










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versão On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.11 no.3 Ribeirão Preto set. 2015
http://dx.doi.org/10.11606/issn.1806-6976.v11i3p168-177
ORIGINAL ARTICLE
DOI: 10.11606/issn.1806-6976.v11i3p168-177
Psychosocial rehabilitation in Psychosocial Care Centers: an integrative review
Marianna de Francisco AmorimI; Márcia Aparecida Padovan OtaniII
ISpecialist in Mental Health, Psychologist, Serviço de Atendimento Psicossocial, Universidade Federal de Mato Grosso do Sul, Campo Grande, MS, Brazil
IIPhD, Professor, Faculdade de Medicina de Marília, Marília, SP, Brazil
ABSTRACT
We investigated the difficulties Psychosocial Care Centers face in carrying out psychosocial rehabilitation by means of an integrative review. We analyzed 35 articles from journals indexed in the LILACS, SciELO, INDEX Psi and PePSIC databases. The results reveal that the concept of psychosocial rehabilitation encompasses a multiplicity of meanings. The articles describe successful experiences, but emphasize various difficulties, such as poor articulation between Psychosocial Care Centers and primary and inter-sectoral care services, actions with a poor level of community focus, few social inclusion initiatives through working, poor support for families and lack of training for health care professionals. We conclude that there must be more debate and reflection on the part of management and professionals in order to improve this process.
Descriptors: Mental Health; Rehabilitation; Mental Health Services; Mental Health Assistance.
Introduction
The process of Psychiatric Reform began in Brazil in the 1970s and lead to various changes in the way the human phenomenon of madness is viewed and dealt with. It was a historical process that sought to question and to draw up proposals to transform the classic psychiatric paradigm (1).
Within the socio-historical context of Brazil, part of current national mental health policy is to create various services to replace the asylum model, of which the Psychosocial Care Centers - Centros de Atenção Psicossocial (CAPS) stand out. CAPS were established by Ordinance 336/GM, 2002, characterized as services primarily responsible for caring for patients with serious and ongoing mental disorders using intensive, semi-intensive and non-intensive treatments and functioning according to territory(2). Thus, the CAPS stand out as being a territorial service, not intramural, like other, traditional, mental health and health care services (3). They are services which enable those with mental suffering to undergo a de-institutionalization process. It should be noted that de-institutionalization means more than breaking down walls, involving transforming ways of viewing and thinking (4).
The CAPS should play an essential role in broadening the social places inhabited by those suffering psychologically (5). Likewise, the importance of strategies to reintegrate users into multiple social contexts is also shown. These services, then, represent a new model of mental health care which should make the psychosocial rehabilitation of their users viable. The objective of CAPS treatment should enable the individuals to manage their own lives, becoming ever more autonomous, increasing users’ capacity to make choices (6).
On the other hand, new types of treatment do not make it certain that individuals undergoing mental suffering are able to take on the condition of citizen, as new services may well be based on former, exclusionary, asylum practices (7). There is also a risk of encouraging the maintenance of the psychiatrized condition in the psychosocial rehabilitation process (7). Thus, the services should be alert and constantly reflect on their practice. There must be constant ethical-technical attention on the part of all involved in the process in order to ensure real change to the care paradigm, considering that rehabilitation implies total transformation of all mental health care service policies (8).
The concept of psychosocial rehabilitation is fundamental to the work carried out in the CAPS. Essential to psychosocial rehabilitation is constructing full citizenship and this depends on variables that affect, positively and negatively, commitments at home, at work and in the social network, corresponding to the subject’s chances of producing emotional and material exchange(8). Thus, the increased contractual power and autonomy of the users should be the principal focus of mental health work.
According to the World Health Organization definition (1987)1, psychosocial rehabilitation is the set of activities that enable the individual’s chances of recovery to be increased, decreasing the debilitating effects of chronic diseases through developing individual, family and community resources(9). It is worth bearing in mind that rehabilitation does not consist of adapting the disabled but rather of a process to alter the rules and to encourage society to live with difference (10), transforming not only mental health care services but also wider society.
The CAPS play an essential role in the articulation of the mental health care network, as it is the service which represents the Brazilian psychiatric reform process. Thus, studies into the difficulties faced by the CAPS in conducting psychosocial rehabilitation, the central tool of these services, become relevant. Moreover, investigating this process may help health care professionals and managers to rethink the practice developed and propose changes to mental health care.
Given the complexity and the implications of the processes of change in mental health care, this study seeks to answer the following question: what are the difficulties the CAPS face in carrying out psychosocial rehabilitation?
This study used an integrative review with the aim of analyzing the descriptions in the literature of the psychosocial rehabilitation process in the CAPS and identify the difficulties faced by these services in the psychosocial rehabilitation process.
Material and Methods
The integrative literature review is a method that allows both experimental and non-experimental studies to be included, giving a synthesis of knowledge with which to understand the specific phenomenon in question (11). Thus, the aim of the integrative review is to produce a consistent and intelligible panorama of the relevant complex concepts, theories or health problems, enabling the results of significant studies to be applies in practice (11).
This study sought to follow the stages described in the process of drawing up an integrative review: 1) drawing up the guiding question; 2) searching or sampling the literature; 3) collecting data; 4) detailed analysis of the studies included; 5) discussion of the results and 6) presenting the integrative review (11).
Documents indexed in the LILACS, SciELO, INDEX Psi and PePSIC databases were analyzed. It is worth noting that broader foreign databases such as PubMed and MEDLINE were not used, as the focus of this study is psychosocial rehabilitation in CAPS, mental health services belonging to the Brazilian Unified Health System.
The descriptors used to search the databases were: Psychosocial Care Center, Mental Health Services, Psychosocial Rehabilitation and Psychosocial Reintegration, specified in the following way: ((center and care and psychosocial) or (service$ and health and mental)) AND ((rehabilitation or reintegration) and psychosocial)).
Criteria for inclusion in the study were: 1) articles in journals published between 2008 and 2012 and 2) studies which approached the psychosocial rehabilitation process in the CAPS. Exclusion criteria included: 1) dissertations and theses, 2) articles describing other mental health care services apart from CAPS and 3) articles which were not related to the aim of this study.
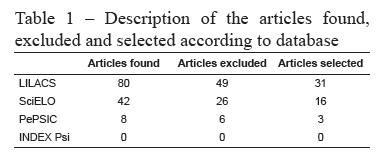
A total of 80 articles were found in the LILACS database, 42 in SciELO, 8 in PePSIC and none in the INDEX Psi, as shown in Table 1. The 130 selected articles were compared, and those which were indexed in more than one database and thus repeated were excluded, leaving 90 articles. Of these, a further 55 were excluded from the analysis, following the pre-established criteria, as they covered topics such as: other mental health care services, characterizing CAPS users, training of mental health care workers and their place in the labour market and validating research instruments. After all exclusions, 35 articles remained to be analyzed, as can be seen in Figure 1.
At the data collection and detailed analysis stages, certain information was analyzed for the articles included, such as: name of authors, year of publication, journal in which published, the background and institution of the lead author and key words used. Later, after successive readings and categorizing of the articles, the aim of the study, the methodological design used (type of study/sample/instruments/type of analysis), main results found, actions conducted by the CAPS and difficulties with psychosocial rehabilitation were identified. From this general panorama, the information obtained were synthesized and discussed.
Results
Based on the analysis of the articles, the data obtained were characterized briefly. The three most commonly used key words in the documents in questions were: “Mental health care services” (49%), “Mental Health” (46%) and “Rehabilitation” (23%). As for the number of publications per State, it was found that, of the 35 articles 16 were from the State of São Paulo (46%), eight from Rio Grande do Sul (23%) and three from Rio de Janeiro (9%). This shows the states in Brazil with the highest scientific output in this area, a fact that can be understood given the historical involvement of these States in the Psychiatric Reform process.
The two journals which published most often on this topic were: Revista da Escola de Enfermagem da USP e Saúde e Sociedade, with three publications each. A further seven journals published two articles each. The two journals with the most publications approach general topics in Nursing and Public Health and do not specialize in the area of mental health.
It was also found that the majority of the publications were the work of nurses (54%), followed by occupational therapists (23%) and psychologists (11%). As for the authors’ links with institutions, except for two articles, all of the authors were linked with higher education institutions (94%), indicating the importance of such institutions in conducting scientific research in Brazil. As for the year of publication, the year with the most was 2011 (29%), followed by 2010 and 2008, both with 20% of the publications.
Regarding the methodological approach used, 32 articles (91%) used qualitative research. Of the rest, one used a quantitative approach (3%) and two used a mixed quanti-qualitative approach (6%). This aspect is explained when the complexity of the object of study in question is considered.
As for the subjects of the research, they were, in descending order: workers (49%), users (43%), family members (26%) and direct observation of CAPS (9%). Many of the studies used more than one subject profile.
With regards the concept of psychosocial rehabilitation in general, it was found that the authors described it in broad terms, encompassing a multiplicity of mental health care actions and there is not, therefore, one single concept. In consequence, the authors approached the psychosocial rehabilitation process in the CAPS in a variety of ways.
As for the actions developed in the CAPS and which could make the psychosocial rehabilitation process viable, it was observed that the authors characterized both the day-to-day activities of the service, as well as the various tools used in health care management.
Of the activities conducted in the CAPS, the treatment workshops and other group activities (operative and therapeutic) stand out. Treatment workshops are an element organized daily in the CAPS and they can be artistic or focus on literacy or on producing income(12). Other actions described include: leisure and recreation activities, family meetings, inter-sectoral and community actions or monitoring treatment, among others (13-16).
The authors point out certain tools for managing mental health care: listening, welcoming, links with professionals, encouraging co-responsibility and autonomy in users, inter-disciplinary work, comprehensive care and individual treatment projects.
In general, the authors mention diverse difficulties in mental health care and in the psychosocial rehabilitation process, as can be seen below.
Social relationships and CAPS
Studies indicate that, for many users, the CAPS is their only social and treatment reference, with their social relationships being limited to this health care service, which in turn limits their social reintegration and realizing the aim of psychosocial rehabilitation (14,17-19).
In the psychosocial rehabilitation process, there are restrictions to the subjects’ commitments to the community, making it difficult to increase and effect emotional and material exchange, as well as hindering social inclusion(14). There is, then, a need to construct, increase and strengthen the resources and power of the social network (14,19). It therefore becomes essential for the subjects with mental disorders to circulate more widely in different spaces in the city (17).
Community and territorial focus
Within the psychosocial rehabilitation perspective, interventions are needed that focus on the community and the territory (19-22), as it is they who guide day-to-day work at the CAPS(21).
In order to be able to conduct effective actions in the territory, the CAPS should be familiar with territorial resources and enable them to be used by the community, in other words, be integrated into the territory so as to allow permeability between the territory and the health care service(21). On the other hand, certain professionals view CAPS as a space of social inclusion in itself, limiting the development of practices which, in fact, enable social reintegration(15,17).
As treatment activities are preferably centered in spaces within the services and minimize territorial and community actions, this means that social inclusion is difficult for those with mental disorders, limiting them to inclusion within the service itself(22). Activities conducted outside of the CAPS are extremely important(15), although there is also the need for the work to have a concrete social reintegration proposal(23).
Insertion in the labor market
Studies show that the quality of life of many users is affected negatively, especially on an occupational and social level(24). The work has different meanings, such as existentialism, social identity, autonomy and sociability (23). In general, in material exchange, the work of those with mental suffering is not of social value (14), making the psychosocial rehabilitation process more difficult.
It is difficult for the CAPS to propose alternatives for inclusion through work, there are practically no projects capable of influencing the conditions of exclusion from the world of work (23). This shows the difficulty of CAPS users becoming part of the labor market (25). Moreover, certain professionals do not consider work as a goal that is within reach of the actions of health care professionals (17). It therefore becomes necessary to develop strategies to produce employment(24), as well as helping users to professionals qualifications through learning a trade (26). Actions related to generating income in the service remain tentative and require greater support if there is to be real inclusion through work for the users, in line with the proposal of psychosocial rehabilitation (27).
Inter-sectoriality
The studies also indicate the importance of partnerships between sectors, that is, greater articulation of the mental health care service network with services in other areas (culture, leisure, accommodation, legal, social services)(17,28-29). Through working with different teams from outside the area of health care, it becomes possible to realize the psychosocial rehabilitation process.
Mental health and primary care
Another important aspect that should be highlighted as essential to the psychosocial rehabilitation process is the articulation between the CAPS and primary health care services. The studies indicate the weakness of this articulation(30-32), there being a lack of planning and implementation of primary health care actions aimed at mental health and fragmentation in the care, and in the reference and counter-reference model (31).
It is, then, necessary for health care services to have an idea of co-responsibility with regards promotion, maintenance and rehabilitating the user in their territory, psychosocial rehabilitation process being worked on through health promotion and disease prevention actions (32).
Health care professionals
Another important point concerning psychosocial rehabilitation is weaknesses in the training of mental health care professionals (30). The service team is broadening its view of mental health when psychosocial rehabilitation is included as the center of care. On the other hand, many professionals hold contradictory conceptions, demonstrating both the psychosocial and the psychiatric paradigm (15). The paradigm shift is taking place gradually(20) and in order for it to come about improvements are needed to both the working conditions and the ongoing education of these professionals (33).
Health care actions are provided with no concrete reference to the guiding proposal the service practice (22,27). Treatment projects are conducted by the professionals as results of directives from management or of the technical guidance belonging to each professional category, but are not activities which are representative of a health care team work philosophy (22). Thus, greater investment is needed in professional training(15), in producing scientific research and practice than enable changes in the position of those who work in CAPS services(26,34).
Family
Dealing with the family and the family’s participation in mental health care is of the utmost importance in the psychosocial rehabilitation process (25,29,35-36). Family members receive little support or guidance about how to act in different situations (14) and the CAPS spaces of participation are seen as important forms of monitoring (26). Thus, interventions are needed to make the family a tool in caring for users (33), understanding that this aspect contributes to psychosocial rehabilitation.
However, there are factors which limit psychosocial rehabilitation in the CAPSm suc as poor articulation between CAPS and primary and inter-sectoral services, actions limited to within the service, without focus on the community and maintaining restricted emotional links, few social inclusion initiatives through work, poor support for families and lack of training for health care professionals.
Discussion
The large increase in the number of CAPS in Brazil, together with reductions in the number of psychiatric beds in recent years show that this type of extra-hospital treatment is a significant dimension for users and their families, as it contributes to reducing the number of hospitalizations and improves quality of life (28).
Some authors considered the activities conducted by the CAPS as equivalent to psychosocial rehabilitation, whereas others analyzed a set of actions as parts of this process, including different management and organization tools in health care.
Studies indicate that psychosocial rehabilitation has not occurred effectively in the CAPS due to the countless difficulties with which these services are faced(14,26,37), demonstrating the risk of the CAPS simply reproducing the asylum model (15). In this sense, psychosocial actions remain on the margins of the treatment project(22), and interventions guided by the psychiatric paradigm predominate. There are also some professionals who do not view such actions as the responsibility of CAPS, but rather of other services, failing to consider the importance of work in the psychosocial care network (38).
There are experiences in which actions conducted in the CAPS, such as treatment workshops and other group activities were decontextualized from the users’ needs, without seeking autonomy, serving only to fill time and thus not contributing to psychosocial rehabilitation(12). This aspect indicates the need for reflection on the theoretical bases of the actions conducted by professionals in the CAPS. Moreover, in the CAPS daily routine, there is a gap between the clinical care and the perspective of psychosocial rehabilitation, indicating the need for practice aimed at broader clinical care, so as to do away with this dichotomy (34).
From this perspective, health care shared with the Psychosocial Care network, as well as with various other sectors, is essential to the psychosocial rehabilitation proposal. The Psychosocial Care Network - Rede de Atenção Psicossocial (RAPS) aims to create, increase and articulate different points of health care for those with mental suffering and needs resulting from alcohol and other drug abuse, with territorial and community based services, encouraging autonomy and citizenship (39). With regards psychosocial rehabilitation, the RAPS encompass initiatives for generating employment and income, solidary enterprises and social cooperatives (39).
As well as the work conducted by the network, that of the inter-disciplinary teams also contributes to the psychosocial rehabilitation process. More horizontal relationships are established between the different disciplines, as well as sharing the same platform of work(40). It is worth noting that a possible tool for establishing inter-disciplinary work is the reference team (40).
Another possible strategy for developing teamwork in the CAPS, as well as improving mental health care and thus psychosocial rehabilitation, is clinical-institutional supervision. The Ministry of Health provides funding for the CAPS Qualification Program, which includes such supervision (41). Clinical-institutional supervision defined as the work of a trained health care professional, from outside of the service, who monitors and discusses the work by the team, the service’s treatment project, the Individual Treatment projects and institutional and management issues, as well as other relevant issues(41).
Overall, mental health care faces many challenges in terms of psychosocial rehabilitation, and many different strategies are needed in order for this process to occur.
Final considerations
In general, it can be seen that the concept of psychosocial rehabilitation, although very present in publications, remains without a univocal definition and encompasses many meanings.
Psychosocial rehabilitation is understood to be a key part of the work done in CAPS, and can be conducted through multiple mental health actions.
This study enables us to state that the analyzed articles describe various experiences in which great efforts are made to realize the psychosocial rehabilitation of individuals being treated, although this process is permeated by several difficulties. The studies also highlight the strategies for coping with such difficulties, which deserve attention from managers and mental health professionals. It is noteworthy that more research is needed to investigate how psychosocial rehabilitation occurs in practice, and how effective this process has been in the lives of individuals with mental disorders, showing its results.
References
1. Amarante PDC, organizador. Loucos pela vida: a trajetória da reforma psiquiátrica no Brasil. 2ª ed. Rio de Janeiro: ENSP; 1995. [ Links ]
2. Ministério da Saúde (BR). Portaria Ministerial n.º 336 de 19 de fevereiro de 2002. Define e estabelece diretrizes para o funcionamento dos Centros de Atenção Psicossocial. Brasília: Ministério da Saúde; 2002. [ Links ]
3. Rabelo AR, organizador. Um manual para o CAPS: Centro de Atenção Psicossocial. 2.ed. Salvador: EDUFBA; 2006. [ Links ]
4. Melman J. Família e doença mental: repensando a relação entre profissionais de saúde e familiares. 2.ed. São Paulo: Escrituras; 2006. [ Links ]
5. Yasui S. A produção do cuidado no território: ‘há tanta vida lá fora’. In: Anais eletrônicos da Conferência Nacional de Saúde Mental; 2010. Brasília: Ministério da Saúde; 2010.
6. Goldberg J. Reabilitação como processo: o Centro de Atenção Psicossocial – CAPS. In: Pitta A, organizadora. Reabilitação psicossocial no Brasil. 2.ed. São Paulo: Hucitec; 2001. p. 33-47. [ Links ]
7. Pinto ATM, Ferreira AAL. Problematizando a reforma psiquiátrica brasileira: a genealogia da reabilitação psicossocial. Psicol Estud. 2010;15(1):27-34. [ Links ]
8. Saraceno B. Reabilitação psicossocial: uma estratégia para a passagem do milênio. In: Pitta A, organizadora. Reabilitação psicossocial no Brasil. 2.ed. São Paulo: Hucitec; 2001. p. 13-8. [ Links ]
9. Pitta A. O que é reabilitação psicossocial no Brasil, hoje? In: Pitta A, organizadora. Reabilitação psicossocial no Brasil. 2.ed. São Paulo: Hucitec; 2001. p. 19-26. [ Links ]
10. Saraceno B. Reabilitação psicossocial: uma prática a espera de teoria. In: Pitta A, organizadora. Reabilitação psicossocial no Brasil. 2ª ed. São Paulo: Hucitec; 2001. p. 150-4. [ Links ]
11. Souza MT, Silva MD, Carvalho R. Revisão integrativa: o que é e como fazer? Einstein. 2010;8(1):102-6. [ Links ]
12. Ribeiro LA, Sala ALB, Oliveira, AGB. As oficinas terapêuticas nos centros de atenção psicossocial. REME Rev Min Enferm. 2008;12(4):516-22. [ Links ]
13. Machado AM, Miasso AI, Pedrão LJ. Sentimento do portador de transtorno mental em processo de reabilitação psicossocial frente à atividade de recreação. Rev Esc Enferm USP. 2011;45(2):458-64. [ Links ]
14. Costa AA, Trevisan ER. Mudanças psicossociais no contexto familiar após a desospitalização do sujeito com transtornos mentais. Saúde Debate. 2012;36(95):606-14. [ Links ]
15. Leão A, Barros S. As representações sociais dos profissionais de saúde mental acerca do modelo de atenção e as possibilidades de inclusão social. Saúde Soc. 2008;17(1):95-106. [ Links ]
16. Carniel ACD, Pedrão JL. Contribuições do acompanhamento terapêutico na assistência ao portador de transtorno mental. Rev Eletrôn Enferm. 2010;12(1):63-72. [ Links ]
17. Leão A, Barros S. Inclusão e exclusão social: as representações sociais dos profissionais de saúde mental. Interface Comum Saúde Educ. 2011;15(36):137-52. [ Links ]
18. Costa CS, Bandeira M, Cavalcanti RLA, Scalon JD. A percepção de pacientes e familiares sobre os resultados do tratamento em serviços de saúde mental. Cad Saúde Pública. 2011;27(5):995-1007. [ Links ]
19. Souza J, Kantorski LP, Vasters GP, Luis MAV. Rede social de usuários de álcool, sob tratamento, em um serviço de saúde mental. Rev. Latino-Am. Enfermagem. 2011;19(1):140-7. [ Links ]
20. Mielke FB, Kantorski LP, Jardim VM, Olschowsky A, Machado MS. O cuidado em saúde mental no CAPS no entendimento dos profissionais. Ciênc Saúde Coletiva. 2009;14(1):159-64. [ Links ]
21. Leão A, Barros S. Território e serviço comunitário de saúde mental: as concepções presentes nos discursos dos atores do processo da reforma psiquiátrica brasileira. Saúde Soc. 2012;21(3):572-86. [ Links ]
22. Fiorati RC, Saeki T. As atividades terapêuticas em dois serviços extra-hospitalares de saúde mental: a inserção das ações psicossociais. Cad Ter Ocup UFSCar. 2012;20(2):207-15. [ Links ]
23. Rodrigues RC, Marinho TPC, Amorim P. Reforma psiquiátrica e inclusão social pelo trabalho. Ciênc Saúde Coletiva. 2010;15(Supl 1):1615-25. [ Links ]
24. Silva TFC, Mason V, Abelha L, Lovisi GM, Cavalcanti MT. A avaliação da qualidade de vida dos pacientes com transtorno do espectro esquizofrênico atendidos nos Centros de Atenção Psicossocial na cidade do Rio de Janeiro. J Bras Psiquiatr. 2011;60(2):91-8. [ Links ]
25. Brasil EGM, Costa EC, Jorge MSB. Representações sociais de usuários e trabalhadores de um centro de atenção psicossocial da região nordeste. Rev Baiana Saúde Pública. 2012;36(2):368-85. [ Links ]
26. Azevedo DM, Miranda FAN. Oficinas terapêuticas como instrumento de reabilitação psicossocial: percepção de familiares. Esc Anna Nery. 2011;15(2):339-45. [ Links ]
27. Kantorski LP, Quevedo ALA, Guedes AC, Bielemann VLM, Heck RM, Borges LR. Oficinas de reciclagem no CAPS Nossa Casa: a visão dos familiares. REME Rev Min Enferm. 2009;13(1):43-8. [ Links ]
28. Nasi C, Schneider JF. O Centro de Atenção Psicossocial no cotidiano dos seus usuários. Rev Esc Enferm USP. 2011;45(5):1157-63. [ Links ]
29. Oliveira E, Oliveira MAF, Claro HG, Paglione HB. Práticas assistenciais no centro de atenção psicossocial de álcool, tabaco e outras drogas. Rev Ter Ocup. 2010;21(3):247-54. [ Links ]
30. Onocko Campos RT, Furtado JP, Passos E, Ferrer AL, Miranda L, Gama CAP. Avaliação da rede de centros de atenção psicossocial: entre a saúde coletiva e a saúde mental. Rev Saúde Pública. 2009;43:16-22. [ Links ]
31. Oliveira FB, Guedes HKA, Oliveira TBS, Lima Júnior JF. (Re)construindo cenários de atuação em saúde mental na Estratégia Saúde da Família. Rev Bras Promoç Saúde. 2011;24(2):109-15. [ Links ]
32. Kantorski LP, Bielemann VLM, Classen BN, Padilha MAS, Bueno MEN, Heck RM. A concepção dos profissionais acerca do projeto terapêutico de centros de atenção psicossocial. Cogitare Enferm. 2010;15(4):659-66. [ Links ]
33. Cavalheri SC. Transformações do modelo assistencial em saúde mental e seu impacto na família. Rev Bras Enferm. 2010;63(1):51-7. [ Links ]
34. Kirschbaum DIR. Concepções produzidas pelos agentes de enfermagem sobre o trabalho em saúde mental com sujeitos psicóticos em um centro de atenção psicossocial. Rev. Latino-Am. Enfermagem. 2009;17(3):368-73. [ Links ]
35. Zanatta AB, Garghetti FC, Lucca SR. O centro de atenção psicossocial álcool e drogas sob a percepção do usuário. Rev Baiana Saúde Pública. 2012;36(1):225-37. [ Links ]
36. Wetzel C, Schwartz E, Lange C, Pinho LB, Zillmer JGC, Kantorski LP. A inserção da família no cuidado de um centro de atenção psicossocial. Ciênc Cuidado Saúde. 2009;8( Supl):40-6. [ Links ]
37. Fiorati RC, Saeki T. Projeto terapêutico nos serviços extra-hospitalares de saúde mental: uma reflexão crítica sobre a forma de elaboração e gestão dos projetos terapêuticos nos serviços. Saúde Soc. 2012;21(3):587-98. [ Links ]
38. Fiorati RC, Saeki T. A inserção da reabilitação psicossocial nos serviços extra-hospitalares de saúde mental: o conflito entre racionalidade instrumental e racionalidade prática. Rev Ter Ocup. 2011;22(1):76-84. [ Links ]
39. Ministério da Saúde (BR). Portaria Ministerial n.º 3088 de 23 de dezembro de 2011. Institui a Rede de Atenção Psicossocial para pessoas com sofrimento ou transtorno mental e com necessidades decorrentes do uso de crack, álcool e outras drogas, no âmbito do Sistema Único de Saúde. Brasília: Ministério da Saúde; 2011. [ Links ]
40. Furtado JP. Equipes de referência: arranjo institucional para potencializar a colaboração entre disciplinas e profissões. Interface Comun Saúde Educ. 2007;11(22):239-55. [ Links ]
41. Ministério da Saúde (BR). Portaria Ministerial n.º 1174 de 7 de julho de 2005. Destina incentivo financeiro emergencial para o Programa de Qualificação dos Centros de Atenção Psicossocial – CAPS e dá outras providências. Brasília: Ministério da Saúde; 2005. [ Links ]
![]() Correspondence
Correspondence
Marianna de Francisco Amorim
Universidade Federal de Mato Grosso do Sul. Serviço de Atenção Psicossocial
Cidade Universitária, s/n. Caixa Postal 549
CEP: 79070-900, Campo Grande, MS, Brasil
E-mail: marianna.amorim@ufms.br
Received: Apr. 30th 2014
Accepted: May 19th 2015
1 World Health Organization. Care for the Mentally III. WHO Collaborating Centre, Douglas Hospital Centre. Montreal; 1987 apud(9)

{kind=link}
{kind=link}