










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
On-line version ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.10 no.1 Ribeirão Preto Apr. 2014
http://dx.doi.org/10.11606/issn.1806-6976.v10i1p-3-10
ORIGINAL ARTICLE
DOI: 10.11606/issn.1806-6976.v10i1p-3-10
Alcohol consumption and results in metabolic control in individuals with diabetes before and after participation in an educational process
Consumo de alcohol y los resultados en el control metabólico en los individuos con diabetes, antes y después de la participación en un proceso educativo
Gabriela Marsola OlivattoI; Vívian Saraiva VerasII; Gabriel Guidorizzi ZanettiIII; Ana Carolina Guidorizzi ZanettiIV; Francisco Guilherme Ribeiro RuizV; Carla Regina De Souza TeixeiraVI
IUndegraduate student in Bachelor’s and Teaching Diploma Program in Nursing, Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, WHO Collaborating Centre for Nursing Research Development, Ribeirão Preto, SP, Brazil
IIPhD, Assistant Professor, Centro Universitário Estácio do Ceará, Fortaleza, CE, Brazil
IIIPhysical Educator, Academia da Força Aérea, Força Aérea Brasileira, Pirassununga, SP, Brazil
IVPhD, Professor, Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, WHO Collaborating Centre for Nursing Research Development, Ribeirão Preto, SP, Brazil
VRN
VIPhD, Associate Professor, Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, WHO Collaborating Centre for Nursing Research Development, Ribeirão Preto, SP, Brazil
ABSTRACT
The aim of this study was to analyze alcohol consumption and metabolic control in people with diabetes, before and after an educational process. This study was conducted with 37 persons with diabetes in two Basic Health Units (UBS), in Ribeirão Preto, SP. To obtain the data of the study, the persons responded the AUDIT questionnaire before and after an educational process in diabetes. As a result, it was observed that the average sum of AUDIT was low risk before and after the educational process. Was noticed a small reduction in score of 0.13 at the end of the process. Thus, it is evident the necessity of using a pedagogical model to address alcohol consumption integrated into the educational process.
Descriptors: Diabetes Mellitus; Nursing; Alcoholism; Health Education.
RESUMEN
El objetivo de ese estudio fue analizar el consumo de alcohol y control metabólico de personas con diabetes, antes y después del proceso educativo. Participaron 37 personas con diabetes en dos Unidades Básicas de Salud de Ribeirão Preto, SP. La recogida de datos ocurrió de agosto a diciembre de 2011. Predominó el sexo femenino, diabetes tipo 2 y tiempo medio de enfermedad de 14 años. El consumo de alcohol predominante fue bajero riesgo antes y después del proceso educativo, con pequeña reducción de 0,13 en el score medio del AUDIT, y discreta reducción del 0,20% en los valores de la Hemoglobina glucosada, sin significancia estadística. De esa manera, se pone evidente la necesidad de otros estudios que aborden el consumo de alcohol integrado al proceso educativo.
Descriptores: Diabetes Mellitus; Enfermería; Alcoholismo; Educación en Salud.
INTRODUCTION
Diabetes mellitus (DM) is a heterogeneous group of metabolic disorders which have in common hyperglycemia. This hyperglycaemia is the result of defects in insulin action, insulin secretion or both. The number of subjects with diabetes is increasing due to population growth and aging, greater urbanization, the increasing prevalence of obesity and sedentary lifestyle, as well as increased survival of people with DM(1).
The foundation of treatment of diabetes mellitus requires education of the individual, aiming to make him/her take effective decisions for self-care and in long term it is intended to reduce or prevent chronic complications(1). Thus, continuing education in diabetes implies important changes in the behavior of subjects, as pharmacological regimens, self-monitoring of blood glucose, changes in dietary patterns from nutritional education and realization of planned physical activities and information about the prevention and treatment of acute and chronic complications in order to maintain blood glucose levels within normal parameters(2).
The educational approach must also grasp the subjective and emotional aspects that influence in treatment adherence and self-care. Anyway, it is essential that health education consider the reality and experience of individuals(3). The way and the manner individuals with diabetes react to the disease interfere directly and indirectly in the performance of self-care roles, fitting to the nurse the role of mediator of the relationship emotional reaction and performance of self-care actions(4). These emotional reactions to the chronic condition of diabetes may contribute to another question that has influenced treatment adherence and self-care activities concomitant to the non-use of oral antidiabetic and omissions of doses of insulin, which is the consumption of alcohol.
A set of expectations emerges parallel to alcohol consumption. These expectations influence the decision to drink, as the reward or pleasure, removing any discomfort or suffering, escape, entertainment, relaxation and disinhibition. Expectations of confidence and well-being can also be confirmed by experience with alcohol and strengthen pre-existing expectations(5).
Are few and relatively new the studies correlating alcohol consumption and incidence of diabetes, but the importance of this relationship has been increasing mainly because it is a disease that is reaching epidemic worldwide values and alcoholism that many years is a huge problem of public health(6). Ethyl alcohol or ethanol is a psychic depressor drug of sedative and hypnotic character whose consumption, highly generalized and even encouraged in our society, causes it to be a mandatory part of many social relations, there is a huge social permissiveness regarding alcohol. This is one of the reasons why it is regarded differently when compared to other drugs. The consumption of alcohol may be coming from the current lifestyle, the high level of stress, anxiety, low self-esteem and depressive feelings(7).
The II Household Survey of the Brazilian Center for Information on Psychoactive Drugs (Centro Brasileiro de Informações Sobre Drogas Psicoativas – CEBRID) performed in the 108 largest cities in the country showed that the prevalence of alcohol use was 74.6% and the estimated dependent patients was 12.3% for alcohol(8). As regards persons with diabetes, the rate of alcohol use was 50.8% for adults with diabetes in a study that aimed to link the consumption of alcohol with adherence to self-care in people with diabetes conducted at Kaiser Permanente Northern – Califórnia. It was concluded that such consumption is a marker of poor adherence to treatment in diabetes, even in people with moderate alcohol consumption(9).
Many professionals say they do not investigate the use of alcohol by people because they can not deal with the problem or do not know rapid screening instruments or because they have not reflected on the influence of problematic use of alcohol in the person’s health(10-11). It is verified that the decline in glycated hemoglobin is statistically significant. As the decline in fasting blood glucose total cholesterol, systolic blood pressure, body weight and waist-hip ratio. On the other hand, it is concluded that the effectiveness of educational interventions in dealing with DM treatment adherence lacks clarification and should be studied further(12). In this context, we note the importance of analyzing alcohol consumption and results in metabolic control in individuals with diabetes before and after participation in an educational process.
MATERIALS AND METHODS
This is an observational, longitudinal, comparative of before and after type study, using strategies of quantitative data collection and analysis, conducted from August 2011 to July 2012.
The study site were two Basic Health Units (UBS) in the Western District of Ribeirão Preto – UBS Dr. Sérgio Botelho da Costa Moraes (UBS Jardim Presidente Dutra) and UBS Dr. Alberto Teixeira Andrade (UBS Vila Recreio). The subjects were 52 users with DM monitored by the Program of self-monitoring of capillary blood glucose at home that participated in the education group.
Inclusion criteria were: individuals with DM, older than 18 years, of both sexes, monitored by the Program of self-monitoring of capillary blood glucose at home at UBS Jardim Presidente Dutra and UBS Vila Recreio, who presented cognitive conditions that enabled the participation with minimal ability to understand the issues of data collection instruments and participate in the education group. Thus, 6 did not agree to participate and 9 did not complete the second phase of the study and then 37 users with DM were part of this study.
During data collection it was identified the research subjects who met the inclusion criteria for this study and the researcher explained the research objectives, requesting their participation. The data were obtained through direct interviews in estimated time of 10 minutes by the researcher and were recorded manually on data collection instruments before the group activities.
The data collection instrument was composed of two parts. The first with 07 questions related to sociodemographic variables and with 05 questions related to clinical variables. The second consisted of instrument AUDIT – Alcohol Use Disorder Identification Test(11).
The sociodemographic variables of the study were: gender, age, marital status, education, household income, occupation. The clinical variables diagnostic time, used treatment, comorbidities and glycated hemoglobin (A1c) was considered good metabolic control the individual presenting A1c below 6.5%(1).
It is noteworthy that AUDIT is a screening instrument for risk use, harmful use or dependence of alcohol, is validated in Brazil and assesses the pattern of alcohol consumption, dependence symptoms and problems related to alcohol use(11).
According to the results of a study to assess the reliability and validity of the AUDIT in primary care patients it was obtained the rate of 0.85 for Cronbach’s alpha. It was concluded that the AUDIT is a reliable screening questionnaire and valid tool for identifying risk consumption and alcohol-dependent individuals(13).
Data collection was performed in two (2) phases: at the beginning of education program, characterized as P0 and after completion of the program in 12 weeks, characterized as P5, described below: STAGE 1: it was evaluated the pattern of alcohol consumption and the results of metabolic control in diabetes. During the implementation of the educational program, the analysis of instruments of stage 1 were presented and discussed with the team that approached in their interventions strategies to minimize self-care deficits found. As were also presented to research subjects during each educational topic related to issues of alcohol and its interference with the adherence to medication, diet, exercise practices and monitoring of disease.
The educational program lasted 12 weeks, from August to December 2011. The educational tool used was the TM Conversation Map that was created by Healthy Interactions Inc. (Chicago, Illinois) in collaboration with the American Diabetes Association and sponsored by Merck & Co. The use of this educational tool in group facilitates interaction between educators and persons with DM, enables changing attitudes of the person in relation to diabetes mellitus, the improvement of self-efficacy and increased effective clinical results. The use of TM Conversation Map educational tool allows meaningful conversations among peers. It differs from traditional groups since it enables a more active group approach and involves participants to draft viable personal health goals. STAGE 2: interference and effectiveness of interdisciplinary education group regarding the pattern of alcohol consumption and the metabolic control of patients with diabetes was evaluated.
The researcher applied the same tools previously answered by the subjects in the first stage.
The data collected were organized and typed with building the database with their validation and double feeding. The adopted level of statistical significance is 5% (p<0.05). On the analysis of the results was used the Statistical Analysis System(14) program. The project was submitted for approval of Research Ethics Committee of School of Nursing of Ribeirão Preto, Universidade de São Paulo, under protocol 014/2011.
RESULTS
Regarding sociodemographic variables, it is noteworthy that, of the 37 participants, there was a predominance of 26 (70%) females, 10 (27%) were 55-59 years and 10 (27% ) 65-69 years, 29 (81%) are married or have a consensual relationship, 14 (38%) have not completed primary education, 25 (68%) have wage income between 3-5 minimum salaries, 18 (49% ) work at home, 27 (75%) have type 2 diabetes, 13 (35%) undergo the treatment with oral antidiabetic and insulin, 9 (24%) have, in addition to diabetes, hypertension and dyslipidemia, and 8 (22 %) are obese with hypertension and dyslipidemia. The mean duration of disease of participants was 14 years.
Table 1 shows the total scores of AUDIT, where 34 (91.9%) of the respondents obtained low risk score, and 3 (8.1%) risk use score, and after the educational process, 33 (89, 2%) of people had low risk score and 4 (10.8%) risk use score, and 100% of risk consumption was observed in males.
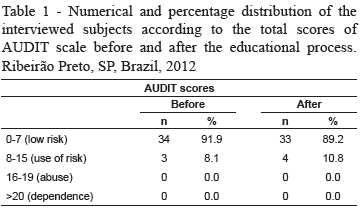
The value increase in the number of risk is explained by the fact that the subject had reported, in the first interview, the question "Has a relative, friend or doctor ever bothered with the fact that you are drinking or suggested you to stop?" that they had never worried about that and after five months a doctor gave them this suggestion. In this population, the prevalence of alcohol abuse and dependence was zero.
Table 2 shows the questions that discuss about alcohol consumption prior to the educational process, it is noteworthy that 16 people reported that they do not consume alcoholic beverages at any time. Before the educational process, three people reported that the frequency of alcohol consumption was 4 or more times per week. Table 3 shows the questions that discuss about alcohol consumption after the educational process and it is noticed that two people have reduced their frequency to 2-3 times a week. The person that maintained 4 or more times a week reported that their doses, before 6 or 7, decreased to 4 or 5. And also reduced the 5 or more doses consumed at one time every week to once per month.
As for the other two people who changed their frequency of alcohol consumption, one person did not alter the dose which was maintained at 4 or 5 doses before and after the educational process while the other person began to think about stopping drinking every week and feel remorse less than once per month. Both reduced the monthly five doses consumed at one time to less than once per month.
In general, the frequency and doses of alcohol improved after the educational process, the same occurred with the consumption of 5 doses at once. As the question relates to quit drinking, two people reported that after the educational process they were afraid of not being able to abstain from alcoholic beverages.
With respect to hemoglobin A1c, the mean obtained before the educational process was 8.38% and after this process was 8.24%, a reduction of 0.20% between before and after shows a slight improvement in metabolic control, but without achieving metabolic control. The sum mean of AUDIT, before and after, was low risk with a small reduction in score of 0.13. Through statistical analysis no evidence of possible statistically significant differences between the before and after times of participation in an educational group of alcohol consumption by people with diabetes.
DISCUSSION
In our findings predominated approximately 90% of the users with low-risk consumption and 50% reported never drinking alcohol. The II Household Survey of the Brazilian Center for Information on Psychoactive Drugs (Centro Brasileiro de Informações Sobre Drogas Psicoativas – CEBRID) performed in the 108 largest cities in the country showed that the prevalence of alcohol use was 74.6% and the estimated dependent patients was 12.3% for alcohol(8).
For adults with diabetes, alcohol use was reported in 50.8% of respondents in a study conducted in California, and 43% consumed less than one dose per day, 4.6% consumed daily doses from 1 to 1.9, 1 , 5% consumed 2 to 2.9 daily doses, and only 1.6% consumed 3 or more doses per day(9). The effects of alcohol use in people who have DM are complex and need further study. It has been suggested that alcohol increases obesity, induces pancreatitis, causes alterations in carbohydrate and glucose metabolism with periods of hypoglycemia when alcohol is consumed excessively and there are long periods of fasting. The effects of alcohol on the DM are classified as short-term such as hypoglycemia, poor metabolic control and metabolic acidosis, and long-term such as hypertension, weight gain and neuropathy(15).
The consumption of alcohol combined with a meal, including carbohydrates, is initially the preferred fuel, leading to an increase in blood glucose and therefore an insulin response. When alcohol is ingested without food and glycogen stores are depleted there is a chance to also develop hypoglycemia due to gluconeogenesis inhibition by alcohol. Another type of hypoglycemia described in relation to alcohol use is the reactive hypoglycemia, probably because of the nature of individual characteristics and the different types of carbohydrates(16).
A population-based study in Shanghai with 3,953 adults showed that alcohol consumption may increase the prevalence of hypertension, hypertriglyceridemia and hyperglycemia. On the other hand, indicates beneficial effects in which alcohol consumption was associated with a lower prevalence of metabolic syndrome, even after adjustment for age and sex(17).
Thus, there is the need to elucidate in literature the relationship between alcohol and improved glycemic control in diabetes. A survey concluded that the long and moderate alcohol exposure improves insulin action without affecting the secretion of β-cell in people with type 2 diabetes, avoiding significant acute changes in their function. This effect may be partly due to the inhibitory effect of alcohol on lipolysis. This evidence could explain the results that indicate that alcohol intake is associated with an improvement in glucose metabolism(18).
The Brazilian Diabetes Society regarding the consumption of alcohol says if the individual choose to drink alcoholic beverages he/she should do within the limit of one dose for women and two doses for men. One dose is defined as 360 mL of beer, 150 mL of wine or 45 mL of distilled beverages. To reduce the risk of hypoglycemia alcoholic beverages should be consumed with food(1).
A population consists of 38,564 adult persons with diabetes was evaluated for the association between alcohol consumption and glycemic control in a period of one year by the Kaiser Permanente Northern California Medical Care Program. In its results also showed that moderate alcohol consumption is associated with better glycemic control, predicting lower glycated hemoglobin levels in approximately 0.5% for an amount of consumption of 2 to 2.9 doses/day, turning into benefits in the prevention of diabetes-related complications. The authors report that this difference is clinically significant and may be compared with the same effect achieved with the beginning of intensive therapy with Metformin(9).
In our findings the predominant use was low risk, no statistical significance in glycated hemoglobin, which remained without achieving metabolic control despite a reduction of 0.20% before and after the participation in educational group, which leads to some questions. It is noted a difficulty in completing the questionnaire, since some information obtained from people seem to be omitted once, in groups, they report their experiences and habits with alcohol but when answering the questions of AUDIT they failed to pass such information, even with the offer of a safe environment without judgment or repression, so that one could get comfortable in speaking the truth, but it is know that these types of omissions occur when answering the instrument.
Thus, even with the small reduction in alcohol consumption reported in this study, the responses to the alcohol habit generate many questions for being vague and imprecise, especially as to the accuracy, since the tendency of the user to deny alcohol abuse not to be labeled as "alcoholic", given the underlying moralistic overtones, this is the main factor that causes patients to minimize their consumption of alcohol(19).
It is questioned to what extent the history obtained on the habits of alcohol intake of a patient should be valued in targeting diagnostic hypotheses, since it is a common question asked in clinical environments both ambulatory and inpatient, which generally is answered as ... "Sometimes, but only a little" ... "one or two doses per day" ... "I drink, but I’m not addicted" ... "I just take alcohol as an aperitif"(19).
The substance use and human behavior are complex issues that require holistic approach continuously in both foci: understanding the cause of the use and application of healthcare practice. Over time, expert authors have developed various healthcare models concerning the understanding of the dimensions of the problem of alcohol and drugs use. Each approach focuses exclusively on one aspect or subset of general phenomena. The nurse since trained, can contribute effectively with their practice in this area of great social relevance. Knowledge of explanatory models may provide ways to subsidize its activities according to the needs of users and health guidelines(20).
Detailed information about the influence of the pattern of alcohol consumption including excessive consumption remains as an important topic for future research. The possible protective effect of moderate alcohol consumption also needs more attention considering the influence of beverage type, frequency of drinking and interaction with other risk factors such as family history of diabetes. Thus, it is need further clinical studies to explore the complex interrelationships between alcohol intake and body weight and obesity, waist-hip ratio, smoking, eating patterns, socioeconomic status, education and physical exercise. It should be avoided recommendations about moderate alcohol consumption for the prevention of type 2 DM, because of possible negative potential effects associated with alcohol consumption for health, not yet clearly elucidated in the literature.
CONCLUSIONS
It is concluded that of the 37 study participants alcohol consumption was low risk and the sum of AUDIT before and after the educational group showed a slight decrease of 0.13 in the score obtained. In relation to the metabolic control, with respect to hemoglobin A1c, the mean obtained before the educational process was 8.38 % and after this process was 8.24% with a reduction of 0.20 % between pre and post, showing a slight improvement in metabolic control with no statistically significant evidence between before and after the participation in educational group on alcohol consumption of people with diabetes.
Thus, to design, plan and guide the brief intervention it is necessary to use a pedagogical model to approach the consumption of alcohol that should be researched and integrated into moments of education. It is also necessary to develop educational programs like this one that aim interventions to improve the living conditions and to clarify questions about alcohol abuse in the presence of diabetes.
REFERENCES
1. Sociedade Brasileira de Diabetes. Diretrizes da Sociedade Brasileira de Diabetes: tratamento e acompanhamento do Diabetes Mellitus. São Paulo; 2011. [ Links ]
2. American Diabetes Association. Recomendações para os portadores de diabetes mellitus. Diabetes Clín. 2001;5(4):258-62. [ Links ]
3. Peres DS, Santos MA, Zanetti ML, Ferronato A. Difficulties of diabetic patients in the illness control: feelings and behaviors. Rev. Latino-Am. Enfermagem. 2007;15(6):1-8. [ Links ]
4. Santos CV Filho, Rodrigues WHC, Santos RB. Papéis de Autocuidado – Subsídios para Enfermagem Diante das Reações Emocionais dos Portadores de Diabetes Mellitus. Esc Anna Nery. 2008;12(1):125-9.
5. Scali DF, Ronzani TM. Estudo das expectativas e crenças pessoais acerca do uso de álcool. SMAD. Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) [Internet]. 2007 [acesso 13 jan 2013];3(1). Disponível em: Disponível em: <http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1806-69762007000100004&lng=pt&nrm=iso> [ Links ]
6. Fraige F Filho. Manifesto de integração e melhoria da atenção integral ao diabetes mellitus no Brasil. Diabetes Clínica. 2004;7(5). [ Links ]
7. Hoffmann MH, Carbonell E, Montoro L. Álcool e segurança no trânsito (I) – epidemiologia e efeitos. Psicol Cienc Prof. 1996;16(1):28-37.
8. Carlini EA, Galduróz JC, Noto AR, Carlini CM, Oliveira LG, Nappo SA, et al. ZVDM. – II levantamento domiciliar sobre o uso de drogas psicotrópicas no Brasil: estudo envolvendo as 108 maiores cidades do país – 2005. São Paulo: Páginas & Letras; 2007.
9. Ahmed AT, Karter J, Liu J. Alcohol consumption is inversely associated with adherence to diabetes self-care behaviours. Diabet Med 2006 Fev;23(7):795-802. [ Links ]
10. Pillon SC, Luis MAV, Laranjeira R. Nurse´s training on dealing with alcohol and drog abuse: a question of necessity. Rev Hosp Clin Fac Med São Paulo. 2003;58(2):119-24. [ Links ]
11. Babor TH, Higgins-Biddle JC, Saunders JB, Monteiro MG. AUDIT – Teste de identificação de problemas relacionados ao uso de álcool – roteiro para uso em atenção primária. Ribeirão Preto: PAI-PAD; 2008.
12. Wens JA, Vermeire E, Hearnshaw H, Lindenmeyer A, Biot Y, Royen PV. Educational interventions aiming at improving adherence to treatment recommendations in type 2 diabetes. A sub-analysis of a systematic review of randomized controlled trials. Diabetes Res Clin Practice. 2008 Mar;79(3):377-88. [ Links ]
13. Daeppen JB, Yersin B, Landry U, Pecoud A, Decrey H. Reliability and Validity of the Alcohol Use Disorders Identification Test (AUDIT) Imbedded Within a General Health Risk Screening Questionnaire: Results of a Survey in 332 Primary Care Patients. Alcoholism Clin Exp Res. 2000 May;24(5):659-65. [ Links ]
14. SAS Institute Inc. SAS/STAT® User’s Guide, Version 9, Cary, NC: SAS Institute Inc.; 2003.
15. Van de Wiel A. Diabetes mellitus and alcohol. Diabetes Metab Res Rev. 2004;20(4):263-7. [ Links ]
16. Torres AS, Castillo Il MMA, GarciaIII KSL. Prevalência de consumo de alcohol en personas con diagnóstico de Diabetes Mellitus tipo 2. SMAD. Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.). [Internet]. 2009 [acesso 13 agosto 2013];5(2):1-13. Disponível em: <http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1806-69762009000200006&lng=pt&nrm=iso [ Links ]
17. Jian-Gao F, Xiao-Bu C, Lui L, Xing-Jian L, Fei D, Jun Z. Alcohol consumption and metabolic syndrome among shanghai adults: a randomized multistage stratified cluster sampling investigation. World J Gastroenterol. 2008 April;14(15):2418-24. [ Links ]
18. Avogaro A, Watanabe RM, Dall’Arche A, Vigili De Kreutzenberg S, Tiengo A, Pacini G. Acute alcohol consumption improves insulin action without affecting insulin secretion in type 2 diabetic subjects. Diabetes Care. 2004 June;27(6):1369-74.
19. Souza LJ, Gicovate C Neto, Chalita FEB, Reis AFF, Bastos DA, Souto JTD Filho, et al. Prevalência de Obesidade e Fatores de Risco Cardiovascular em Campos, Rio de Janeiro. Arq Bras Endocrinol Metab. 2003;47(6):669-76. [ Links ]
20. Pillon SC, Luis MAV. Explanatory models for alcohol and drugs use and the nursing practice. Rev. Latino-Am. Enfermagem. 2004;12(4):676-2. [ Links ]
 CORRESPONDENCE
CORRESPONDENCE
Carla Regina de Souza Teixeira
Universidade de São Paulo. Escola de Enfermagem de Ribeirão Preto
Departamento de Enfermagem Geral e Especializada
Av. Bandeirantes, 3900
Bairro: Monte Alegre
CEP: 14040-902, Ribeirão Preto, SP, Brasil
E-mail: carlarst@eerp.usp.br
Received: Aug. 13th 2012
Accepted: Nov. 11th 2013
