










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versão On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.11 no.4 Ribeirão Preto dez. 2015
http://dx.doi.org/10.11606/issn.1806-6976.v11i4p208-216
ARTIGO ORIGINAL
DOI: 10.11606/issn.1806-6976.v11i4p208-216
Alcohol consumption and the sense of coherence in young people in educational training
El consumo de alcohol y el sentido de coherencia en jóvenes en formación educativa
Lidia Susana Mendes MoutinhoI; Aida Maria de Oliveira Cruz MendesII; Manuel Jose LopesIII
IDoctoral student, Universidade de Lisboa, Lisboa, Portugal. RN, Centro Hospitalar Psiquiátrico de Lisboa, Lisboa, Portugal
IIPhD, Professor, Escola Superior de Enfermagem de Coimbra, Coimbra, Portugal
IIIPhD, Professor, Escola Superior de Enfermagem de Évora, Évora, Portugal
ABSTRACT
The rate of consumption of alcoholic beverages has undergone changes as well as the factors that influence it. In order to understand the significance of drinking patterns, this study was conducted with a sample of young adults (N = 260) ages 20 to 30, in Lisbon. The instruments used were The Alcohol Use Disorders Identification Test and the Sense of Coherence Questionnaire. The results show that 10.8% had problems with alcohol. Those who had a lower sense of coherence, especially in the dimension of investment capacity, presented with more harmful and risky consumption patterns. We conclude that health promotion behaviors should include measures to strengthen a sense of coherence.
Descriptors: Alcohol Drinking; Young Adult; Sense of Coherence.
RESUMEN
El consumo de bebidas alcohólicas ha sufrido alteraciones, y también los factores que lo influencian. Con objeto de percibir el papel del sentido en el estándar de consumo de bebidas alcohólicas, fue desarrollado un estudio en una muestra de jóvenes adultos (N=260) con edad entre 20 y 30 años, en Lisboa. Los instrumentos utilizados fueron el The Alcohol Use Disorder Identification Test y el Questionário do Sentido de Coerência. Los resultados muestran que el 10,8% tiene problemas de consumo de alcohol. Aquellos que poseen sentido de coherencia más bajo, principalmente en la dimensión capacidad de inversión, presentan mayor consumo nocivo y de riesgo. Se concluye que la promoción de comportamientos de salud debe incluir medidas que visen al fortalecimiento del sentido de coherencia.
Descriptores: Consumo de Bebidas Alcohólicas; Adulto Joven; Sentido de Coherencia.
Introduction
Excessive alcohol consumption is considered by the World Health Organization as a major threat to global public health. The world’s highest level of alcohol consumption is in Europe, with about 23 million Europeans (5% of men, 1% of women) dependent on alcohol(1). This fact becomes more worrying if we take into account the increase in risky consumption throughout Europe in the younger population, Portugal without exception.
In Portugal, epidemiological studies on alcohol consumption put this country within a group of countries with mortality rates adjusted for the higher age in Europe, in both sexes(2). With regards to consumption patterns, until a few years ago, it was mostly males, and they preferred to drink wine and beer. Their use was initiated around 15 years old, and, in boys, the onset was earlier(3). In recent decades, however, alcohol consumption has undergone changes with regards to experimentation age, type of drinks and consumption patterns. According to a literature review conducted by Barroso, Barbosa e Mendes(4), the consumption of alcoholic beverages increases progressively with age and the beginning of the consumption is on average 12 years old, verifying identical percentages of individuals of both sexes(5-6). Data revealed by the Drugs and Addiction Institute (DAI)7 reported that in 2011, compared to 2007, there were higher percentages of consumers between 13 and 15 years and most increased alcohol consumption was among girls compared to boys.
In respect to the beverages consumed, differences were also found, especially among young people, who show a notorious preference for beer and spirits(7) to the detriment of wine.
Drinking patterns also changed, with frequent binge drinking, i.e. consuming five or more alcoholic drinks in the same occasion on at least one day in the last 30 days. In a study conducted in Portugal it was concluded that 27.7% of young people aged between 13 and 19 years have adopted this way of drinking(8). Data revealed by the European Survey on Alcohol Consumption and Other Drugs(7) showed that compared to 2007, there was a significant increase in intensive consumption patterns of binge drinking among students from 16 to 18 years.
In Portugal, alcohol is responsible for 60% of the diseases, alcoholic cirrhosis and death by road accident having the greatest impact, particularly among the young(9). It is also known that persons who initiate alcohol consumption during adolescence are more likely to develop dependency(10), so as to undergo direct consequences on the central nervous system, such as cognitive dysfunction, learning and memory restrictions(11).
Thus, these are the known the consequences of alcohol consumption on individual health, its impact on public health and the changes in the patterns of consumption among young people. It is unknown yet what has influenced this change, that is, what has caused each individual to choose to adopt healthy lifestyles or risky behaviors.
If we consider that individual health status depends on how each person interprets life, their cognitive point of view, emotional and motivational, and mobilize the resources available to maintain health and well-being(12); know how individuals face life events, according to their intrinsic and extrinsic characteristics; then this can be useful for integrating successful interventions. An example of an intrinsic feature is the Sense of Coherence (SOC)(13). This takes into account cognitive, affective and motivational characteristics that will allow the individual to deny the clutter from their life, restoring order and coherence to integrate this event into their life experience. It encompasses three dimensions: responsiveness and understanding of capacity - this refers to the ability of the individual to perceive stimuli originating from internal or external means of their existence; manageability or management capacity, with regards to the perception that the individual has about their personal or social resources ability to meet the demands posed by these stimuli; and investment capacity or meaningfulness, with regards to the ability of the individual to make sense of their life events and, therefore, find reasons to invest their energy and interest. A sense of coherence is developed primarily during the first decades of life, being relatively stable after this, especially after 30 years(14).
The existence of the relationship between the perception of health, including components of mental health and a sense of coherence is well documented as being considered a good predictor of adopting health behaviors(15). Work already carried out indicates that there is a relationship between health behaviors and a sense of coherence, which, however, infrequently analyzes their connection with alcohol consumption. In order to understand the role of the sense of coherence in alcohol consumption, this study was developed with a student population in Lisbon, with the research question: "What is the influence of the sense of coherence on alcohol consumption in young adults in educational training, ages 20 to 30 years?"
Methodology
This is a descriptive correlational quantitative study. For its completion, participants were selected from educational establishments, higher education and vocational training, using a sampling technique of convenience. The sample consisted of 260 individuals of both sexes, ages between 20 and 30 years, in the municipality of Lisbon. The application for authorization was performed by the directors of the different institutions and the study was approved by an evaluation committee at the University of Lisbon. After a positive response, we had a meeting with the coordinators of the courses to determine the most appropriate context for the completion of data collection. It was done in the classroom, at previously scheduled times, and the objectives of the study was made known to the participants. After the explanation of the individual’s right to refuse participation at any time without consequences and assurances of confidentiality of the data collection and anonymity of respondents was given, each participant read and signed the Terms of Informed Consent before distribution and completion of the questionnaires. These included an optional field for placing a cell phone number in case of an indication for verification and acceptance of future contacts. Participants with higher score than 8 on the Alcohol Use Disorders Identification Test (AUDIT) were contacted by telephone as recommended by the World Health Organization (WHO), with regards to awareness and education on the consequences of alcohol consumption. After collecting the questionnaires, codification was carried out and the Statistical Package for Social Sciences (SPSS) version 19 was used for the analysis of the data.
The data collection instruments that were used were The Alcohol Use Disorders Identification Test - AUDIT(16-17) and the Sense of Coherence Questionnaire - SOC(14,18).
The selection of the AUDIT was based on the fact that it was developed by the WHO with the specific purpose of screening for problems related to alcohol use. It aims to identify risky drinkers, assesses consumption, dependence symptoms, and the personal and social consequences of drinking in the past 12 months. It consists of 10 questions which include three items on the use of alcohol, four on addiction and three on problems resulting from consumption. It takes about 5 minutes to fill out. This questionnaire can deliver results with scores ranging from zero to forty and displays 92% sensitivity and 93% specificity. A score equal to or greater than one on question two or on question three indicates risk drinking and a score greater than zero on four to six questions, especially with daily or weekly symptoms implies the presence or onset of dependence. The points obtained on questions seven to ten indicate that there are already damages related to alcohol consumption(16). It also allows for the classification of the level of risk and, according to this, a guideline for intervention ranging from information about alcohol consumption to diagnostic assessment with referral to treatment. Risk levels are obtained from the submitted scores. A score of less than 7 corresponds to Zone I, i.e., low risk consumption or abstinence, a score between 8 and 15 identifies medium risk and is referred to as Zone II, participants within Zone III have scores of between 16 and 19, which corresponds to high risk, and scores of 20 or more exhibit criteria for dependence and are referred to as Zone IV.
The Sense of Coherence Questionnaire (SOC)(14,18) consists of 29 items and aims to measure the internal sense of coherence.
The operationalization of the variable, with its three components, is across a range of 29 semantic differential items with seven points (Likert type), positioned between two reference sentences(18). The scores for each subscales is obtained by adding the scores of the respective items, and the items 1, 4, 5, 6, 7, 11, 13, 14, 16, 20, 23, 25, 27 to the reverse. The SOC value is the sum of all items, and the higher the score the greater the internal sense of coherence in question. The psychometric properties of the scale originally created by Antonovsky(13) have a high internal consistency, Cronbach’s alpha for the total scale is between 0.82 and 0.95. Temporal stability is also said to be very satisfactory for intervals 1 year or less (correlation test/retest 0.76 for one year, six months, and 0.80 to 0.91 for two weeks apart)(13,18), the long version of its operational work on the concept sense of coherence was also used. In this study, the value of the coefficient for internal consistency, Cronbach’s alpha, varied between 0.83 and 0.90.
Results
The sample consisted of 260 participants, 32.7% males and 67.3% females with a mean age of 23.87. With regards to the sources of economic support, 20.8% of the cases were coming from a labor occupation, 22.7% had scholarship, 64.2% family support and 6.5% from other sources. The sum is greater than 100% as there are students who reported more than one source of financial support. Participants reported having friends, being the average number of friends of 15.13, a minimum of zero and a maximum of one hundred. Regarding the existence of a stable affective relationship it was concluded that 76.5% reported that this exists and 21.2% said that they do not have one. Six (2.3%) chose not to answer this question.
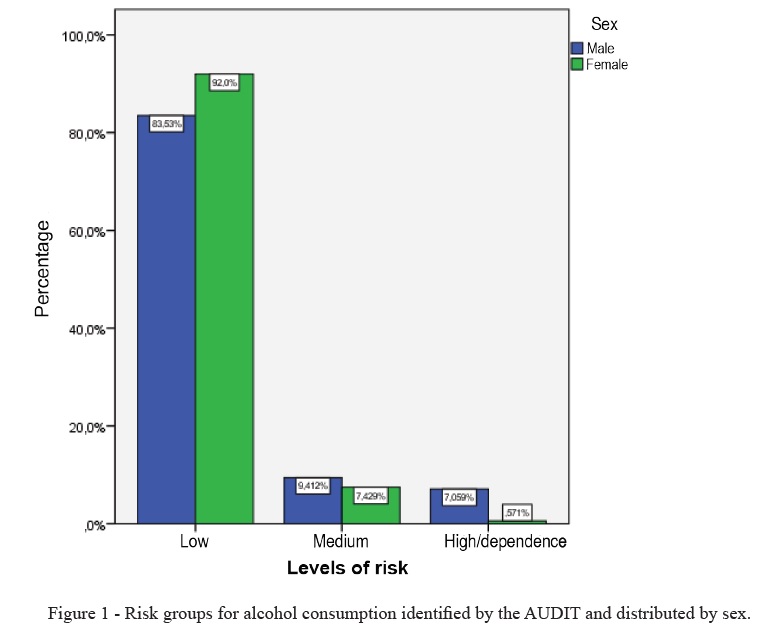
With respect to identifying a pattern of risky or harmful alcohol consumption, it was found that according to the data obtained by the AUDIT, 89.2% of the sample shows no consumption risk. However, 10.8% showed a risky or harmful consumption (Figure 1). When the consumption pattern was analyzed in both sexes, it was found that there were statistically significant differences (t = 3.78; p = 0.00), with male participants presenting the highest consumption risk (X♂ (AUDIT) = 4.99; X♀ (AUDIT) = 2.71).
As far as the sense of coherence, it was found that the average was 139.74. When making the comparison between the two sexes, by t test for independent samples, with the total value of SOC, it was concluded that there are no statistically significant differences (t (230) = -1.387, p = 0.167). However, when analyzing the differences in the three dimensions of SOC statistically significant differences were found in "Investment Capacity" (t (242) = - 2.583, p = 0.01) and the average of this was lower in male participants (average (m) = 41.77, with a standard deviation (SD) = 7.94) compared to women (m = 44.63, SD = 8.16).
When looking at the differences between the groups defined by the AUDIT and the measurement of internal sense of coherence there are differences among the groups for the amount of SOC, F (2.231) = 4.62, p = 0.01. The post-hoc comparisons by Bonferroni test indicated that in Group I, the participants who present low risk or are abstinent, have a higher SOC (m = 140.70, SD = 8.89) compared to Group III (m = 119.42, SD = 8.89), or the group with participants at high risk and/or dependence. This difference is statistically significant to a p-value of 0.01.
As regards to the analysis by the three dimensions that are part of the SOC, it is concluded that there are significant differences in the size or significance of Investment Capacity, F (2, 241) = 3.91, p = 0.02. Group III has significance, i.e. an investment capability that allows them to disconnect from the sense of the events in their life, lower than in Group I (m1 = 43.97/m3 = 35.29, p = 0.02 in test Bonferroni).
Discussion
The sample studied is now in early adulthood, with a mean age of 24 years while still attending school, and 20.8% have already experienced working life. Their group of friends is still extensive, as a characteristic of adolescence, an average of 15 friends who can extend up to a maximum of 100. On the other hand, in accordance with the age group studied, most state that they have a stable loving relationship. According to Erickson(19), up to 30 individuals between 18 and 20 years sought to build deep relationships and initiate professional interest. After a social moratorium and the resolution of the adolescent task of building an identity, young adults develop their skills of relationship with each other and establish commitments, in what Erickson appointed intimacy versus isolation. At the same time, this is a stage of life where individual responsibility for their own eating habits, exercise and lifestyles in general is increasingly dependent on their individual choices. People in this stage of life build their autonomy and develop an overview of their life goals(20). So this is a stage where there are facilitating conditions for alcohol consumption, such as greater autonomy, that can counteract the greater sense of responsibility, less peer influence and more actions based on their own convictions. This is also a stage where young people get education and training necessary for their future careers(21) and where there is a use of alcohol during this important transition, may hinder the success of developmental tasks. It is during the first decades of life, according to Antonovsky (1987)(14), the individual begins to position themselves to view the stimuli from the middle, to identify the resources available to deal with the events of the day, and to distinguish from these, which ones are worthy of their investment and commitment. For this author the individual goes through a continuous process in which, throughout their life, will be faced with two poles of this continuum, one pole being health and the other disease; because they are continually exposed to stimuli originating from the middle, which is necessary for the realization of choices that allow them to remain closer to the pole of health. The choice for healthy behaviors and setting limits to situations that might call into question assumptions that are inherent in individuals with a high SOC(12); these individuals are less likely to participate in harmful consumption(14). With regards to alcohol consumption in the study sample, it is concluded that the highest percentage of participants chose consumption that does not compromise their health. However, considering the entire sample, it is found that 10.2% had risky consumption, and in five cases there was dependence. This value corroborates the data presented by Santana and Negreiros(22), in an investigation in Portugal, which had identical percentages of student’s ages between 16 and 30 years. Other studies conducted in the country, with student’s ages between 13 and 19; found that 68.3% of young people had risky consumption(8). The decreased risk of consumption in the sample can be related to the greater age of this group and they may be more responsible in choosing behaviors that may not jeopardize health.
Considering the equalization of age, alcohol experimentation by individuals of both sexes, and the results of the sample, it is clear that the age at which people develop a relationship with alcohol does not progress in the same way as it occurs predominately in the male participants with medium and high risk drinking. The results are consistent with those of Santana and Negreiros(22), with regards to the predominance of males with this kind of consumption.
In the sample studied, there are not statistically significant differences between the sexes in the sense of coherence, which meets the assumptions defended by Antonovsky (1987)(14) which states that sex does not interfere with the constitution of the sense of coherence. This idea is confirmed in a study conducted for the scale measurement for the Portuguese population which concluded that both sexes showed similar distribution around the median(18). However, there was a statistically significant difference in the dimension of "Investment capacity or meaningfulness" which proved likewise, differentiating the groups regarding the risk levels of consumption. In fact, the participants with higher risk and dependence criteria are mostly male and have a lower sense of coherence, particularly within the meaningfulness or investment capacity. These results agree with those of Mattila et al.(22) pointing at a statistically significant relationship between a low SOC and alcohol consumption. Although each component of the SOC, per se, has no meaning, Antonovsky imparts each centrality differently, and the investment capacity is the most important. This component is seen as the motivational element, referring to how a person feels that their life makes sense on a cognitive and emotional level. The values found indicate the existence of difficulties in these elements of the sample in giving meaning to their life experiences and therefore it is difficult for them to find reasons to invest energy and interest.
The results show that the student population, have different standards of health behaviors in relation to alcohol consumption. Although most of the sample has adequate health behaviors in respect to alcohol, there is a percentage of consumption with the risk of dependence, despite the relatively young age of the group. This reality leads us to reflect on the role of alcohol as an obstacle to the success of the expected developmental tasks and building the sense of coherence in the age group studied.
Conclusion
This study aimed to understand the influence of the SOC in the consumption of alcoholic beverages, and found that there was no difference between the standard consumer groups and sense of coherence. Participants with dependence criteria are mostly men and had a lower SOC than those who did not consume alcohol.
The promotion of behaviors aimed at strengthening the SOC, particularly in the investment capacity component, showed that this is important for the prevention of alcohol consumption. Thus, the promotion of health behaviors should include the provision of information on alcohol consumption and its consequences, but also awareness of the importance of the individual in finding reasons/activities that deserve their interest and investment.
The unevenness of the sample with respect to gender is a limitation of the study, as it would allow for a more precise comparison in respect to consumption patterns and the sense of coherence among the participants. In future research on the subject it will be important to collect information to clarify the binge drinking phenomenon, as well as realize the influence of the sense of coherence on this kind of consumption.
References
1. Anderson P, Baumberg B. Alcohol in Europe - a public health perspective. A report for the European Commission. Institute of Alcohol studies. London: 2006. 446 p. [ Links ]
2. Leifman H, Esa Österberg E, Ramstedt M. Alcohol in postwar Europe: a discussion of indicators on consumption and alcohol-related harm. Stockholm: National Institute of Public Health – Sweden: 2002. 111p.
3. Antunes M. Os jovens e o consumo de bebidas alcoólicas. Referência. 1998;1: 29 -39p. [ Links ]
4. Barroso T, Barbosa A, Mendes A. Programas de prevenção de uso do álcool em jovens estudantes – Revisão sistemática. Referência. 2006, II Série (3):35-44.
5. Feijão F, Lavado E. Assimetrias geográficas e jovens consumidores de drogas. Portugal 2001. Revista Toxicodependências 2003, 9(1):73-84. [ Links ]
6. Matos M, equipa do Projecto Aventura Social e Saúde. A saúde dos adolescentes portugueses: (quatro anos depois): Relatório Português do Estudo HBSC 2002. Lisboa: Edições Faculdade Motricidade Humana. 508 p. [ Links ]
7. Instituto da Droga e Toxicodependencia. Relatório. Estudo sobre o Consumo de Álcool, Tabaco e Drogas – ECATD/ 2011 ("European School Survey on Alcohol and other Drugs – Portugal/ESPAD – Portugal/2011"). Lisboa. 16 p.
8. Reis A, Barros J, Fonseca C, Parreira L, Gomes M, Figueiredo I, et al. Prevalência da Ingestão de álcool nos adolescentes – Estudo PINGA. Revista portuguesa Clínica Geral. 2011 27, 338-346 p.
9. Marinho RART. O álcool e os jovens. Revista Portuguesa de Clínica Geral. 2008 24, 293-300. [ Links ]
10. Dawson D. Defining Risk Drinking. Alcohol Research & Health. 2008; 34(2):144 -57. [ Links ]
11. Zeigler DW, Wang CC, Yoast RA, Dickinson BD, McCaffree MA, Robinowitz CB, et al. The neurocognitive effects of alcohol on adolescents and college students. Preventive Medicine. 2005; 40(1):23-32. [ Links ]
12. Bengel J, Strttmatter R, Willmann H. What keeps people healthy? The current state of discussion and the relevance of Antonovsky’s salutogenic model of health. Research and Practice of Health Promotion. Cologne: Federal Centre for Health Education; 1999 Vol.4.
13. Antonovsky A. The structure and properties of the sense of coherence scale. Social Science and Medicine. 1993; 36(6):725-33. [ Links ]
14. Antonovsky A. Unravelling the mystery of health: how people manage stress and stay well. San Francisco: Jossey-Bass; 1987. [ Links ]
15. Erikson M, Lindstrom B. Antonovsky’s sense of coherence scale and the relation with health: a systematic review. Journal Epidemiol Community health. 2006; 60(5):376-81.
16. Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. AUDIT: The Alcohol Use Disorders Identification Test. Guidelines for Use in Primary Care. 2nd. WHO; 2001. [ Links ]
17. Cunha J. Validação da versão portuguesa dos questionários AUDIT e Five –Shot para identificação de consumo excessivo de álcool. Lisboa: Internato Complementar de Clínica Geral da Zona Sul. 2002.
18. Nunes L. O sentido de coerência como conceito operacionalizador do paradigma salutogénico. IV Congresso Português de Sociologia. Coimbra, Portugal. 2000 Comunicação apresentada no IV Congresso da Associação Portuguesa de Sociologia, no contexto das práticas sociológicas: desafios conceptuais e experiências profissionais (CT 10-07), 17 – 19 de Abril.
19. Levinson DJ. The Mid-Life Transition: A Period in Adult Psychosocial Development. Psychiatry 1977; 40(2):99-112. [ Links ]
20. Schulenberg J, Maggs J, O’Malley P. How and why the understanding of developmental continuity and discontinuity is important: The sample case of long-term consequences of adolescent substance use. In: Mortimer JT, Shanahan MJ, eds. Handbook of the Life Course. New York: Kluwer Academic/Plenum Publishers; 2003. p. 413-36.
21. Santana S, Negreiros J. Consumo de álcool e depressão em jovens portugueses. Revista de Toxicodependências 2008; 14(1):17-24p. [ Links ]
22. Mattila M-L, Rautava P, Honkinen P-L, Ojanlatva A, Jaakkola S, Aromaa M, et al. Sense of coherence and health behavior in adolescence. Acta Paediatrica 2011; 100:1590-5. [ Links ]
Received: Oct. 17th 2014
Accepted: Jun. 24th 2015
Corresponding Author:
Lidia Susana Mendes Moutinho
Rua Martin Luther King 12 10ª Lisboa, AC, Portugal
E-mail: lidiamoutinho@live.com.pt


{kind=link}
{kind=link}