










Servicios Personalizados
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versión On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.10 no.2 Ribeirão Preto ago. 2014
http://dx.doi.org/10.11606/issn.1806-6976.v10i2p61-69
ORIGINAL ARTICLE
DOI: 10.11606/issn.1806-6976.v10i2p61-69
Alcohol and/or drug use: evaluating spiritual and religious aspects
Angelica Martins de Souza GonçalvesI; Manoel Antônio dos SantosII; Sandra Cristina PillonIII
IPhD, Adjunct Professor, Departamento de Enfermagem,
Universidade Federal de São Carlos, São Carlos, SP, Brazil
IIPhD, Associate Professor, Faculdade de Filosofia, Ciências e
Letras, Universidade de São Paulo, Ribeirão Preto, SP, Brazil
IIIPhD,
Full Professor, Escola de Enfermagem de Ribeirão Preto, Universidade de São
Paulo, WHO Collaborating Centre for Nursing Research Development, Ribeirão
Preto, SP, Brazil
ABSTRACT
The aim of this study was to evaluate spiritual and religious aspects in drug and/or alcohol users. It is a descriptive, exploratory study using a quantitative approach. A total of 138 men participated, all with links to rehabilitation institutions or support groups, responding to a socio-demographic questionnaire, the AUDIT-C, and to the Brazilian version of the Spirituality Self Rating Scale. In the sample, 47.1% were alcohol users, 52.9% drug users. The results demonstrated differences between the groups concerning religious aspects: the alcohol users were Catholics (63.1%) or did not practice any religion (50.8%) and the drug users were evangelical (43.1%) or practicing a religion (72.2%). With regards aspects of spiritual practice, no differences were found between the groups. Both were shown to distinguish between the concepts of religiosity and spirituality. The findings broadened understanding of how the nurse can implement care which takes into consideration subjective aspects of the psycho-active substance user in their day-to-day practices.
Descriptors: Spirituality; Religion and Psychology; Substance-Related Disorders.
Introduction
The importance of religion and spirituality in relation to mental health has become increasingly widespread, constituting a phenomenon that has been widely studied in the academic environment, especially related to social sciences and health(1-3). From this perspective, a bibliographical review showed that there had been an increase in the number of publications involving the topics of spirituality and substance use(4).
The literature suggests that there are conceptual differences between the terms "spirituality" and "religiosity"(5-7), as these terms can sometimes be treated as synonyms. Differentiating between the terms considers spirituality as that which gives people a meaning and goal in life, while religiosity is identified with sectarian practice(8), part of an organized belief system with practices, rites and symbols created in order to facilitate individuals' approximation to dimensions of the sacred or the transcendent(7).
Religiosity and spirituality are becoming increasingly valued in the field of mental health, being recognized as a treatment response available to alleviate human suffering, which is both singular and multidimensional, involving mind, body and spirit(1-2,9). Despite this recognition and value of these aspects in the field of knowledge, within health practices there is still little interest in including the spiritual dimension in care due to elevated technology development(2).
Thus, although the role of spirituality in the area of health, as a resource for personal well-being, is known, it is neglected in care practices. Some studies have suggested that nurses are in need of a personal-spiritual perspective in order to be able to provide spiritual care(10-12). This care could be developed by acquiring knowledge that assists these professionals to acquire spiritual care skills and abilities, so as to help patients deal with their own spirituality(11).
From the patient's point of view, especially those recovering from addiction, the relevance lies in the fact that higher levels of religiosity and spirituality are predictors of a more optimistically oriented view of life, better social support, greater resilience to stress and lower levels of anxiety. The literature indicates that spiritual practices are associated with sobriety, remaining abstinent and promoting attitudes that facilitate the process of entering treatment, as a resource of personal strength(3,13). On the other hand, the mechanisms through which spirituality influences such recovery processes are little known, due to their complexity(4,14).
Moreover, reviews of spirituality in the area of addiction have concluded that the way in this construct us defined and measured is frequently precarious(14-15).
Spirituality, as a personal dimension, permeates the individual's entire history, whereas religiosity refers to a means for manifesting spiritual aspects (related to treatment or otherwise). In this context, despite the fact that many people resort to spiritual resources to recover from addiction, being connected to a religion usually occurs at a later moment in time, due to success observed in other people, or in their own gradual recovery(3).
In the early 20th century, certain scientists were convinced that, with the development of modern science and rationality, religion would be doomed to disappear. What occurred, however, was value coming to be placed on subjective aspects of the individual, seeking responses to life's fundamental questions through a relationship with the transcendent, a phenomenon known as the "transmutation of religion into spirituality"(16).
Considering the need to better understand the topic of the various contexts in which nursing operates, the aim of this study was to identify use of alcohol and/or other drugs and evaluate the aspects of spirituality and religiosity in users in rehabilitation institutions and support groups
Method
This was a descriptive, exploratory study with a quantitative approach.
The sample was composed of 138 psycho-active substance users with links to rehabilitation institutions and support groups in four municipalities in the State of São Paulo, namely: a Treatment Community TC (evangelical, Catholic, of no religion), a Psycho-social Alcohol and Drugs Care Center (CAPS-ad) and an Alcoholics Anonymous (AA) group.
This study was derived from a Master's dissertation(17), from which the study on validating the Brazilian version of the Spirituality Self Rating Scale (SSRS-br)(18) also originated. Criteria for inclusion in the sample were: being aged 18 or over; being linked to a Treatment Community or support group (Alcoholics Anonymous - AA). Exclusion criteria were illiteracy or not being in a condition to be able to understand the research instruments.
The data were collected between August and October 2007. A self-applied instrument was used which was divided into two parts, containing socio-demographic information, questions related to drug use, the Test to Identify Alcohol Use version C (AUDIT-C) and the SSRS-br(18).
The AUDIT-C is a questionnaire containing three questions (number of doses, frequency of use and consumption of five or more doses on one single occasion). In order to read the risk levels of consumption, the responses needed to be summed, varying between zero and 12 points, with scoring differentiated by sex. For men, scores above five indicate harmful consumption and recommend intervention(19).
The SSRS is a scale composed of six (uni-directional) items that aims to measure to what extent the subject considers or judges spiritual issues to be important and applies them to his/her life. It has been validated with users of psycho-active substances and its psychometric properties are satisfactory, with Cronbach's Alpha coefficients of 0.83, varying between 0.70 and 0.88(18). The items of which the SSRS is composed include religious practices and theoretical precepts of 12-step-based programs. The responses are marked on a Likert-type scale and vary from "1 =I agree totally" to "5=I totally disagree". In order to calculate the scores, each item needs to be re-codified (ex.: 5 = 1; 4 = 2; 3 = 3; 2 = 4; 1 = 5), giving a total value. The higher the value identified, the greater the level of spiritual orientation.
The data were inputted into the Statistical Package for Social Sciences (SPSS), version 10. In order to evaluate the religious aspects in the group of alcohol and/or drug users, the Chi-square test and the Student's t-test were used to evaluate differences between the mean scores for age, age of first use, the SRSS-br and the AUDIT-C between the groups evaluated. The Kruskal-Wallis test was also used to evaluate the ranking of the mean scores for the SRSS and the AUDIT-C with the socio-demographic variables and religious aspects. The level of significance was 5%.
The study was approved by the Research Ethics Committee from the Ribeirão Preto School of Nursing, Universidade de São Paulo, Process no 0804. The research was explained to all of the participants and they signed an informed consent form.
Results
Socio-demographic information
The study sample was made up of 138 men with a mean age of 39 (standard deviation±13.60), varying between 18 and 69. Of the participants, 81 (58.7%) were linked to the TCs, 30 (21.7%) to the AA and 27 (19.6%) to the CAPS-ad; 87 (63%) lived alone, 64 (46.4%) had gone to high school (graduated or otherwise), 95 (68.8%) had formal employment, 65 (47.1%) had worked full time within the last year. All the users attending the locations researched during the period in which data were collected were included in the study.
Regarding the type of drug, 65 (47.1%) were alcohol users and 73 (52.9%) drug users. No one from the alcohol users group was identified as also using drugs, although there was a significant number from the other group who used cocaine, marijuana and alcohol. Differences were observed between the groups evaluated, with the drug user group standing out, with regards to the following variables: type pf drug for which they were seeking treatment, length of time in treatment and history of institutionalization. These differences were statistically significant. The results can be seen in Table 1.
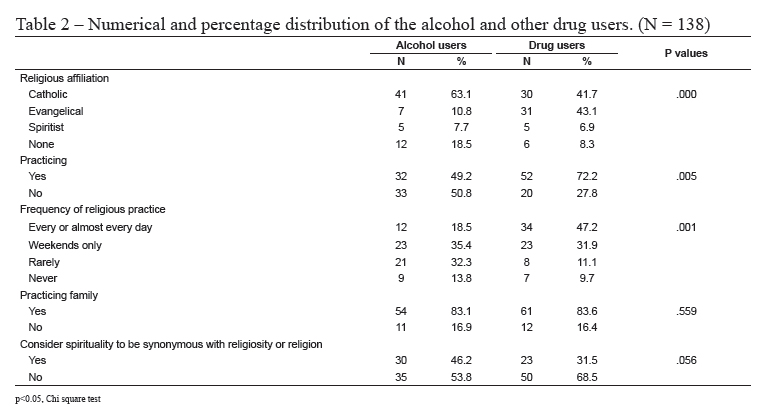
Regarding religious aspects, differences were found between the groups: in relation to alcohol users, 41 (63.1%) were affiliated to the Catholic religion, 33 (50.8%) did not practice any religion and 23 (35.4%) only attended at weekends. As for the drug users, 31 (43.1%) were evangelical, 52 (72.2%) were practicing, 34 (47.2%) attended religious sessions every, or almost every, day. Both groups belonged to families practicing families that practiced religion and did not consider religiosity to be synonymous with spirituality (Table 2).
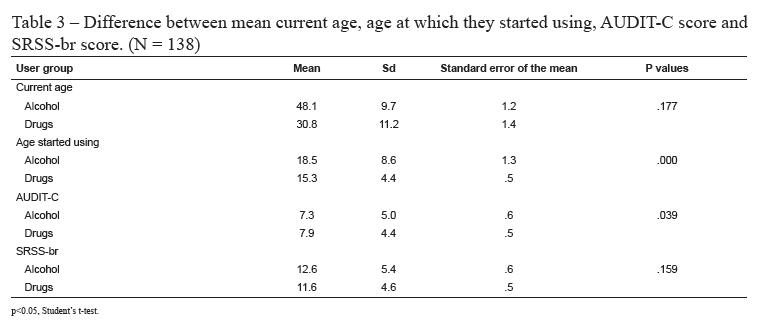
Table 3 shows that there was a statistically significant difference between the groups of alcohol and drug users concerning age at which they began to using and the AUDIT-C score. Although alcohol users had higher mean age and higher SRSS-br scores compared with drug users, the differences were not statistically significant.
The mean SRSS-br scores were higher in the drug user group treated at the CAPS-ad and among those with part-time work. However, the differences were not statistically significant.
When comparing the mean SRSS-br and AUDIT-C scores with the variables sex, age, marital status and type of drugs used, no significant differences were found. Now were there any statistically significant differences between age, SRSS scores and AUDIT-C scores.
No differences were found between the mean SRSS scores of users whose families practiced a religion and of those who stated that their family was not practicing, although the mean SRSS scores were higher in the group of users with practicing family members.
Regarding the level of severity of alcohol consumption, measured using the AUDIT-C, the highest scores were from those who did not worked and who made use of the CAPS-ad, with statistically significant differences.
Users who considered spirituality to be synonymous with religiosity had higher SSRS-br scores, although the difference between groups was not statistically significant.
Discussion
This study sought to improve understanding of alcohol and/or other drug use and religious/spiritual aspects in users in rehabilitation institutions and support groups.
The sample's socio-demographic characteristics were similar to those of other studies in the literature, with a predominance of male users, adults, with low levels of education(3,7-8,14,19).
Concerning psycho-active substance use, differences were found between the groups evaluated. Alcohol users did not use other types of drugs and were mostly linked with TCs (40%), whereas drug users were poly-users (60%) also linked to TCs (75.3%), and had been institutionalized (97.3%).
These data suggest that drug users are turning to integrated institutionalization services as a treatment resource which distanced them from social life and, thus, from environments that encouraged substance use. In effect, TC use has expanded in recent decades. It is a treatment model with characteristics differing from those of traditional methods, using the environment and the users themselves to promote the learning and changes needed to break the cycle of addiction; use, abstinence and relapse(8,20).
When evaluating religious aspects (affiliation, practice, frequency) among users, it was observed that those who used alcohol were affiliated with Catholicism, were not practicing and frequented their religion less intensely when compared with the group of drug users. Religion provides many users with social support, as well as an effective cognitive clinical scheme that contributes to reducing stress and increasing subjective wellbeing(2,4) in those dependent on alcohol and/or other drugs in the rehabilitation process(3,6).
Studies indicate that encouragement to exercise the spiritual dimension can potentially facilitate the process of rehabilitation from drug and/or alcohol dependence, although the mechanisms of this action are little known. This may be linked to adopting a new lifestyle in which bonds, day-to-day practices and even adherence to a specific religion are encouraged in order for the individuals to avoid situations that encourage psycho-active substance use(15,17).
The findings of the study show that spirituality does not depend on the religious aspects in the individual's life, whether concerning practice and attending religious ceremonies within the personal or family ambit, or in relation to religious doctrine at school, corroborating the findings in the literature(4,6-7).
These results have implications for integrated care practices. the nurse should be aware of the religious and spiritual dimension, respecting the service users' values and beliefs, understanding that spirituality is an integral part of human needs and an essential dimension of the recovery process(1,9-10).
The fact that religiosity was not seen as synonymous with spirituality was not significant in the sample investigated, in contrast to what is indicated in the literature(6-7), which is encouraging as it suggests that the spiritual dimension can be worked on in any treatment environment.
The spirituality identified among psycho-active substance users, according to the means identified in this study, appear to be related to the search for a more stable and balanced life, perhaps because of the recognition that this personal feeling may stimulate a positive outcome to the problem they face, facilitating abstinence, improving interpersonal relationships and helping to tolerate disruptive feelings, such as anxiety. A study of other health problems, not involving drug addiction, indicates that a significant number of patients view their spiritual needs as important and would like to receive some care directed at this dimension(15). Within the ambit of drug addiction, spirituality may be related to reduced use and, in the case of treatment, it has been an important treatment tool in reducing episodes of cravings, improving health and quality of life(7).
Among this study's limitations, we can mention difficulties in measuring religiosity, due to the polysemy of the concept, especially when evaluated using variables such as affiliation (for example, Catholic or Evangelical), religious practice (practicing/not practicing) or frequency of attending services (weekly, monthly). These evaluation strategies are considered limited as they restrict the study of something as complex as religiosity in a patient's life to one single variable.
Another difficulty concerns differentiating between the concepts of religiosity and spirituality, as people tend to attribute different meanings to these constructs. This poses a challenge for the nursing professional who, in their care practice, needs to be aware of this semantic multiplicity. Historically, aspects of religiosity and spirituality have been present in the discourse, teaching and assumptions of exercising nursing care(1,12). In spite of this, professionals in the area do not always have the skills to deal with such dimensions, partly because of the need to better understand the complexity of the concepts and because of issues concerning the way this care is programmed in clinical practices(1-10).
In the instrument used to measure spirituality, there are subjective differences in understanding what it is and how it can be exercised. Finally, the type of sample used is only representative of the places investigated, and cannot be extrapolated and generalized for other contexts.
Conclusion
This study shows that there is a complex relationship between religious and spiritual aspects in psycho-active substance users. There was statistically significant difference in the religious aspects between the alcohol and the drug using groups; however, spirituality and the concepts of religiosity and spirituality used did not differ between the groups. These results have important implications for treatment and psycho-social rehabilitation, as religion and spirituality can function as elements in the positive outcome among protecting factors for drug use. Thus, the findings offer support for holistic care to become more effective in daily nursing practice, broadening understanding of how this professional can implement care that takes into consideration subjective aspects of psycho-active substance users.
Referências
1. Draper P. An integrative review of spiritual assessment: implications for nursing management. J Nurs Manag. 2012 Dec;20(8):970-80. [ Links ]
2. Mohr K. Spiritual issue in psychiatric care. Perspect Psychiatr C. 2006 Aug;42(3):174-83. [ Links ]
3. Sanchez ZM, Nappo SA. A religiosidade, a espiritualidade e o consumo de drogas. Rev Psiquiatr Clín. 2007;34(supl 1):73-81. [ Links ]
4. Cook CCH. Addiction and spirituality. Addiction. 2004;99(3):539-51. [ Links ]
5. Guimarães HP, Avezum A. O impacto da espiritualidade na saúde física Rev Psiquiatr Clín. 2007;34(supl 1):88-94. [ Links ]
6. Clarke JA. Discussion paper about "meaning" in the nursing literature on spirituality: an interpretation of meaning as "ultimate concern" using the work of Paul Tillich. Int J Nurs Stud. 2006;43(7):915-21. [ Links ]
7. Moreira-Almeida A, Koening HG. Retaining the meaning of the words religiousness and spirituality: a commentary on the WHOQOL SRPB group's "a cross-cultural study of spirituality, religion, and personal beliefs as components of quality of life". Soc Sci Med. 2006;63(4):843-5. [ Links ]
8. Galanter M, Dermatis H, Bunt G, Willians C, Trujillo M, Steinke P. Assessment of spirituality and its relevance to addiction treatment. J Subst Abuse Treat. 2007;3(33):257-64. [ Links ]
9. Monod S, Brennan M, Rochat E, Martin E, Rochat S, Bula CJ. Instruments measuring spirituality in clinical research: a systematic review. J Gen Intern Med. 2011;26(11):1345-57. [ Links ]
10. Chung LYF, Wong FK, Chan MF. Relationship of nurses´ spirituality to their understanding and practice of spiritual care. J Adv Nurs. 2006 April;58(2):158-70. [ Links ]
11. Narayanasamy A. Nurses´awareness and educational preparation in meeting their patients' spiritual needs. Nurse Educ Today. 1993 Jun;13(3):196-201. [ Links ]
12. Greenstreet WM. Teaching spirituality in nursing: a literature review. Nurse Educ Today. 1999;19(8):649-58. [ Links ]
13. Poage ED, Ketzenberger KE, Olson J. Spirituality, contentment, and stress in recovering alcoholics. Addict Behav. 2004;29(9):1857-62. [ Links ]
14. Lillis J, Gifford E, Humphreys K, Moos R. Assessing Spirituality/Religiosity in the Treatment Environment: The Treatment Spirituality/Religiosity Scale. J Subst Abuse Treat. 2008;35(4):427-33. [ Links ]
15. Arnold RM, Avants K, Margolin A, Marcotte D. Patient attitudes concerning the inclusion of spirituality into addiction treatment. J Subst Abuse. 2002;23:319-26. [ Links ]
16. Siqueira D. O labirinto religioso ocidental: da religião à espiritualidade, do institucional ao não convencional. Soc e Estado. 2008;23(2):425-62. [ Links ]
17. Gonçalves AMS. Estudo dos níveis motivacionais em relação ao uso de substâncias psicoativas e a espiritualidade. [dissertação]. Ribeirão Preto: Escola de Enfermagem de Ribeirão Preto da Universidade de São Paulo; 2008. [ Links ]
18. Gonçalves AMS, Pillon SC. Adaptação transcultural e avaliação da consistência interna da versão em português da Spirituality Self Rating Scale (SSRS). Rev Psiquiatr Clín. 2009;36(1):10-5. [ Links ]
19. Meneses-Gaya C, Zuardi AW, Loureiro SR, Hallak JE, Trzesniak C, de Azevedo Marques JM, et al. Is the full version of the AUDIT really necessary? Study of the validity and internal construct of its abbreviated versions. Alcohol Clin Exp Res. 2010 Aug;34(8):1417-24. [ Links ]
20.
Fracasso L. Comunidades Terapêuticas. In: Diehl A, Cordeiro DC, Laranjeira R,
organizadores. Dependência química. Porto Alegre: Artmed; 2011. p. 61-9. [ Links ]
Received: Oct. 17th 2012![]() Correspondence
Correspondence
Angelica Martins de Souza Gonçalves
Universidade Federal de São Carlos
Centro de Ciências Biológicas e da Saúde
Departamento de Enfermagem
Rodovia Washington Luís, Km 235
Caixa Postal 676
CEP: 13.565-905, São Carlos, SP, Brasil
E-mail: angelicamartins@ufscar.br
Accepted: Dec. 19th 2013

{kind=link}
{kind=link}
{kind=link}