










Servicios Personalizados
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versión On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.10 no.2 Ribeirão Preto ago. 2014
http://dx.doi.org/10.11606/issn.1806-6976.v10i2p85-92
ORIGINAL ARTICLE
DOI: 10.11606/issn.1806-6976.v10i2p85-92
Conception of health professionals who work in emergency mental health
Marcos Hirata SoaresI; Eloisi Delalibera RuzzonII; Maira Sayuri Sakay BortolettoIII
IDoctoral Student, Escola de Enfermagem de Ribeirão Preto,
Universidade de São Paulo, WHO Collaborating Centre for Nursing Research
Development, Ribeirão Preto, SP, Brazil
IIStudent, Programa de Residência Multiprofissional em Saúde da
Mulher, Universidade Estadual de Londrina, Londrina, PR, Brazil
IIIRN, Departamento
de Saúde Coletiva, Universidade Estadual de Londrina, Londrina, PR, Brazil
ABSTRACT
This study compared the conceptions about mental illness of administrative professionals, nurses and doctors of emergency health services in the city of Londrina, PR. The design was cross-sectional, using the Opinions about Mental Illness (OMI) scale with a random sample of 30% of the professionals, totaling 96 subjects in the period 2010 to 2011. The data was statistically analyzed by the Statistical Package for Social Sciences (SPSS); with two factors of the OMI scale and nurses, there was normality in the sampling distribution. The Kruskall-Wallis test indicated a significant variation with respect to four of the seven factor components of the OMI (p <0.05). The professionals that work in emergency health services require training in the area of mental health, and there is a need for further studies on this topic, with a larger number of subjects.
Descriptors: Mental Disorders; Emergency Medical Services; Psychiatric Nursing; Emergency Services, Psychiatric.
Introduction
Psychiatric reform in Brazil has historically been a political, social and economic movement that has contributed to the provision of assistance to people with mental health disorders not only in psychiatric hospitals, but also in Psychosocial Care Centers (PCC) and other network services in mental health care. For example, Family Health Units (FHU) and emergency services, assist in providing more citizenship for these individuals and contribute to the demystification of the patient and mental illness (1).
During psychiatric care in emergency situations the exclusive focus often lies on the biological aspects of care, such as administering medication and hygiene(2), many times preserving life without considering the mental health aspects, not featuring the integral care of mental health.
A study in São Paulo found that 70% of patients with a first episode of psychosis were admitted to the health care system through the emergency department, and 50% of cases were made within four weeks of the onset of symptoms(3).
It is common for studies on this topic to exclude many professionals such as administrative support. In this study, there was the initiative to include other professionals beyond nursing, precisely because of their direct or indirect contact with these clients; this also demanded the need for training to achieve better coping with this population because one of the major challenges in Psychiatric Reform is rescuing the citizenship of mental patients and reducing the stigma and prejudice against mental illness(4-5).
Among the many health professionals who work in mental health, the nurse and his/her team have the most contact with the patient. However, nurses often present an Authoritarian role with the patient, observe and overpower at the same time, in which the best course of action is to apply therapeutic attitudes toward psychological distress in the client; for example, welcoming and empathy, as well as having good knowledge of psychopharmacology, psychopathology, underpinned by the principles of Psychiatric Reform and Psychosocial Rehabilitation.
In the literature, there is a reference to the study "Attitudes toward mental illness: a comparative study between freshmen and graduate nursing", that found there are changes in the behavior of the students with a higher level of education in relation to the mental health patient(6). Also the study "Attitudes of entrepreneurs in Southern Brazil in relation to people with mental health diseases," found that administrators have a protectionist view, damaging and dangerousness, possibly due to misinformation and prejudice(7).
A study(8) made in Greece with 239 medical students and 361 various employees found that professionals in the psychiatric wing had more positive attitudes in relation to patients with mental illness. The authors concluded that contact with mentally ill patients and training are important in reducing the stigma among the mental health staff and other sectors. However, no studies in Brazil were found to involve professionals such as doctors and administrative assistants, within emergency services.
In order to assess the view of mental illness in professionals of urgent and emergency care services we used the OMI (Opinions about Mental Illness) scale, validated in Brazil(9), to evaluate the conception of mental illness in administrative professionals, nurses and doctors working in Londrina, PR; since there is no information on this topic, this is the pioneering study on this subject. Thus, the hypothesis for this study is that there are differences in the conception of the mentally ill, but what is not yet certain is the description of how or what these differences are and the other variables that are associated with this process. It is important to describe these concepts to ensure high quality care is provided to patients, because by identifying the conceptions of mental illness using the subjects of this study more professional groups can become qualified in mental health care.
Objective
Compare the conception of mental illness between administrative professionals, nurses and doctors in urgent and emergency health care services in the city of Londrina, PR.
Methodology
This is a cross-sectional individuated study, with analysis of 96 professionals from various emergency care services and Londrina emergency medical services including: Regional University Hospital of Northern Paraná, Emergency Medical Services (EMS), the Psychosocial Care Center (PCC) and two secondary state hospitals.
Subjects and Location
The data was collected at an appropriate time where there was no hindrance during working hours and at the best time for the subjects who agreed to participate. The survey sample was 30% of those working in emergency and urgent care services, represented by nurses, technicians and nursing assistants1, doctors, and administrative staff; obtaining a total of 96 (90.5% of the total sample) participants interviewed of both genders.
The inclusion criteria for a subject in this research study was done by simple random sampling, including only professional emergency service participants, i.e. the emergency rooms of various locations; based on 30% of the professional staff of each service and category, and given first choice by various shifts, followed by a raffle that allowed consideration of the respondents for participation.
If the professional refused, a new raffle was performed. If for some reason the subject did not answer the OMI scale, she was again invited to participate, up to a maximum of three times. So, if by any chance the professional does not accept, another individual was again randomly selected.
Due to the dynamics of urgent care and emergency services, it was impossible for eight nursing technicians and two doctors to participate in the research, causing others to be drawn in their place; data collection was conducted in November and December 2010 and from January until April 2011.
Data collection instrument
A self-administered questionnaire composed of two parts was used as an instrument in this study. The first part included information such as: age, sex, occupation, work experience, and education, and the second part consisted of a range of attitudes - "Opinions about Mental Illness." This scale is represented in Brazil by the initials ODM (Opiniões sobre a Doença Mental), so named when translated and validated for the Portuguese language(10-11).
In this Latin version, the scale consists of seven factors for analysis and 51 questions, each with six alternatives, they are a Likert type scale following the progressive sequence of six points of agreement, from "strongly agree" to "strongly disagree." The higher the score, the greater the person's belief of the idea contained in each facto; the lower the score, the lower the belief. The scale has seven factors described below:
- Authoritarianism. Reflects the view that the mental health patient needs to be isolated from other patients, remaining under locked doors and surveillance. Includes the concept of personal and social impairment of the patient and the idea that they are dangerous. There are nine statements included in this factor.
- Benevolence. Reflects the view that due to their unhappiness the mentally ill must be supported by good and paternalistic protectionism, based on care, personal attention and comfort material. There are five statements included in this factor.
- Mental Hygiene Ideology. Is the idea that the mental patient is a person similar to normal people, with quantitative differences, but not qualitative. They can perform specialized activities and take care of children. There are eleven statements included in this factor.
- Social restriction. Interpret mental illness as a kind of hereditary defect, completely different from other diseases, whose holder can contaminate the family and society, and must therefore be protected by restriction of personal and social rights of the patient, even after hospitalization. There are seven statements included in this factor.
- Interpersonal Etiology. Explains mental illness as originating in interpersonal experiences, with emphasis on the interaction with parental figures. There are six statements included in this factor.
- Mental Effort Etiology. Reflects the idea that mental illness comes from "excessive cerebral effort" by the exaggerated intellectual work, by thinking too much or having negative thoughts. There are eight statements included in this factor.
- Minority view. Interprets the concept of mentally ill to be very different from health subjects, can be easily recognized in a human group, mainly because of its external appearance. There are five statements included in this factor.
Data analysis
The raw factorial scores obtained with the implementation of the OMI were processed by the Sten system (11-12), which provides a standard comparison among the factors varying from 1 to 10, an average of 5.5 and a standard deviation equal to 0.5. A database was created that was analyzed by SPSS- v. 15. The initial step was to conduct a normality test, choosing between parametric tests, if the distribution was normal and non-parametric, then it was not normal. The level of significance was set at α = 0.05.
Procedure
Initially, contact was made with the institutions involved in the study for the proper authorization, with the presentation of the survey submitted to the Committee on Ethics in Research Involving Human Beings from the State University of Londrina SUL/ Regional University Hospital of Northern Paraná RUHNP (CAAE no. 3060.0.000.268 -09). The City of Londrina Authority of Health was also contacted for the collection of data of the medical emergency public services of Londrina. Thus, 30% of each class was randomly selected, being nurses, technicians, medical and administrative staff. All participants signed the informed consent for research subjects.
Results
The first step in the statistical analysis was to perform the Kolmogorov-Smirnov and Shapiro-Wilk normality test. These tests indicated that only the Mental Hygiene Ideology and Minority View factors have a normal distribution (p> 0.05) and only for the nursing profession. The other factors and professions all have non-normal distribution (p <0.05). Therefore, we chose to characterize the sample as non-normal distribution and used the non-parametric Kruskall-Wallis test to compare if there are statistically significant differences between the medians of the four professions.
The research involved 96 professionals, 17 nurses (14.2 %), 57 nursing technicians (47.5 %), 14 doctors (11.7 %), and 8 administrative assistants (6.7 %). In terms of gender, 54.1% were female and 45.9% male. The ages ranged from 20 to 66 years, getting an average of 24 years old. The professionals in greater number were nursing technicians with 57 interviewees, corresponding to 47.5%, followed by nurses with 17 subjects representing 14.2% of the respondents, 14 doctors and 8 administrative assistants, corresponding to 11.7% and 6.7 %, respectively. This was to be expected, since the majority of the professional health care team is represented by the nursing staff.
As for education, the highest percentage was vocational school (22.5%), followed by college (20%), post-graduate/residency (19.2%) and college incomplete (16.7%). As for the location of the study, 29 workers were interviewed (24.2%) at the University Hospital due to the greater number of existing employees in this environment, followed by the State Hospital with 22 (18.3%) participants, 19 (15, 8%) in EMS and 6 (5.0%) in Psychosocial Care Center (PCC). As for professional experience, there were 54 (45%) workers with 1 to 10 years of experience, 29 (24.2%) with 11 to 20 years, and 13 (10.80%) with over 20 years of experience.
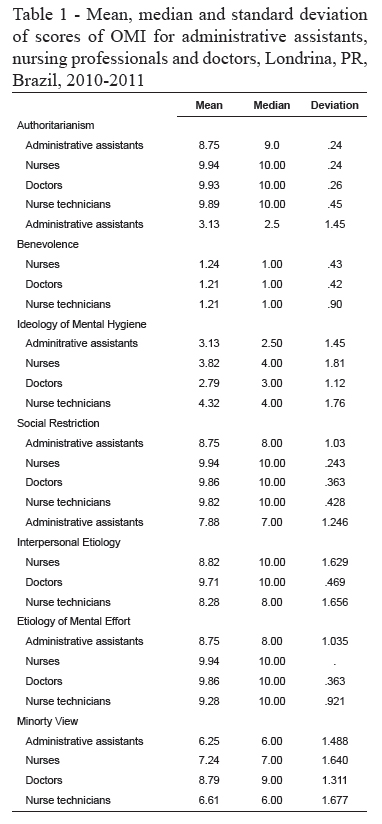
The means, medians, and standard deviations for the factor scores on the OMI scale are presented in Table 1.
Discussion
Within the factor Authoritarianism, the median 10.0 in relation to the Sten score and the data in Table 1 indicate that the vast majority of the population interviewed presents strong tendencies to be authoritarian, stating that the patient with mental disorder should be isolated from other people, because there is no recoverability. The score of 1.24 in the Benevolence factor, median 1.00, corroborates an authoritarian approach, because the less benevolent an individual tentds to be, the greater their tendency toward authoritarianism. When comparing the scores of the present study to a study with nurses in psychiatric services, it is noted that the nurses in this study are more authoritarian and less benevolent than nurses in psychiatric services(5).
It is observed in Table 1 that the factors Benevolence and Mental Hygiene Ideology were the factors with scores below average as described in this validation study(9) and the other factors were, in general, well above the expected average. This characteristic describes the conception of mental illness of emergency service professionals as extremely authoritarian, less benevolent and unaware of the factors that trigger a mental disorder. In reguards to the factors that are above the expected average, it is possible to characterize the conception of professionals who work in emergency services as prejudiced, at the same time this indicates that there is little scientific knowledge about mental disorders.
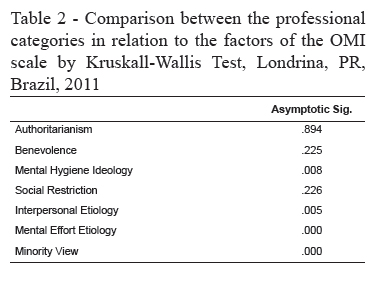
In Table 2, the Kruskall-Wallis test showed no statistical significance between the administrative assistant, nurse, nurse technician and doctor in relation to these factors of the OMI scale, Authoritarianism, Benevolence and Social Restriction (p=0.894, p=0.225 and p=0.226 respectively); the null hypothesis for the test is accepted, with respect to these factors, but not ruling out such an association in a larger sample study. For the other factors, there are statistically significant differences (p< 0.05).
In the Mental Hygiene Ideology factor for nurses, the median of 4.00 remains slightly below the quantile 50 in relation to the Sten score, signifying a below average belief that the mentally ill are similar to people called normal, however, this belief is different from one found in another study of nurses in two hospitals that had Sten scores of 6 and 7(5).
The Kruskall-Wallis test, in Table 2, showed that there were no statistically significant differences between the four professions examined in relation to the Mental Hygiene Ideology (p= 0.008), Interpersonal Etiology (p= 0.005), Mental Effort Etiology (p= 0.000) and Minority View (p= 0.000); in other words, the four professions have differing points of view on the mentally ill in these factors, confirming the hypothesis of this study.
Within the Social Restriction factor, the responses indicated a total belief that these patients exhibit hereditary disorders, and should stay in conviviality of their family (median= 10). However, the scores were lower than those found in studies of three hospitals that were analyzed, which ranged from 3.5 to 5.5 with a sample only of nurses(5). This is a dangerous notion more rooted in these nurses than in nurses in psychiatric services(5).
According to Table 1, for health professions, in the Social Restriction factor, we obtained a median of 10.00 for nurse technicians, nurses and doctors, getting a Sten score of 9.82, 9.94 and 9.86. However, according to Table 2, the Kruskall-Wallis test showed no statistically significant differences between the four professions (p= 0,226).
In relation to Interpersonal Etiology, the subjects believed strongly that mental disorders are related to interpersonal aspects linked to degrees of relationships (median= 9.0). All things considered, another study(5) showed Sten scores of less than average or equal to 4.6 in which nurses in four institutions that were analyzed believed that the disorders of these patients are originating in interpersonal experiences.
Concerning Mental Effort Etiology, there is an indication that all professionals believe that this disease is from exacerbated mental effort (median= 10). Finding a discrepancy(5), in the presentation of another study, it did not identify the belief that clients have developed mental disorders by excessive mental effort.
The Kruskall-Wallis test, Table 2, showed a statistically significant difference between the four professions in relation to the Mental Hygiene Ideology (p= 0.008), Interpersonal Etiology (p= 0.005), Mental Effort Etiology (p= 0.000) and Minority View (p= 0.000) factors; that is to say, the four professions have differing points of view on the mentally ill, influenced, probably by their professions and academic backgrounds.
With respect to the Minority View, it is thought that patients are different due to their appearance, differentiating them from the so-called normal (median= 7), refuting this argument(5), the nurses in this study exhibited low scores in relation to this factor, less than or equal to 3.7. The Kruskall-Wallis test in Table 2, showed there was no statistically significant difference between the four professions (p= 0.000), that is, the four professions have differing points of view on the mentally ill.
Final Considerations
With the exception of the factors Benevolence and Mental Hygiene Ideology, the other factors showed high scores, well above the average value identified in the validation study of the OMI scale. For nurses, it is concluded that they have a more stereotyped belief in relation to mental illness and the disease than nurses in mental health services.
When thinking about the professional categories studied, the differences found in the four factors of the OMI were important to describe the type of differences in the conception of mental illness; since, until this moment, these differences were assumed but there was no knowledge of their magnitude. In this aspect, this is a pioneer study that provides important contributions to this subject.
The normality test demonstrated that the nurse has a normal distribution in its sample for the Mental Hygiene Ideology and Minority View factors, i.e., the conception of mental illness for nurses, within these two factors, tend to present the same pattern in larger samples with these characteristics.
The sample size was considered a limitation in this study and may lead to a possible type I error, one condition is the financial possibilities of implementing the research, as well as the lack of research involving the other professional categories studied, limiting the analysis of data. Therefore, it emphasizes the importance of further studies, in addition to investing in continuing education for all professional categories involved, especially the nurses, since the scale used suggests an undesirable attitude, permeated with prejudice and stigma in the face of mental illness.
References
1. Gonçalves AM, Sena RR. Psychiatric reform in Brazil: contextualization and consequences regarding the care for the mentally ill in their family environment. Rev. Latino-Am. Enfermagem. 2001;9:48-55. [ Links ]
2. Scherer ZAP, Scherer EA, Labate RC. Psychiatric nursing consultation and liaison: how do nurses understand this activity? Rev. Latino-Am. Enfermagem. 2002;10:7-14. [ Links ]
3. Del-Ben CM, Rufino AC, Azevedo-Marques JM, Menezes PR. Differential diagnosis of first episode psychosis: importance of optimal approach in psychiatric emergencies. Rev Bras Psiquiatr. [Internet]. 2010;32(Suppl 2)S78-86. [acesso 2 nov 2011]. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1516-44462010000600004&lng=en. http://dx.doi.org/10.1590/S1516-44462010000600004. [ Links ]
4. Souza AMA, Braga VAB. Brazilian psychiatric reform: a lot to reflect on. Acta Paul. Enferm. [Internet]. 2006 [acesso 2 nov 2011]. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-21002006000200013&lng=en. http://dx.doi.org/10.1590/S0103-21002006000200013. [ Links ]
5. Tavares RR, Pedrão LJ. Comparative analysis of nurses' views from different psychiatric units on an individual in psychic suffering] Cogitare Enferm. 2003;8:75-86. [ Links ]
6. Pedrão LJ, Avanci RC, Malaguti SE, Aguilera AMS. Atitudes frente à doença mental: estudo comparativo entre ingressantes e formandos em enfermagem. Medicina. (Ribeirão Preto). 2003;36(1):37-44. [ Links ]
7. Delevati DM, Palazzo LS. Businessmen attitudes regarding mental disordered individuals in the south of Brazil. J Bras Psiquiatria. 2008;57:240-6. [ Links ]
8. Arvaniti A, Samakouri M, Kalamara E, Bochtsou V, Bikos C, Livaditis M. Health service staff's attitudes towards patients with mental illness. Soc Psychiatry Psychiatr Epidemiol. 2009;44(8):658-65. [ Links ]
9. Rodrigues CRC. Atitudes frente à doença mental: estudo transversal de uma amostra de profissionais da saúde. [Tese de doutorado]. Ribeirão Preto: Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo; 1983. [ Links ]
10. Cohen J, Struening EL. Opinions about mental illness in the personnel of two large mental hospitals. J Abnorm Socy Psychol. 1962;64:349-60. [ Links ]
11. Canfield AA. The sten scale: a modified C. scale. Educ Psychol Measure. 1951;11:295-7. [ Links ]
12. Struening EL,
Cohen J. Fatorial invariance and other psychometric characteristics of five
opinions about mental illness fators. Educ Psychol Measure. 1963;23:289-98. [ Links ]
Received: Mar. 18th 2012 1 In Brazil, the technical nurse is
a professional who has a secondary level of education and performs technical procedures
under the supervision of nurses.![]() Correspondence
Correspondence
Marcos Hirata Soares
Universidade Estadual de Londrina, Centro de Ciências da Saúde.
Departamento de Enfermagem
Av. Robert Koch, nº 60
Bairro: Vila Operária
CEP: 86.038-350 Londrina, PR, Brasil
E-mail: mhirata@uel.br
Accepted: Dec. 19th 2013
