










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versão On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.10 no.3 Ribeirão Preto dez. 2014
http://dx.doi.org/10.11606/issn.1806-6976.v10i3p159-166
ORIGINAL ARTICLE
DOI: 10.11606/issn.1806-6976.v10i3p159-166
The social network of individuals after attempted suicide: the eco-map as a resource
La red social de individuos pos-tentativa de suicidio: o eco-mapa como recurso
Fernanda Pâmela Machado1; Marcos Hirata Soares2; Juliana Stuqui Mastine1
IUndergraduate student in Nursing, Universidade Estadual de Londrina, Londrina, PR, Brazil
IIDoctoral student, Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, WHO Collaborating Centre for Nursing Research Development, Ribeirão Preto, SP, Brazil. Professor, Universidade Estadual de Londrina, Londrina, PR, Brazil
ABSTRACT
The purpose of this study is to characterize, by means of the eco-map, a social support network of people who have attempted suicide. A qualitative study was conducted; the participant observation method was used between 2011 and 2012, in Londrina, Parana, Brazil, with patients who attempted suicide by toxins. During this period, 6 subjects who attempted suicide were interviewed. Two tables and an eco-map for each subject were created to present the data. Two categories were also created from the data: life history and daily social support of the subjects. It was observed that in patients who have attempted suicide to solve their problems, the eco-map was a useful resource to characterize their social support network, which was weakened, allowing prevention strategies for new attempts.
Descriptors: Social Support; Suicide; Mental Health; Suicide, Attempt.
RESUMEN
El objetivo fue caracterizar, por medio del eco-mapa, la red de apoyo social de personas que intentaron suicidarse. Se realizó un estudio cualitativo, del tipo observación participante entre 2011 y 2012, en Londrina, Paraná, Brasil, con pacientes que intentaron suicidarse mediante productos químicos. En ese período, fueron entrevistados 6 sujetos que intentaron suicidarse. Para presentar los datos, se crearon dos cuadros y un eco-mapa para cada sujeto. A partir de los datos, se crearon dos categorías: historial de vida y apoyo social en lo cotidiano de los sujetos. Se observó que los pacientes intentaron suicidarse para solucionar sus problemas y el eco-mapa se presentó como un recurso útil para identificar su red de apoyo social (la cual se presentaba frágil), posibilitando estrategias de prevención de nuevas tentativas.
Descriptores: Apoyo Social; Suicidio; Salud Mental; Intento de Suicidio.
Introduction
Suicide is a phenomenon found in many countries, developed and developing, being the fourth leading cause of death among the population of 15 to 44 years old. The World Health Organization(¹) reports that suicidal behavior has been increasingly identified as a public health problem; in 2003, there were around 900 thousand cases in the world and for the past 45 years. The mortality rate of people who attempted suicide varied from younger to older (15 to 45 years).
Suicidal behavior, understood as a continuum, ranging from the initial thought to the fait acompli, has complex causes, which are interrelated. Certain psychiatric disorders, such as depression, schizophrenia and alcohol dependence play an important role, but physical diseases, particularly the painful and debilitating are factors as well. Poverty, loss of loved ones, disagreements with family or friends, broken relationships are, admittedly, risk factors that affect those who are predisposed, or especially vulnerable to suicide(²).
There are several factors that can lead human beings to commit suicide, for example: hopelessness, previous attempts, people with chronic pain, educational difficulties, inability to sort out daily problems, stressful or traumatic events, in addition to individuals dissatisfied with life, as well as, pessimistic individuals. Other studies have suggested that there is, however, a relationship between social support and suicide(³). In a case-control study, the relationship between social support networks and suicide was examined, and it was concluded that the social support network can be both a risk factor and protection for suicidal behavior. In a second study, also case-control, social support was linked to stressful life events, depression, and suicide attempts; it was shown that there is a need to implement public policies for social support, directed at employment and education, as well as treatment and intervention in mental disorders(4).
The social support for mental health is understood as assistance available to individuals and groups, in which this community can receive a kind of "shock absorber" against adverse events and stressful life situations, thus, obtaining positive resources to improve their quality of life. The configuration of the social network includes: the frequency a person visits religious groups, clubs, places of leisure, family, friends, spouses, neighbors, service workers, along with interactions in the workplace and in society in general(5).
The social support network seems to have a broad impact on physical and mental health, as it influences the way in which a person perceives stressful situations. Social support along with self-esteem, and a sense of control and dominion over one's own life make up the social resources and individual coping strategies that people use as a response to stressful situations; these aspects are considered protective factors and health promoters, helping them cope with specific situations such as acute or chronic illnesses, stress, crisis development and social or physical vulnerability(6).
Therefore, social support is an adjunct part to the theory of adaptation to stress, the characteristics of stressors, coping strategies and the subjective evaluation of the situation(7). In this sense, this study is important for the characterization of the social network of people who attempted suicide because it may be able to identify key points for prevention of new suicide attempts.
Objective
Characterization of the social support network of people who attempted suicide.
Methodology
It is a qualitative study, participant observation type, carried out between October 2011 and February 2012, in the city of Londrina, PR, which has 506,701 inhabitants, in an area of 1.653km² and Human Development Index (HDI) of 0.824.
The subjects were recruited from case notification to the researchers, from the Toxicological Information Center (TIC), linked to the University Hospital of the Northern Region of Parana (UHNRP), which admits all types of poisoning by toxins and medicines, where several cases can be considered suicide attempts.
Indirect interviewing was the technique used for data collection with the patients with suicide attempts at (UHNRP). The indirect interview is based on the principles of Interpersonal Relationship Therapy, used in Psychiatric Nursing, to improve the communication process and, at the same time, allow the expression of feelings by the patient, in order to also make the therapeutic period of the patient the subject of study.
There were 14 patients referred by TIC, however, only 6 managed to be located while they were hospitalized due to the rapid hospital discharge process. The inclusion criteria for this study were: a suicide attempt by toxins, living in the city of Londrina, and willingness to report their history to interviewers. There was no refusal to participate in the study. The research was approved by the Research Ethics Committee (C. A. A. E. 0289.0.268.000 -11).
The subjects were always met in pairs: while one interviewer interacted with the patient, the other documented the information reported. We used this feature, instead of recording the interview, because of the fact that we believe it improves the interaction between the interviewer and the subject, considering the delicacy of the issue addressed in this study.
Results
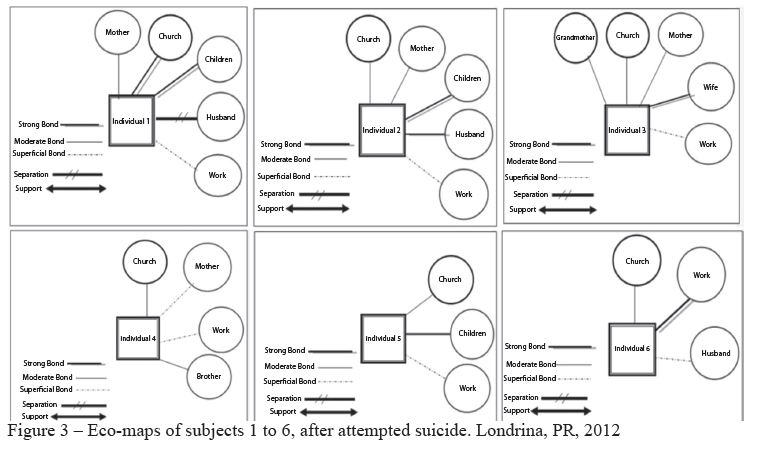
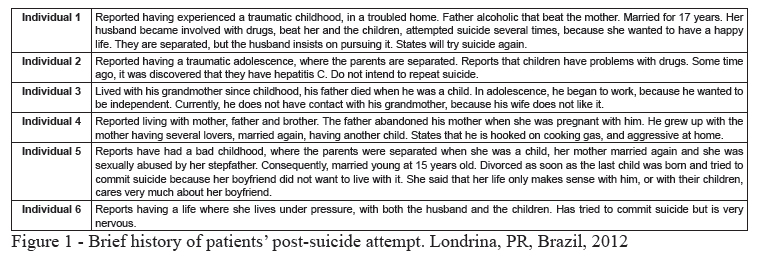
There were two figures for subject categorization constructed and a figure representing all the eco-maps of the subjects in the study, to represent the social network of people post-suicide attempt. The purpose of the eco-map is to represent the relationships of individuals and families with the other systems, setting up a strategy for greater visual impact and a quick view of information.
The eco-maps (Figure 3) and figures 1 and 2 represent the synthesis of the data obtained in the interviews. The subjects were four female and two male. The ages ranged from 18 to 46 years. The level of instruction was consistent with an incomplete secondary education and, as for occupation; the participants included a sales clerk, a production assistant, a student, a housewife and two that reported not having jobs.
Discussion
Life history
Looking at the cases studied it was found that, with the exception of subject 2, the others showed traumatic events in their childhood in their family history(8). All people go through a cycle of life, where they are born, grow, mature, grow old and die. However, many may or may not face something as serious as violence in their childhood and adult life. Teens who commit suicide have in their background, a higher proportion of fights, problems with the police, with the law, in school, at work, with teenage pregnancy and abortions. Therefore, as they get older, they cannot help but recall those moments of frustration, suffering and separation. Unable to bear the burden of distressing feelings, they opt for suicide; thinking this is the solution to their problems in their relationships and interactions with family and society (9). Along with social support, the eco-map, helps assess family relationships with the social environment for rehabilitation.
As in the cases studied, Figure 3 eco-maps showed that individuals 1 through 6 did not have links to other people except for those living with them. This is believed to be one of the factors that caused their suicidal behavior (10).
When examining Figure 1-3, individuals 1-5 are seen to have psychosocial problems that accompanied them since childhood. The first individual reported to have had a troubled childhood, as well as the other individuals. Individuals 2 and 5 also experienced times of suffering, in the presence of a dysfunctional family, without social support and especially without familial support. The presence of childhood trauma is common in the life history of many patients with psychiatric disorders. The magnitude of the problem is variable, with some studies pointing to the occurrence of childhood trauma in approximately 50% of adults with psychopathology(11).
In Figure 1, individual 6 reports living under pressure with her husband and children and individual 4 reported that his father abandoned his mother when he was a child and he grew up watching his mother having several boyfriends. In childhood, it is common for children, that when faced with marital conflicts and other adverse events, do not feel able and/or self-confident to face the problems of which they witness or live. This dynamic tends to continue through adulthood, there is no quick fix without proper treatment. Individuals who have been through traumatic situations have extremely negative emotions and dysfunctional thoughts, but psychotherapy can provide excellent resources for overcoming traumas(12).
Thus, from these case studies, it was observed that the use of eco-map can benefit the practice of nurses as well as other mental health professionals, because it allows for a diagnosis of social support shown by the individual and thus making timely interventions in prevention, protection and promotion of mental health of the subject, enabling suicide prevention.
Social support in the subjects' everyday lives
In all patients, according to Figure 2, we can see weak social support, indicated by the absence of friends and leisure activities. Failure to report the bond of friendship and to trust no one, the only refuge is to be alone, or even to attempt suicide. One of the factors that can be directly linked to the increase of suicide is interpersonal difficulty, preventing the individual to make new friends and share aspects of their life with friends. Therefore, they feel isolated, without close contacts or confidants(13).
The human being exists as a being in relation to other people, that is, needs to be included in a social environment. Everyone needs to have the bonds of friendship, leisure time, additional close contacts, or significant relationships from the interaction point of view. Teens who feel excluded from their social groups feel despised, betrayed, sad, even manifesting psychosomatic symptoms; all these feelings of pain and loneliness cause acts of negative thoughts that can lead to isolation and even suicidal behavior(13).
In relation to work, according to Figure 2, only subjects 3, 4 and 5 were employed, with subjects only 3 and 5 reporting work as good. All subjects stated that they did not leave the house, suggesting few recreational options and few physical activities. We emphasize the importance of leisure activities outside of the house and working-out. The practice of physical activities, in general, is a behavioral option that offers a health promotion strategy, as well as improving self-esteem. Social behavior can be improved with the use of eco-map, because by using it you can view the information more effectively, enhancing the social bonds of the individual and search for support(14).
It is common for people to seek psychosocial care though these aspects: the therapist, prayer group, self-esteem group, self-help group and others. The routine of everyday life hinders the reduction of stress, participating in leisure with family and friends, for example, alleviates daily excessive stress. For these people it is important and necessary to reduce the perceived stress by the individual(15).
The person with stress overload, discouraged and looking for relief can often look to church and worship. Through participation in church or in church services there is more contact with people, increasing their number of friends, improving the social bond of these people. Philosophers, social scientists and social psychologists have entered into an agreement in which they consider religion an important aspect of life, with life's setbacks and suffering. Religion is fundamentally important during times of crisis for individuals, such as: the loss of close people, serious illness, disability and death. It is an essential element for humans to have faith and believe that things can be improved, that life gets better, with an emphasis on conversations about health and mental disorders(16).
According to Figure 2, only the individual 6 went to church. Individual 1 participated in church, however infrequently, suggesting their social ties had an impact on maintaining health, functioning as a protective factor in stressful situations; this can reduce their impact on psychological well-being. Thus, having a social support network and receiving help from individuals belonging to this network can benefit their health and well-being. On the other hand, poor social relations is mental health risk factor(17).
Social support is associated with health problems and stress, and is based on two different models. One is the direct effect model that considers social resources beneficial to health, regardless of whether the person experiences stressful events or not. The indirect effect model proposes that social support is associated only with well-being. It can be seen in Figure 2, that social support is absent; therefore, becoming a factor that increases the vulnerability of the subject to stress, psychological distress, depressive feelings and suicidal behavior(18).
Conclusion
The social support network can be a predictor of suicide, but also serves as a resource for prevention of suicide, from the perspective of stress coping theory and also for planning mental health promotion activities. The eco-map proves to be a valuable tool for nurses. It is an assessment tool that can be used to help the user to work out social ties, highlighting those that need to be kept, broken or strengthened as social support. The eco-map serves as a resource to identify and evaluate the social support network, which showed it as weakened, suggesting the psychosocial vulnerability of the subject to new suicide attempts.
It is believed that this study is important for professional nursing practice, as it allows the identification of risk and protective factors for suicide, helping to prevent this event which is important in the current context.
The limitation of this study is that it does not research the care provided to the subject within the health care system, which does not draw conclusions on the merits of health care, however, instead it provides opportunities for important reflection on the social contexts from where the patients are coming, which is important for intervention.
References
1.Organização Mundial de Saúde (OMS). Prevenção do suicídio: um recurso para conselheiros. Genebra: OMS; 2006. [ Links ]
2. Soares MH, Bueno SMV. Saúde mental: novas perspectivas. São Caetano do Sul: Yendis; 2011. [ Links ]
3. Gaspari VPP, Botega NJ. Rede de apoio social e tentativa de suicídio. J Bras Psiquiatria. 2002;51(4):233-40. [ Links ]
4. Fonseca DM, Abelha L, Lovisi GM, Legay LF. Apoio social, eventos estressantes e depressão em casos de tentativa de suicídio: um estudo de caso-controle realizado em um hospital de emergência do Rio de Janeiro. Cad Saúde Coletiva. 2010;18(2):217-28. [ Links ]
5. Nutbeam D. Health promotion glossary. Health Promot Internation. 1998;13(4):349-64. [ Links ]
6. Gonçalves TR, Pawlowski J, Bandeira D, Piccinini CA. Avaliação de apoio social em estudos brasileiros: aspectos conceituais e instrumentos. Ciênc Saúde Coletiva. 2011;16 (3):1755-69. [ Links ]
7. Lazarus RS, Folkman S. Stress, appraisal and coping. New York: Springer; 1984. [ Links ]
8. Mann J. The neurobiology of suicide. Nat Med. 1998;4:25-30. [ Links ]
9. Avanci RC, Pedrão LJ, Costa Júnior ML. Perfil do adolescente que tenta suicídio em uma unidade de emergência. Rev Bras Enferm. 2005;58(5):535-9. [ Links ]
10. Nascimento LC, Rocha SMM, Hayes VE. Contribuições do genograma e do ecomapa para o estudo de famílias em enfermagem pediátrica. Texto Contexto Enferm. 2005;14(2):280-6. [ Links ]
11. Zavaschi LMS, Satler F, Poester D, Vargas CF, Pizenski R, Rohde LAP, et al. Associação entre trauma por perda na infância e depressão na vida adulta. Rev Bras Psiquiatr. [Internet] 2002 [acesso 10 jan 2013]; 24(4):189-95. Disponível em: http://www.scielo.br/pdf/rbp/v24n4/12728.pdf [ Links ]
12. Avanci RC, Pedrão LJ, Costa ML Júnior. Perfil do adolescente que tenta suicídio em uma unidade de emergência. Rev Bras Enferm. 2005;58(5):535-9. [ Links ]
13. Baptista VM. Planejamento social: intencionalidade e instrumentação. São Paulo: Veras; 2007. [ Links ]
14. Pondé MP, Cardoso C. Lazer como fator de proteção da saúde mental. Rev Cienc Med. 2003;12(2):165-72. [ Links ]
15. Dalgalarrondo P. Religião, psicopatologia e saúde mental. Porto Alegre: Artmed; 2008. [ Links ]
16. Harold GK, Religião, espiritualidade e transtornos psicóticos. Rev Psiq Clín. 2007;34(Suppl 1):195-204. [ Links ]
17. Schneider A, Ramires V. Vínculo parental e rede de apoio social: relação com a sintomatologia depressiva na adolescência. Aletheia; 2007;26:95-108. [ Links ]
18. Fonseca DM, Abelha L, Lovisi GM, Legay LF. Apoio social, eventos estressantes e depressão em casos de tentativa de suicídio: um estudo de caso-controle realizado em um hospital de emergência do Rio de Janeiro. Cad Saúde Coletiva. 2010;18(2):217-28. [ Links ]
![]() Correspondence
Correspondence
Marcos Hirata Soares
Universidade Estadual de Londrina. Centro de Ciências da Saúde
Departamento de Enfermagem
Av. Robert Koch, 60
Vila Operária
CEP: 86038-350, Londrina, PR, Brasil
E-mail: mhirata@uel.br
Received: May. 13th 2013
Accepted: Apr. 22nd 2014

{kind=link}
{kind=link}
{kind=link}