly important(3).
Presently, suicide is considered a public health problem in many countries, especially in Brazil, as a developing country. It affects all social classes, and despite prevention efforts, it has seen a dramatic increase in the past years(4).
According to certain authors, the suicidal behavior is classified into three different categories or domains: suicidal ideation, suicide attempt and completed suicide(3). Suicidal behavior is seen as "any act by which a person causes injury to himself, whatever the degree of lethal intent and knowledge of the real reason of this act. This notion merges the suicidal behavior with the idea of self-destruction and moves from the threat and gesture to attempt, and finally consummates the act of suicide(5). Suicidal ideation refers to thoughts of self-destruction or suicidal ideas. It encompasses individual desires, attitudes or plans to take his own life Probably the early identification of the ideas helps prevent attempts and to prevent a successful self-harm(3). In the suicide plan, the individual is determined to put an end to his life, he plots the death, and details such as the method, place, and time(6). In addition to the risk factors mentioned, certain authors suggest that patients suffering from psychiatric disorders have more than a 50% chance of committing suicide(7).
In a relevant study, the authors mentioned that among those who attempt suicide, 10 to 15% complete the act(8). Depression and physical illness were the main risk factors associated with attempted suicide in the elderly(9). Although it is impossible to predict suicide, rates among the general population can be reduced with the proper assistance from professionals skilled in the identification and treatment of risk factors(8).
Worldwide, the suicide mortality rate, is of about 16 cases per 100,000 populations(1). In Brazil is the averages 4.5/100,000 (Pop.). Therefore, relatively low on a global-scale. However, among the cities, regions, and population groups (e.g., young people in large cities, indigenous people from the Midwest and North, and among the farm workers of the Rio Grande do Sul); the numbers approach or exceed the countries with high rates, such as in Eastern Europe and Scandinavia. As reported, the suicide rates have increased in the country, especially among the youth and young adult males(6).
In Ceará, in 2004, the suicide mortality accounted for 9.4% of the deaths recorded, with the highest concentration among males(10). In Fortaleza, from 1998 to 2008, there were 1,299 suicide deaths, 1,040 males and 259 females. Among men, the mortality rate was about 9.9 per 100,000 (Pop.), in addition the rate among women was about 2.2 per 100,000 (Pop.)(10).
In the case of a suicide attempt, the outlook is far more serious. As the data demonstrates, the numbers may be up to forty times greater than the suicides. Per the World Health Organization (WHO) in a global perspective, the rates maybe twenty times higher. The injuries or traumas resulting from suicide attempts are the sixth leading cause of health problems and physical disability among young people ages 15-44. This represents a serious public health problem worldwide, affecting increasingly younger people, with serious damage to health, including psychological and social-economic factors(11). Suicide attempts have considerable impact on health services and, according to the estimates, 1.4% of the global disease burden in 2002 were caused by suicide attempts. That figure is expected to reach 2.4% in 2020(6). The WHO also highlights that someone somewhere in the world commits suicide every 40 seconds and that someone tries to take their own life every three seconds For every suicide, there are at least ten attempts serious enough to require medical attention, and for each recorded attempt there are four unreported ones. Suicide has a visible impact on at least six people, within the family, friends and others; the psychological, social, and financial impact is immeasurable(5). This research is a result of the paucity of data on the subject matter available in Fortaleza, developed as part of a doctoral thesis, which aims to describe the main characteristics of suicide attempts victims staying at the public institutions of this city, from June 2011 to May 2012. Based on the national and international literature, a study was conducted to identify the psychosocial characteristics of patients with a history of suicide attempt being treated at a CAPS.
METHODOLOGY
This is a cross-sectional, descriptive, analytical study developed at the Center for Psychosocial Care (CAPS) in Fortaleza, the capital of state of Ceará, Brasil. It attends patients referred by other health services as psychiatric emergencies or that were released from hospital confinement The referred center belongs to the Regional III from the municipal Health Department, which includes the Fortaleza metropolitan area.
The sample consisted of all patients diagnosed with suicide attempt, being attended at the CAPS. Data collection took place for twelve consecutive months, in twelve hour shifts three times a week, in the form of psychiatric care between June 2011 and May 2012. It started with an analysis of the charts from all patients scheduled for medical care after a suicide attempt. During the consultation, after the identification, the patient was invited to participate in the study.
The data collection consisted of interviews lasting an average thirty minutes following a standardized form used by nurses, pharmacists, and other professionals previously trained and supervised by the technicians from the Violence Group, School of Medicine/Federal University of Ceará. The sample integrated 113 patients identified with suicide attempts. The survey included every victim with attempted suicide at least once, during any period of their lives. There were no exclusions. During the analysis of the medical records, those with doubtful diagnosis of suicide attempt, or unable to answer the questions were not selected. The investigation included the following variables: gender, age, education level, marital status, household income, having a job, religion, enjoy work, have friends, psychiatric confinement, type of care, and referral.
The research employed the tenth revision of the International Classification of Diseases (ICD-10), comprising the categories x60 to x84. The data was analyzed employing the Stata, version 10 software, using descriptive statistics with the preparation of absolute frequencies and percentages, organized in tables and analyzed according to the related literature. Bivariate analysis was performed between the outcome variable (more than one suicide attempt), and the combined predisposing factors using the Fisher exact test with p <0.050. In the final model, the multivariate logistic regression included the variables statistically significant at p<0.20.
The Ethics Committee on Research of the Maternity-School Assis Chateaubriand/Federal University of Ceará approved the research according to the Resolution No. 196, from 10/10/1996, from the National Health Council.
RESULTS
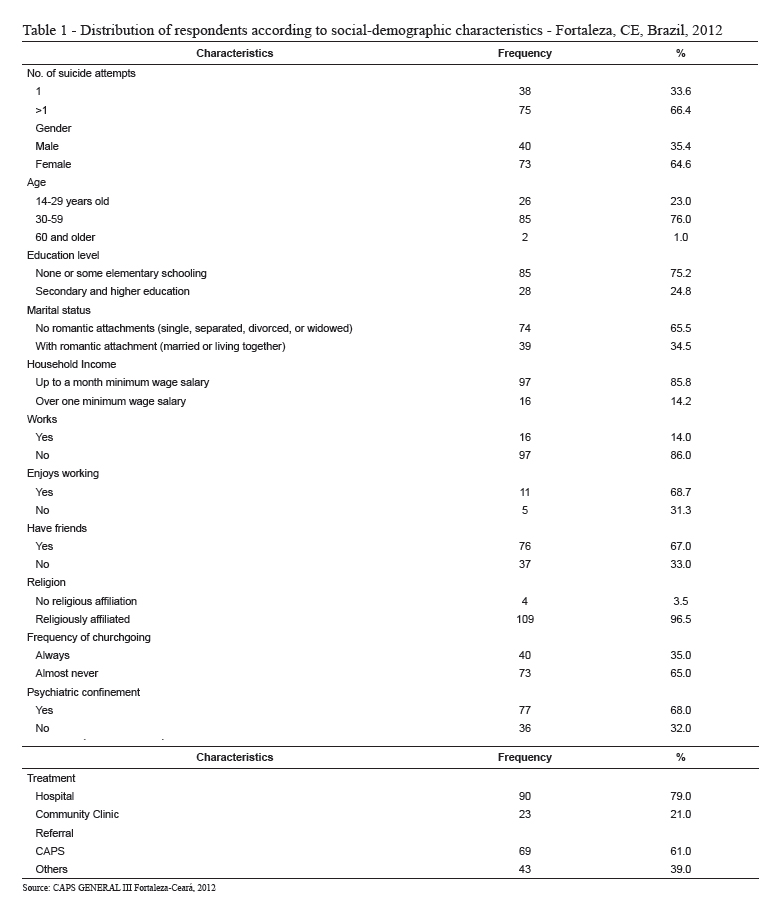
Table 1 shows the social-demographic characteristics of the participants. Of the 113 victims surveyed, 66.4% had attempted suicide more than once. Of these, 64.6% were females, i.e., over half of the sample. As for age groups, 76.0% were between 30-59 years of age. According to the data, 75.2% had no schooling or some elementary school education. Regarding marital status, the highest rate of suicide attempts occurred among patients without romantic attachments (65.5%). In regard to income, the majority (85.8%) received up to one month minimum wage salary. Moreover, the minority had work, 16 (14.0%), and among these, 68.7% were motivated to do so. As for a social life, 67.0% reported having friends. Furthermore, there was a predominance of religious affiliations (96.5%). However, the majority (65.0%) almost never went to church. As a whole, 68.0% had a history of psychiatric confinement. The hospital care was higher (79.0%) after the attempted suicide, when compared to the community clinic. Of the total, 61.0% were referred to the CAPS.
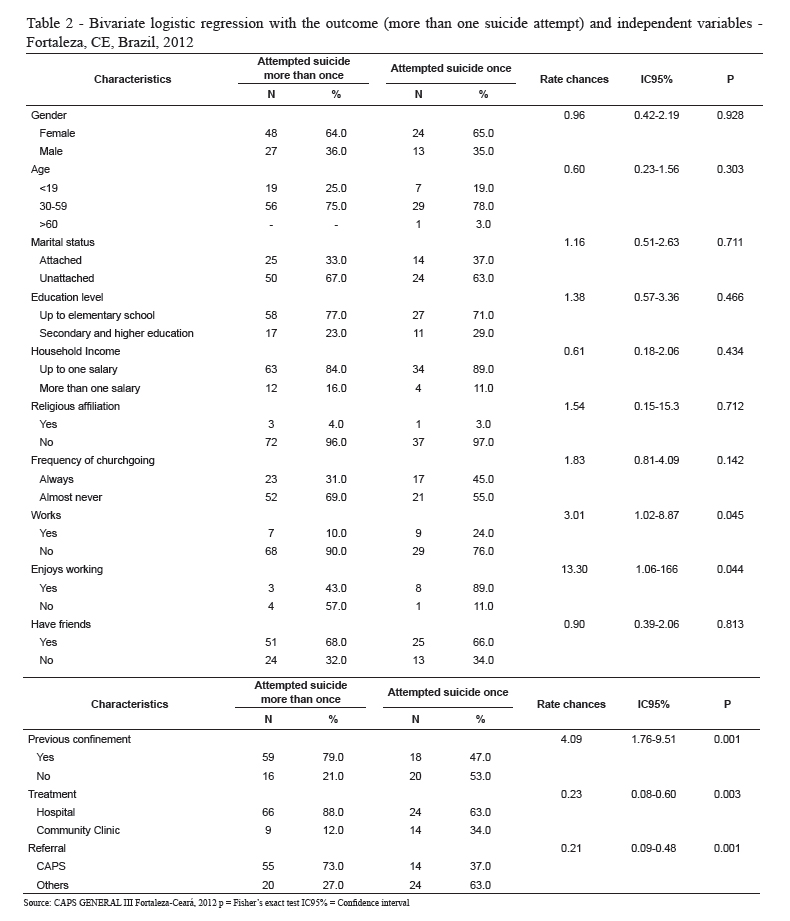
Table 2 shows the bivariate analysis between the outcome (more than one suicide attempt) and the independent variables. As noted at the outset, the variables gender, age, marital status, education, household income, religion, frequency of churchgoing, and friends do not show statistical variance, p> 0.05.
Not working was associated with more than one suicide attempt, RC = 3.01 (IC 95%: 1.02-8.87) P = 0.045. Victims who reported disliking work denoted thirteen times greater risk of attempting suicide than those who reported enjoying it, RC = 13.3 (IC95%: 1.06-1.66), P = 0.044. Likewise, victims with a history of psychiatric confinement demonstrated significance associated with the outcome studied, RC = 4.09 (IC95%: 1.76-9.51), P<0.001. As for the type of care after the suicide attempt, the hospital functioned as a protective factor, RC = 0.23 (IC95%: 0.08-0.60), P<0,001. With respect to referrals, related to the outcome, it was also related to protective factors, RC = 0.21 (CI95%: 0.09-0.48), P<0.001.The multivariate logistic regression analysis included variables significantly associated with the outcome (more than one suicide attempt) with p < 0.20
Table 3 shows that in the multivariate logistic regression analysis, after controlling the confounding factors with the independent variables, the risk of more than one suicide attempt remained statistically significant with: History of psychiatric hospitalization over a suicide attempt, OR = 3.55 (IC95% 1.44 to 8.75) p = 0.006; Hospitalization after a suicide attempt has significant prevalence with the protective factor, OR=0.30 (CI95% 0.10 to 0.86) p = 0.026, as well as the referral to the CAPS, OR= .56 (CI95% 0.32-0.97) P = 0.040.
DISCUSSION
The sample contained 113 victims. Of these, 66.4% have made more than one suicide attempt. An alarming situation since the literature demonstrates an increased risk of suicide for people with a history of previous attempts(12).
As noted, 64.6% (n = 73) of the suicide attempts were from females, which corroborates the literature(3-13). According to a study conducted in Ribeirão Preto - SP, the victims in 77.8% of the cases were females(14). However, a study conducted in Minas Gerais, between 1998 and 2003 from 14,443 admissions in the Unified Health System (SUS), 55.4% were males(5). As for the age, 76.0% were from 30 to 59 years of age. In Minas Gerais, a study identified two peaks of the suicide rate among young people (10-14 and 15-19 years of age) (5). In an emergency room, in Fortaleza, in 2000, two other peaks were also identified: 35% between 21 and 30 years of age and 32% between 10 and 20(13).
It has also showed that 75.2% of patients had no education or some elementary schooling. The research confirms the findings of a study conducted in Itabira (Minas Gerais), which demonstrated that the majority of the suicide victims are people with only elementary education. According to the authors, this may be a result of the lack of opportunities in the social and economic environments(15). Furthermore, low educational levels (66.7%) are also found among the victims in a hospital located in Rio de Janeiro(8).
This study demonstrated a predominance of patients without romantic attachments (65.5%), consistent with an epidemiological analysis of suicide in Brazil conducted from 1980 to 2006(12), and in Mato Grosso do Sul(16). As the results of epidemiological studies show, in general, the suicide rate is higher among single, widowed or divorced persons than among the married ones(17). Of the victims, 97 (85.8%) reported household income below the poverty level; thus, more likely to attempt suicide because of social-economic difficulties. These data corroborate a study on suicide attempts and deaths in Ceará, in which the majority had income below the minimum wage levels(18).
The same study demonstrated that only a small proportion of people worked (14.0%); however, the majority (68.7%) would like to do so. The authors demonstrate an association between work with better health and lower risk of mortality(19). As for companionship, the majority (67.0%) reported having friends. Regarding the suicide planning, maintaining healthy relationships with friends and colleagues is of extreme importance as a protective factor for quality of life(3).
It highlighted the predominance of patients with religious affiliations (96.5%), although the majority (65.0%) rarely attended worship services. Therefore, confirming a study conducted in Rio Grande do Sul that religion is among the protective factors against suicide attempts (3).
In the sample, the variable psychiatric hospital confinement accounted for 68.0% of the attempts. As for the prevention of suicidal behavior, the majority of the victims are individuals with severe psychiatric disorders, often requiring hospital confinement(20). In this light, hospital care after the suicide attempt was essential (79.0%). According to the literature, patients with suicidal behaviors usually have a previous diagnosis of mental illness, which increases the risk of suicide attempts with serious injuries that often requires hospital care(21).
At last, referrals for treatment in the CAPS reached 61.0% of the sample. The care in specialized health services seems to be the most effective form of prevention. According to a study conducted in Gotland, Sweden, there was a decrease in the suicide rates among the patients under medical care(22).
In the bivariate analysis, the not working variable is higher when compared with the suicide attempts among workers. These findings are corroborated by a study on the epidemiological characteristics of suicide conducted in Rio Grande do Sul, in which the authors found a statistical association between unemployment and suicide, it may also affect their mortality rates(23). Moreover, participants who said they did not like to work presented more than thirteen times higher risk of suicide attempt, compared with the others. Unemployment is a risk factor. Job and life satisfaction in addition to positive adaptability are protective factors(24).
It is intriguing to note that, among variables in a statistical association with outcome, there is statistical significance between more than one suicide attempt and a history of admissions to psychiatric hospitals. In the sample, 79.0% had a history of prior hospital confinement with more than one attempt and the risk of four more times. However, in a study conducted in São Paulo, there were no association between suicide attempts and psychiatric confinements(25).
The ratio between hospital care and the number of suicide attempts was strongly associated as a protective factor when compared to those without care. The system is essential for the capture of such cases, with the potential for collecting meaningful information for future use in support of policy making, prevention, and effective protection to reduce the damage in the population.
Furthermore, the monitoring in health facilities such as the CAPS is critical, with excellent statistical significance to the outcome, as a protective factor. The medical care is an experience in mental health, in which situations are observed, analyzed and efforts are made toward providing quality of life to people. According to certain authors, the best strategy for high-risk populations is to improve health services and develop effective interventions in patients with a suicide attempt, with the appropriate monitoring(24). In this context, knowledge of the epidemiological profile is a step toward the role of suicide prevention, as well as paving the way for the training of health professionals focused on the specific care, to identify suicide risks, as well as the implementation of intervention plans.
Throughout the study, there were some methodological limitations. During the data collection, as a result of a reduction in the number of psychiatrists working at the CAPS, fewer victims were attended, and consequently interviewed.
It is noteworthy that the sample was not representative of all attempted suicide cases registered in the municipality of Fortaleza. It consisted only of those seeking care at the CAPS located at the Regional III, from the Health Department. Therefore, the behavior of those who attempt suicide, and seek private medical care is unknown.
CONCLUSION
As for the results, certain points should be considered: the propensity of more women attempting suicide than man, the lower educational levels, lack of romantic attachments, and lower incomes. The victims with a history of psychiatric confinement are at a higher risk, compared with those without a history. As the research shows, it is necessary to further examine the data, in particular the adoption of preventive and intervention measures. The data is not as alarming when compared to other Brazilian states and capitals; however, particular attention should be given to both the prevention, and the training of the health professionals to minimize the situation.
Knowledge of the profile of those who attempt suicide is essential to the health team since it allows for a better medical care and perhaps, a change of mind from the victim. Since suicide is considered to be a global public health problem; policy makers and health professionals should use educational strategies to value life, improve self-esteem and the prospects of the population segments who are most vulnerable to suicidal tendencies. Given the situation, it is essential that health services are adequately prepared and structured to assist the victims, in conjunction with support networks in monitoring these people. It is hoped that this work will contribute to the achievement of these objectives and the implementation of future studies, aimed at the prevention and intervention in the lives of individuals exposed to such acts.
REFERENCES
1. Parente ACM, Soares RB, Araújo ARF, Monteiro CFS. Caracterização dos casos de suicídio em uma capital do Nordeste Brasileiro. Rev Bras Enferm. julho-ago 2007;60(4):377-81. [ Links ]
2. Durkheim E. O suicídio. São Paulo: Martin Claret; 2008. 358 p. [ Links ]
3. Werlang BSG, Borges VB, Fensterseifer L. Fatores de Risco ou Proteção para a Presença de ideaçcão suicida na adolescência. Rev Interam Psicol. 2005;39(2):259-66. [ Links ]
4. Organização Mundial da Saúde. Prevenção do suicídio: um manual para profissionais das equipes de saúde mental. Brasília: OMS; 2006. [ Links ]
5. Abasse MLF, Oliveira RC, Silva TC, Souza ER. Análise epidemiológica da morbimortalidade por suicídio entre adolescentes em Minas Gerais, Brasil. Ciênc Saúde Coletiva. mar-abr 2009;14(2):407-16. [ Links ]
6. Botega NJ. Suicídio: saindo da sombra em direção a um Plano Nacional de Prevenção. Rev Bras Psiquiatr. set-dez 2007; 29(1):7-8. [ Links ]
7. Ruengorn C, Sanichwankul k, Niwatananun W, Mahatnirunkul S, Pumpaisalchai W, Atumanond J. A risk-scoring scheme for suicide attempts among patients with bipolar disorder in a Thai patient cohort. Psychol Res Behav Manage. 2012;(5):37–45. [ Links ]
8. Soloff PH, Chiappetta L. Prospective Predictors of Suicidal Behavior in BPD at 6 Year Follow-up. Am J Psychiatry 2012 May;169(5):484–90. [ Links ]
9. Pires MCC, Kurtinaitis LCL, Santos MSP, Passos MP, Sougey EB, Bastos OC Filho. Fatores de risco para tentativa de suicídio em idosos. Neurobiologia. out-dez 2009;72(4):21-8. [ Links ]
10. Ceará. Secretaria da Saúde do Estado. Doenças e agravos não transmissíveis - DANT no Ceará: situação epidemiológica, 1998 a 2004. Fortaleza: SESA; 2006. [ Links ]
11. Ministério da Saúde (BR). Relatório mundial de saúde 2003: Construindo o Futuro. Genebra: Organização Mundial de Saúde; 2003. [ Links ]
12. Lovisi GM, Santos AS, Legay L, Abelha L, Valencia E. Análise epidemiológica do suicídio no Brasil entre 1980 e 2006. Rev Bras Psiquiatr. 2009;31 Suppl 2:S86-93. [ Links ]
13. Regadas RP, Veras TN, Lins EB, Cavalcante LO, Aguiar JC, Davis M. Tentativas de suicídio por auto envenenamento: um estudo retrospectivo de 446 casos. Pesq Med Fortaleza. jan-dez 2000;3(1-4):50-3. [ Links ]
14. Avanci RC, Pedrão LJ, Costa ML Junior. Tentativa de suicídio na adolescência: considerações sobre a dificuldade de realização diagnóstica e a abordagem do profissional de enfermagem. SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) (Ed. port.) [Internet]. 2005. [acesso 5 junho 2012];1(1). Disponível em: http://www.revistasusp.sibi.usp.br/scielo.php?pid=S1806-69762005000100007&script=sci_arttext.
15. Souza ER, Minayo MCS, Cavalcante FG. O impacto do suicídio sobre a morbimortalidade da população de Itabira. Ciênc Saúde Coletiva. 2006;11 Supp 1:S1333-42. [ Links ]
16. Santos J. Suicídio em Mato Grosso do Sul, Brasil: fatores sociodemográficos. [Tese de Doutorado]. Rio de Janeiro (RJ): Escola de Saúde Pública da Fundação Oswaldo cruz; 2010. 65p. [ Links ]
17. Bezerra JG Filho, Werneck GL, Almeida RLF, Oliveira MIV, Magalhães FB. Estudo ecológico sobre os possíveis determinantes socioeconômicos, demográficos e fisiográficos do suicídio no Estado do Rio de Janeiro, Brasil, 1998-2002. Cad Saúde Pública. jan-mai 2012;28(5):833-44. [ Links ]
18. Pordeus AMJ, Cavalcanti LPG, Vieira LJES, Coriolano LS, Osório MM, Ponte MSR, et al. Tentativas e óbitos por suicídio no município de Independência, Ceará, Brasil. Ciênc Saúde Coletiva. nov-dez 2009;14(5):1731-40. [ Links ]
19. Denney JT, Rogers RG, Krueger PM, Wadsworth T. Adult Suicide Mortality in the United States: Marital Status, Family Size, ocioeconomic Status, and Differences by Sex. Soc Sci Q. 2009;90(5):1167–85. [ Links ]
20. Botega NJ, Werlang BSG, Cais CFS, Macedo MMK. Prevenção do comportamento suicida. Psico. set-dez 2006;37(3):213-20. [ Links ]
21. Costa J. Tentativa de Suicídio. [Dissertação de Mestrado]. Lisboa (Portugal): Faculdade de Ciências da Saúde. Universidade da Beira Interior. 2010. 78 p. [ Links ]
22. Chachamovich E, Stefanello S, Botega N, Turecki G. Quais são os recentes achados clínicos sobre a associação entre depressão e suicídio? Rev Bras Psiquiatr. 2009;31 Suppl 1:S18-25. [ Links ]
23. Meneghel SN, Victora CG, Faria NMX, Carvalho LA, Falk JW. Características epidemiológicas do suicídio no Rio Grande do Sul. Rev Saúde Pública. dez 2004;38 (6):804-10. [ Links ]
24. Bertolote JM, Mello-Santos C, Botega NJ. Detecção do risco de suicídio nos serviços de emergência Psiquiátrica. Rev Bras Psiquiatria. 2010;32 Suppl 2:S87-95. [ Links ]
25. Moreira CLRL, Brietzke E, Lafer B. General medical comorbidities in Brazilian outpatients with bipolar disorder type I. Rev Psiq Clín. 2011;38(6):227-30. [ Links ]
Received: Apr. 2nd 2013
Accepted: Aug. 14th 2013

{kind=link}
{kind=link}
{kind=link}